
Abstract
Background and Aims:
The aim of this study was to evaluate the effect of smoking and body mass index on the occurrence of complications after alloplastic breast reconstruction.
Materials and Methods:
A consecutive series of 56 patients treated with immediate or delayed alloplastic breast reconstruction, including six cases combined with latissimus dorsi flap, at three hospitals between 2012 and 2018 were included. Complications were scored and defined according to Clavien–Dindo. To evaluate the impact of smoking, body mass index, and other potential risk factors on the occurrence of any and severe complications, univariate and multivariate logistic regression analyses were applied to estimate odds ratios and 95% confidence intervals.
Results:
In 56 patients, 22 patients had a complication. As much as 46% of smokers had severe complications compared to 18% of non-smokers. Of patients with body mass index ⩾ 25, 40% had severe complications compared to 10% with body mass index < 25. Smokers had eight times more chance of developing severe complications than non-smokers (ORadjusted = 8.0, p = 0.02). Patients with body mass index ⩾ 25 had almost 10 times more severe complications compared to patients with body mass index ⩽ 25 (ORadjusted = 9.9, p = 0.009). No other risk factors were significant.
Conclusion:
Smoking and body mass index ⩾ 25 both increased the complication rate to such an extent that patients should be informed about their increased risk for complications following alloplastic breast reconstruction and on these grounds surgeons may delay alloplastic breast reconstruction. It is an ethical dilemma whether one should deny overweight and obese patients and those who smoke an immediate alloplastic breast reconstruction. For both life style interventions, adequate guidance should be made available.
Keywords
Introduction
Breast cancer is the most common cancer among women in the Western world, with almost 230,000 new cases in the United States each year. Around 35%–58% of women diagnosed with breast cancer undergo mastectomy, of which 25% undergo immediate and 17% delayed breast reconstruction (BR) in the United States (1). The immediate reconstruction rate is similar in the Netherlands (27%), but much higher in the tertiary care center where this study was conducted (48%), according to the Dutch National Breast Cancer Audit for 2016 (2). Complications after alloplastic BR may lead to loss of the reconstructed breast which can have a serious impact on the patient’s emotional well-being (3–6).
According to the literature (7, 8), complications after alloplastic BR are common and occur in about one third of cases. Detailed analysis of complications after BR is necessary to design strategies to prevent these. Individual risk factors need to be detected and if possible eliminated beforehand. It is well established that both smoking and high body mass index (BMI) reduce general health and increase individual morbidity and mortality (9, 10). Smoking was found to increase the risk of developing postoperative complications after reconstruction with autologous flaps (11–14) and following alloplastic BR (15–17). However, not all research is equivocal on this aspect (18–20). For example, a study on tissue expansion did not find smoking to be a risk factor for developing complications, possibly due to low smoking incidence in that study population (8%) (21). In patients with BMI > 30, higher morbidity in autologous BR compared to alloplastic BR has been found (22). In the case of alloplastic BR, BMI > 35 is also associated with an increased risk of postoperative complications (23). Currently, no data are available on the relation between BMI and complications after alloplastic BR with a cut-off point of 25, even though 25 is the international cut-off point between healthy weight and overweight and a BMI of over 25 is known to be associated with higher morbidity and mortality (24, 25).
Because of the disparity in results published on smoking and BMI in relation to complications after alloplastic BR (18–21, 26), we set out to evaluate the effect of smoking, BMI ⩾ 25, and other possible risk factors on the occurrence of complications after alloplastic BR at our study centers. The outcome of this study may help improve individual counseling for women who contemplate to undergo BR with implants or tissue expanders (TEs) after prophylactic mastectomy or breast cancer treatment.
