
Abstract
Background and Aims:
The management of duodenal trauma remains controversial. This retrospective audit of a prospectively maintained database was intended to clarify the operative management of duodenal injury at our institution and to assess the risk factors for leak following primary duodenal repair.
Materials and Methods:
This was a retrospective study undertaken at the Pietermaritzburg Metropolitan Trauma Service, Pietermaritzburg, South Africa. Operative techniques used for duodenal repair were recorded. Our primary outcome was duodenal leak in the postoperative period. Patients from January 2012 to December 2016 were included. All duodenal injuries were graded according to the American Association for the Surgery of Trauma (AAST) grading. Only patients who had a primary repair were included in the final analysis.
Results:
During the five-year data collection period, a total of 562 patients underwent a trauma laparotomy; of which 94 patients sustained a duodenal injury. A primary pyloric exclusion and gastro-jejunostomy (PEG) was performed in three patients. These three were then excluded from further analysis. Of the 91 primary duodenal repairs, seven (8%) subsequently leaked. These were managed by PEG in three and by secondary repair and para-duodenal drainage in four. The two physiological parameters most associated with subsequent leak were lactate and pH level. There was a significantly higher mortality rate for those who leaked vs those who did not leak. Chi-squared test revealed a significant difference in the leak rate between AAST I (0%), AAST-II (1.6%) and AAST-3 (66.7%) grade injuries (p <0.01).
Conclusion:
The trend towards primary repair of duodenal injuries appears to be justified. However duodenal leak remains a significant risk in certain high risk patients and strategies to manage injuries in this subset requires further work.
Keywords
Introduction
The management of duodenal trauma remains controversial. These injuries are relatively rare and their management is made challenging by the retroperitoneal position of the duodenum and by its physiological function (1, 2). This has led to a number of proposed surgical strategies developed to restore continuity of the duodenum while reducing the flow of secretions over the repair (3, 4). The plethora of strategies has created confusion in the literature as to the optimal management approach. Although almost all reports on this injury and its management are by necessity retrospective, the trend in the literature for the management of these injuries has been away from complex operative strategies towards a more minimalistic approach. This study reviews our overall experience with these injuries and aims to benchmark our operative management of this injury, as well as describing the risk factors for leakage.
Materials and Methods
This was a retrospective study undertaken at the Pietermaritzburg Metropolitan Trauma Service (PMTS), Pietermaritzburg, South Africa. The PMTS provides definitive trauma care to the city of Pietermaritzburg, the capital of Kwa Zulu Natal (KZN) province. It is one of the largest academic trauma centers in KZN, serving as the referral center for 19 rural hospitals within the province, with a total catchment population of over 3 million people. The annual admission volume exceeds 4000 trauma victims with over 50% having sustained penetrating trauma.
Patients from January 2012 to December 2016 were reviewed from our regional electronic trauma register—the Hybrid Electronic Medical Registry (HEMR). Ethical approval for this study and for maintenance of the registry was obtained from the Biomedical Research Ethics Committee of the University of Kwa Zulu Natal (reference: BE 207/09 and BCA 221/13). A search of the registry was performed, and all patients with duodenal injury identified at trauma laparotomy were retrieved and analyzed. All of the included patients in this study underwent a laparotomy, during which the duodenum was exposed and mobilized as required. Duodenal injuries were graded operatively using the American Association for the Surgery of Trauma (AAST) grading system (Fig. 1). Operative techniques used for duodenal repair were recorded. For clarity, only those who underwent primary duodenal repairs were included in the further analysis. Details of the site and grade of the injury, the operative management, and the clinical outcome were recorded. The duodenal injury was classified according to the AAST scale. Associated visceral and vascular injury, presenting physiology, and mechanism of injury were retrospectively collected. Our primary outcome was duodenal leak in the postoperative period, and the secondary outcomes of intensive care unit (ICU) stay and patient mortality were also assessed.
