
Abstract
Background and Aims:
Patients with liver tumors involving the inferior vena cava have a poor outcome without surgery. Liver resection en bloc with inferior vena cava resection and reconstruction is now performed in many centers. The purpose of this study is to investigate the safety and efficacy of inferior vena cava reconstruction during hepatic resection.
Materials and Methods:
A review of 12 centers reporting 240 patients with combined hepatectomy and inferior vena cava resection and reconstruction for malignant tumors was performed. Sample size, patient characteristics, histological type of the tumor, method of reconstruction, complications, and long-term survival (1-, 2-, and 5-year survival) were evaluated.
Results:
A total of 240 patients from 12 institutions (male 58%) with mean age 54 years underwent combined liver resection and inferior vena cava resection and reconstruction for colorectal liver metastases (43%), cholangiocarcinomas (26%), hepatocellular carcinomas (19%), leiomyosarcomas (4%), and other tumors (7.9%). Reconstruction included primary closure (35.8%), patch repair (13.3%), or interposition graft (50.8%) In-hospital mortality was 6.25% and overall morbidity was 42.1%. 1- and 10-year survival rates were 79.7% and 28.9%, respectively.
Conclusion:
Tumors arising in or extending to inferior vena cava that require liver resection should be considered for surgery as it can be performed with an acceptable mortality and morbidity in centers with liver transplantation and hepato-pancreato-biliary facilities.
Keywords
Introduction
Surgical resection continues to be a potentially curative option for malignancies arising in or extending to the inferior vena cava (IVC). Complete or partial resection of the IVC with or without reconstruction may be required in order to achieve negative surgical margins (1–3). The complexity of such surgery is related to the level and extent of caval and adjacent organ (e.g. liver) involvement. Liver tumors often extend into the retrohepatic IVC and vice versa due to their adjacency (kidney, adrenal gland or retroperitoneal, and mesenchymal tissue).
The evolution of surgical techniques (e.g. in situ cold preservation and ex vivo resection) and peri-operative management (cardiopulmonary or veno-venous by-pass) has led to successful outcomes even when the tumor infiltrates large segments of the IVC including the hepatic vein confluence (4, 5).
Simple IVC ligation may be possible in the presence of long-standing obstruction with established collaterals. However, in the absence of preoperative obstruction or when collateral pathways have to be sacrificed during tumor excision IVC ligation may be not tolerated. Caval reconstruction techniques vary from simple suturing or patch repair to synthetic or biological graft interposition. If the hepatic confluence is involved, then hepatic vein reimplantation may be required (6–8).
Hepatectomy with en bloc resection of the IVC carries a higher surgical risk compared to liver resection alone. Therefore, careful preoperative evaluation of patient’s surgical candidacy is the key (7–9).
This study is a comprehensive review, aiming to evaluate the safety and efficacy of IVC reconstruction during hepatic resection, by assessing the morbidity, mortality, and long-term survival of these surgical techniques.
Materials and Methods
A comprehensive review using the PubMed database, aiming to investigate the safety and efficacy of IVC reconstruction during hepatic resection, was performed. Isolated and combined terms of “inferior vena cava resection,” “inferior vena cava surgery,” “inferior vena cava reconstruction,” and “liver resection/hepatectomy with IVC resection” were used. Data were accumulated from published registries, case series, and trials reporting surgical outcomes after IVC surgery and reconstruction combined with liver resection during cancer operations.
Inclusion criteria for eligibility were (1) peer-reviewed articles written in English, (2) studies including any type of hepatectomy in combination with resection and reconstruction of the IVC, and (3) studies originally published between January 2000 and December 2015. The citations in each article were reviewed to locate additional references that were not retrieved during the initial search. Baseline study (year and sample size) and patient (age, gender) characteristics were reviewed. The histological type of the tumor, peri-operative and post-operative characteristics (duration and type of surgery and reconstruction, complications, duration of hospital stay) and long-term survival (1-, 2-, and 5-year survival) were evaluated.
