
Abstract
Background and Aims:
Cardiovascular complications are common in hip fracture patients but the role of fracture type and operative method in these is unclear. This prospective cohort study aimed to evaluate the impact of fracture- and operative characteristics on perioperative cardiovascular complications and prognosis in unselected hip fracture patients.
Material and Methods:
During a 7-month trial registration period, a population of 197 consecutive hip fracture patients (median age 84 years) diagnosed with femoral neck or pertrochanteric fracture was formed. The exclusion criteria were patient refusal, subtrochanteric fracture, or death preoperatively. Pre- and postoperative troponin T (TnT) elevation, perioperative N-terminal fragment of pro-B-type natriuretic peptide (NT-proBNP) level, perioperative cardiovascular adverse events, and all-cause 30-day and 2- and 5-year mortalities were studied.
Results:
Femoral neck fracture was independently associated with preoperative myocardial injury witnessed by TnT elevation (HR 2.95, 95% confidence interval 1.21–7.19, p = 0.018). The fracture type, surgery delay, or operative method were not significantly associated with NT-proBNP levels, cardiovascular adverse event diagnoses, or prognosis. Cardiovascular adverse events were clinically diagnosed in 28 (14%) participants, and these had a higher mortality compared to participants without such diagnosis (at 30 days, 32% vs 5%; 2 years, 71% vs 31%; and 5 years, 86% vs 59%; p < 0.001).
Conclusion:
While the femoral neck fracture independently predicts preoperative cardiovascular morbidity, the operative method does not affect perioperative cardiovascular complications or the prognosis, and it may be selected by the treating clinician based on other criteria.
Keywords
Introduction
Perioperative myocardial injury is a common, yet often asymptomatic, complication after noncardiac surgery (1). It independently predicts higher mortality of operative patients (2).
During the past years, it has been observed that patients with a hip fracture often suffer from clinically silent perioperative myocardial injury witnessed by an elevated troponin level (3–7). However, in hip fracture patients, half of the troponin elevations appear already before the surgery, suggesting that the fracture itself might be the reason for the myocardial injury (8). It has also been established that hip fracture patients have high levels of N-terminal fragment of pro-B-type natriuretic peptide (NT-proBNP), which typically demonstrates heart failure (9). As has been demonstrated by us and others, perioperative troponin T (TnT) and NT-proBNP elevation are independent predictors of mortality in patients with hip fracture (4, 5, 7–10). Thus far, the impact of fracture- and operative characteristics in these biomarkers have been unclear. We sought to assess the role of the fracture type and operative methods and delays in the development of perioperative cardiovascular complications and the prognosis in hip fracture patients.
Material and Methods
The study is part of a wider ongoing protocol targeted on assessing thrombotic and bleeding complications of invasive procedures in Western Finland (3, 11). All the consecutive patients who were diagnosed with a hip fracture at Turku University Hospital between 19 October 2009 and 19 May 2010 were enrolled. Inclusion criteria were admittance to the traumatology ward due to a hip fracture and approval by the patient or next of kin. Informed written consent was obtained from every patient, or in the case of impaired cognition from the next of kin, after a full explanation of the study protocol. The primary exclusion criterion was patient refusal (n = 1), resulting in 200 hip fracture patients. The primary fracture classification was established by the clinician at hospital admission, and the classification was re-evaluated by one traumatologist in January 2016 in line with the current AO/OTA (American Orthopaedic Trauma Association) and Garden classifications. The latest classifications were used in the analysis, and patients with subtrochanteric fracture (n = 2), and death prior to surgery (n = 1) were excluded, resulting in a final study group of 197 patients.
