
Abstract
Background and Aims:
No previous studies have analyzed the connection between total hip replacement and induced abortion. We evaluated the nationwide induced abortion rates among women with and without total hip replacement.
Materials and Methods:
Data for this cohort study were gathered from national registers from 1987 to 2007. All fertile-aged (15–44 years old) females who had undergone primary total hip replacement in Finland were selected. The total hip replacement patient group comprised 1713 women and the reference group 5148 women. Information on all pregnancies for both groups before and after total hip replacement/index date was gathered from the medical birth register and the register of induced abortion. Logistic regression model was used to analyze the adjusted odds ratio for induced abortion. Adjustment was made for age at induced abortion, parity, previous induced abortions, previous deliveries, and marital status.
Results:
Women had higher induced abortion proportions after total hip replacement (17.9%) compared with women before total hip replacement (14.1%) and the referents (13.9%), but the differences were not statistically significant. Women in the total hip replacement patient group had significantly more induced abortions after total hip replacement due to maternal health issues (14.7%) compared with the referents (2.7%), p = 0.003. Patients in the total hip replacement group were not more likely to have their pregnancy ending in induced abortion than the women in the reference group (odds ratio 1.32, 95% confidence interval 0.89–1.96, p = 0.17). However, in the adjusted analysis, there was a trend for higher risk for pregnancy to end in induced abortion in the total hip replacement group in relation to the reference group (adjusted odds ratio 1.50 (confidence interval 0.99–2.28, p = 0.05).
Conclusion:
The total hip replacement patient group had higher, but statistically insignificant, induced abortion proportions compared with the reference group before and after the operation. After total hip replacement, the patients were not more likely to have a pregnancy ending in induced abortion. This finding remained statistically insignificant after adjusting with possible confounders.
Keywords
Introduction
Total hip replacement (THR) is a highly effective surgical procedure (1) that results in major improvements in the patients’ quality of life, pain, sleep, physical ability, and sexual function (2–4). The main indications for THR in patients under 30 years of age are rheumatoid arthritis (RA) (36%) and avascular necrosis (23%) (5), whereas indications for overall primary THR for all ages in Finland are primary osteoarthritis (78%) and RA (7%) (6).
In Finland, the total number of primary THR per year has grown from slightly over 5000 in 2000 to over 10,000 in 2017 (7). Of these, almost 60% of patients were female. Every year, almost 500 THRs are carried out on patients under 50. The number of patients in this age group has grown slightly since 2003 (7). In 2007, the incidence of THR for young patients (30–49 years old) was 39 per 100,000 person years and the incidences increased slightly from 1980 to 2007 (8).
A few studies with small sample sizes and regional data have investigated the effects of THR on pregnancies and deliveries and vice versa. According to these previous studies, THR does not seem to be a contraindication for pregnancy or delivery (9, 10). Moreover, neither pregnancy nor delivery decrease implant survival after THR (9–13). Women who have undergone THR seem to have lower fertility rates (14). One reason for the lower fertility rates might be that women have concerns about pregnancy and delivery after THR (9). These findings could therefore implicate reproductive problems or an increased induced abortion (IA) rate.
The rate of IA in Finland was 8.7 per 1000 fertile-aged women (15–49 years old) in 2013 (15), which was the lowest rate in the Nordic countries. In 2013, the IA rate for the Nordic countries was 13.5/1000 fertile-aged women. Although rates of IA have been stable in the Nordic countries for much of the 21st century, a small decline has been seen during the last 2 years (15). Overall, the worldwide rate of IA has been stable (29/1000 fertile-aged women in 2003 versus 28/1000 in 2008) (16). The main indications for IA in Finland are social reasons (91.8%), fetal defects (3.4%), female aged over 40 at the start of the pregnancy (3.1%), and female aged under 17 at the start of the pregnancy (2.7%) (15).
Women with a lower socioeconomic status (SES) have a higher risk for IA compared with those of a higher SES (17). A Brazilian study estimated that women over 40 years of age or unmarried have more IAs than any other group (18). Furthermore, a previous IA may lead to repeat abortion (19, 20). In addition, a short time between delivery and the next pregnancy increases the risk for abortion (21).
To the best of our knowledge, no previous studies have evaluated the relationship between THR and IA. The aim of the present study is therefore to investigate whether women with THR have a higher risk of IA compared with a reference group without THR at the national level.