Case reports and studies with mixed cases including (1) IVC resection and ligation without reconstruction, (2) IVC tumor thrombectomy, (3) concomitant abdominal aortic resection, (4) superior vena cava (SVC) resection, (5) isolated hepatic vein resection without IVC component, and/or (6) IVC resection without hepatectomy were excluded.
Studies were selected and data were extracted independently by three reviewers (K.M., M.P. and C.K.). Disagreements were resolved by consensus after discussion between the reviewers. The studies were evaluated carefully for duplicate or overlapping data. Full texts were reviewed and analyzed when all criteria were met. The reported results of the individual studies were combined. Survival curve was calculated using IBM SPSS Statistics 23.0
Results
Baseline Study and Patient Characteristics
Initial search yielded 16,861 manuscripts. We reviewed the published abstracts. After application of pre-selected inclusion and exclusion criteria, 78 manuscripts were selected for full-text review. Further analysis revealed that 12 case series with total 240 patients fulfilled all pre-selected analysis criteria (Fig. 1). Five series were published from groups in Europe, five from the USA, one from Japan, and one from Brazil. The mean age of the patients was 54 years, of whom 138 (58%) were male with a mean follow-up of 30 months. The most common malignancies were colorectal liver metastasis 104 (43%), cholangiocarcinomas 62 (26%), hepatocellular carcinomas 45 (19%), and leiomyosarcomas 10 (4%), while others, such as adrenocortical, gastrointestinal stromal tumor, squamous cell carcinoma, hepatoblastoma, inflammatory pseudotumor, and renal cell carcinoma accounted the remaining 19 cases (7.9%).
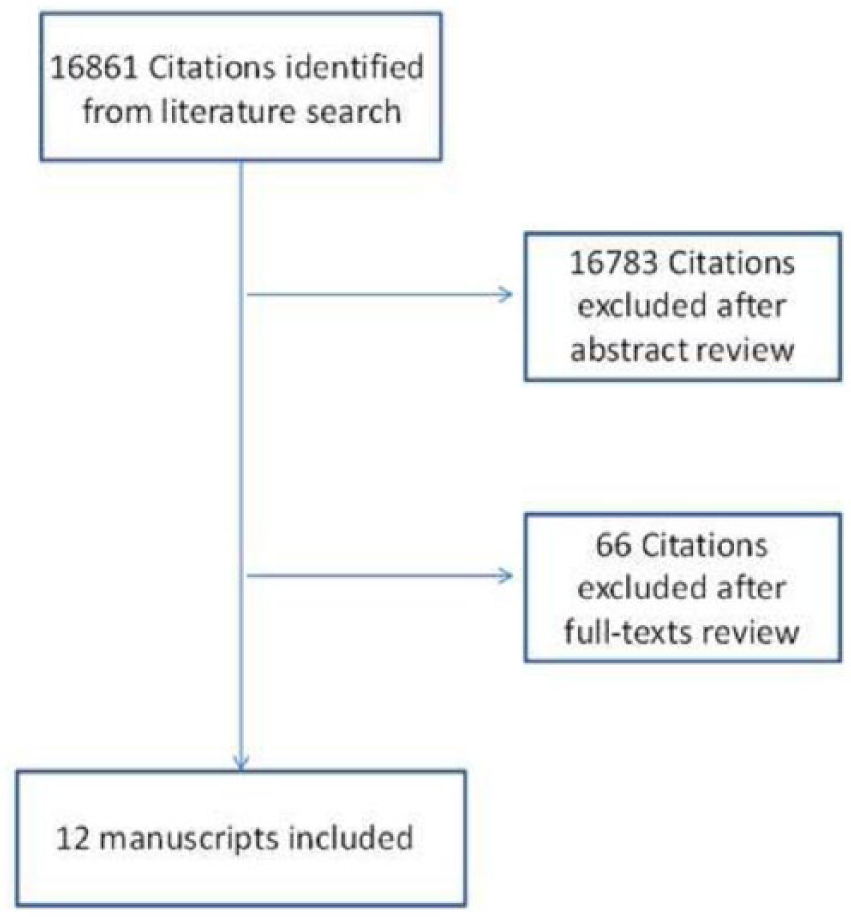
Publications searching analysis.