On admission, the patients were assigned an American Society of Anesthesiologists (ASA) physical status classification by an on-call anesthesiologist. The patients’ usual medications (excluding diuretics) were given on the day of the operation and continued throughout the hospital stay. A lumbar epidural catheter was inserted for pain control at hospital admission. Doses of a mixture of a local anesthetic (bupivacaine, Chirocaine, Baxter Health Care, Castlebar, Ireland) and an opiate (fentanyl, B. Braun Melsungen AG, Ruby, Spain) were given via the catheter until the second postoperative day. A low molecular weight heparin for deep venous thrombosis prophylaxis was started as soon as possible. The patients were operated preferably under spinal anesthesia with isobaric bupivacaine. In the event of hypotension (blood pressure < 100/60 mm Hg) rapid fluid challenge, vasopressors, and atropine were used as appropriate. Significant operative blood loss (leading to a hemoglobin level less than 90 g/L), was treated with red blood cell transfusion. The operation was performed as soon as possible depending on overcrowding in the operative theaters. The surgery delay was counted from the time the patient was registered at the emergency room of the study hospital. If the patient was sent from an affiliate hospital where the primary diagnosis had already been made, the registration time at the first hospital was considered. If the patient was already in the study hospital during the injury, the delay was assessed from the moment of fracture diagnosis. The choice of operative method was made according to the fracture and patient characteristics by the treating traumatologist. In general, hemiarthroplasty and cannulated screws were the choice for femoral neck fractures, and cannulated screws were more commonly chosen for younger patients, while trochanteric- and long intramedullary nails were used for pertrochanteric fractures. There was only one exception to this, since one patient with a fracture classified as pertrochanteric was operated with cannulated screws.
Blinded determination of TnT levels and an electrocardiogram (ECG) recording were performed on arrival, preoperatively, and on the first and second postoperative mornings, and a measurement of the NT-proBNP level at least once during the hospital stay, between hospital admission and the fourth postoperative day. These results were available to the treating traumatologist if clinical suspicion of a perioperative cardiovascular event arose based on the patients’ clinical condition. Computed tomography (CT) of the head was performed when an acute intracranial process was suspected based on symptoms or clinical picture. A chest x-ray was taken of each patient at arrival, and later when clinically indicated. If the clinical findings or symptoms suggested a perioperative cardiovascular event, a cardiologist, internist, or neurologist was consulted for diagnostics and treatment. Information on patients’ medical history was retrieved from the medical records. The patients were followed until January 2016. Primary outcome measures were pre-, post-, and perioperative TnT elevation; perioperative NT-proBNP elevation; and clinical cardiovascular complication diagnoses and secondary outcome measures were 30 days, and 2- and 5-year mortalities. Follow-up data were accessible for all participants.
An electrochemiluminescence immunoassay (ECLIA) on a Modular E170 automatic analyzer (Roche Diagnostics GmbH, Mannheim, Germany) was used to determine the TnT and NT-proBNP levels. Upper reference limits for NT-proBNP and TnT levels were ⩾50 ng/L and ⩾0.03 µg/L, respectively. In cases where multiple NT-proBNP measurements were performed perioperatively, only the highest level was used in the analyses.
Statistics
Data are presented as frequency and percentage, mean values and standard deviation (SD), or median and interquartile range [IQR] or range, as appropriate. The Kolmogorov–Smirnov and Shapiro–Wilk tests were used for testing for normal distribution. The Fisher exact test and Chi-square test were used for comparison of the differences between categorical variables. The Student t test, Mann–Whitney U test, one-way analysis of variance (ANOVA), and Kruskall–Wallis test were used for comparison of continuous variables in groups as appropriate. When univariate analysis showed association of variables, a logistic multivariable regression analysis was performed to identify independent association of variables, and all variables with p-values <0.1 were included. Survival analysis was performed using Kaplan–Meier log rank test. Differences were considered significant if the null hypothesis could be rejected at the 0.05 probability level. All analyses were performed using SPSS software version 22 and 23 (SPSS Inc., Chicago, Illinois).
Results
Population Characteristics
The median [IQR] age of the participants was 84 [11] years and 66% were female. The median [IQR] ASA class was 3 [1]. A history of any cardiovascular disease was known in 142 (72%) of the participants (Table 1).
Comparison of the different hip fracture types. Data are presented in count (%) or median [IQR].