Materials and Methods
Context
For an ongoing prospective cohort study on BR, we included 104 patients to evaluate long-term changes in quality of life between women treated with alloplastic and autologous reconstruction. Women undergoing BR were asked to participate at one tertiary care center and two general hospitals: University Medical Center Groningen (UMCG), Nij Smellinghe Hospital Drachten, and Medical Center Leeuwarden (MCL). Ethical approval for this study was obtained from the Medical Ethics Committee (2010.190). In this cohort, we included a consecutive series of 56 women treated with alloplastic BR. Prior to starting this project, our primary interest was the effect of smoking on complications. We performed a power analysis to determine the sample size needed to confirm our hypothesis that smokers have an increased risk. Assuming 26% smokers, the sample size of 56 patients would be sufficient to identify a difference in the complication rate of 50% in smokers and 10% in non-smokers. Therefore, data of these 56 patients were used for the current analyses on complications after alloplastic BR.
Patients, Inclusion, and Exclusion
Patients that had been counseled for alloplastic BR since 2012 were approached to participate when scheduled to undergo one of the following reconstruction techniques: immediate or delayed reconstruction with TE or implant, or TE or implant combined with a local/regional flap. Both patients with current or previous breast cancer and patients undergoing prophylactic mastectomy were included. Written informed consent was obtained from all the participants. A minimum follow-up of 30 days after reconstruction was necessary for inclusion. Patients treated with autologous BR, patients below 18 years of age, patients who were legally incompetent, and patients who had a poor prognosis due to stage IV breast cancer were excluded.
Data Collection
We collected data on patient characteristics, complications, reconstruction technique, and subsequent procedures related to and following BR. Patient characteristics were prospectively gathered in the context of our quality-of-life study through a detailed intake by a nurse specialized in BR counseling (Table 1). These included smoking status, BMI, age, BRCA mutation, breast side(s) to be operated, comorbidities, and adjuvant breast cancer therapies. Data on subsequent procedures, secondary surgeries, and complications were retrieved from the electronic patient records.
