
Abstract
Background and Aims:
Michigan Hand Outcomes Questionnaire is a widely used patient-reported outcome measure in hand surgery. The aim of this study was to translate and validate the Michigan Hand Outcomes Questionnaire into Finnish for Finnish patients with hand problems following international standards and guidelines.
Material and Methods:
The original English Michigan Hand Outcomes Questionnaire was translated into Finnish. Altogether, 115 patients completed the Finnish Michigan Hand Outcomes Questionnaire, and reference outcomes: Disabilities of the Arm and Shoulder, EQ-5D 3L and pain intensity on a visual analog scale. Grip and key pinch forces were measured. After 1–2 weeks, 63 patients completed the Finnish Michigan Hand Outcomes Questionnaire the second time. The Michigan Hand Outcomes Questionnaire was analyzed for internal consistency, repeatability, correlations with the reference outcomes, and factor analysis.
Results:
Cronbach’s alpha ranged from 0.90 to 0.97 in all the Michigan Hand Outcomes Questionnaire subscales, showing high internal consistency. The intraclass correlation coefficient showed good to excellent test–retest reliability ranging from 0.66 to 0.91 in all the Michigan Hand Outcomes Questionnaire subscales. In factor analysis, the structure with six subscales was not confirmed. All the subscales correlated with Disabilities of the Arm and Shoulder score, and five subscales correlated with EQ-5D index.
Conclusion:
The Finnish version of the Michigan Hand Outcomes Questionnaire showed similar properties compared to the original English version and thus can be used as patient-reported outcome measure for Finnish patients with hand problems.
Keywords
Introduction
A variety of methods have been used to evaluate hand function and disability (1). Measurements of capacity such as sensitivity, grip and pinch strength, range of movement, and dexterity tests only partially reflect actual problems encountered in daily living in patients with hand problems or disabilities (2). To better measure the functional outcome of patients with hand disabilities, a growing number of patient-reported outcome (PRO) measures have been introduced. PRO measures, used to assess hand problems, should be specific to hand, valid, reliable, and reflect what is important to patients. Thus, disease-specific measures are needed to more accurately measure what is relevant to the patient with hand problems.
There are only a few upper extremity-specific PRO measures translated into Finnish: the Disabilities of the Arm and Shoulder (DASH), the Quick DASH, and the Patient-Rated Wrist Evaluation Questionnaire (3, 4). The Michigan Hand Outcomes Questionnaire (MHQ) is a measure developed at the University of Michigan in 1998 using psychometric principles capable of measuring health state domains in patients with hand disorders (5). It has proven to be reliable, valid, and responsive with patients suffering from a wide range of hand problems such as radius fracture, rheumatoid arthritis, carpal tunnel syndrome, and Dupuytren’s disease (6–9). It has been translated and validated into several languages (10–15). It is the only widely used PRO measure that assesses the right and left hand separately. Compared to DASH, which currently is the most widely used PRO measure with Finnish patients with hand problems, MHQ is more comprehensive reflecting not only hand function in everyday life but also subjective feelings and satisfaction. As such, we chose the MHQ for validation in Finnish.
The aim of this study was to translate and validate the MHQ into Finnish for Finnish patients with hand problems in accordance with international standards and guidelines (16).
Material and Methods
This study consisted of two phases: (a) translation of the MHQ into the Finnish language and (b) reliability and validity testing of the Finnish version of the MHQ. The official license and translation agreement from the Regents of the University of Michigan were obtained (academic license #8153). The study was approved by the local Ethics Committee.
Translation and Cross-Cultural Adaptation
The cross-cultural adaptation process was carried out following the instructions of the American Academy of Orthopedic Surgeons Outcome Committee (16). First, two surgery residents fluent in both Finnish and English independently translated the English version of the MHQ into Finnish and made a synthesis between the two forward translations. The reconciled version was back-translated into English by two bilingual translators with no medical background and no knowledge of the original MHQ instrument. A consensus committee composed of one hand surgeon, one physiatrist, one physiotherapist, and two surgery residents specializing in hand/orthopedic surgery reviewed the translations and commented on them. A pre-final version of the Finnish MHQ was made as a conclusion of the consensus committee. A total of 10 patients filled in the pre-final version, and we interviewed them to find if they had difficulties to understand any of the items. As they experienced no difficulties, linguistic professionals of Finnish language finalized the questionnaire.
