
Abstract
Background and Aim:
Post-traumatic hydrocephalus is a common complication that arises after head injury. However, risk factors associated with the outcome of post-traumatic hydrocephalus have seldom been addressed. Therefore, we performed this clinical study to analyze the risk factors affecting the outcome of post-traumatic hydrocephalus in patients with head injuries.
Methods:
A total of 116 post-traumatic hydrocephalus patients, admitted in our hospital between March 2012 and October 2017 were reviewed. The related factors assessed were age, gender, Glasgow Coma Score on admission, platelet count, plasma fibrinogen levels, D-dimer concentration, subarachnoid hemorrhage, subdural hygroma, cerebral hernia, cisterna ambiens, decompressive craniectomy, cranioplasty, ventriculoperitoneal shunt implantation, intracranial infection, and duration of comatous state. The patient outcomes after 6 months of treatment were evaluated by the Glasgow Outcome Scale. Risk factors for the outcome of post-traumatic hydrocephalus were evaluated by applying logistic regression analysis.
Results:
Poor outcome was observed in 66.4% of the patients (77/116). Univariate and multivariate analyses revealed that the disappearance of cisterna ambiens, the long duration of comatous state (>2 months), the high levels of plasma fibrinogen, and the ventriculoperitoneal shunt implantation were related to adverse outcomes (p < 0.05).
Conclusion:
The disappearance of cisterna ambiens, the prolonged duration of comatous state (>2 months), the high plasma fibrinogen levels are the most important factors affecting the outcome of post-traumatic hydrocephalus, and the ventriculoperitoneal shunt implantation is the most critical predictor of the outcome of post-traumatic hydrocephalus.
Introduction
Post-traumatic hydrocephalus (PTH) is a common secondary complication that follows traumatic brain injury (TBI) (1). It is an active and progressive process of excessive cerebrospinal fluid (CSF) accumulation due to liquorodynamic disturbances following craniocerebral injury. PTH is considered to be one of the main reasons for unexpected deterioration during rehabilitation after TBI. PTH if left untreated often leads to high mortality rates and occurrence of vegetative state after craniocerebral injury (2). Up to date, the studies about risk of developing PTH have been reported by many articles. But there are limited reports on the risk factors associated with the outcome of PTH. Therefore, we reviewed our patient records from 2012 to 2017 to identify factors that may influence the patient outcome. The purpose of this study was to investigate the association between various clinical factors and the outcome of PTH, in order to identify candidate risk factors for predicting PTH in patients with TBI.
Methods
Patient Population
A total of 1125 TBI patients were admitted at our institute from March 2012 to October 2017. In 116 patients with PTH, defined as hydrocephalus secondary to TBI, there were 86 male cases with an average age of 45.3 years, and 30 female cases with the average age of 44.8 years. Patients diagnosed with craniocerebral trauma in their first computed tomography (CT) scans, within 6 h post-injury, and later developed hydrocephalus, as observed during follow-up examinations, were included in this study. Patients exclusion criteria were as follows: (1) patients whose initial CT scan showed the presence of hydrocephalus, (2) patients with a history of neurological disease or intracranial pathological changes before their injury; and (3) patients who lost contact in the follow-up period (Fig. 1).