Patient characteristics.
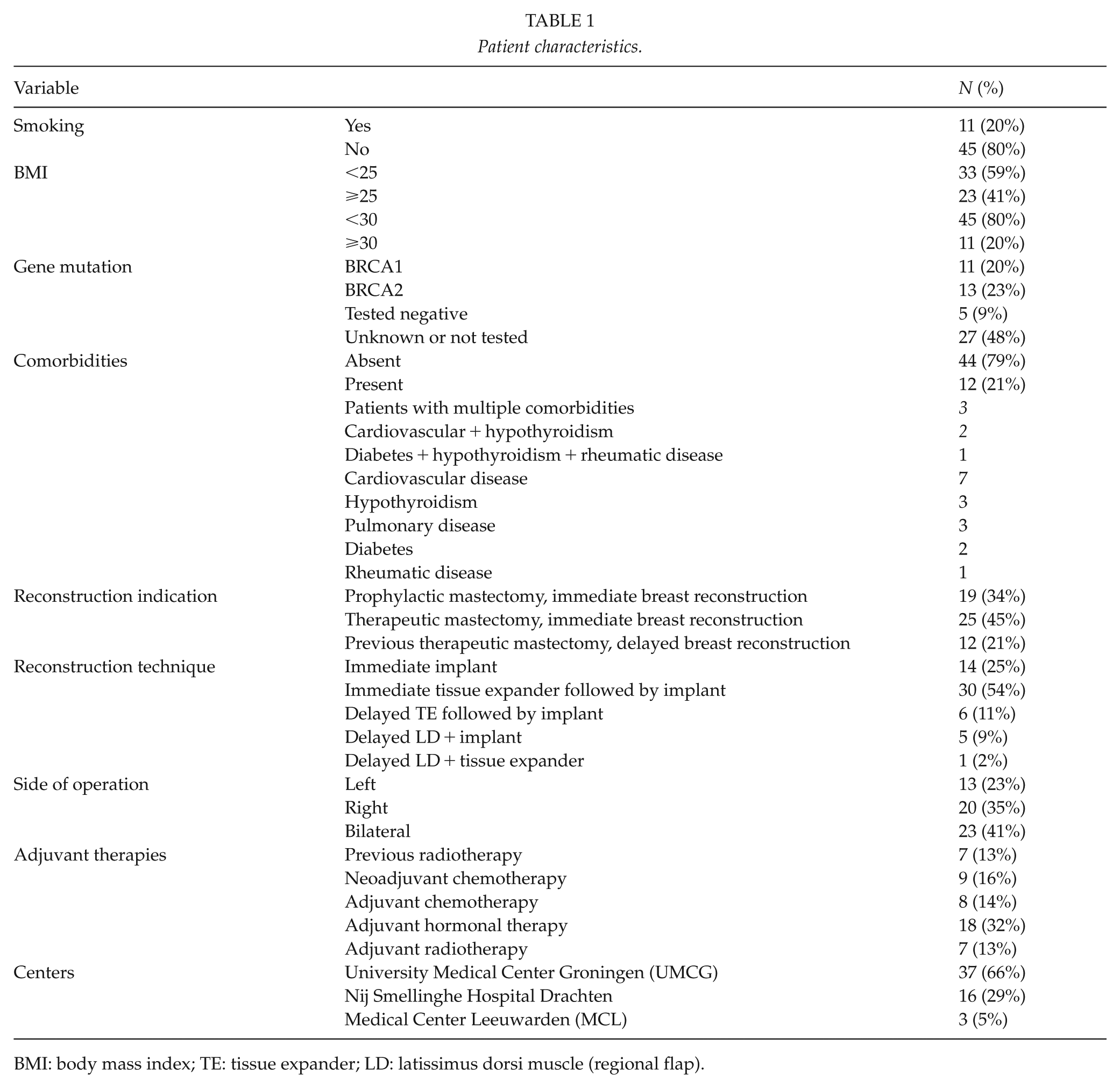
BMI: body mass index; TE: tissue expander; LD: latissimus dorsi muscle (regional flap).
Definitions
Smoking status was dichotomized as “smoker” or “non-smoker.” “Non-smokers” were either patients who never smoked or stopped for a minimum period of 6 months prior to reconstruction. BMI was calculated in kg/m2. Age was calculated in years on the day of the reconstruction. BRCA mutation was divided into known (BRCA1 or BRCA2), unknown (not tested), or tested and not positive. Breast side was left, right, or bilateral. The following comorbidities were included: diabetes, hypothyroidism, lung disease, cardiovas-cular disease, and rheumatic disorders. Adjuvant therapies included radiotherapy before or after reconstruction, adjuvant hormonal therapy, and neoadjuvant or adjuvant chemotherapy.
The treatment of alloplastic BR often involved multiple stages. In the case of TE reconstruction, TE exchange for the permanent implant is Stage 2 of reconstruction. The final surgical stage of reconstruction is nipple reconstruction (Stage 3). In the case of immediate implant reconstruction, the surgical nipple reconstruction is Stage 2. Surgical nipple reconstruction is often followed by nipple tattooing (Stage 4, respectively 3). Additional surgical procedures for cosmetic improvement may include dog ear corrections, lipofilling, symmetrizing augmentation, or symmetrizing reduction mammoplasty.
The primary outcome measure was complications. All postoperative complications of reconstruction were scored. The Clavien–Dindo (CD) classification (Table 2) was used to categorize the complications (27). Grade I refers to complications such as self-limiting superficial skin/nipple necrosis and seroma. Grade II refers to superficial infections (not opened at the bedside) treated with oral antibiotics but without surgical intervention, mostly cellulitis. Grade IIIa is skin necrosis requiring surgical intervention under general anesthesia. Grade IIIb contains complications requiring surgical intervention under general anesthesia such as deep infection, leakage of TE, and postoperative hemorrhage. In this study, the choice was made to define seroma that was treated by watchful waiting combined with prophylactic administration of antibiotics as a Grade I complication and not Grade II, since we interpreted this to be less severe than the therapeutic administration of antibiotics that were Grade II complications.