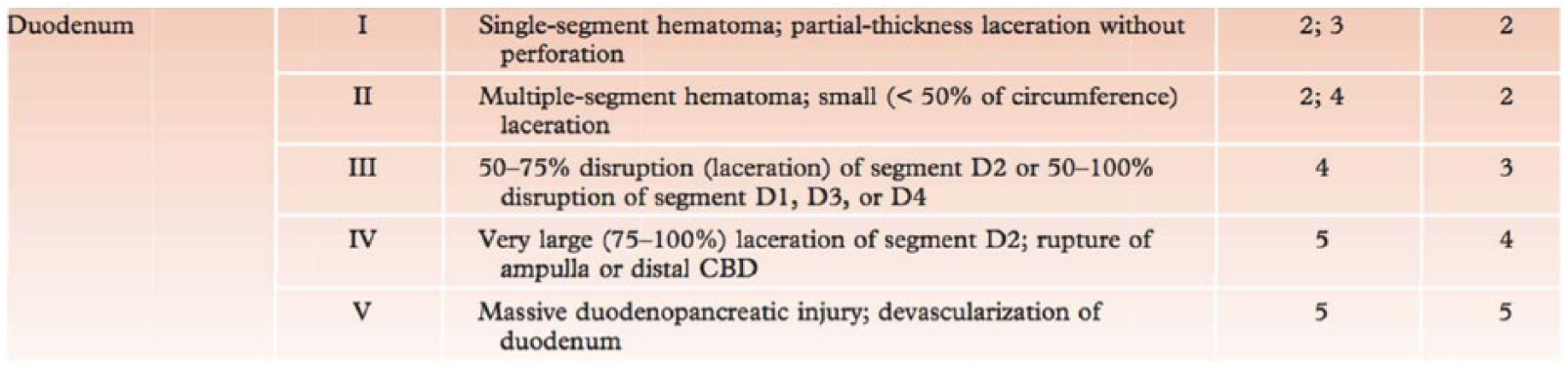
Duodenal injuries are graded operatively using the American Association for the Surgery of Trauma (AAST) grading system.
Management of Duodenal Injuries
Our approach for most duodenal injuries is to perform a primary duodenal repair using an interrupted suturing technique and leave a para-duodenal drain. A feeding tube is passed beyond the injury and secured with a nasal halter. Generally, we reserve the pyloric exclusion and gastroenterostomy (PEG) procedure for cases where there is an excessive delay or if there is a large duodenal wall defect or combined pancreatic injury. Pancreatico-duodenectomy is reserved for destructive lesions of the head of the pancreas and the duodenum and is almost never performed as an emergency procedure.
Statistics
Statistical analysis was performed using STATA software 15.0©. Unpaired t-test was used to compare continuous variables and chi-square analysis for categorical variables. If the expected value is <5, Fisher’s exact test was alternatively used. Statistical significance was accepted for p ⩽0.05 throughout. We tested whether or not each continuous variable met the assumptions for parametric tests; medians (Q1, Q3) instead of means were used to describe the data for those that were not normally distributed.
Results
During the 5-year period, a total of 562 patients underwent a trauma laparotomy, of which 94 patients sustained a duodenal injury. PEG was performed in three patients. The remaining 91 patients underwent a primary repair (Fig. 2). Of these three cases who had a primary PEG, all were blunt in mechanism, and all survived and none leaked. This subset was not included any further in this analysis.