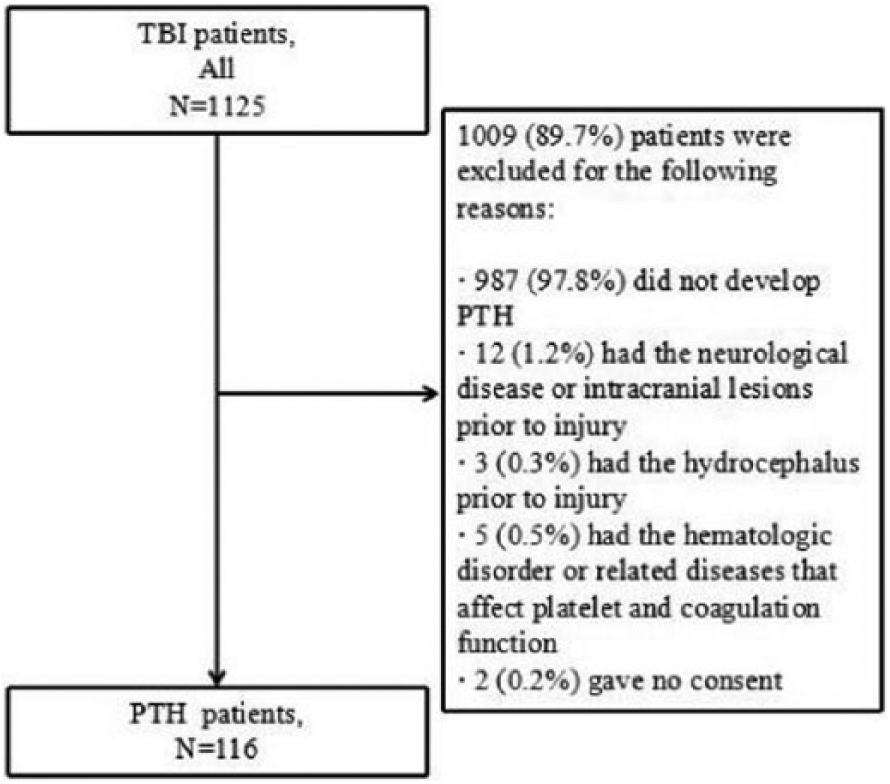
Patient flow diagram.
Patient Management
The patient diagnosis and treatment conformed to the international guidelines of the Brain Trauma Foundation (2007). All patients were evaluated with the CT scan and were followed with serial neurological examinations after admission. Intracranial lesions with midline shift greater than 5 mm, the volume of hematoma greater than or equal to 30/10 mL (supratentorial/infratentorial), or neurological deterioration were surgically removed. Decompressive craniectomy (DC) with standard large bone flap resection was performed in patients who have the diffuse brain swelling or massive intraoperative brain swelling. After surgery, all patients were returned to the neurological care unit for standard medical management.
PTH Diagnosis and Surgery
The main criteria for PTH diagnosis used in our study included both radiographic evidence and clinical manifestations of hydrocephalus.
These diagnostic criteria are as follows: (1) the Gudeman criterion, which is the enlargement of lateral ventricle and the three ventricles, with or without the presence of the cerebral sulcus on serial CT scans (2). (2) The Evans index, which represents the largest width of the frontal horns of the lateral ventricles divided by the internal diameter of the skull at the same level, is greater than 0.3 (3). (3) Clinical characteristics of PTH, such as neurobehavioral and cognitive impairment, increased flap tension in patients undergoing DC, and no improvement or deterioration of consciousness in patients with coma.
All patients with clinical and radiological signs of PTH were treated with a shunt. For conscious patients, before shunt operation, all patients were checked or followed up serially by brain CT. In our study, 70 patients underwent shunt operations. All patients with PTH were given ventriculoperitoneal (V-P) shunts. The interval time between trauma and shunt operation was all within 5 months in our study. In addition, 46 patients did not accept the shunt operations. Of them, 28 patients had the radiological signs of PTH, but they refused the shunt operations, because of the mild symptoms. 10 patients gave up the treatment due to family poverty. 8 patients were died before undergoing the shunt operations.
Clinical Variables Analyzed
Clinical data of the patients were collected from our institute’s clinical medical records and the admission and follow-up radiological database. The data collected included demographics (age and gender), Glasgow Coma Score (GCS) on admission, platelet count, plasma fibrinogen levels, D-dimer concentration, duration of comatous state, intracranial infection, cranial CT findings, and surgery. Cranial CT findings included subarachnoid hemorrhage, subdural hygroma, cerebral hernia, and cisterna ambiens. DC, cranioplasty, and V-P shunt implantation were classified as surgery.
In our study, the patients were divided into three age groups: ⩽44, 45–59, and ⩾60 years. The patients were also classified into two groups based on their GCS on admission (⩽8 and >8). The platelet count was defined as low when <100 × 109/L, normal for the range of 100–300 × 109/L, and high when >300 × 109/L. Plasma fibrinogen levels were considered low when they were <2 g/L, normal for the range of 2–4 g/L, and high when >4 g/L. The D-dimer concentration was divided into high (>200 µg/L) and normal (⩽200 µg/L) groups. Finally, the patients were allocated into two groups, based on the average duration of comatous state (⩽2 and >2 months).