Patients
Within 6 months in 2017, we recruited 115 participants with various hand problems treated in general orthopedic outpatient clinic. We only included adult participants whose first language was Finnish, had no cognitive dysfunction, and could read and write independently. Before the appointment, the participants filled in the Finnish version of the MHQ, the Finnish version of the DASH, the Finnish version of the EQ-5D 3L, and pain on a visual analog scale (VAS). Signed, informed consent was obtained from all the study participants. If both hands were affected, the worse one in the participants’ opinion was analyzed. Basic demographic information, such as handedness, occupation, and other illnesses, was collected. Grip and key pinch forces were measured using a Baseline hydraulic hand dynamometer and a pinch gauge (White Plains, NY, USA). A total of 63 participants filled in another copy of the Finnish MHQ and a short health survey 1–2 weeks after their visit to the hospital.
Instruments
The MHQ includes 37 core items. The items are divided into six subscales: overall hand function (five questions per hand), activities of daily living (ADLs, five questions per hand and seven additional questions) work performance (five questions), pain (five questions per hand), esthetics (four questions per hand), and patient satisfaction with hand function (six questions per hand). Each item is answered on a scale of 1–5. The total score in each six domains ranges from 0 to 100 and can be calculated separately for both hands; higher score indicating better hand function in all other subscales except pain, in which it indicates more intense pain.
We selected the DASH, the EQ-5D 3L and pain on a VAS scale as reference outcome measures. The DASH has 30 questions and additional work and sports/music scales to measure physical function in patients with upper extremity problems (17). The final outcome is scored from 0 to 100, a higher score indicating worse function.
The EQ-5D 3L is a standardized measure developed by the EuroQol Group (18) as a measure of health-related quality of life that can be used in a wide range of health conditions and treatments. It has five questions with three options. The health state can be converted to a single index varying from −0.011 to 1 in the Finnish version of EQ-5D 3L, lower score indicating poorer health-related quality of life. The EQ-5D 3L also has a separate unidimensional visual analog scale (EQ-VAS) measuring patient’s subjective general health (0–100, a higher score indicating better general health). Pain was measured on a 100-mm line (0 mm indicates no pain, 100 mm indicates worst possible pain) (19).
Statistics
The data are presented as means with standard deviation (SD), 95% confidence intervals (95% CI), as counts with percentages or as ranges. The statistical analysis was performed using R version 3.4.2.
Cronbach’s alpha was calculated for internal consistency. A threshold value of 0.80 was considered acceptable. Floor and ceiling values were calculated by dividing the number of maximum or minimum scores with the total number of patients who completed the questionnaire subscales.
The intraclass correlation coefficient (ICC) was calculated using a one-way random-effects model with absolute agreement to assess relative test–retest reliability. The ICC value was categorized according to the classification by Cicchetti et al. (20) as poor (<0.40), fair (0.40–0.59), good (0.60–0.74), or excellent (0.75–1.00). The coefficient of repeatability (CR) was used to calculate the expected maximum size of 95% of the absolute differences (absolute reliability) between paired observations. For the ICC and the CR, 95% CIs were calculated using bias-corrected and accelerated bootstrapping (1000 replications) techniques.
Spearman’s rank correlation coefficient was used to calculate correlation with the reference outcomes (DASH, EQ-5D, grip strength, key pinch strength, pain on a VAS). The following hypotheses were stated as follows: r ⩽ −0.70 or r ⩾ 0.7 shows large correlation; −0.7 < r ⩽ −0.5 or 0.7 < r ⩽ 0.5 shows moderate correlation; and −0.5 < r ⩽ −0.3 or 0.3 ⩾ r > 0.5 shows at least small correlation between the MHQ subscales and the different reference outcomes.
Linear regression analyses were applied to measure adjusted correlation with the reference outcomes. All regression models were standardized by age and gender. The correlation was assessed using regression Beta (β) coefficients. The β-value can be used to assess how strongly each predictor variable influences the criterion (dependent) variable, in this case the MHQ scores. Units of standard deviation were used to measure the β. Values 0.10, 0.30, and 0.50 represent small, moderate, and large correlations, respectively.
Exploratory factor analysis with Varimax rotation was used to investigate the construct validity of the different subscales of the MHQ. Confirmatory factor analysis (CFA) was performed to further investigate factor loading and verify or dismiss the findings from the exploratory analysis. A comparative fit index (CFI) and a Tucker–Lewis index (TLI) were calculated, and CFI ⩾ 0.9 and TLI ⩾ 0.9 were considered acceptable fits.