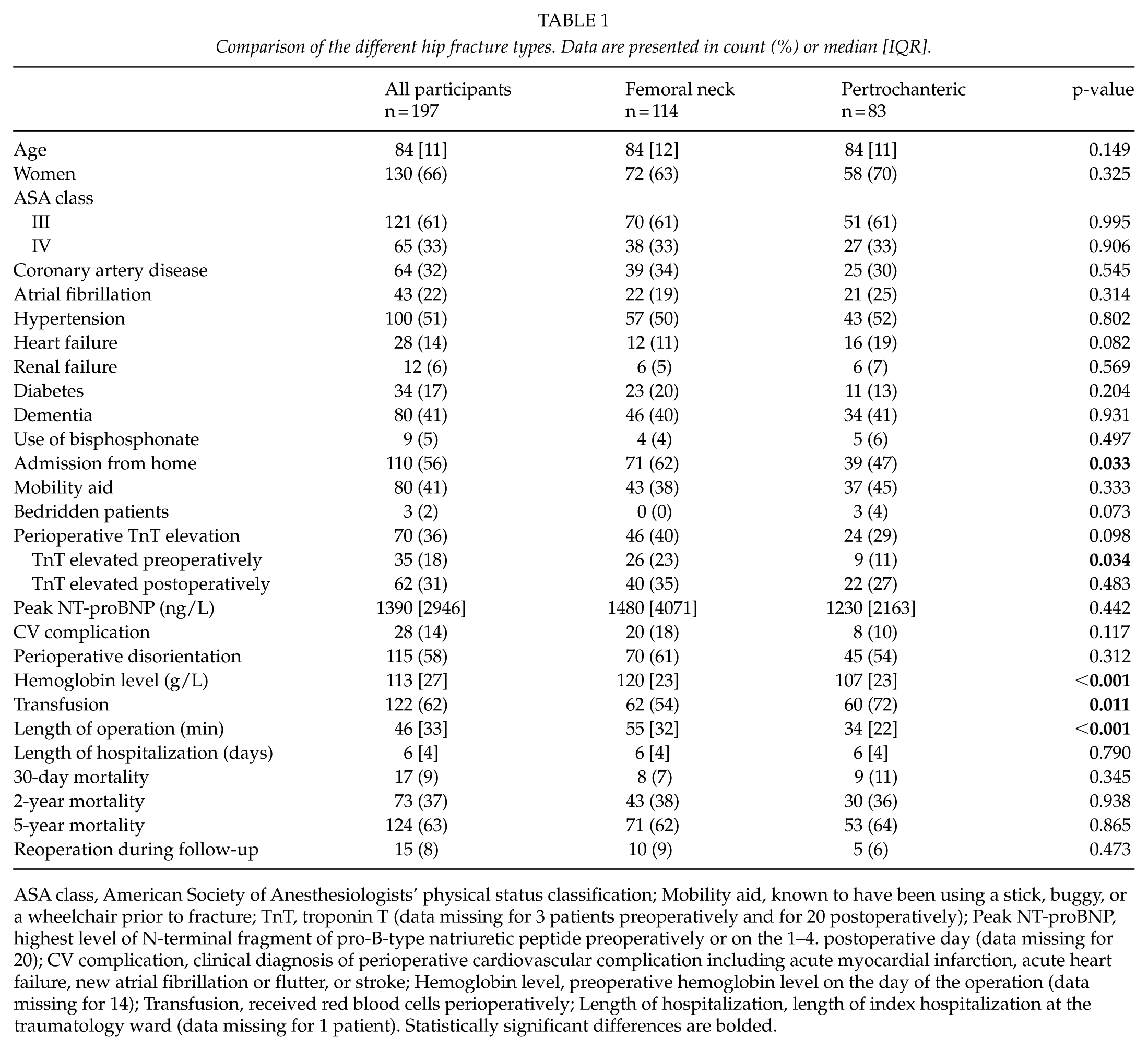
ASA class, American Society of Anesthesiologists’ physical status classification; Mobility aid, known to have been using a stick, buggy, or a wheelchair prior to fracture; TnT, troponin T (data missing for 3 patients preoperatively and for 20 postoperatively); Peak NT-proBNP, highest level of N-terminal fragment of pro-B-type natriuretic peptide preoperatively or on the 1–4. postoperative day (data missing for 20); CV complication, clinical diagnosis of perioperative cardiovascular complication including acute myocardial infarction, acute heart failure, new atrial fibrillation or flutter, or stroke; Hemoglobin level, preoperative hemoglobin level on the day of the operation (data missing for 14); Transfusion, received red blood cells perioperatively; Length of hospitalization, length of index hospitalization at the traumatology ward (data missing for 1 patient). Statistically significant differences are bolded.