Type of Surgery, Peri-Operative and Post-Operative Characteristics
The most common liver resection was right or extended right hepatectomy 174 (72.5%) followed by left or extended left hepatectomy 41 (17.1%). In 25 (10.4%) cases, a segmentectomy and/or caudate lobectomy was performed. In 118 (49.2%) cases, a tangential resection of the cava was performed and no caval replacement was required. In 86 (35.8%) of these patients, primary closure of the cava with direct suturing was performed, while 32 (13.3%) required the use of a patch (polytetrafluoroethylene (PTFE), bovine or autologous).
A further 122 patients (50.8%) underwent circumferential resection of the IVC with either PTFE (113; 47.1%) or Dacron graft (8; 3.3%) reconstruction. A cadaveric caval homograft was used in one case. During resection veno-venous by-pass was used to maintain hemodynamic stability in 43/205 (19.8%) patients (one study did not report results). Hepatic vein(s) had to be reimplanted in 19 (9.3%) of cases. In addition, 34 cases (14.2%) with anticipated prolonged ischemia of liver during total vascular exclusion had in situ cold perfusion of liver. Two studies reported a total of 12 cases (6 in each) with ex vivo resection.
The surgery was performed by either a Liver Transplant team or by a Hepatobiliary and a vascular surgeon and the average duration was 361 min. Patients remained in hospital for a mean of 16.1 days. An R0 resection was achieved in 181/212 (84.77%) cases, while in 60/211 (28.4%) cases, no microscopic IVC wall invasion from the cancer could be identified. Standard peri-operative (5–8 days) anticoagulation with either heparin infusion or low molecular weight heparin (LMWH) was used in all studies (four studies did not provide data). Long-term post-operative prophylaxis (>1–6 months) with aspirin, warfarin, or LMWH was given mostly for graft patients. In one study, no post-operative anticoagulation agent was recommended, and in four studies, no data were provided. In terms of graft patency, four PTFE (3.5% 4/113) (two with non-occlusive thrombus) and two Dacron (25% 2/8) thrombosis cases were reported. The actual rates of IVC thrombosis might be higher in long term, as in most studies it is unclear whether a structured follow-up to assess IVC patency was followed. In addition, two cases of IVC stenoses and one external compression from tumor recurrence were reported.
Mortality–Morbidity
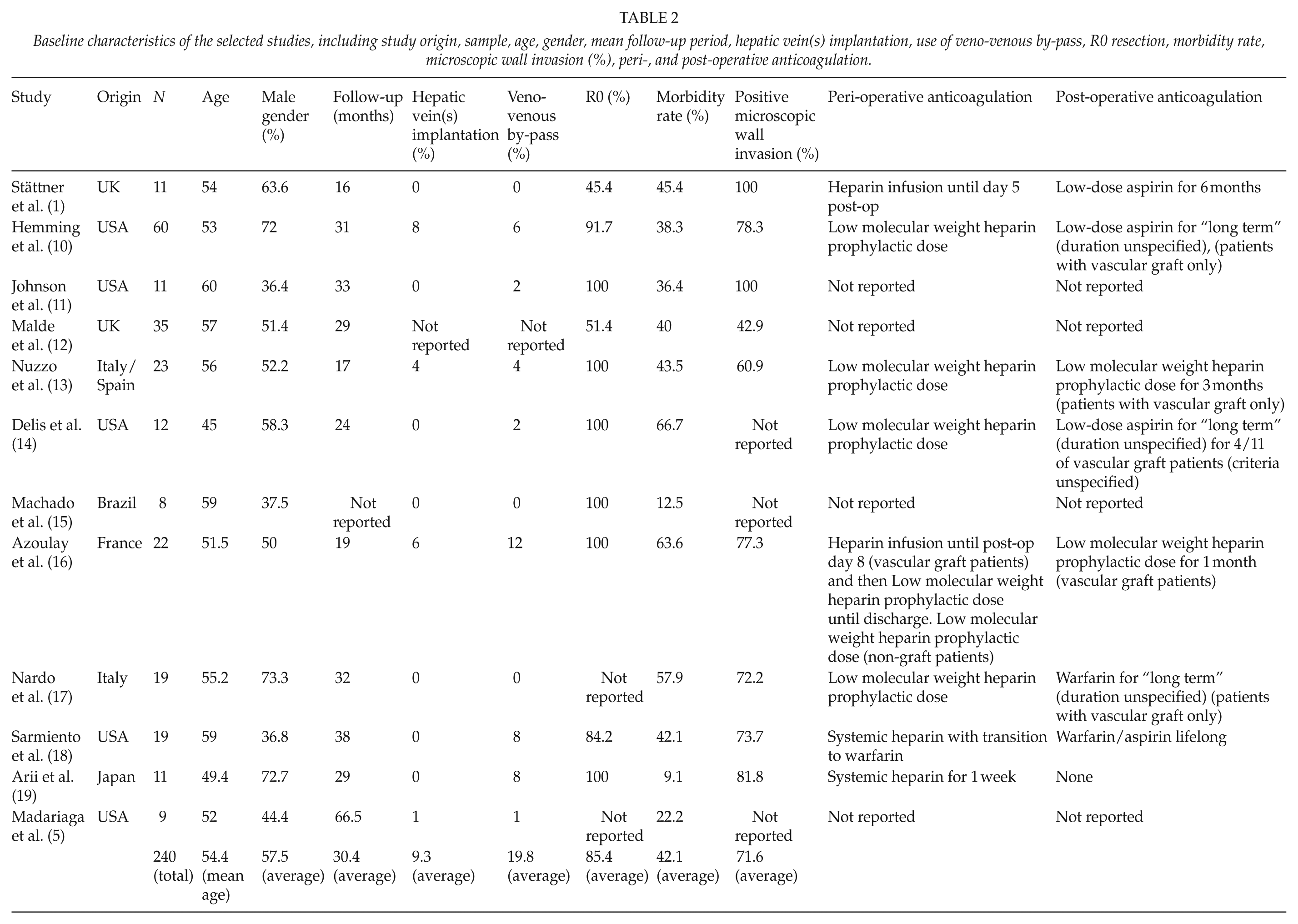
The overall in-hospital mortality was 6.25% (15/240). The most common causes were sepsis and multi-organ failure, small for size syndrome and intractable bleeding associated with coagulopathy. The overall morbidity was 42.1% (9.1%–66.7%). The most common complications were hepatic and renal failure (12.9% and 4.6% of cases, respectively), pleural effusion (8.3%), bile leak (6.7%), intra-abdominal abscess and sepsis (3.75%), ascites (2.5%), graft thrombosis (2.5%), post-operative bleeding (2.1%), wound infection (1.25%), bile duct stricture (1.25%), and others ((5.4%) atrial fibrillation, chylous leak, deep venous thrombosis (DVT) of lower extremities, adrenocortical insufficiency, cardiac arrest, pneumothorax, nerve palsy, brain hemiparalysis, lower extremities lymphedema, myocardial infarction, and ileus) (Table 1). Detailed data of the studied cases are shown in Table 2.
List of complications.