Results
The basic demographic features of the patients are presented in Table 1. Of the 115 participants, 48 were otherwise healthy. There were isolated cases of cancer, endocrinological disease, multiple sclerosis, and urological/gynecological illness. The most common educational level was high school/vocational school (66 participants).
Patients’ demographic and clinical characteristics.
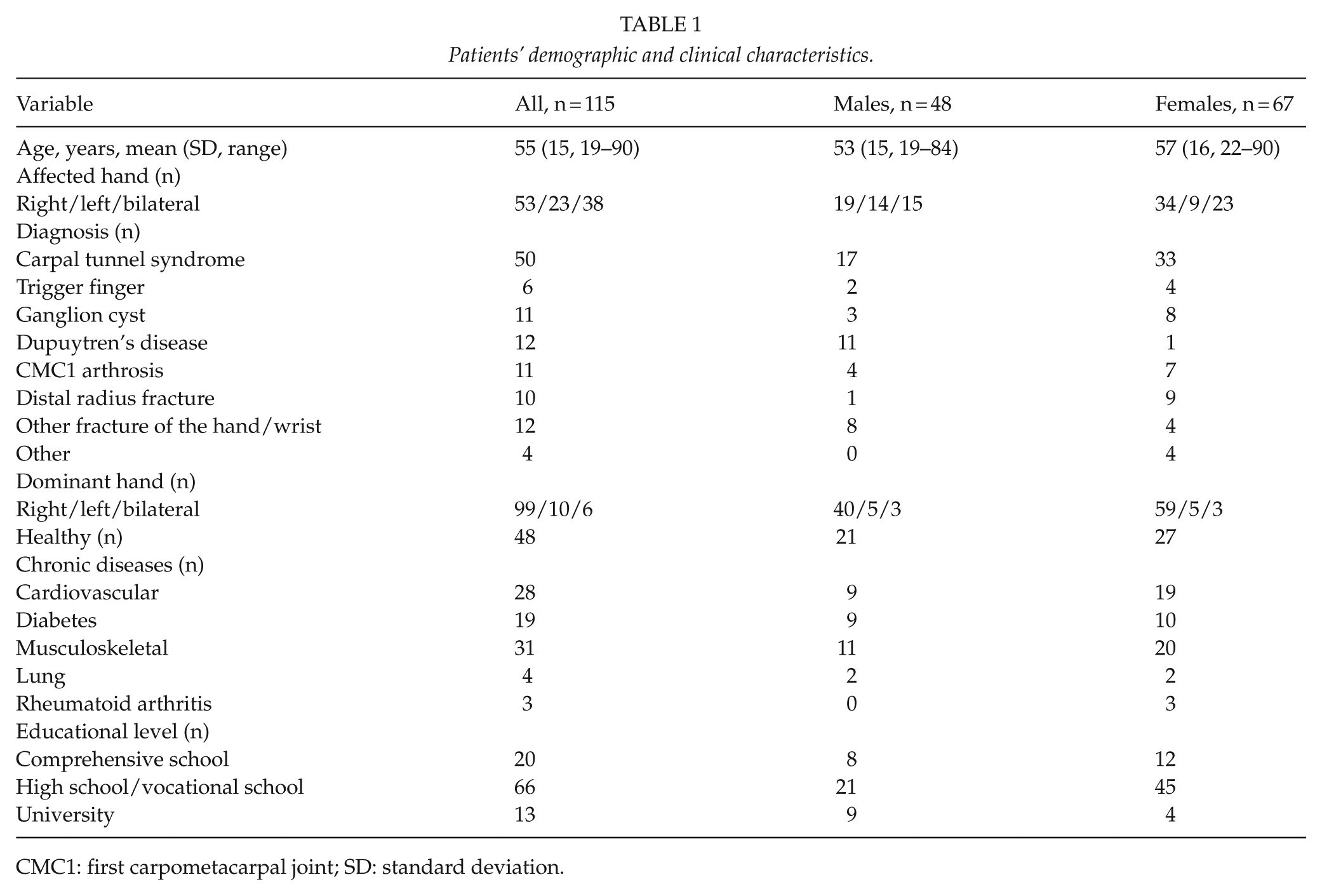
CMC1: first carpometacarpal joint; SD: standard deviation.
In the translation process, some minor issues were discussed: the word “please” was left out, “hand(s)/wrist(s)” was not translated in plural, and the options in the second subscale were not translated word-for-word to suite the Finnish language better.