Materials and Methods
In this nationwide register-based retrospective cohort study, data were obtained from five national health registers: the Finnish Arthroplasty Register (FAR), the Register of Induced Abortion (RIA), the Finnish Population Information System, the National Medical Birth Register (MBR), and the register of medical reimbursement (RMR) due to chronic diseases maintained by the Social Insurance Institution of Finland.
The THR patient group consisted of all fertile-aged women (15–44 years old) who had undergone their first primary THR in Finland between 1987 and 2007. The THR patients were identified from the FAR that is maintained by Finnish National Institute for Health and Welfare (THL). The FAR contains information on all hip and knee prostheses carried out in Finland. All the information in the FAR has been collected prospectively. The current (2017) completeness of the register is 95% for primary THR and it matches well with data from the Finnish Hospital Discharge Register (7).
For every THR patient, three reference persons without THR were obtained from the Population Information System maintained by the Finnish Population Register Center. These reference persons were individually matched to THR patients by age, place of residence, and mother tongue. Information on the number of biological children born to the patients and the referents before the end of 2007 was also gathered from the population information system. The index date for the referents was the day their matching patient underwent THR.
Information on IAs from 1987 to 2007 was obtained from the RIA. The RIA contains information on abortion rates and indications, as well as background information on females who have undergone IA. The overall coverage of the RIA is high, as is the validity of most of the variables. However, some problems have been reported with the coverage of SES and gestational age (22).
Information on pregnancies from 1987 to 2007 was obtained from the MBR. The register contains information on all births after gestational week 22 + 0 or birth weight over 500 g. The MBR also contains information on maternal background characteristics, pregnancy history, pregnancy and delivery diagnoses, and neonatal data up to 7 days after birth. The MBR has high coverage and good quality of data, which has improved over time (23).
The RMR contains information on reimbursable costs due to chronic diseases. For reimbursement, a medical certificate issued by a certified doctor is required. Information on RA was gathered for study population and participants with no record of RA reimbursement in the RMR were classified as not having the disease.
The start of the abortion follow-up was the 1st of January 1987 or the day the patient turned 15 years old, whichever occurred last. The endpoints for the abortion follow-up were the 31st of December 2007, or the date of the patients’ 45th birthday, emigration, or death, whichever occurred first.
Ethics
All the data were linked with the unique identification number assigned to all residents of Finland. In accordance with Finnish regulations, no informed written consent was required because participants in the study were not contacted individually. Permission for the data use was granted by the register holders. Permission number: THL/599/5.05.00/2010.
Statistics
The logistic regression model was used to evaluate whether THR increased the risk of IA. Both unadjusted and adjusted odds ratios (ORs) with 95% confidence interval (CI) were calculated. In the adjusted model, the following potential confounders or modifiers were adjusted for age at time of abortion, parity, previous IAs, previous deliveries, and marital status.
Comparisons between the groups both before and after the THR/index date on abortion rates as well as on indications for abortions were carried out. Chi-square test or Fischer’s exact test was used to analyze categorized variables between the THR patient group and the reference group. The CI for the difference between two proportions (later as proportion difference = PD) was used to evaluate the intergroup differences before THR and after THR in the THR patient group and before and after index date in the reference group. Statistical analyses were conducted with IBM SPSS for windows version 22 software. P-values under 0.05 were considered statistically significant.
Results
The total number of female participants in this study was 6861. Among these, a total of 6608 pregnancies and 885 (13.4%) IAs occurred. The THR patient group comprised 1713 women, with 1274 pregnancies and 187 (14.7%) IAs. Of these, 199 pregnancies and 35 (17.9%) IAs occurred after the THR. The reference group comprised 5148 women with 5334 pregnancies and 698 (13.1%) IAs. Of these, 1308 pregnancies and 182 (13.9%) IAs occurred after the index date. Mean age at the beginning of the abortion follow-up was 27.4 years and mean age at the THR/index date was 37.3 years in both groups. The basic demographics of the patients and the referents are presented in Table 1.
Background characteristics of study population.