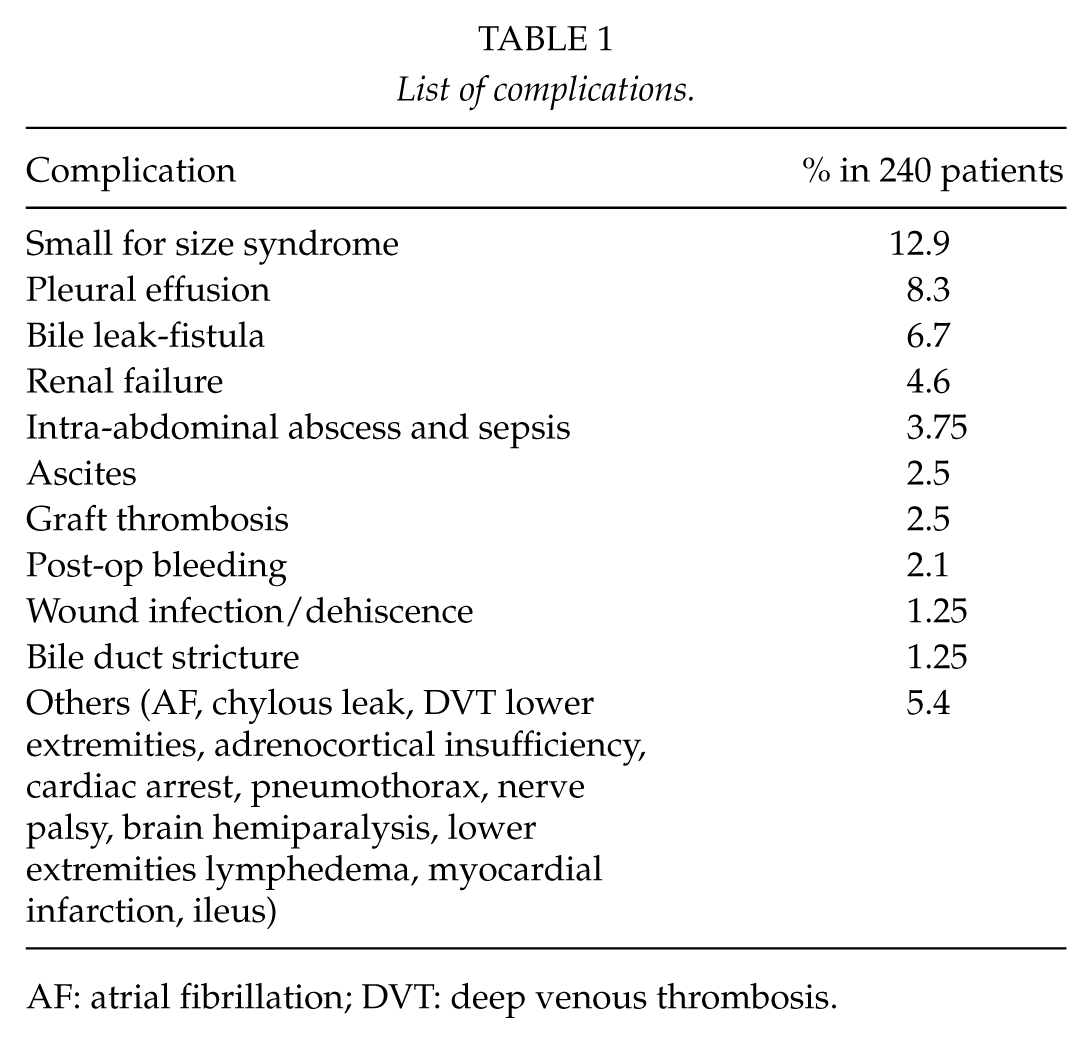
AF: atrial fibrillation; DVT: deep venous thrombosis.
Baseline characteristics of the selected studies, including study origin, sample, age, gender, mean follow-up period, hepatic vein(s) implantation, use of veno-venous by-pass, R0 resection, morbidity rate, microscopic wall invasion (%), peri-, and post-operative anticoagulation.
Long-Term Follow-Up
Outcome data for individual patients were reported in eight studies (5, 11, 14, 16, 18–21). 1-, 3-, and 5-year survival rates for those studies were 78.1%, 47.7%, and 40.0%, respectively, with a median overall survival of 34 months. One study reported a median overall of 38 months and 5 year survival of 21%, another reported actuarial 1- and 5-year survival rates of 89% and 35%, respectively, the third had a median follow-up of 16 (range of 8–24 months and 1-year survival of 90.9%), and the fourth did not provide survival data. Overall, 1-year survival from 11 studies was 79.7% (Fig. 2).