The internal consistency of all the subscales was high (Table 2). Cronbach’s alpha ranged from 0.90 to 0.97 in all the MHQ subscales. There were no floor or ceiling values except for the aesthetics subscale (ceiling value 27.8%). The number of missing items was very small in every MHQ subscale (range: 0–4).
Internal consistency of the Finnish version of the MHQ.
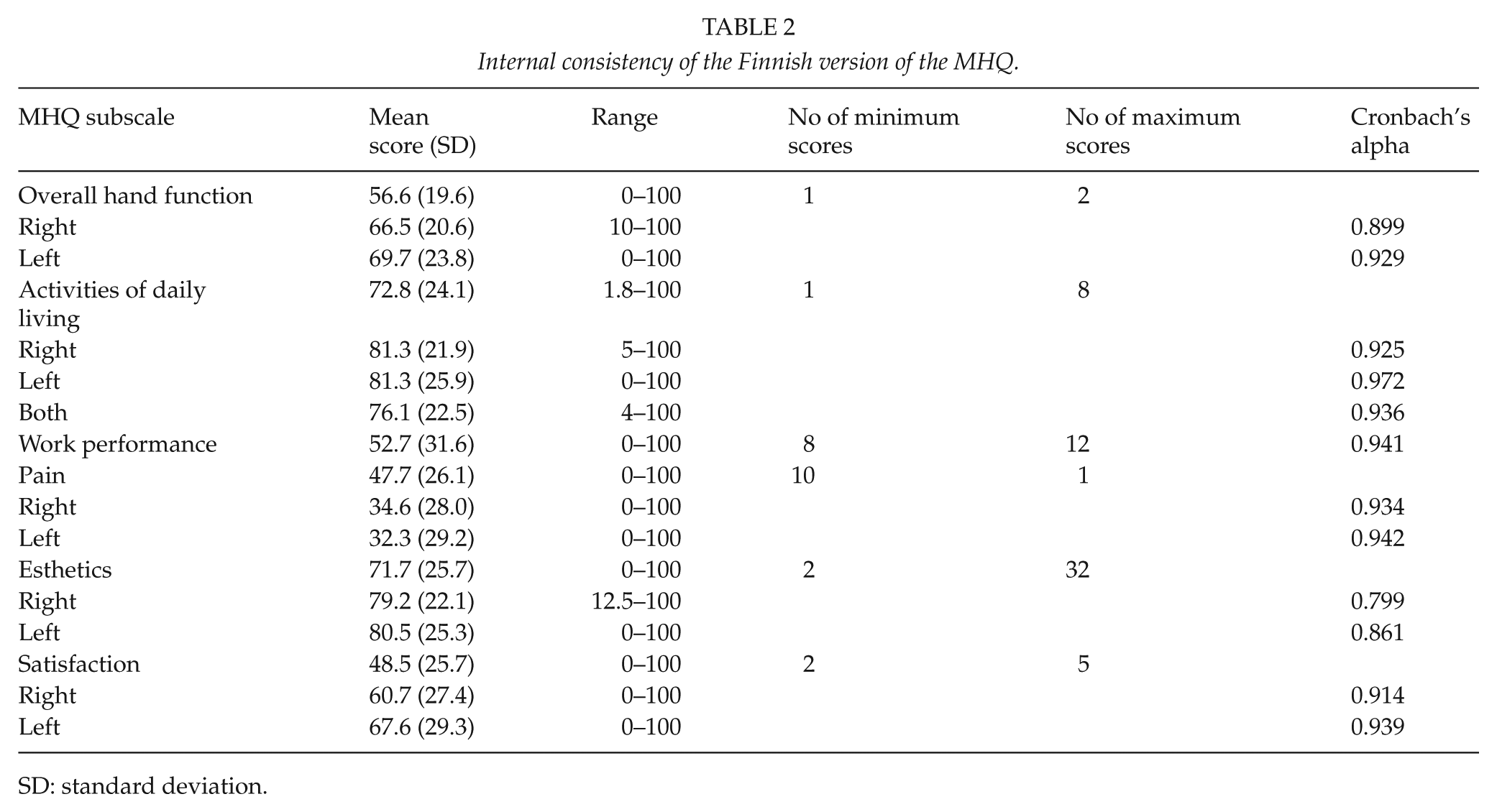
SD: standard deviation.
The ICC showed good to excellent test–retest reliability ranging from 0.66 to 0.91 in all the MHQ subscales. None of the patients reported significant changes in their health between the test and retest in the health survey obtained from all the study participants retested. The results are shown in Table 3.