Fracture and Operative Characteristics
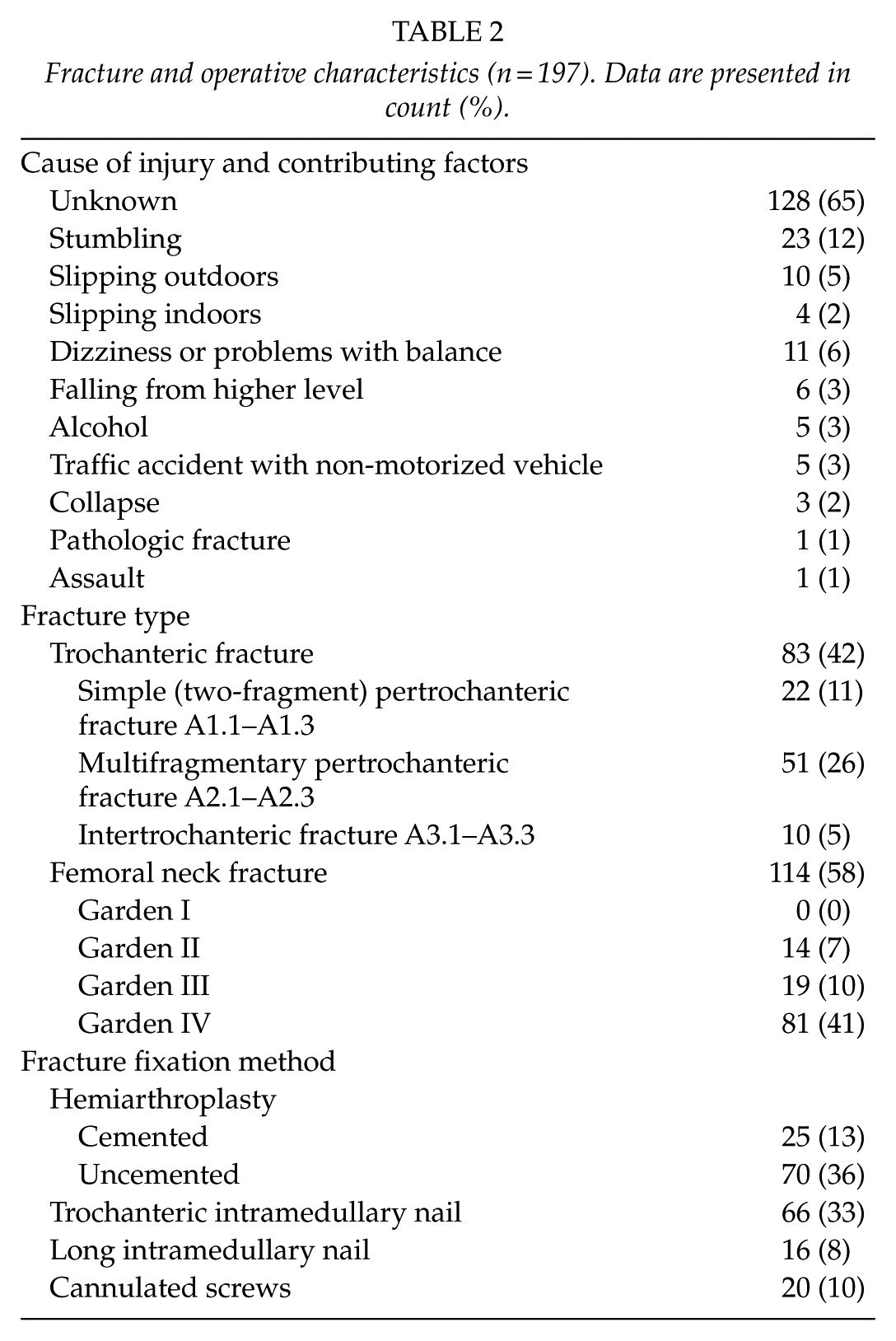
Of the femoral fractures, 114 (58%) were fractures of the neck and 83 (42%) were pertrochanteric. An accompanying fractured upper limb was diagnosed in 10 (5%) participants, and pneumothorax in 1 (0.5%). The operation was performed within 24 h for 97 (49%) participants, within 24–48 h for 78 (40%), and after 48 h for 22 (11%) participants. Of the participants with a surgery delay exceeding 48 h, 64% were men, compared to 30% of participants with a shorter surgery delay (p = 0.002); however, no statistically significant difference was seen between the participants with different surgery delays concerning median age, ASA class, cardiovascular diseases, renal failure, dementia, fracture classification, TnT elevation, hemoglobin level, or chest x-ray findings on admission (data not shown). The median [IQR] length of the operation was 46 [33] min. The operative treatment methods were cemented (n = 25) and uncemented (n = 70) hemiarthroplasty, cannulated screws (n = 20), trochanteric (n = 66), and long (n = 16) intramedullary nail (Table 2).
Fracture and operative characteristics (n = 197). Data are presented in count (%).
The median length of hospitalization on the traumatology ward was 6 [4] days, without significant difference between the different fracture types or operative methods (Tables 1 and 3). Participants with a fractured femoral neck had a significantly higher preoperative hemoglobin level, required less blood transfusions, and arrived more often from home than participants with a pertrochanteric fracture (Table 1). Cemented hemiarthroplasty was more commonly chosen for participants who had been using a mobility aid prior to fracture, while cannulated screws were most commonly used for those arriving from home (Table 3).