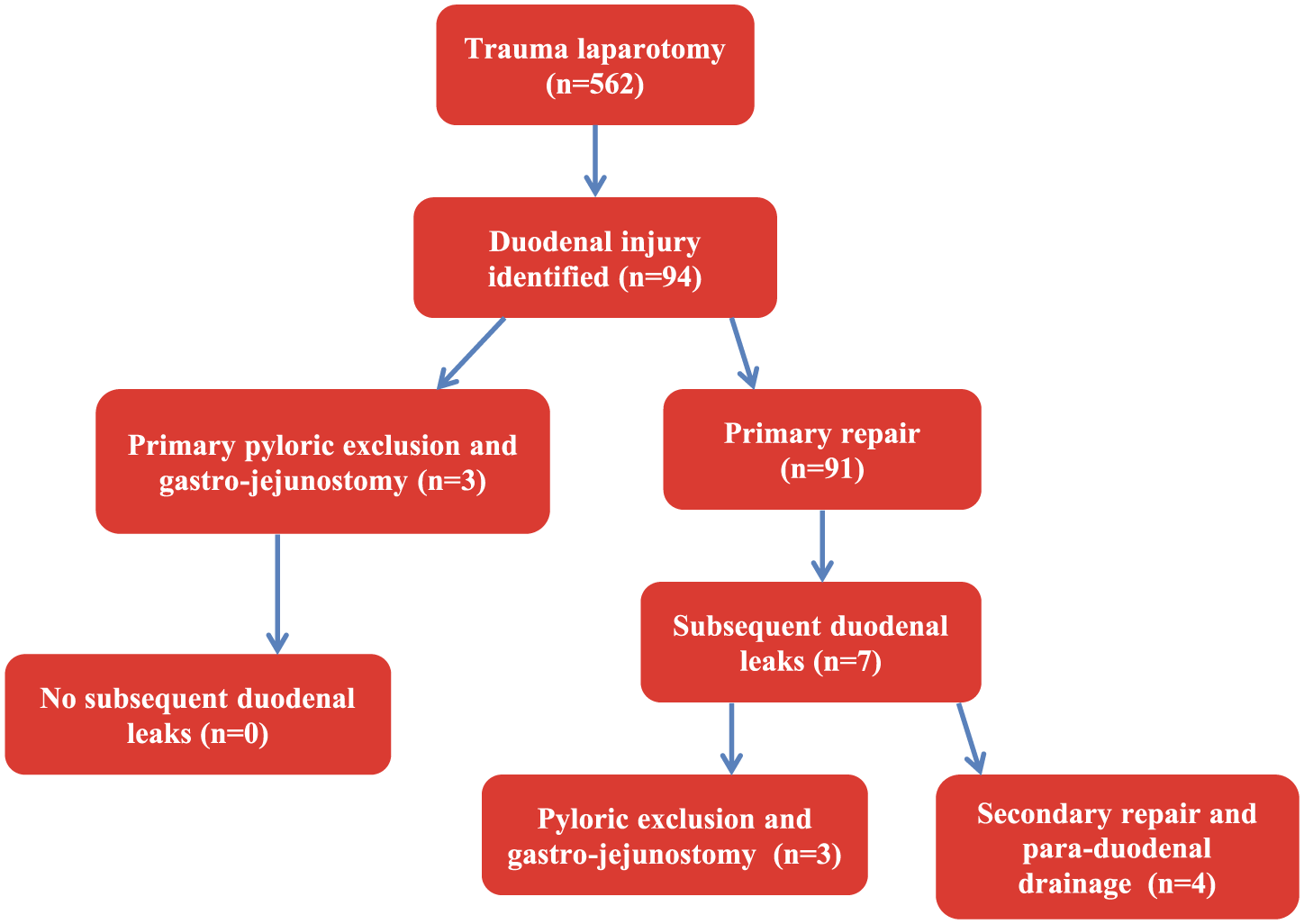
Flow diagram of patients. Note: only the primary repair arm is included in statistical analysis and tables. All patients in this series had a trauma laparotomy and those with discovered duodenal injury were included.
Within the duodenal group, the average age was 29 years (SD ±11). There were 79 males and 12 females. The mechanism of injury was blunt trauma in 32 (33%) and penetrating trauma in 59 (65%). There were 22 gunshot wound (GSW; 37%) and 37 stab wound (SW; 63%) injuries. Demographic data are displayed in Table 1.
Demographics of duodenal injury population dependent on mechanism of injury.