Test–retest reliability of the Finnish version of the MHQ.
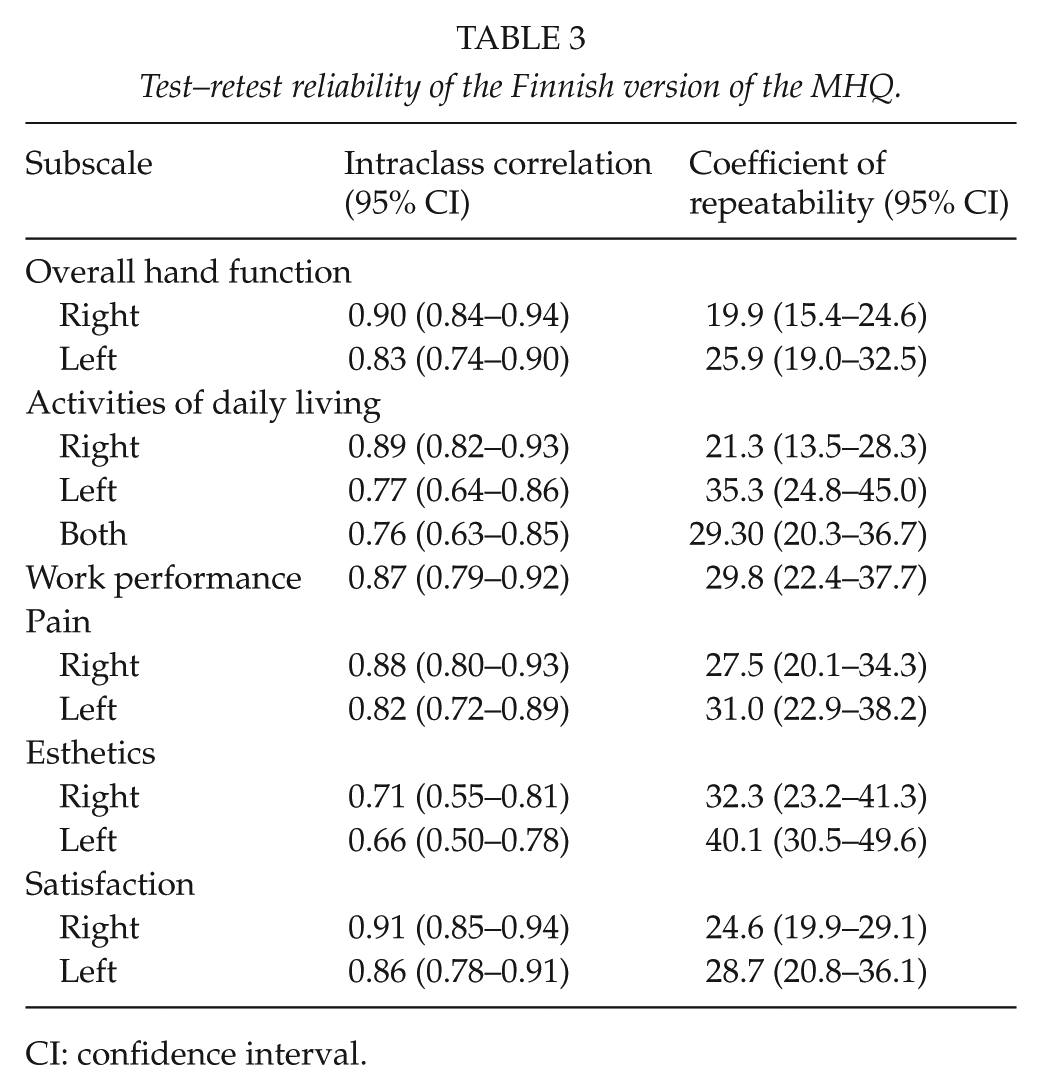
CI: confidence interval.
There were weak to moderate correlations between all the MHQ subscales and the key pinch and grip strengths of the injured/affected hand. With negative correlations, it is worthy of note that greater score in DASH disability/symptom scale and pain on VAS indicate poorer hand function and more pain. The MHQ subscales overall hand function, ADLs, work, and pain had a strong correlation with the DASH score. All the MHQ subscales, except the esthetics subscale, had at least a mild correlation with the EQ-5D index and the EQ-5D VAS score and pain intensity on a VAS. Table 4 shows the correlations between the MHQ subscales and all the reference outcomes. The correlations remained when standardized with age and gender, as shown in Fig. 1.