Comparison of the different operative methods. Data are presented in count (%), median [IQR], or mean (± SD).
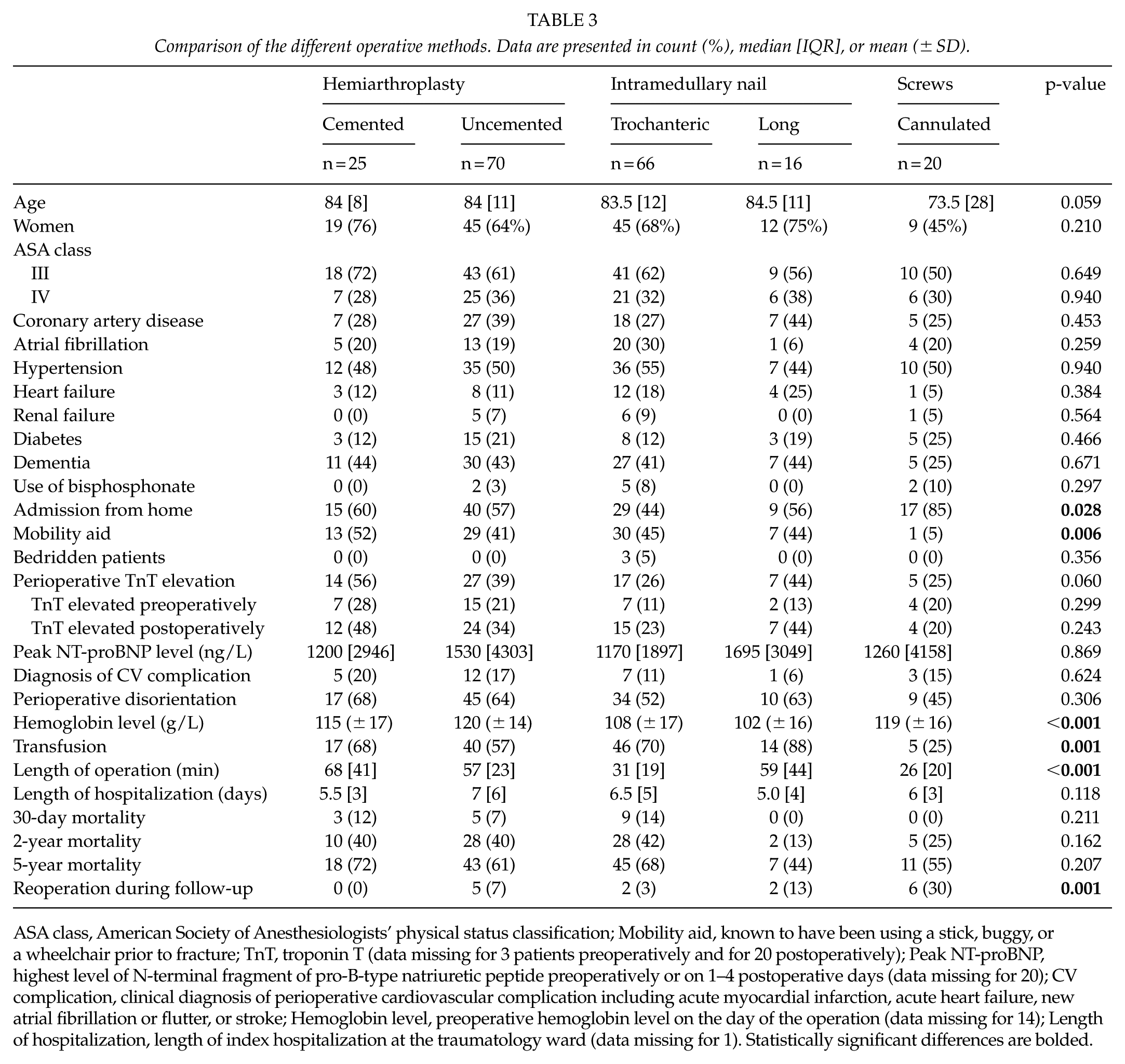
ASA class, American Society of Anesthesiologists’ physical status classification; Mobility aid, known to have been using a stick, buggy, or a wheelchair prior to fracture; TnT, troponin T (data missing for 3 patients preoperatively and for 20 postoperatively); Peak NT-proBNP, highest level of N-terminal fragment of pro-B-type natriuretic peptide preoperatively or on 1–4 postoperative days (data missing for 20); CV complication, clinical diagnosis of perioperative cardiovascular complication including acute myocardial infarction, acute heart failure, new atrial fibrillation or flutter, or stroke; Hemoglobin level, preoperative hemoglobin level on the day of the operation (data missing for 14); Length of hospitalization, length of index hospitalization at the traumatology ward (data missing for 1). Statistically significant differences are bolded.
Cardiovascular Events During Hospitalization
During hospitalization, 28 (14%) participants were diagnosed with some perioperative cardiovascular complication. Acute myocardial infarction, acute decompensated heart failure, or both were diagnosed in 25 (13%) participants, a new-onset atrial fibrillation or flutter in 4 (2%), and a stroke in 1 (1%), but no deep venous thrombosis or pulmonary embolism were diagnosed. A cardiologist, internist, or anesthesiologist was consulted for 31 (16%) participants. Preoperative TnT elevation was more common in participants with a femoral neck fracture (Table 1), but the possible dislocation