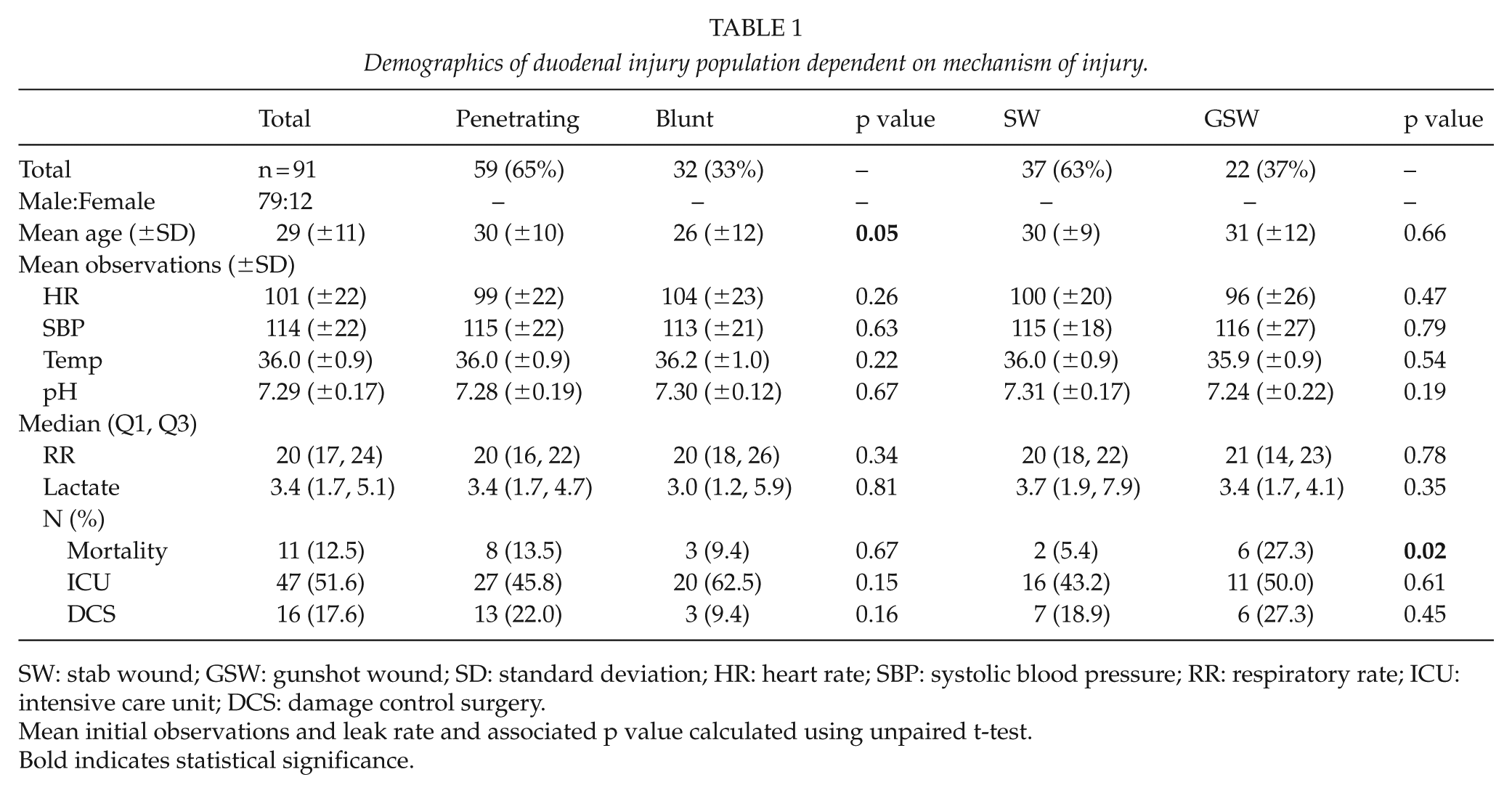
SW: stab wound; GSW: gunshot wound; SD: standard deviation; HR: heart rate; SBP: systolic blood pressure; RR: respiratory rate; ICU: intensive care unit; DCS: damage control surgery.
Mean initial observations and leak rate and associated p value calculated using unpaired t-test.
Bold indicates statistical significance.
The mean presenting observations are displayed in Table 1. There was no difference in respiratory rate, heart rate, systolic blood pressure, temperature, pH, lactate, ICU admission, damage control surgery (DCS), or leak rate between penetrating versus blunt, or GSW versus SW mechanisms. A significantly higher mortality for GSW versus SW is seen (27.3% vs 5.4%, p = 0.02). The associated injuries included small bowel (39), liver (32), stomach (19), pancreas (15), large bowel (15), kidney (9), inferior vena cava (8), gall bladder (7), diaphragm (5), ureter (4), intra-abdominal vascular injury (IAVI) (3), omentum (2), bladder (1), and spleen (1). The highest mortality was seen with IAVI at 66.7%.