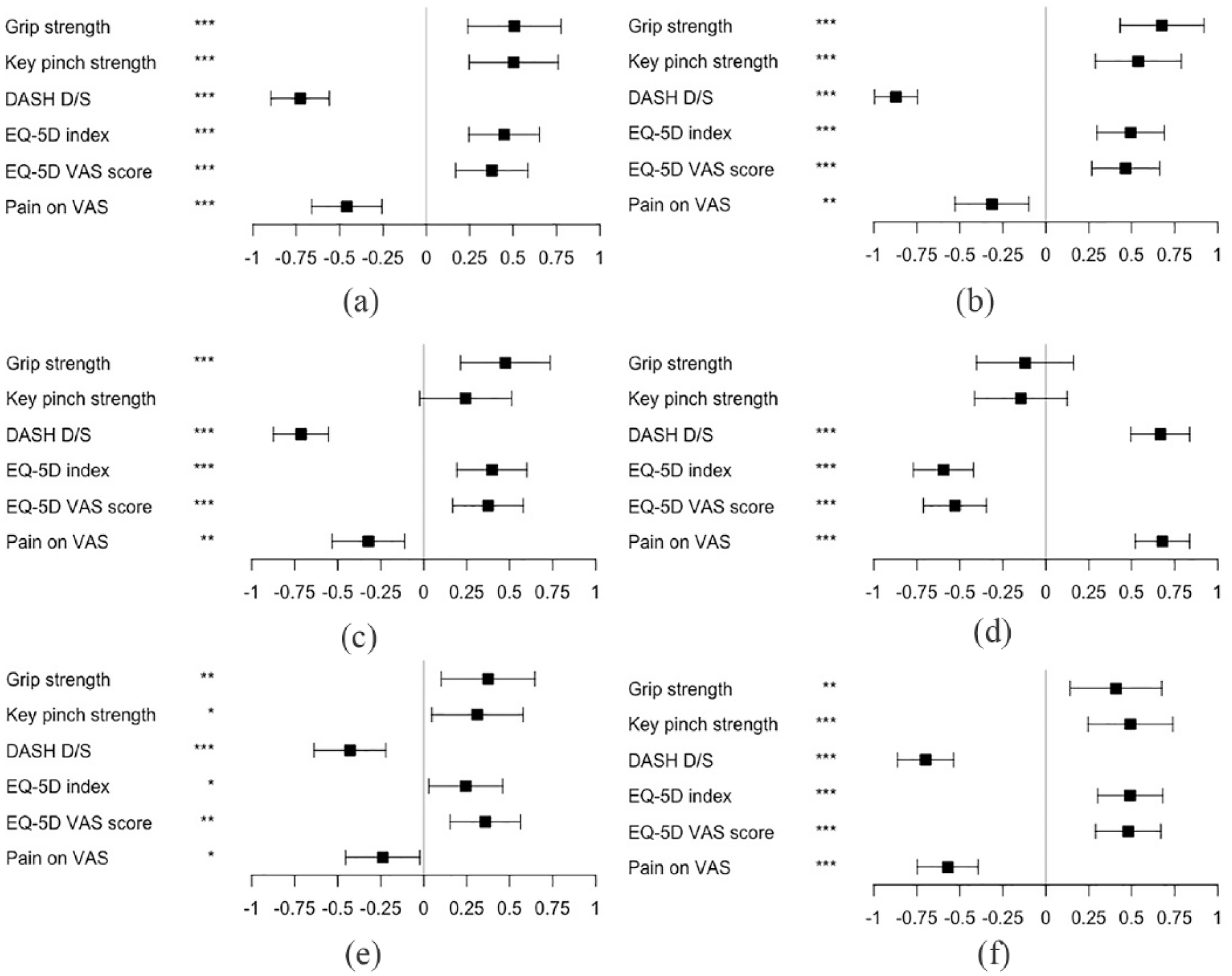
Age- and gender-standardized regression coefficients β of the Michigan Hand Outcomes Questionnaire subscales: (a) overall hand function, (b) activities of daily life, (c) work, (d) pain, (e) esthetics, and (f) satisfaction. The box plot indicates mean values and the whiskers represent 95% confidence intervals. Values on the x-axis represent correlation coefficients. *p < 0.05; **p < 0.01; ***p < 0.001.
Spearman’s correlation of the MHQ with grip strength, key pinch strength, dash score, EQ-5D index, EQ-5D score, and pain intensity on a VAS scale.