of the fracture did not further affect the incidence (23% in dislocated vs 24% in non-dislocated femoral neck fractures, p = 1.00). Multivariable regression analysis, with age, preoperative ASA class, coronary artery disease, prior coronary revascularization, and renal failure showed that having a fractured neck of the femur hazard ratio (HR) 2.95, 95% confidence interval (CI) 1.21–7.19, p = 0.018), increasing age (HR 1.06, 95% CI 1.01–1.11, p = 0.03), and renal failure (HR 5.89, 95% CI 1.44–24.1, p = 0.014) independently predicted preoperative TnT elevation. Although postoperative TnT elevation and diagnosis of cardiovascular complications were numerically more common in participants with a femoral neck rather than a pertrochanteric fracture, and in cemented hemiarthroplasty than when using the other operative methods, these differences were not statistically significant (Tables 1 and 3). There were no differences in peak NT-proBNP levels between the fracture types or operative methods (Tables 1 and 3). Even when participants with the same fracture type were analyzed in their own separate analysis, there was no statistically significant difference in TnT elevations, NT-proBNP levels, or diagnoses of perioperative cardiovascular complications between the different operative methods (data not shown). Cardiovascular events were diagnosed in 13% of the participants operated within 48 h and in 23% operated after 48 h, but the difference was not statistically significant (23/175 vs 5/22, p = 0.211). Incidence of TnT elevation and median peak NT-proBNP levels were similar in participants who were operated within 48 h or later (35% vs 36%, p = 0.931, and 1330 (IQR 2945) vs 1760 (3452) ng/L, p = 0.591, respectively).