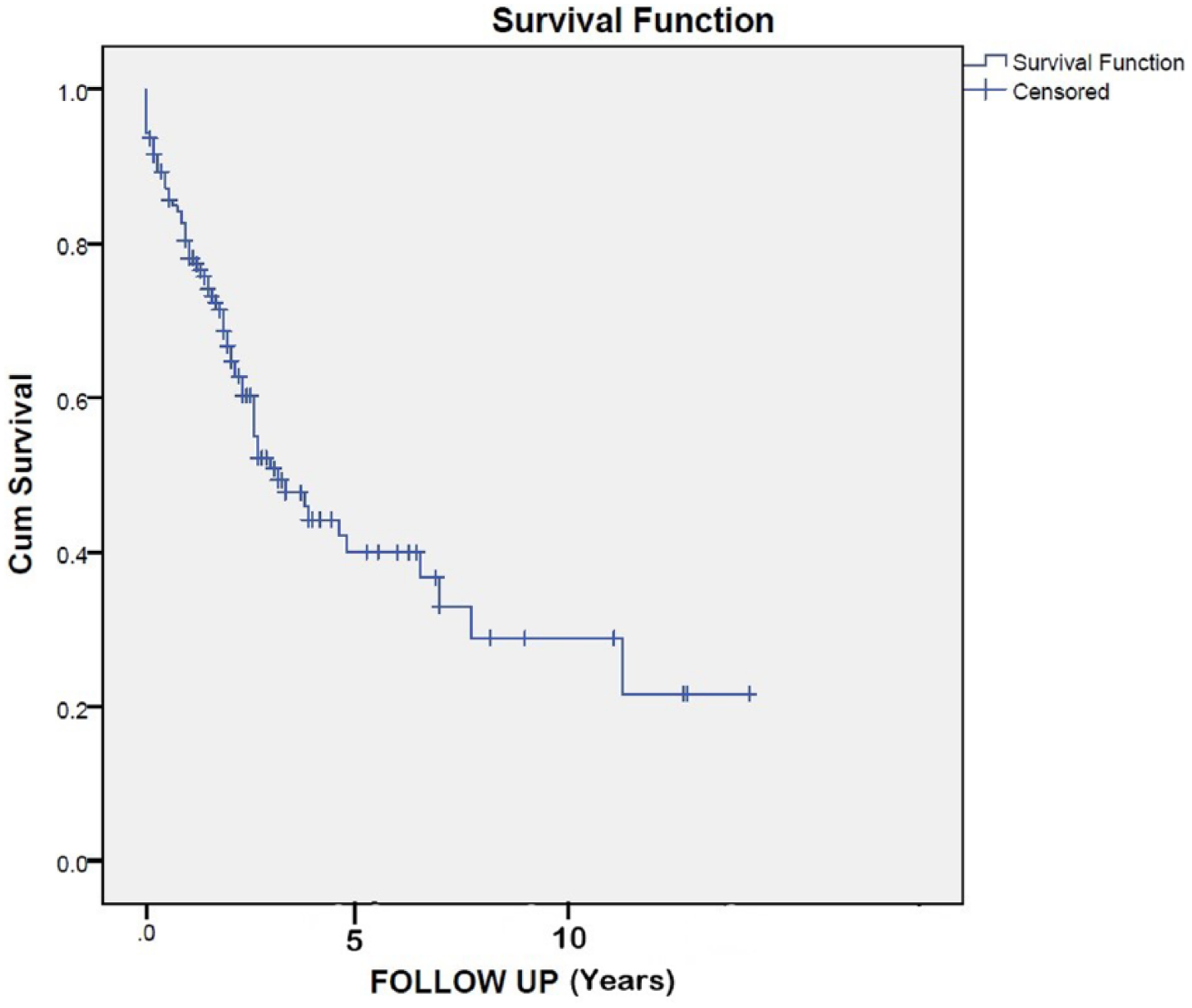
Kaplan–Meier survival curve as reported in eight studies (Arii et al., Malde et al., Madariaga et al., Johnson et al., Azoulay et al., Delis et al., Nardo et al., Nuzzo et al.).
Discussion
Patients with liver tumors involving the IVC, often presenting with symptomatic venous obstruction, have limited options for treatment with chemotherapy or interventional radiology. Survival without surgery is typically less than 1 year (9). Depending on the tumor type and histology, neoadjuvant treatment may be an option aiming to downstage the malignancy and lessen the extent of resection or convert to a resectable state. In the past, if long segments of IVC had to be removed, simple ligation was applied when tolerated; however, this technique was associated with post-operative renal impairment and venous engorgement (10, 22).