Outcomes After PTH
The outcome of patients was evaluated by the Glasgow Outcome Scale (GOS) 6 months after the trauma. The GOS index definition is as follows: 1 = death, 2 = vegetative state, 3 = severe neurological deficit, 4 = mild neurological deficit, and 5 = premorbid level of functioning or complete recovery (2). For patients with GOS score ⩽3, the outcome was defined as unfavorable, and for those with GOS score >3, the outcome was defined as favorable.
Statistical Analysis
The statistical platform of Statistical Program for Social Sciences (SPSS version 19.0; SPSS Inc., Chicago, IL, USA) was used for analyses. The 15 factors assessed were defined as the independent variables, and the patient outcomes after 6 months were defined as the dependent variables. The chi-square and Mann–Whitney U tests were used for univariate analysis; the significant independent variables were incorporated into the multivariate regression model for multivariable analysis. Differences with p values less than 0.05 were considered statistically significant.
Results
In total, 33.6% (39/116) of the patients evaluated had a good outcome, 66.4% (77/116) were with poor outcome, and 6.9% (8/116) died. The results of the 15 factors assessed and the statistical comparisons between the two groups were as follows.
Univariate Analysis Results
The chi-square and the Mann–Whitney U tests revealed that there were significant correlations between the outcome of PTH and patients’ admission GCS (⩽8), subarachnoid hemorrhage, subdural hygroma, intracranial infection, cisterna ambiens disappearance, duration of comatous state (>2 months), high plasma fibrinogen levels, and V-P shunt implantation. Age, gender, platelet, D-dimer concentration, DC, and cranioplasty did not influence the outcome of PTH (Table 1).
Clinical factors of patients and univariate analysis of risk factors associated with the outcome of PTH.
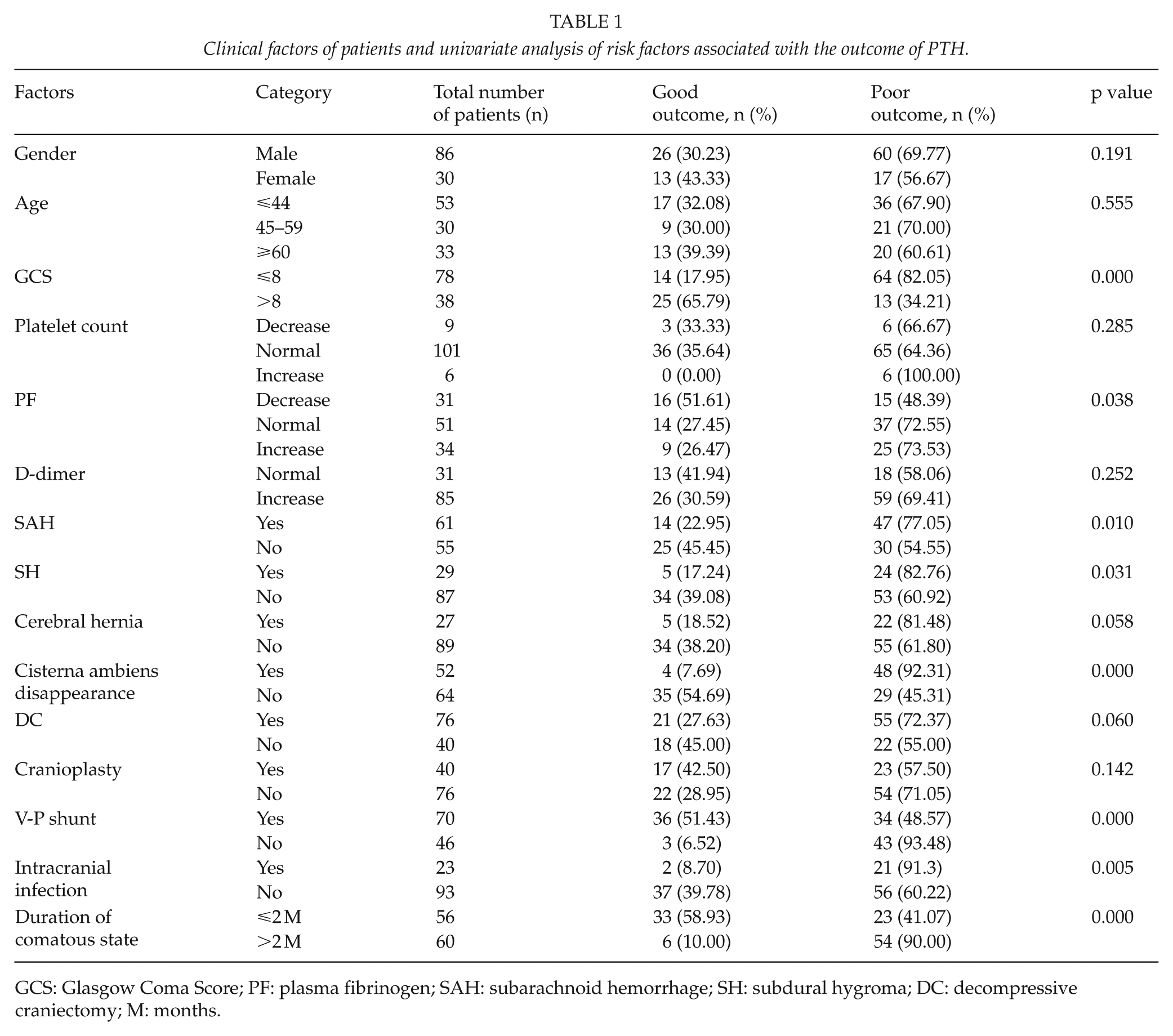
GCS: Glasgow Coma Score; PF: plasma fibrinogen; SAH: subarachnoid hemorrhage; SH: subdural hygroma; DC: decompressive craniectomy; M: months.
Multivariable Analysis Results
Results of multivariate logistic regression analysis are summarized in Table 2. In this model, cisterna ambiens disappearance, long duration of comatous state (>2 months), and high plasma fibrinogen levels were associated with the outcome of PTH, and the V-P shunt implantation was the most critical predictor of the outcome of PTH. There was no independent association between the outcome of PTH and the admission GCS, subarachnoid hemorrhage, subdural hygroma, or intracranial infection.
Multivariate logistic regression analysis of risk factors associated with the outcome of PTH.
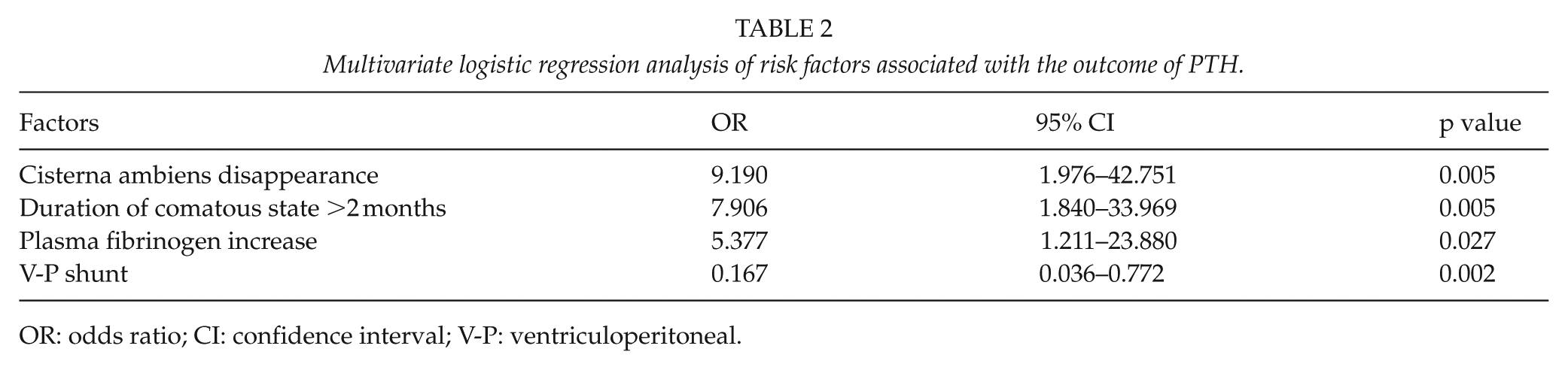
OR: odds ratio; CI: confidence interval; V-P: ventriculoperitoneal.