Of the 91 patients who underwent a primary repair, a total of 7 (7.7%) developed a duodenal leak. Table 2 summarizes these leaks. The leaks were managed by PEG in three and by secondary repair and para-duodenal drainage in four. Five of the seven cases who developed a leak had undergone a primary DCS procedure and three of them died (Table 2). The operative interventions are illustrated in flow chart format in Fig. 2. There is a statistically significant difference in mortality in those with leak (75%) versus no leak (9.2%) (p value <0.01). This relationship, however, was not significant in a multivariate logistic regression model. This is a significant limitation and reflective of the lower power of the study.
Leak rates and p values calculated using Fisher exact test for ICU, mortality, and damage control surgery (DCS).
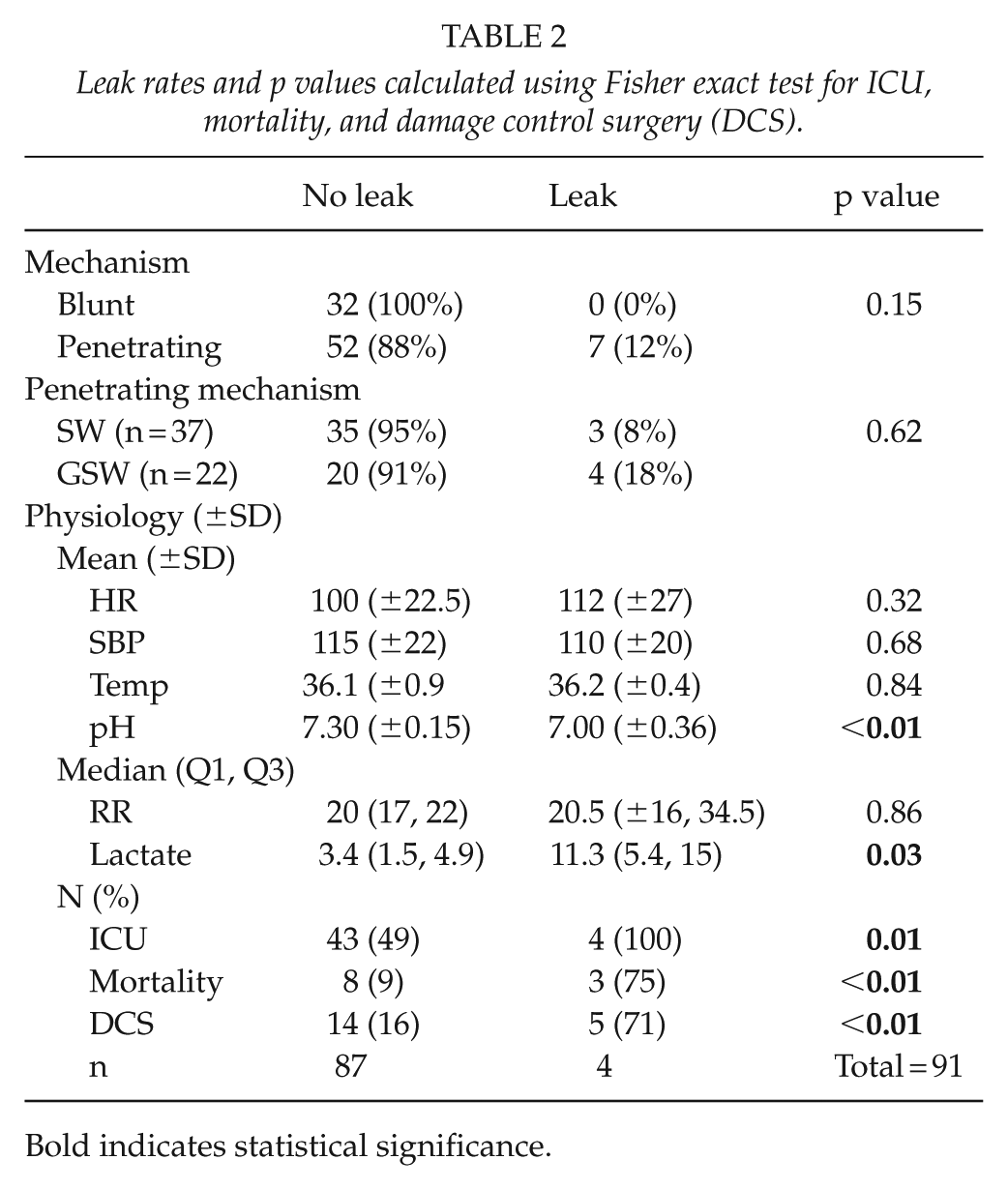
Bold indicates statistical significance.