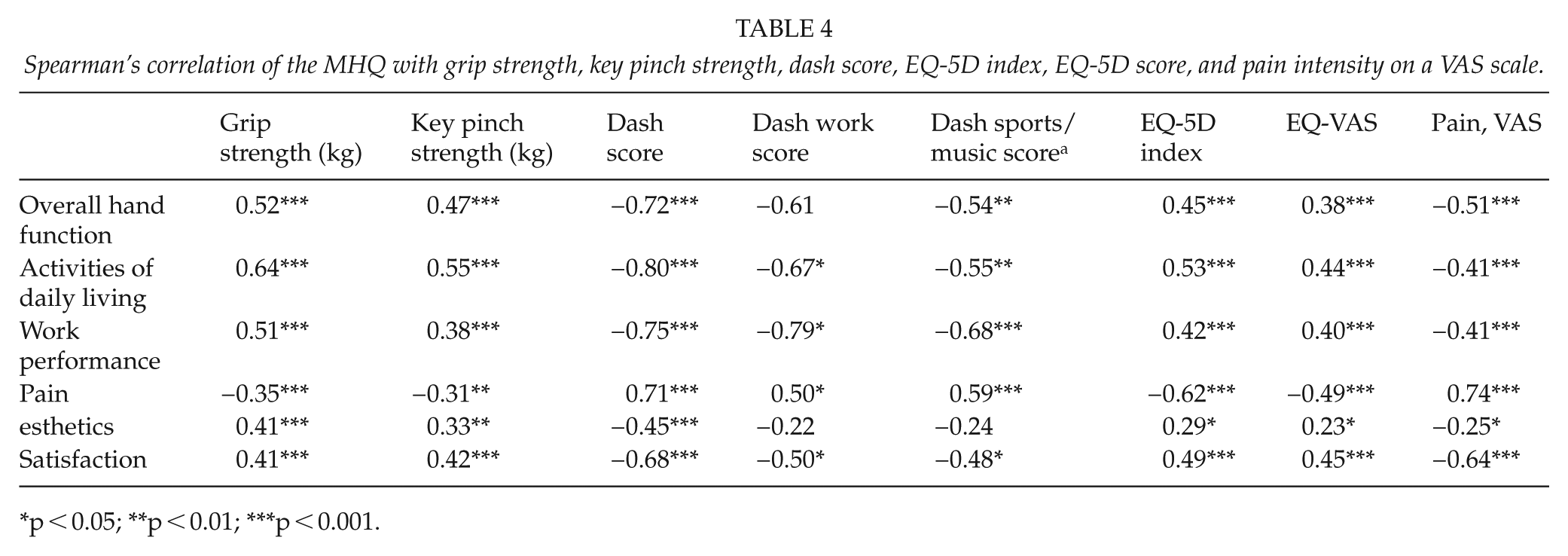
p < 0.05; **p < 0.01; ***p < 0.001.
In exploratory factor analysis, the MHQ loaded on four factors with the satisfaction subscale removed. Subscales overall hand function and ADLs loaded on the same factor. The factor loadings of the model are shown in the Supplementary material Table 5. This model showed the best fit in the CFA. However, the model fit was still considered not acceptable (CFI = 0.84 and TLI = 0.83).
Discussion
In our study, the Finnish version of the MHQ showed good validity and reliability when applied to a heterogeneous patient population who had hand problems. Psychometric properties were comparable to the original English version in relation to internal structure, correlations with reference outcome measures and factor analysis (5, 21).
No major problems were revealed in the translation and cultural adaptation. The participants found the questionnaire easy to answer. The completion rate of the Finnish MHQ was very high, with only 0–4 participants missing per each MHQ subscale, indicating excellent motivation of the participants.
Generally, cultural differences between the Finnish and US health systems, patient compensation, and other factors could be reflected in this kind of PRO measure. In Finland, the public healthcare system provides majority of all healthcare. In Finnish public healthcare, patients come from all socio-economical classes and represent the normal population very well. As healthcare systems are similar in other Scandinavian countries, we assume that our study reflects not only the Finnish system but also the whole of Scandinavia in the sense of cultural adaptation.
The participants are a representative sample of population of interest, as they were invited to the study while visiting the general orthopedic outpatient clinic in public healthcare. All the participants were examined by a surgeon or surgery resident, who informed about the study and trained the participants to perform the measurements properly.