Reconstruction of IVC is considered to be a surgical challenge, but due to evolution in surgical techniques and experience from liver transplantation, it has become more routine, and most published series and case reports have shown successful outcomes in selected patients (12, 20). The use of veno-venous or cardiopulmonary by-pass or the use of cold perfusion into the liver extends the duration of vascular occlusion, thus allowing for more complex resections. The use of synthetic grafts can provide excellent restoration of caval flow with option of additional implantation of other veins (e.g. hepatic and renal) when required (12, 20). Good surgical candidates are considered to be <75 years old, with no evidence of multifocal or distant disease, absence of hepatic or renal insufficiency, and evidence of adequate cardiopulmonary reserve (10).
Important factors influencing surgical strategy include (1) the level of IVC involvement and the need for hepatic veins(s) implantation, (2) circumferential and longitudinal extend of IVC wall involvement, and (3) other organs associated with the tumor (e.g. kidney, portal vein, and bile duct) (17, 21). The site of IVC that needs to be resected will determine the type of vascular occlusion required in association with inflow and outflow control during parenchymal transection. Caval clamping below the hepatic vein confluence and above the renal veins for infrahepatic IVC access is mostly used in the reconstruction of the retro- and suprarenal cava (13, 17, 23). Tumors involving the IVC at the hepatic confluence require total vascular exclusion (TVE) including both portal venous and hepatic arterial inflow as well as occluding the IVC above and below the hepatic veins. TVE is considered to be less well tolerated in terms of venous return and hepatic ischemia (16, 18). Depending on the hemodynamic status of the patient and the anticipation of prolonged reconstruction (e.g. hepatic vein(s) implantation), if the ischemic time is expected to exceed 45–60 min, veno-venous by-pass and cold perfusion of the liver with a standard preservation solution may be used (10, 12, 23, 24). Tumors reaching the right atrium require thoracotomy/sternotomy and the use of cardiopulmonary by-pass with circulatory arrest (25, 26).
Tumors that extend to the peri- or infrarenal portion of IVC need additional considerations. Post-operative transient or prolonged renal impairment is often seen due to temporary or permanent renal vein occlusion during reconstruction (25–28).
Of 11 (out of 12 studies), which have reported on the use of veno-venous by-pass, 43 cases (19.8%) were identified where by-pass was used regardless of TVE. The use of veno-venous by-pass increases the possibility of other complications, including venous thromboembolism and air embolism. However, its use reduces congestion and is helpful in complex cases particularly if a kidney is included in the resection (10, 26). Some authors from these publications have suggested that the indication is primarily based on the duration and type of vascular occlusion and efforts should be made to avoid this if possible. In addition, many units have little or no experience of veno-venous by-pass unless they use it to perform liver transplantation (11, 19, 23).
Preoperative imaging provides information on the extent of caval involvement, but definitive decision on resection and reconstruction is made intraoperatively (29). If less than 30% of the circumference of the IVC wall is involved then, simple suturing in a longitudinal or transverse fashion will usually suffice (15). A patch closure is appropriate for larger defects. A variety of options (synthetic or autologous) such as internal jugular vein, bovine pericardium or PTFE have been utilized, depending on surgical expertise, availability, and potential contamination status (10, 12, 14).
For defects of greater than 50%, an interposition graft is required. This review has shown that in half of the reported 240 cases (50.8%), a tube graft was applied with ring-reinforced PTFE in the majority 113/122 (92.6%) or Dacron 8/122 (6.6%). Dacron was the option of choice in the past, but has been associated with a high incidence of thrombosis and stenosis (5). PTFE graft is preferred due to its inert and biocompatibility properties (10, 17, 16, 25). The surrounding ring resists compression by adjacent structures. Common modalities used for follow-up check of IVC patency included ultrasonography, helical imaging (CT or magnetic resonance imaging (MRI)), and invasive venography in some occasions (17, 18).