Risk Factors for a Leak
To establish if admission physiology is predictive of subsequent duodenal leak, a comparison was made of all physiological variables for leak versus no leak (Table 2). The two physiological parameters most associated with subsequent leak were lactate and pH level. pH level was significantly lower in cases with subsequent leak (7.00 ± 0.36) versus those without leak (7.30 ± 0.15) (p < 0.01), and lactate levels were higher for those with leak (11.3 mmol/L) versus those without leak (3.4 mmol/L) (p = 0.03). There was a significantly higher ICU rate (100% vs 49%; p = 0.01), mortality (75% vs 9%; p < 0.01), and DCS (71% vs 16%; p < 0.01) for those with leak versus those without leak. Penetrating injuries had a higher leak rate than blunt (12% vs 0%), as did GSWs compared to SWs (18% vs 8%), although neither were statistically significant.
All duodenal injuries were graded according to the AAST grading (Table 3): AAST 1 (18), AAST 2 (64), and AAST 3 (9). There were no AAST injuries >3. The anatomical site of all the 91 duodenal injuries was D1 (31), D2 (12), D3 (37), and D4 (16) (total of 96, as in some, more than one segment was injured). Chi-square test revealed a significant difference in the leak rate between AAST-I (0%), AAST-II (1.6%), and AAST-3 (66.7%) grade injuries (p < 0.01). Six of seven (86%) patients who developed a leak had an AAST grade III injury and one a grade II injury. AAST grade III injuries also had significantly higher mortality rates (33.3%) than grade II (9.3%) and grade I (11.1%) injuries (p = 0.04).
Chi-square analysis of American Association for the Surgery of Trauma (AAST) grade with blunt (BT), stab wound (SW), gunshot wound (GSW), associated damage control surgery (DCS), mortality, and intensive care unit (ICU) rates.
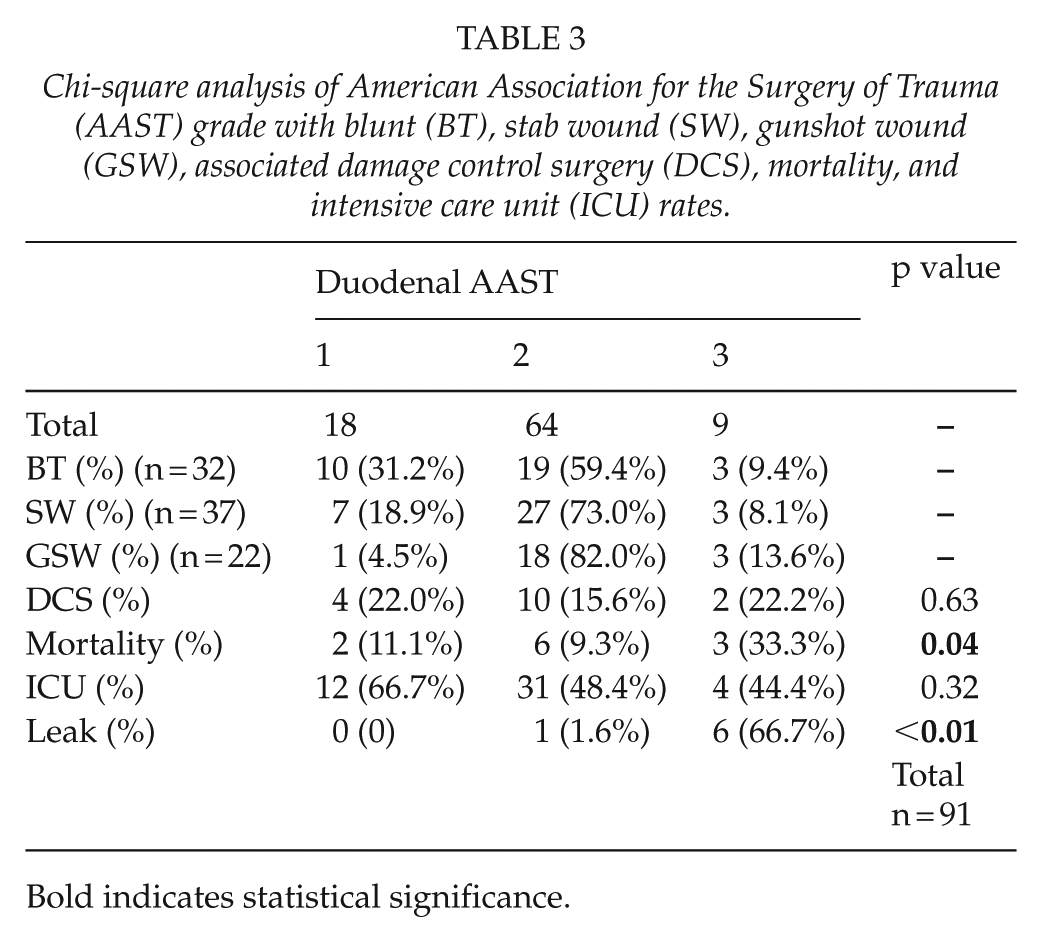
Bold indicates statistical significance.