Complications by grade in the Clavien–Dindo classification.
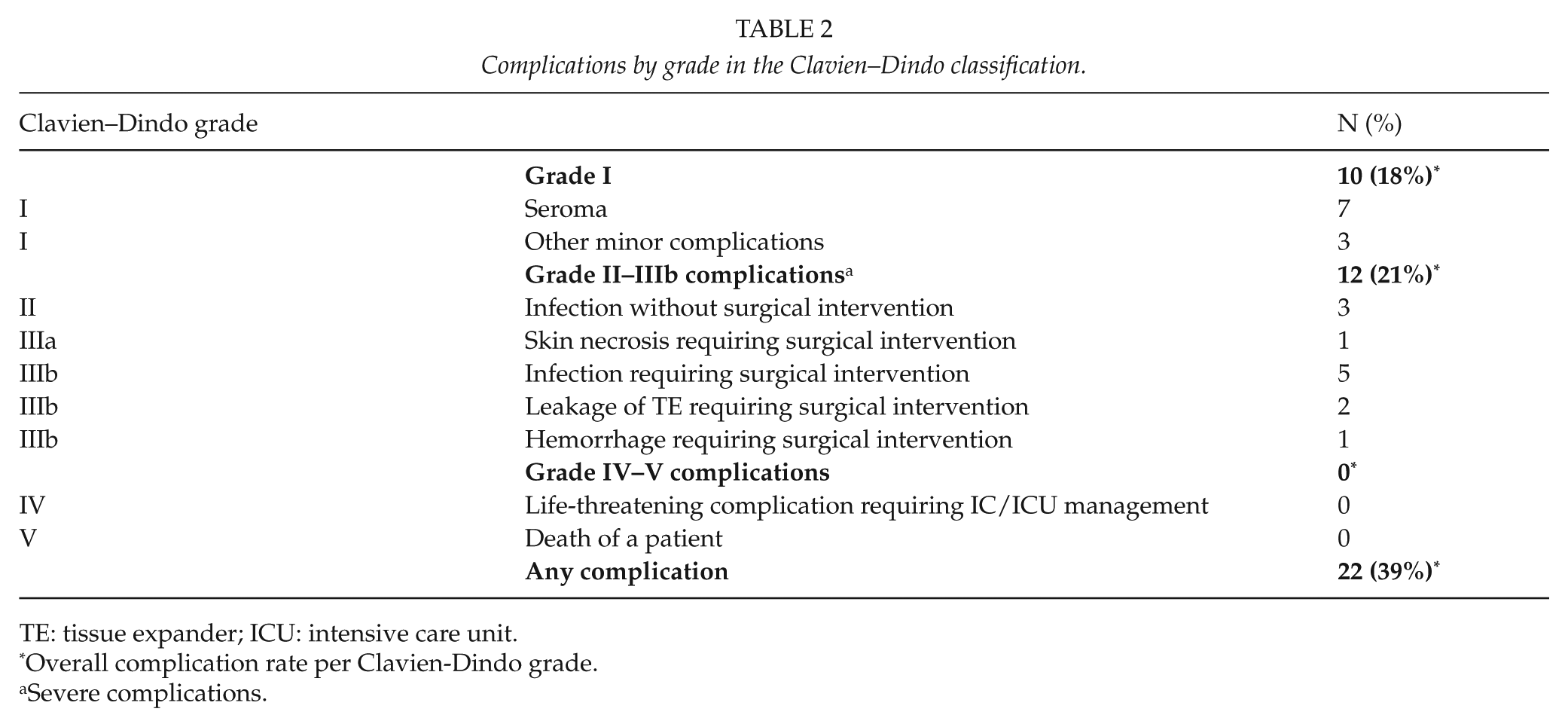
TE: tissue expander; ICU: intensive care unit.