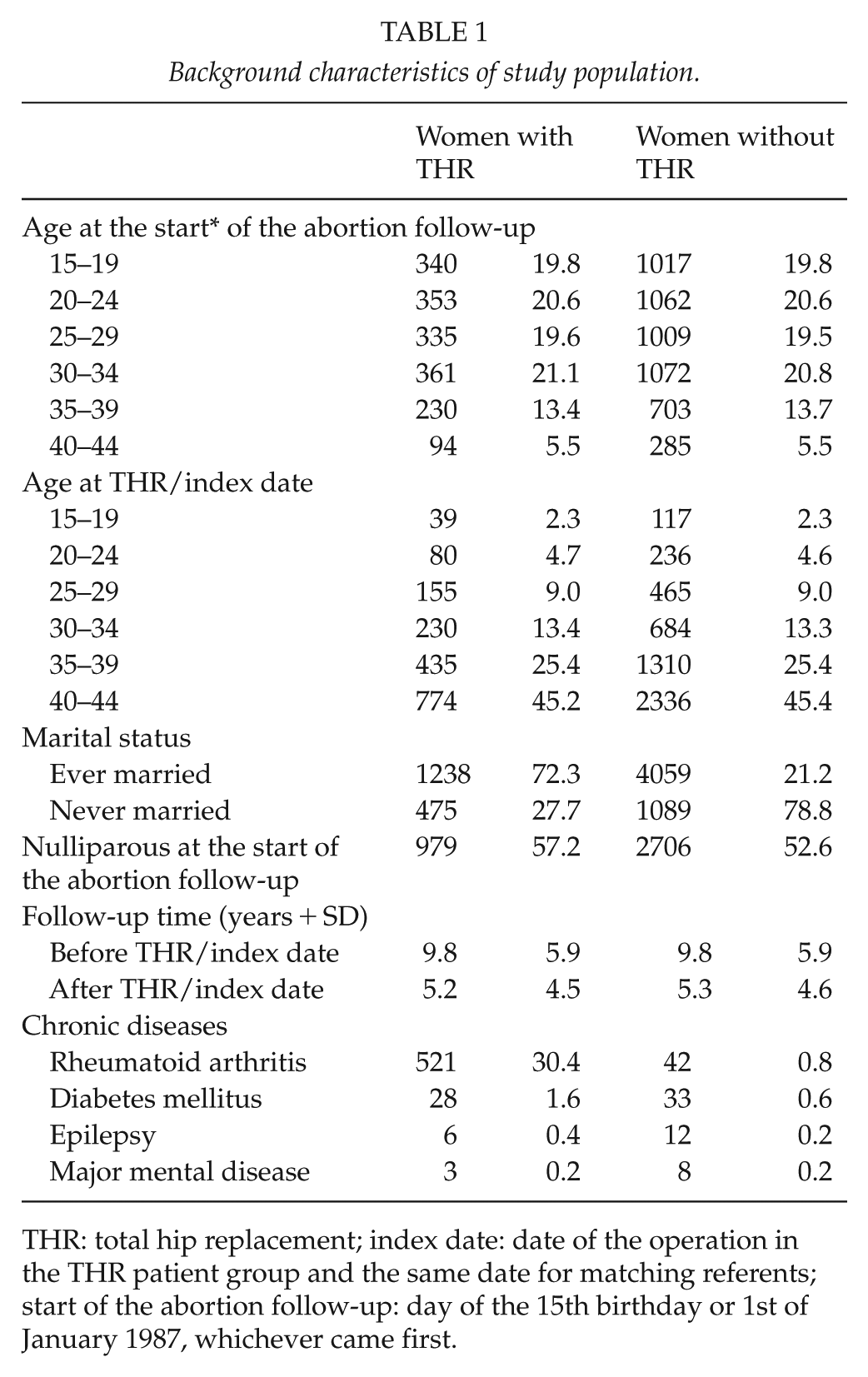
THR: total hip replacement; index date: date of the operation in the THR patient group and the same date for matching referents; start of the abortion follow-up: day of the 15th birthday or 1st of January 1987, whichever came first.
In the patient group, the abortion rate was 9.0/1000 person years (pyrs) before the THR and 3.9/1000 pyrs after the THR. In the reference group, the rates were 10.2/1000 pyrs before the index date and 6.6/1000 pyrs after the index date. In the patient group, abortion rates were 17/100 births before the index date and 21/100 births after the index date. In the reference group, the abortion rate was 15/100 births before the index date and 16/100 births after the index date.