Prediction of Prognosis by Regression Analysis
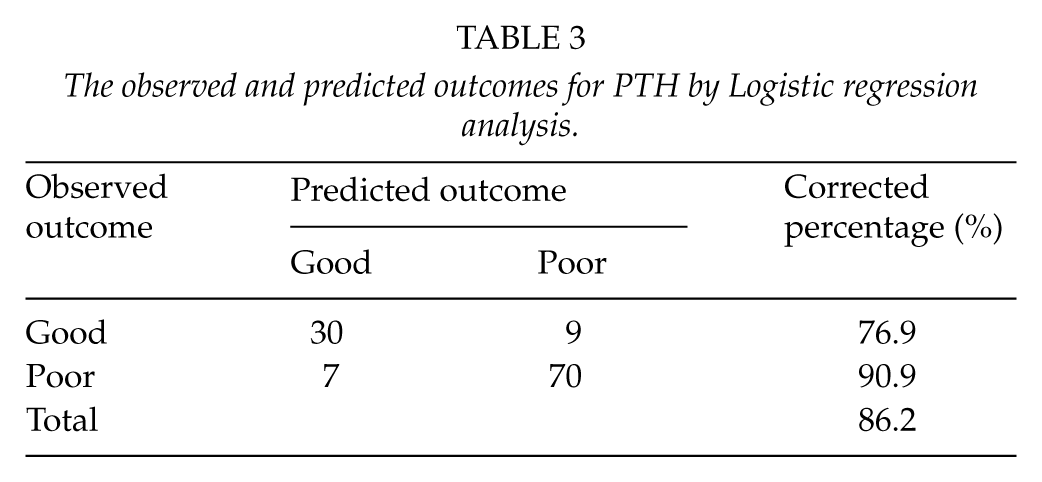
Out of the 39 patients with good outcome (based on our observational findings), 30 were predicted to have a good outcome by logistic regression analysis; the corrected rate was 76.9%. For the 77 patients defined with a poor outcome, the logistic regression analysis predicted that 70 patients would have a poor outcome; the corrected rate was 90.9%. The total coincidence rate of our logistic regression analysis was 86.2% (Table 3).
The observed and predicted outcomes for PTH by Logistic regression analysis.
Discussion
PTH is a common and serious complication that arises after TBI. It is usually characterized by ventriculomegaly, cerebrospinal fluid pathway obstruction, or cerebrospinal fluid absorption disorder (3). The incidence of PTH has increased up to 45% after it was first reported by Dandy and Blackfan in 1914 (4, 5). This may be attributed to the advancement of diagnostic tools, which makes the diagnosis of PTH more clear; in addition, the advancement of the ICU treatment improves the survival rate in severe TBI, which results in more patients developing to PTH. PTH often leads to metabolic disorder and dysfunction of the brain tissue, so if it is not diagnosed and treated on time, it can aggravate the clinical condition and neurological function of patients with TBI, thus affecting the rehabilitation of patients (5–12). At present, many studies have reported the risk factors of hydrocephalus after TBI, but few studies have focused on the related factors that affect the outcome of patients with PTH (11–15). In our study, clinical data of 116 patients with hydrocephalus after TBI were collected, and the possible factors affecting the outcome of the patients were investigated. Our study can contribute to the improvement of the PTH patients’ quality of life and prevent the burden on society and family by early intervention and effective treatment.
By univariate analysis, our data indicated that patient’s admission GCS (⩽8), subarachnoid hemorrhage, subdural hygroma, intracranial infection, cisterna ambiens disappearance, duration of comatous state (>2 months), high plasma fibrinogen levels, and V-P shunt implantation were risk factors for the outcome of PTH. There were no correlations between the outcome of PTH and age, gender, platelet, D-dimer concentration, DC, and cranioplasty. However, multivariate logistic regression analysis revealed that cisterna ambiens disappearance, long duration of comatous state (>2 months), high plasma fibrinogen levels, and V-P shunt implantation were associated with the outcome of PTH.