Overall complication rate per Clavien-Dindo grade.
Severe complications.
In case seroma developed into infection, this was registered as one complication and defined as infection. In case patients had more than one complication during multiple stages of treatment, the most severe event was scored. The number of complications per patient was tracked. We analyzed both the occurrence of any complication and separately the occurrence of severe complications CD II–V. CD II–V were considered severe complications since these are complications that led to medical or surgical intervention and can have a serious impact on emotional well-being (28).
Statistics
Univariate and multivariate logistic regression analyses were applied to estimate odds ratios (ORs) and 95% confidence intervals (CIs) to analyze the association between possible risk factors for both any and severe complications. Based on the literature (12), the following determinants were dichotomized (yes/no) for logistic regression analyses: smoking, radiotherapy regardless of timing, adjuvant hormonal therapy, neoadjuvant or adjuvant chemotherapy, any comorbidities, and simultaneous bilateral surgery. BMI was non-normally distributed and categorized as BMI < 25 or BMI ⩾ 25. In addition, we performed analyses on BMI < 30 and BMI ⩾ 30 since most of the previously published articles used this cut-off point. Age was normally distributed and implemented as a continuous variable. A p-value < 0.05 was considered statistically significant. All analyses were conducted with IBM SPSS statistics version 23.
Results
Twenty percent of the participants smoked (Table 1). All former smokers had ceased smoking for more than 6 months preoperatively. The median BMI of the whole cohort was 23.9, ranging from 17 to 39 (mean 25.7, standard deviation (SD) = 4.9). In total, 23 patients had a BMI ⩾ 25 where 11 patients had a BMI ⩾ 30. The mean age of participants was 46.5 years (SD = 10.5, range 27–73). Prophylactic mastectomy followed by immediate BR was performed in 19 patients (34%) all of which were BRCA mutation carriers. Almost half of the patients (n = 25; 45%) underwent therapeutic mastectomy followed by immediate BR. Out of the 44 patients undergoing an immediate BR, 14 (32%) were reconstructed using definitive implants and 30 (68%) underwent two-stage reconstruction with a TE as the first stage. The remaining 12 patients (21%) underwent a delayed reconstruction after previous mastectomy for breast cancer with either TE (n = 7) or definitive implant (n = 5). Overall, in total 37 patients were reconstructed with TE, of which 33 (90%) ultimately received a permanent implant (Stage 2). Surgical nipple reconstruction was performed in 13 women after TE exchange (Stage 3) and in 8 as Stage 2 after reconstruction with direct implants. As a result, 42% (8/19) of patients underwent two surgical procedures and 40% (13/33) underwent three surgical procedures. 10 patients underwent additional surgical procedures for cosmetic improvement: dog ear corrections (N = 2), lipofilling (N = 2), symmetrizing augmentation (N = 1), and symmetrizing reduction mammoplasty (N = 5). The average follow-up of patients in this study was 24.5 months (range 4–60).
Complications
The overall complication rate was 39% (22/56). Severe complications of the category CD II–III occurred in 21% of patients (12/56; Table 2), CD IV–V complications did not occur in this study. Most complications (17/22; 77%) occurred within 30 days of the first stage of the reconstruction. One patient had an infection (cellulitis) 1 week after replacement of the TE with a permanent implant, which was resolved by administration of antibiotics. Another patient had a superficial infection of the nipple 3 weeks after surgical nipple reconstruction, which was treated with antibiotic cream. In total, 19 patients had complications (19/22; 86%) within 30 days of any surgical procedure. Of the three remaining patients, one had explantation of the implant after 2 months because of infection, and one had antibiotics for a deep infection of the TE 4 months after insertion. Another patient had replacement of the TE after 4 months because of leakage of the TE during the expansion phase. The incidence of complications after exchange of the TE for the permanent implant (Stage 2) was low (2/33; 6%). The proportion of patients with severe complications was similar for those who received an immediate implant (3/14; 21%) and those who received an immediate TE (7/30; 23%). Among patients undergoing delayed reconstruction, the rate of severe complications was 17% (2/12). Out of the 12 patients treated with delayed reconstruction, 6 underwent BR combined with latissimus dorsi (LD), of which one patient suffered from a hemorrhage which led to a reoperation (1/6; 17%); of the remaining six patients treated by delayed reconstruction without LD, one patient had an infection which also led to reoperation (1/6; 17%). One patient that underwent prophylactic mastectomy followed by immediate reconstruction suffered from an infection which led to removal of the implant; after a second reconstruction attempt, another infection occurred again leading to loss of the implant. The patient was a renowned smoker with a BMI of 22.8. No other secondary events were registered.