IA indications varied slightly between the women with and without THR (Table 2). More abortions were carried out due to maternal health reasons in the THR patient group. The rate of the first abortion was higher after THR compared with rates before the THR and the reference group. Interestingly, married women seemed to have fewer abortions after THR than unmarried women.
Total number of abortions for women with and without total hip replacement (THR) before and after THR/index date in Finland between 1987 and 2007.
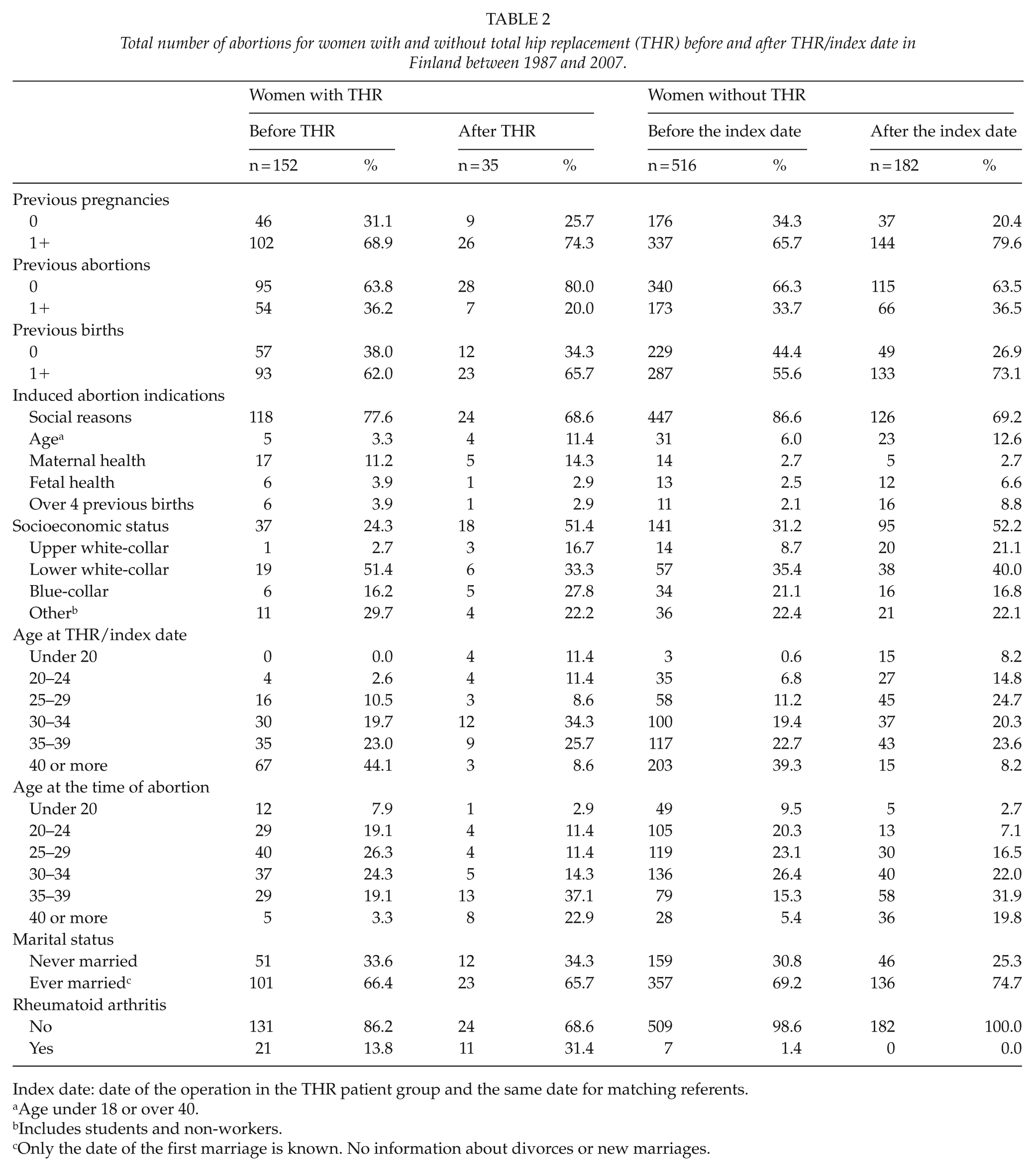
Index date: date of the operation in the THR patient group and the same date for matching referents.