Anticoagulation policy varied among these studies, and in the literature, there is no universal protocol to guide management (7). It seems that the majority of surgeons routinely use a systemic intraoperative heparinization, especially in cases where a vascular graft or a patch is used or prolonged by-pass is performed. The use of topical heparinized saline instead of intravenous heparin has been proposed by others as this has been associated with less intra- and post-op bleeding (6, 26). In-hospital anticoagulation with low molecular weight heparin (LMWH) or heparin infusion as a standard prophylaxis regardless the complexity of surgery or the use of vascular graft appears to be widely accepted by the authors of those studies. Long-term anticoagulation with LMWH or warfarin and its duration to prevent graft thrombosis is controversial. An alternative option could be the low-dose aspirin for short or longer period of time. It is unclear whether the low rate of post-operatively graft thrombosis in this review is directly associated with the use of anticoagulation, as some studies have reported good results without. Potential benefit may exist for high-risk patients (previous venous thromboembolism, coagulopathy due to massive intraoperative bleeding and transfusion, large tumors, implantation of hepatic or renal veins).
Benefit from en bloc liver resection with IVC during cancer operation arises from the negative margins obtained. In the current review, R0 resection was achieved in almost 85% of cases (181/212). Of note, microscopically positive IVC wall invasion was identified in 151/211 (71.6%) of cases. In the literature, it has been reported that between 18% and 39% of patients undergoing any form of IVC resection, show no histologic involvement of the IVC wall, despite strong radiological evidence and macroscopically apparent invasion (10). Associated desmoplastic and inflammatory reaction between the tumor and the IVC wall may offer an explanation for this. In practice, it is difficult to assess the degree of potential inflammation and may be impossible to obtain a safe plane without creating a caval defect (10, 19).
The in-hospital mortality was 6.25% and was predominantly due to small for size liver syndrome and sepsis. The overall morbidity was 42.1%, but accurate correlation and comparison of specific types of IVC repair was difficult to derive, as precise data from each study were not provided. It seems that both morbidity and mortality were not directly associated with the IVC resection and repair but more with the extent of liver resection and its complications. Again, small for size syndrome was the leading factor, and most of other complications were directly or indirectly related to it. It is anticipated that more complex cases with prolonged vascular occlusion, hepatic ischemia, and additional organs resection and reconstruction (e.g. portal vein and bile duct) would carry higher risk. Interestingly, overall complications related to IVC manipulation and reconstruction such as thrombosis, external compression and occlusion or infection, lower extremities edemas, and DVT with associated pulmonary embolism were very low (<3%). Interestingly, in the literature, general long-term (5 years) patency rates after IVC resection and reconstruction with or without liver resection have been reported between 67% and 92% (23, 28).
The average 5-year survival reported in eight studies, reached 40%. Two other studies reported 5-year survival of 21% and 35%. 1-year survival was 79.7% in 11 studies. However, these reports mix patients with a variety of primary and metastatic tumors and represent a limitation of this review, as it is difficult to identify differences in outcomes and disease-free intervals based on histological type and adjuvant treatment. Surgery seems to provide a substantial oncological and survival benefit with an acceptable mortality and morbidity rate in these selected patients, while alternative treatments are associated with poor outcomes. Careful selection of patients after multidisciplinary evaluation and referral to a specialized center with appropriate facilities (e.g. liver transplantation) should be considered and may contribute to improved outcomes (30).
This comprehensive review is limited by the fact that the data from the individual studies was combined without taking into account the in-between study variability, and as a result, the summary estimates may be imprecise. In addition, some studies have not provided data for important parameters, such as long-term prognosis and post-operative anticoagulation policy. In the absence of formal study quality assessment, most studies were single-center series reporting on a variety of indications, patient populations, and specific procedures with lots of clinical heterogeneity. In addition, the summary estimates generated by this review should be interpreted with some caution and be seen as a rough guide to the expected outcomes following these procedures given the high degree of clinical heterogeneity between studies.
In this review, an attempt was made to identify publications reporting hepatectomies with reconstruction of the IVC for malignancy. This study demonstrates the effectiveness of the different surgical approaches with a variety of tumors. IVC invasion by primary or secondary malignant tumors that require liver resection should not be considered a contraindication for surgery as it can be performed with an acceptable mortality and morbidity in experienced centers. Despite the relatively small number of such operation reported worldwide, future studies with less heterogeneity focusing on specific tumor types may help define criteria for selecting patient with favorable outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.