Internal consistency was tested using Cronbach’s alpha. It ranged from 0.90 to 0.97 in all the MHQ subscales, indicating excellent internal consistency in all subscales. It tells that the items in the same subscale are correlated with each other and measuring the same construct. Our results on internal consistency of the MHQ subscales are similar to those in other language versions of the MHQ (10–14). There were no floor or ceiling values except for the esthetics subscale. The instrument has the ability to discriminate different health states in both ends of the spectrum apart from the esthetic outcome.
Test–retest reliability was tested with ICC and CR. ICC was excellent in 11 of 12 subscales, only the ICC of the esthetics subscale for the left hand was good. The esthetics subscale’s first question is the opposite of the other three questions of the subscale, so some of the study participants might have misunderstood it and given contradictory answers to that question. In addition, in the original English MHQ validation study, the ICC of the esthetics subscale for the left hand was the lowest of all MHQ subscales, but this was not discussed further (5). The CR represents a value in individual level, above which the change in the score is likely to be caused by true change in the health state and not by measurement error. The esthetics subscale had the highest CR, indicating poorer repeatability than those of the other subscales.
There were weak to moderate correlations between all the MHQ subscales and the key pinch and grip strengths (20). This implies that measurements of capacity such as grip and key pinch forces only partially reflect the disability patients suffer, as the maximal capacity is rarely needed in normal daily activities. Compared with other language versions of the MHQ, the correlations we found were slightly stronger (10–14). Four MHQ subscales had a strong correlation with the DASH score, with the ADLs subscale having the strongest correlation. The questions in DASH mainly represent capability to perform different tasks in daily living. Five MHQ subscales had at least mild correlation with the EQ-5D index and EQ-5D VAS score and pain on a VAS scale. This reflects the influence and importance of hand disabilities in their general health. The MHQ subscales ADLs and pain had the highest correlation with the reference outcome measures. This might be due to similar questions in those subscales of the MHQ and the reference outcome measures. The esthetics subscale had the lowest correlation. This implies that the reference outcomes to test the concurrent validity of the esthetics subscale may have been inappropriate for the purpose.
Explorative factor analysis (EFA) was performed in developing the original MHQ (5). CFA was done years later, and the MHQ structure of six subscales was not supported (22). In the EFA, the Finnish version of the MHQ did not load on six subscales. Multiple different models with two to five factors were tried out. None of these models met the criteria for an acceptable fit. Usually, items in the same subscale loaded on the same factor with each other, reflecting similarity among them. Next, we performed the EFA with a reduced MHQ. The subscales Overall hand function and Satisfaction consist of very similar items, so a model with the Satisfaction subscale removed was considered the best possible option logically. The EFA suggested that the optimal number of factors for this model was four. In the best model we created, the Satisfaction subscale was removed, and the rest of the items loaded on four factors. The subscales Overall hand function and ADLs loaded on the same factor. In Spearman’s correlation, these subscales had the highest correlation with each other among all the subscales of the MHQ (r = 0.76, p < 0.001). Our findings are similar to the CFA performed on the original MHQ, in which the MHQ structure of six subscales was not confirmed (21). To our knowledge, this is the first translation study to represent factor analysis for MHQ, further indicating the similarity of the Finnish MHQ to the original MHQ. The findings indicate that the MHQ describes the outcome in multiple different fields. Thus, it is recommended that the MHQ should not be single-scored, but scores calculated per subscale.
Compared with other PRO measures existing in Finnish already, the MHQ is more comprehensive, and the only instrument assessing both hands separately. Treating patients with hand problems often requires a multi-professional group and multiple appointments with hand therapists and surgeons.
To conclude, the Finnish version of the MHQ showed similar properties compared to the original English version, and thus can be used as PRO measure for Finnish patients with hand problems.
Supplemental Material
Supplemental_PDF – Supplemental material for Cross-Cultural Adaptation and Validation of the Finnish Version of the Michigan Hand Outcomes Questionnaire
Supplemental material, Supplemental_PDF for Cross-Cultural Adaptation and Validation of the Finnish Version of the Michigan Hand Outcomes Questionnaire by S. Hulkkonen, J. P. Repo, A. Häkkinen, J. Karppinen and J. Ryhänen in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors would like to thank the staff of Central Hospital of Länsi-Pohja, surgery outpatient clinic and statistician Paula Bergman of Helsinki University Hospital and University of Helsinki for their contribution to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethical Committee of the Northern Ostrobothnia Hospital District (ETTMK 34/2017).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
An informed consent was obtained from all the study participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.