Short-Term Prognosis
The 30 day mortality was 7% for participants who were operated within 24 h, 9% for participants who were operated in 24–48 h, and 14% for those who were operated more than 48 h later, but the difference was not statistically significant (p = 0.602). There was no statistically significant difference in the short-term mortalities between different fracture types or operative methods (Tables 1 and 3), even when patients with femoral neck and pertrochanteric fracture were viewed in separate analyses (data not shown). Participants who were diagnosed with a cardiovascular complication had a 30-day mortality of 32% compared to 5% for participants with no diagnosis of cardiovascular complication (9/28 vs 8/169, p < 0.001).
Long-Term Prognosis
At the 2-year follow-up, 73 (37%) participants had died and at the 5 year, 124 (63%); the mortalities did not differ between the fracture types (Table 1). In addition, the outcome was not affected by the operative method choice (Table 3), even when femoral neck and pertrochanteric fractures were analyzed separately (data not shown). Participants with a diagnosis of perioperative cardiovascular complication had higher mortality compared to the other participants (at 2 years, 71% vs 31% and at 5 years, 86% vs 59%, p < 0.001). There was no statistically significant difference in long-term mortalities between participants with a surgery delay of less or more than 48 h (at 2 years, 36% vs 45%, p = 0.280, and at 5 years, 63% vs 64%, p = 0.610).
Discussion
This was the first study to evaluate the independent association of hip fracture type with preoperative myocardial injury assessed by troponin elevation. Although participants with a femoral neck fracture arrived more frequently from home, had a higher preoperative hemoglobin level, and required less blood transfusions than participants with a pertrochanteric fracture, a femoral neck fracture was shown to independently predict preoperative TnT elevation. This might be connected with the anatomical differences of femoral neck and pertrochanteric fractures. Also other laboratory parameters have been shown to differ between patients with these two hip fracture types (12). The differences in postoperative TnT levels were modest and did not reach statistical significance. To the best of our knowledge, only two groups have previously compared troponin elevation in femoral neck and pertrochanteric fractures, the first of these observed no differences in peri- and postoperative TnT levels and the second observed numerically greater amounts of postoperative TnT in femoral neck fracture patients, but did not report whether this finding was statistically significant (12, 13). This was the first study to assess the impact of hip fracture type on NT-proBNP levels, and no significant differences where observed.
The operative method did not significantly affect perioperative TnT or NT-proBNP levels or cardiovascular complication diagnoses, although perioperative TnT elevation was observed in more than half of participants treated with cemented hemiarthroplasty compared to 25%–44% of the participants operated with some other operative method. While no earlier studies have evaluated the potential impact of the operative method on perioperative NT-proBNP levels, two earlier studies have compared the effect of different operative methods on troponin levels. The first of these does not present the results but explains that they did not find differences in perioperative TnT levels between the surgical methods. However, the second found a numerically, but not statistically significant, greater amount of postoperative TnT elevation when choosing hemiarthroplasty compared to gamma nail (5, 14).