Factors Associated with The Occurrence of Complications
Complications occurred in 82% of smokers against 29% in non-smokers, and in 57% of patients with BMI ⩾ 25 against 42% of patients with BMI < 25 (see Table 3; OR: 11; 95% CI = 2.1–58 and OR: 3.5; 95% CI = 1.1–11, respectively). Severe complications also occurred more often in smokers (46%) than in non-smokers (18%), and in patients with BMI ⩾ 25 (40%) against 10% of patients with BMI < 25 (see Table 3; OR: 4.5; 95% CI = 1.1–19 and OR: 6.4; 95% CI = 1.5–28, respectively). Radiotherapy regardless of timing, adjuvant hormonal therapy, neoadjuvant or adjuvant chemotherapy, any comorbidities, and simultaneous bilateral surgery were no significant predictors of the occurrence of complications. In a multivariate analysis, the risk of developing a severe complication was 8 times higher in smokers (ORadjusted = 8.0, 95% CI = 1.3–49, p = 0.02) and almost 10 times higher in patients with a BMI ⩾ 25 (ORadjusted = 9.9, 95% CI = 1.8–55, p = 0.009).
Univariate and multivariate logistic regression analyses of complications.
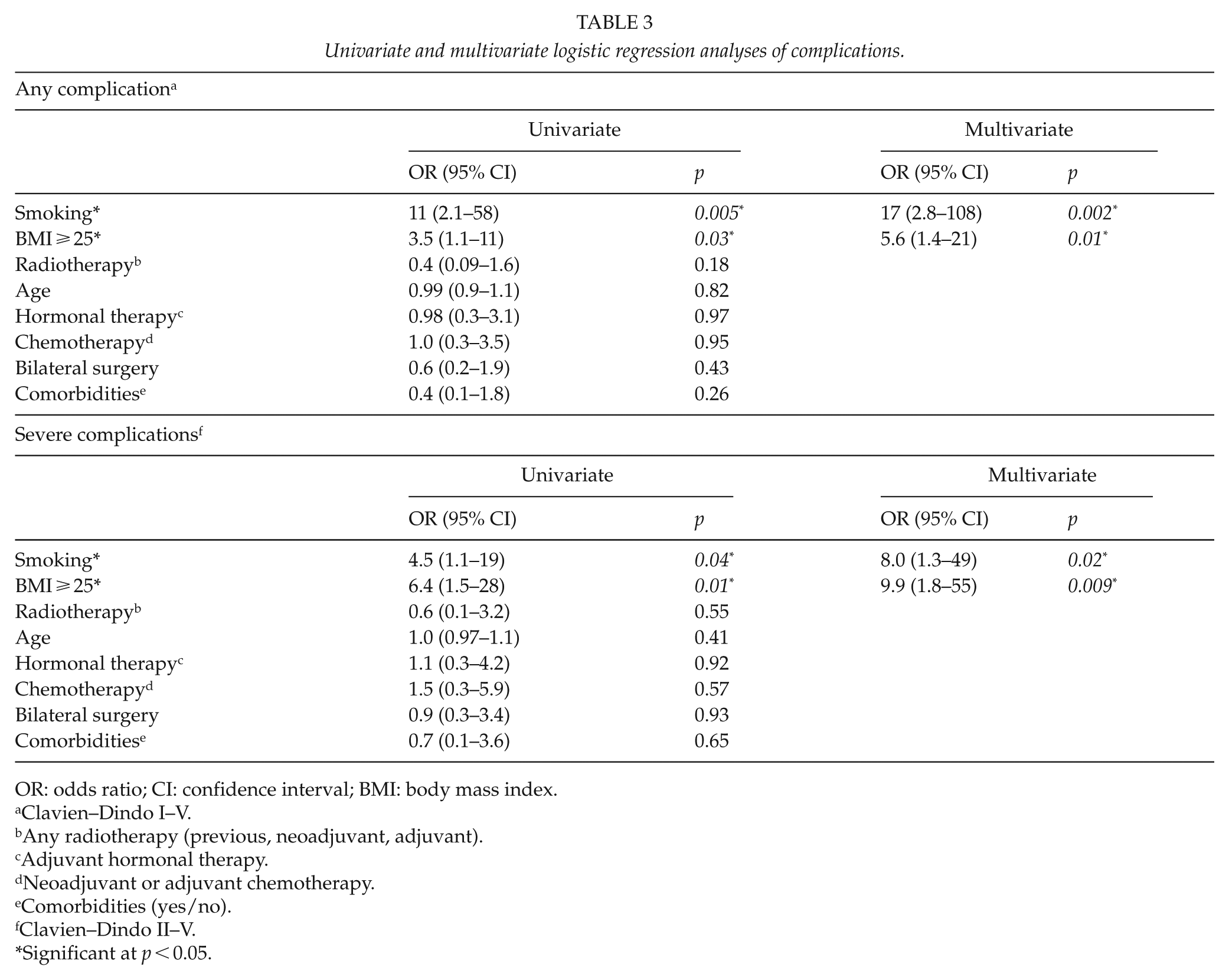
OR: odds ratio; CI: confidence interval; BMI: body mass index.
Clavien–Dindo I–V.
Any radiotherapy (previous, neoadjuvant, adjuvant).
Adjuvant hormonal therapy.
Neoadjuvant or adjuvant chemotherapy.
Comorbidities (yes/no).
Clavien–Dindo II–V.
Significant at p < 0.05.
For patients with a BMI ⩾ 30 compared to patients with a lower BMI, the association between being overweight and the occurrence of complications was comparable; see supplementary Table 1.
Discussion