Age under 18 or over 40.
Includes students and non-workers.
Only the date of the first marriage is known. No information about divorces or new marriages.
Before the THR/index date, there were 152 (14.1%) IAs among the THR patient group and 516 (12.8%) in the reference group, p = 0.25. After the THR/index date, the THR patient group had 35 (17.9%) IAs and the reference group 182 (13.9%), p = 0.17. In the THR patient group, number of IAs varied from 152 (14.1%) before the THR to 35 (17.9%) after THR (PD = 3.5, CI −1.7 to 9.7). In the reference group, number of IAs before the index date were 516 (12.8%) and 182 after the index date (13.9%), PD = 1.1, CI −1.0 to 3.3. Median time after the THR to IA was 4.0 (range 0.1–20.4) years in the THR patient group and before the THR, the median time from IA to THR was 8.4 years (0.2–20.5). Median times in the reference group were 3.9 years (0.0–19.7) after the index date and 7.1 years (0.0–20.7) before the index date.
Women in the THR patient group were more likely to undergo their first IA after THR rather than before THR, or women in the reference group. Women in the youngest and the oldest age group had higher IA proportions than those in the moderate age groups (Table 3).
Proportions of pregnancies ending in induced abortion with 95% confidence interval (CI) among women with and without total hip replacement (THR) before and after THR/index date in Finland between 1987 and 2007.
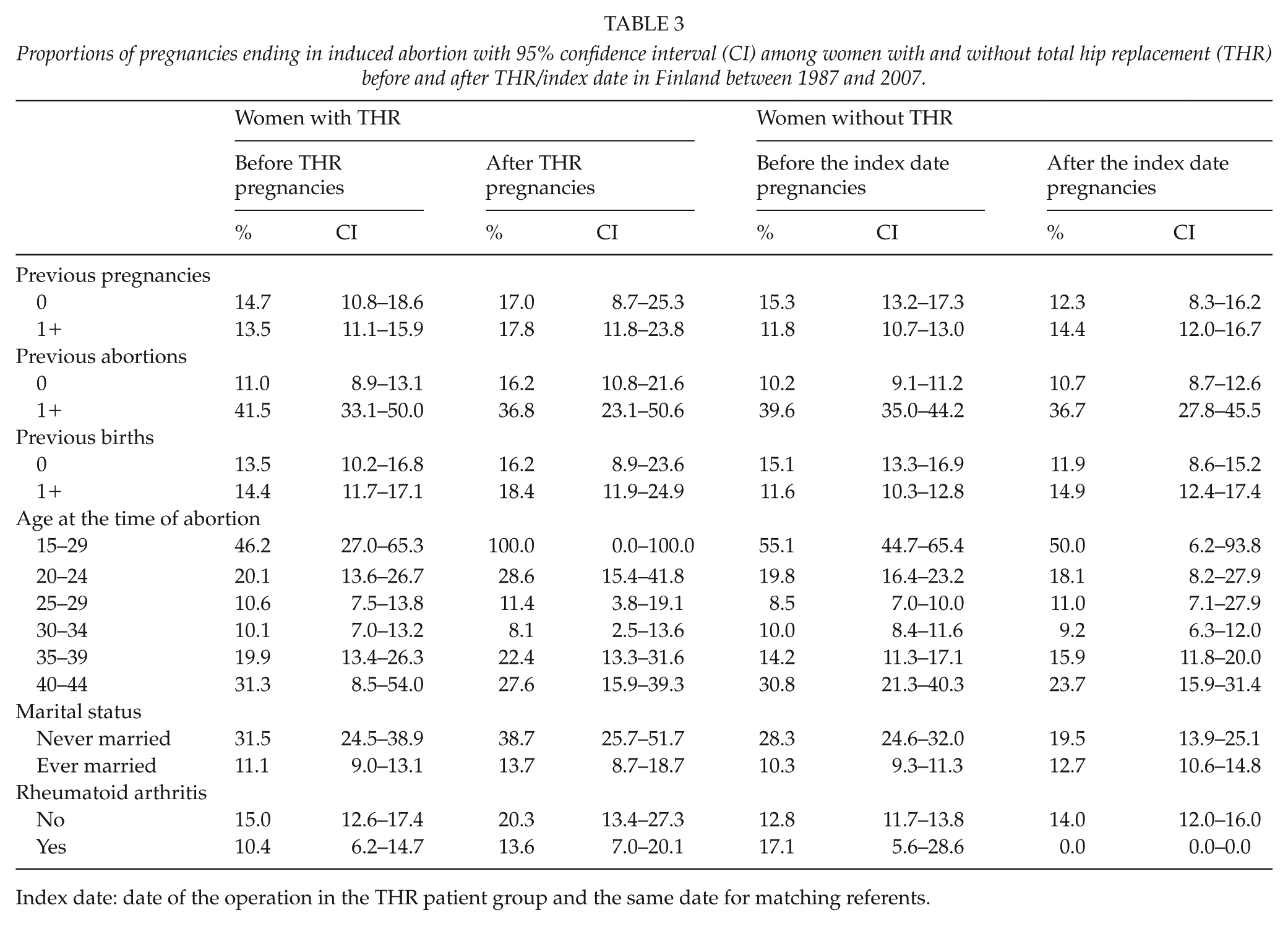
Index date: date of the operation in the THR patient group and the same date for matching referents.
Unadjusted OR for pregnancy ending in IA in the THR patient group after index date was 1.32 (CI 0.89–1.96), p = 0.17, in relation to the reference group (Table 4). When adjusted with the variables of marital status, age (<20 or >39), previous IAs, and previous deliveries, there was a trend for higher risk for pregnancy to end in IA in the THR group in relation to the reference group (OR 1.50, CI 0.99–2.28; p = 0.05).
Odds ratios (ORs) with 95% confidence interval (CI) for pregnancy ending in induced abortion of women with total hip replacement (THR) in relation to the reference cohort of women without THR before and after THR/index date, Finland 1987–2007.
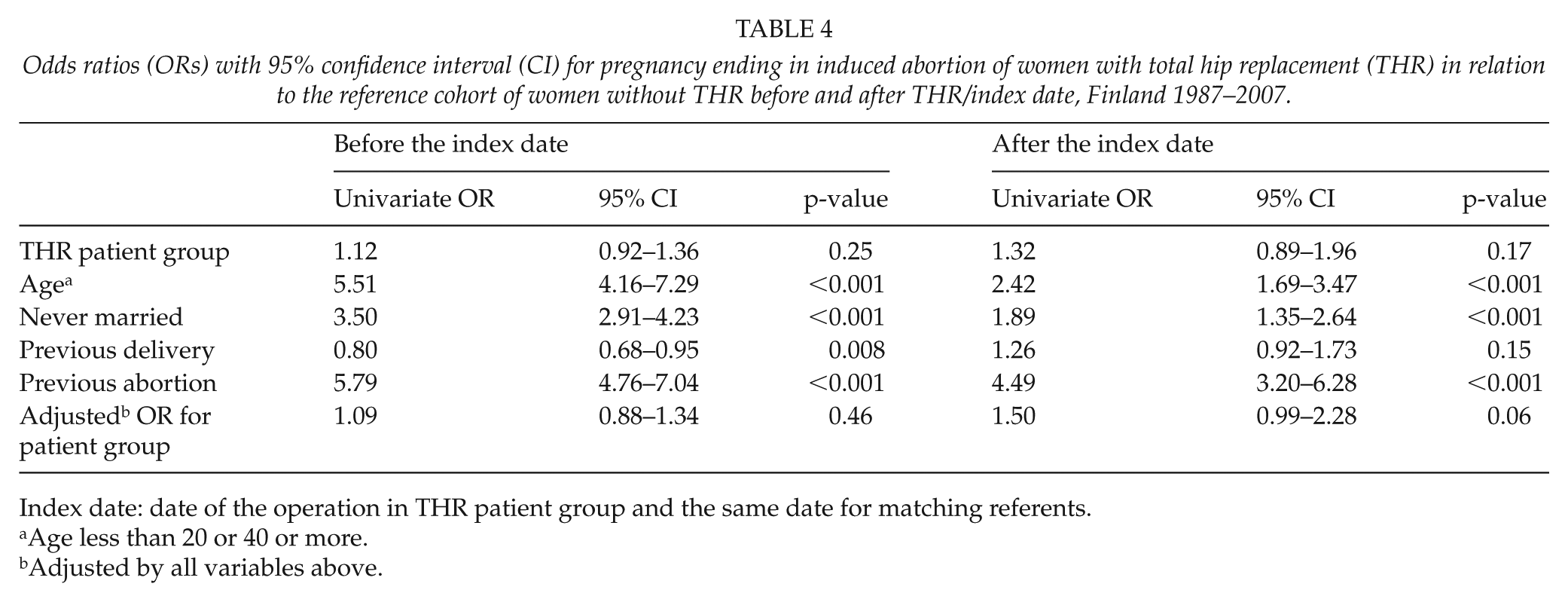
Index date: date of the operation in THR patient group and the same date for matching referents.