Discussion
The management of duodenal trauma has undergone a paradigm shift over the last two decades. The initial concern was that the duodenum dealt with over 3 L of enzymatic fluid within a 24-h period and that this predisposed to breakdown of duodenal repairs. For this reason, a plethora of complex operative strategies were proposed to try and reduce the flow of enzyme-rich fluid over such a repair. These approaches included the use of gastric and duodenal tube drainage, attempts to diverticularize the duodenum (3), and pyloric exclusion (5, 6) in conjunction with a gastrojejunostomy. All these approaches tended to increase the complexity of the initial operation and of the subsequent postoperative management.
In our series, 91 of 94 underwent a simple, primary repair. A more complicated PEG was performed in three patients. These repairs were performed in patients not requiring DCS; all were blunt in mechanism, with no subsequent leak and all survived. In one of these cases, all four segments of the duodenum (D1–D4) were injured. This patient had an AAST-II duodenal injury, with no other associated visceral injuries. The other two cases of primary PEG were AAST grade III injuries, one of which had associated pancreatic injury.
There were a heterogeneous group of attending surgeons covering trauma calls during the earlier period of this study, and this may well have contributed to the use of complex repairs in these three patients. It may well have been feasible to manage these patients with a less complex primary procedure.
Over the last 10 years, the literature has increasingly favored simple primary repair over complex strategies designed to divert and reduce the flow of secretions over the repair (7 –11). The Cape Town group published a large series of duodenal injuries secondary to GSWs in which they used primary repair or resection and anastomosis almost exclusively (12). They reported a primary repair rate of 87%, and duodenal leak-related complications of 15%, with leak-related complications being independent of surgical technique. These authors pointed out that a confounding factor in the literature on duodenal injury is that most series have tended to include all duodenal injuries regardless of mechanism.
Our current data support this and the idea that it is naive to compare duodenal injuries without taking the mechanism of injury into account. In this current series, the duodenal leak rate following blunt and SW-related injury is much lower than following a GSW. Although we have included all duodenal injuries in our series regardless of mechanism, our leak rate of 7% is very much in keeping with those reported in the literature.
From our data, it would appear that duodenal leak is associated with GSWs, with the need for DCS and with higher grades of duodenal injury. In the subset of patients with grade III injury, the leak rate was in the order of 66%. The development of a duodenal leak is associated with an increased need for ICU stay and increased mortality. Mortality appears to be closely associated with combined injuries to the pancreas and duodenum (13), concomitant injuries to the stomach, the need for DCS, and with GSWs. While this does not mean that complex strategies to divert the flow of secretions are appropriate, it does suggest that the operating surgeon needs to have a heightened sense of vigilance in this cohort of patients in the postoperative period.
Conclusion
The trend toward simple primary repair of duodenal injuries away from more complex strategies appears to be justified. However, there appears to be a cohort of patients who are at risk for a duodenal leak following primary repair. Future work needs to focus on clarifying these risk factors and reviewing management strategies in this subset of patients.
Footnotes
Acknowledgements
Any original data that constituted this study can be accessed freely upon individual request from Dr Ross Weale at
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Victor Kong, Damian Clarke, John Bruce, Graant Laing and George Oosthuizen are all current ATLS instructors.
funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.