Cisterna ambiens disappearance was significantly correlated with the outcome of PTH in our study (odds ratio (OR) = 9.190, p = 0.005). In total, 52 patients did not have cisterna ambiens and 48 of them had a poor outcome; only 4 patients had a good outcome. Therefore, the disappearance of the cisterna ambiens has a significant effect on the prognosis of patients with PTH. The cisterna ambiens is a part of the perimesencephalic cisterns. It can reflect the pathological changes and functions of the brain stem, and can also indicate the state of intracranial pressure (ICP) (16, 17). The disappearance of the cisterna ambiens indicates that the brain stem is pressed and may shift its position (17–19), which can cause a series of complications and affect the prognosis of the patient.
Most of the patients with PTH in our study had severe craniocerebral trauma. After the occurrence of hydrocephalus, many patients had poor consciousness and a long duration of comatous state. In addition, some patients were in a vegetative state for a prolonged period of time. In this study, the average duration of comatous state in our patients was 2 months, and we found that in 60 out of the 77 patients who had a poor outcome, the duration of comatous state lasted for longer than 2 months. Furthermore, multivariate logistic regression analysis showed that comatous state with the duration of >2 months was related to the patients’ poor outcome (p < 0.05). This result is in agreement with the findings reported by Linnemann et al. (4).
Another important finding in this study was that the high plasma fibrinogen levels were associated with the outcome of PTH, according to multivariate logistic regression analysis. To the best of our knowledge this observation has not been previous reported by other similar studies. However, reports on the prognostic value of plasma fibrinogen levels for stroke patients have increased in recent years (20). We speculate that in patients with TBI, due to the severity of the brain trauma, the coagulation process is activated and this promotes an increase in the levels of plasma fibrinogen. Consequently, this may lead to increased blood viscosity in TBI patients. In addition, the blood–brain barrier is usually compromised, which might cause the high plasma fibrinogen levels to block the circulation of the cerebrospinal fluid and lead to the development of PTH. In such cases, the rehabilitation of patients will be affected. However, the mechanisms by which the increased plasma fibrinogen levels affect the outcome of patients with PTH still need further research.
Admission GCS, subarachnoid hemorrhage, subdural hygroma, and intracranial infection were all related to the outcome of PTH according to our univariate analysis results. However, multivariate logistic regression analysis showed that they could not serve as risk factors for predicting the outcome of PTH. This finding is contradictory to the results previously reported in the literature (4, 7). In addition, V-P shunt implantation as the best treatment for hydrocephalus was found had obvious correlation with the outcome of PTH in our study. This is similar to the clinical treatment. Kim et al. (7) reported that the V-P shunt has no significant effect on the outcome of the patients with PTH, but they included short follow-up periods and low patient numbers. Thus, we think that the V-P shunt still plays a critical role in patients with PTH.
Finally, there are several limitations in our study. First, the number of patients included is small, which might have introduced a significant bias in the patient selection process. Therefore, it is necessary to conduct further studies with larger sample size. Second, our study is retrospective and non-randomized, which may produce biases regarding patient selection, data collection and analysis. In addition, some factors such as ICP and repeated operation were excluded from our study because the data was incomplete. Therefore, prospective and controlled studies are required.
Conclusion
Hydrocephalus is a frequent complication that develops in patients with TBI. Here, we have demonstrated that the cisterna ambiens disappearance, long duration of comatous state (>2 months), high plasma fibrinogen levels, and V-P shunt implantation can be potential risk factors for predicting the outcome of PTH. The results can be used to assess the prognosis of PTH in patients with TBI. Early and more aggressive treatment of this targeted population can potentially contribute to the improvement of the PTH outcome.
Footnotes
Acknowledgements
S.S. and H.Z. contributed equally to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The article was funded by the High Level Talent Project of Jiangsu (2017WSW-166).