In total, 39% of the patients had any complication and 21% had severe complications. Out of 11 smokers, 81% had any complication compared to 29% of non-smokers, where 57% of the patients with BMI ⩾ 25 had any complication. In multivariate regression analysis, smokers had an 8 times higher risk of developing severe complications and patients with BMI ⩾ 25 almost 10 times higher risk (ORadjusted = 8.0, 95% CI = 1.3–49 and ORadjusted = 9.9, 95% CI = 1.8–55, respectively).
The absolute incidence of complications in this study was slightly higher (any complication 39%) than the incidence of complications found in the literature (30%–34%) (7). There may be several reasons that explain this. The percentage of smokers in the previously published articles had a large variation (8%–23%) (7, 12, 16, 21, 29) and was relatively high in our population (20%). This can partly be explained by the high percentage of smokers in the area of our study centers: in 2016, 21%–24% of women aged 45–64 in the north of the Netherlands smoked. A study on complications after BR in the northeast of the United States reported 14% smokers (16), which is consistent with the percentage of smokers in that area (13%) (30). The women in our study had a slightly higher mean BMI (25.7 ± 4.9) than women in other studies (24.8 ± 3.6) (7). The higher percentage of overall complications may also partially be explained by the high percentage of immediate reconstruction (79%), which seems to lead to more complications than delayed reconstruction (31, 32). The incidence of severe complications (21%) was similar to the literature (21.2%–23.2%) but should be interpreted with care since the classification used may be different from the CD classification (8, 26, 32). Some studies define scar corrections, dog ear corrections, and other reoperations for cosmetic improvement as complications, but these were not registered as complications in this study and therefore do not explain our high incidence of complications (7, 12, 15, 33).