Cemented and uncemented hemiarthroplasty have been widely compared to each other in the treatment of dislocated femoral neck fractures, but mostly without any findings of significant differences in the postoperative cardiovascular complication diagnoses (15–18). However, only one of these earlier studies, with a small population of 130 participants, conducted routine troponin measurements, and the results of these have not been reported (15). In the present study, almost half of the participants treated with cemented hemiarthroplasty had a TnT elevation after the operation, compared to a third of those treated with uncemented hemiarthroplasty, but this result was not statistically significant. The possibility of a bone cement implantation syndrome in the use of cemented hemiarthroplasty is well known and possible symptoms reviewed in the literature include hypotension, hypoxia, cardiac arrhythmias, and cardiac arrest (19). Although a previous study on patients with dislocated femoral neck fracture has reported blood pressure and blood saturation drops during or immediately after cementation suggesting fat embolism (20), no patient was suspected of having an embolism in the current study. The surgery delay did not significantly affect the occurrence of TnT or NT-proBNP elevation or cardiovascular complication diagnoses; in contrast however, the findings of an earlier study showed an independent association between a longer surgery delay and postoperative cardiovascular complications (21).
Earlier hip fracture studies have found a 1-month mortality of 5%–10% (22–25), and the current study is in line with these results with 9% of participants dying during the first month. The long-term mortality was also high with approximately two-thirds of participants dying during the 5-year follow-up. This study is consistent with the findings of those previous studies concluding that the fracture or fixation type does not affect mortality (12, 15, 17, 22, 26–28). An earlier study has suggested that in addition to the prognosis, causes of death are also similar for patients with femoral neck and pertrochanteric fracture (12, 26). However, the causes of death were beyond the scope of the current study.
There has been conflict in earlier studies as regards the role of surgery delay in the prognosis. Many studies conclude that short-term mortality is higher in patients with a longer surgery delay (22, 24, 29, 30). However, patients who have a longer surgery delay tended to have more comorbidities (22, 29), and when surgery delay exceeded 24 h, the majority of patients had an active medical problem or were pending medical clearance (24, 25). Some studies have suggested that a surgery delay exceeding 1 or 2 days is not an independent predictor of mortality when these comorbidities have been considered (24, 30). Contrary to this, another study concludes that surgery delay is associated with greater mortality even after adjustment for comorbidities (29). In the current study, where male gender was overrepresented in the group of participants operated more than 48 h after hospital admission, participants with a longer surgery delay seemed to have higher 30-day and 2-year mortalities; nevertheless, this was not statistically significant. This result may, however, be biased due to the small sample sizes, since the surgery delay was over 48 h for only 22 participants.
Perioperative cardiovascular complications are common in hip fracture patients. Those participants who were diagnosed with perioperative cardiovascular complication had the poorest short-term outcome and the difference persisted throughout the whole 5-year-long follow-up. Since the perioperative cardiovascular complications were not affected by operative choices, the focus should be on screening for complications and treating them. Although TnT elevations indicating myocardial injury were common, traumatologists who were blinded to these study-based laboratory results infrequently consulted cardiologists or internists for heart problems.
Even though this study is restricted by a limited population, it was the first to show an independent association between preoperative TnT elevation and femoral neck fractures. However, further studies with larger study populations are needed, especially to determine the role of surgery delay and cemented hemiarthroplasty in the development of postoperative cardiovascular complications. The results of this observational study should be viewed as hypothesis generating. Ideally, NT-proBNP measurements should be obtained both pre- and postoperatively. Decisions were at the discretion of the treating traumatologists and the physicians and the clinical variables not assessed in this study may account for these decisions. The strengths of this study are the prospective setting of the study, the inclusion of all consecutive patients treated for a femoral neck or pertrochanteric fracture without exclusion criteria, and the complete follow-up data of all 197 participants.
In conclusion, perioperative cardiovascular complications are important in assessing the prognosis of patients with a hip fracture. While fracture characteristics play a role in preoperative cardiovascular morbidity, the operative method does not seem to have a major impact on perioperative cardiovascular complications or the prognosis. Therefore, the operative method may be chosen by the treating clinician based on other criteria.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Finnish Foundation for Cardiovascular Research, Helsinki, Finland.
Informed Consent
All study participants gave their informed written consent.