Age less than 20 or 40 or more.
Adjusted by all variables above.
Discussion
Our study showed no increase in the risk of pregnancy ending in IA in women with THR compared with women in the reference group. When adjusting for available confounders, such as age, marital status, previous deliveries, and abortions, the risk for abortion was increased in relation to the reference group but remained non-significant. More abortions were carried out due to maternal health reasons in the THR patient group than in the reference group.
No differences in IA proportions between the groups were observed when the THR patients were compared with the referents. The IA proportions in all groups were similar to the overall national abortion proportion in 2015 (14.5%). IA rates in the THR patient group were lower compared with the reference group and national rates. This finding was due to the lower number of pregnancies per woman in the THR patient group. Our previous study showed that women have lower birth rates after THR (14).
Since no previous studies have analyzed the connection between THR and IA, we must evaluate the effect of other possible factors. Women with THR had lower SES than the referents. Low SES is a risk factor for IA. Women with a lower educational level or income have a higher rate of IA when compared with women with a higher educational level and income (24, 25). The same effect was seen in our study population where blue-collar workers had higher IA numbers than persons with a higher SES. Although THR patients had lower SES, our study showed no increase in risk for IA in the THR group. However, the number of persons with missing information on SES was high in our study.
Previous IA was a high risk factor for IA in this study. Previous studies verify evidence on repeat IA, where the decision to have a second IA is easier after a previous IA (26). The incidence of repeated IAs is decreasing, however (27). After THR, women were more likely to have their first IA, which may indicate that THR might increase the IA risk.
In the THR patient group, there were more abortions both before and after THR due to maternal health indications than in the referents. Women with THR might have concerns about pregnancy, but the risk of IA was not increased (9). There is no evidence of THR complicating pregnancy or affecting pregnancy outcome (9, 10, 13). The THR patients might have had more baseline diseases compared with the referents. Some diseases are known to increase IA rates. For example, women using psychotropic medication or biological RA medication have increased abortion rates (28, 29). This finding could not, however, be identified in our present study due to the small incidences of chronic diseases (except RA) and the information on exact medications was not available.
This is the first study that has evaluated the relationship between THR and IA. One of the strengths of the study is the large, nationwide study population with long follow-up. Our study also compares the IA rates before and after THR. Another strength of the study is the high quality of the register data (6, 23). Our study provides nationwide population-based findings that include a large and comprehensive study population of THR patients and the reference cohorts. Furthermore, the register-based approach eliminates possible recall-bias, that is, possible previous IAs were identified from reliable registers, not with questionnaires.
Although the register data had high coverage and validity in most variables, information on SES was not fully available for this study. For example, data on the SES of only 34.1% of the participants were available. Moreover, even though the coverage was better in the MBR than in the RIA, it was still not possible to calculate reliable abortion ratios for each SES group or use them as a part of the logistic model. In addition, information on the marital status of the women at the exact time of the abortion was not available. Instead, we only had information on whether the women had ever been married.
Conclusion
Further studies are needed to confirm the clinical significance of these novel findings. This study shows that THR does not seem to be an independent risk factor for pregnancy ending in IA, although maternal health issues were a more common IA indication in the THR patient group. Further studies are needed to provide information on pregnancies and deliveries after THR.
Footnotes
Acknowledgements
The authors would like to thank Mr Peter Heath MA for the language editing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Competitive Research Funding of Pirkanmaa Hospital District, Tampere, Finland, representing governmental funding.