We found comparable ORs for smoking (ORunadjusted = 4.5 compared to ORunadjusted = 4.9) and BMI (ORunadjusted = 6.4 compared to ORunadjusted = 6.9) compared to other research on complications (16). Previously published research on reconstructive failure (CD III) showed that smokers had a five times higher risk and patients with BMI ⩾ 30 had a seven times higher risk for reconstructive failure (16). Remarkable is that our results are comparable, though we used a cut-off point of 25 for BMI instead of 30. We decided to do so because a BMI ⩾ 25 is considered overweight (25). Moreover, in our study, we included CD II in our severe complications as these complications need medical treatment. In contrast to most publications, radiotherapy did not seem to have an effect on the incidence of complications, probably due to our small study sample and low percentage of patients with radiotherapy on study (11%) (12, 34, 35).
One of the strong aspects of this study is that patients have been included prospectively which prevents selection bias, and relevant data were prospectively recorded. Thus far, most research on complications was of retrospective nature. Complications were well defined with the use of the CD classification (27) and there was a strong discrimination between real infections and antibiotics prescribed to prevent infection. The small study group was a limitation to further perform analyses per type or timing of complication, and most (86%) complications occurred within 30 days of any surgical procedure. As a consequence, we were not able to differentiate between early- and late-onset complications. BMI was assessed objectively, as length and weight were measured during the preoperative consultation. Although higher BMI was clearly linked to more complications, BMI alone probably does not provide sufficient insight into individual physical fitness. Abdominal circumference, muscle fat proportions, and physical activity should also be taken into consideration when helping choose adequate treatment (25). This will be one of the goals of future research at our department.
This study has clearly pointed out that smoking and BMI ⩾ 25 strongly increase the rate of complications after alloplastic BR and these could be the factors that may be used for interventions aiming at the reduction of complications. In the participating hospitals in this study, smokers are already denied autologous BR until they have ceased smoking for 6 months. This restriction is not maintained for alloplastic BR. We are currently adopting the policy that all patients should be encouraged to cease smoking before any type of BR. To support patients, a referral to smoking cessation clinics, usually covered by health insurance companies, is offered. What the optimal cessation period should be before surgery remains unclear. For at least 4 weeks of cessation, a significant decrease in complications was found (36–38). In the context of a cancer diagnosis, a delay of 4 weeks between the first consultation and surgery is acceptable to allow to stop smoking and reduce the chance of developing complications. Thus far, there are no studies on the effect of preoperative weight loss on the occurrence of complications.
Conclusion
In this study, smokers had an 8 times higher risk and patients with a high BMI had almost 10 times higher risk of developing severe complications. On these grounds, surgeons may consider to delay alloplastic BR. It is an ethical dilemma whether one should deny overweight and obese patients and those who smoke an immediate alloplastic BR. For both life style interventions, adequate guidance should be made available.
Supplemental Material
Supplementary_Table_1_Analyses_with_BMI – Supplemental material for The Effect of Smoking and Body Mass Index on The Complication Rate of Alloplastic Breast Reconstruction
Supplemental material, Supplementary_Table_1_Analyses_with_BMI for The Effect of Smoking and Body Mass Index on The Complication Rate of Alloplastic Breast Reconstruction by N. Sadok, I. S. Krabbe-Timmerman, G. H. de Bock, P. M. N. Werker and L. Jansen in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors are indebted to the women who participated in this study and to the surgeons, physician assistants, nurses, and supporting staff from the participating departments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.