
Abstract
Background and Aims:
The present standard of care in treating lower extremity soft tissue sarcomas is function-sparing, limb-preserving resection and reconstruction with or without oncological therapy. The aim of this pilot study was to test the suitability and adequacy of the Finnish translations of two functional outcome questionnaires (Toronto Extremity Salvage Score and Musculoskeletal Tumor Society score) and to perform a preliminary investigation of functional outcomes of Finnish lower-limb soft tissue sarcoma patients after operative treatment.
Materials and Methods:
Between June 2015 and December 2015, consecutive surgically treated outpatients were asked to participate in the study. Demographic, clinical, surgical, and oncological outcome data were collected. Two functional outcome questionnaires were used (Toronto Extremity Salvage Score and Musculoskeletal Tumor Society scores). A comparative analysis is presented.
Results:
A total of 19 lower-limb soft tissue sarcoma patients with a mean follow-up time of 2 years and 10 months were included. All (n = 19) invited patients participated in the study. Mean age was 62.3 years. In total, 13 had high-grade sarcomas. Eight wounds were closed directly, four used skin grafts, and five required flap reconstructions. One patient required a tumor prosthesis, and one required a rotationplasty. A total of 14 patients received oncological therapy. No problems or difficulties were reported in using and completing the Finnish versions of the Toronto Extremity Salvage Score or Musculoskeletal Tumor Society questionnaires. The overall Toronto Extremity Salvage Score and Musculoskeletal Tumor Society scores were 88 and 76, respectively.
Conclusion:
This pilot study suggests that the Finnish versions of the Toronto Extremity Salvage Score and Musculoskeletal Tumor Society questionnaires are suitable for measuring functional outcome after lower extremity soft tissue sarcomas treatment. Functional outcomes vary from moderate to excellent.
Introduction
Soft tissue sarcomas (STS) are rare malignant tumors that represent approximately 1% of all solid malignancies in adults (1, 2). These tumors are a group of heterogeneous mesenchymal neoplasms that can arise in any anatomical site. Over half are situated in the extremities and the most common location is the lower extremity (3). The age-adjusted incidence of STSs in Finland has been stable at approximately 4.1 cases per 100,000 person-years, with 220 new cases in 2015 (ICD-10 codes C48-49) (4).
Treatment of STS is based on surgical excision and oncological therapy. Historically, the only reasonable treatment option for tumors near the vascular bundle was amputation (5). The present standard of care in treating lower extremity STS is function-sparing, limb-preserving resection (6). Reconstruction is indicated for tissue defects, filling of the resection cavity, or wound closure. The methods of reconstruction include skin grafts, local fasciocutaneous flaps, pedicled flaps, or free flaps (7). Oncovascular reconstruction has also been used more often recently and is required in cases where major vascular structures are involved and resected (8, 9).
Oncological treatments are radiotherapy or chemotherapy (or both) and can be administered preoperatively or postoperatively (or both). In some cases, preoperative chemotherapy is used to facilitate surgical treatment. When wide surgical margins are achieved, oncological therapy can sometimes be omitted (10).
Health status or health-related quality-of-life measures evaluate treatment effectiveness and guide treatment decisions (11–13). To allow benchmarking and accuracy of outcomes, it is important to use validated questionnaires to investigate functional outcome. The Toronto Extremity Salvage Score (TESS) and the Musculoskeletal Tumor Society (MSTS) score are the most frequently used patient-reported outcome measures (PROMs) for measuring functional outcome in lower extremity sarcoma patients (14).
The aim of this pilot study was to test the suitability and adequacy of the Finnish translations of the TESS and MSTS scores and to investigate functional outcomes of Finnish lower-limb STS patients after operative treatment. This study is a part of the translation and transcultural adaptation process for the Finnish versions of the TESS (15) and MSTS score (16) measures.
Materials and Methods
The study was accepted by the ethics committee of Helsinki University Hospital. All participants provided written informed consent. The inclusion criteria were lower extremity STS, local disease at the time of diagnosis, operative treatment, a minimum 6-month follow-up time, and written informed consent. Between June 2015 and December 2015, consecutive patients were identified in the outpatient clinic of Helsinki University Hospital Comprehensive Cancer Center during routine follow-up visits. All patients had the opportunity to comment or remark on the questionnaires or the overall procedure for completing them.
PROMs
We used the TESS (15) and MSTS scores (16) to measure functional outcome. The translation and cultural adaptation of the questionnaires were performed adhering to internationally accepted guidelines (17, 18). The TESS questionnaire was mailed to patients before the follow-up visit, and the MSTS questionnaire was completed during the follow-up visit. TESS and MSTS results were recorded (15, 16).
TESS
The TESS is a reliable and valid PROM. It measures activity limitations in patients who have undergone surgery of the extremities. There are separate measures for upper and lower extremities, which consist of 29 and 30 questions, respectively. The measure observes everyday activities such as working, dressing, and driving a car. All questions are rated on a scale from one to five, with five representing normal activity. The result is a percentage of the maximum score (15).
MSTS Score
The MSTS score is an oncology-specific PROM. The revised 1993 version of the MSTS places less importance on clinical parameters in favor of functional outcome (16). Six items are completed together by a physician and patient. Six different parameters are measured. Pain, function, and emotional acceptance are measured for both upper and lower extremities. For the lower extremity, use of walking aids, gait, and walking are evaluated. Hand positioning, dexterity, and lifting ability are evaluated for the upper extremity. All six categories are rated on a scale from zero to five, with five representing normal function. Function is expressed as percentage of the maximum score (16). The MSTS is intended to measure limb tumor patients’ functional outcome and impairment (16). We used MSTS version 1993 (16) for this study.
Translation and Cross-Cultural Adaptation Protocol
The process is presented in Fig. 1. In step 1, two native Finnish speakers well acquainted with Anglo-Saxon culture independently translated questionnaires into Finnish. One translator had a medical background. In step 2, after thorough discussion with translators, a first consensus version translated questionnaires were produced. In step 3, two bilingual native English speaker translators back-translated the first consensus version into English. In step 4, a panel consisting of all four translators and the authors discussed all previous work, including the translation process, results, and reports. An issue concerning the TESS instrument was resolved by contacting the author of the original version. Next, pre-final versions of the questionnaires were produced. In step 5, a pilot study was performed among 19 consecutive patients with surgically treated lower extremity STS. A structured interview was conducted with all patients after completing the questionnaires, in accordance with the guidelines of the European Organization for Research and Treatment of Cancer (EORTC) (19). Subjects were asked about the difficulties of words, phrases, or questions; possible confusions; potentially shocking emotional reactions; and alternative forms of presentations or questions. In step 6, after discussion of the interview results, the final versions of the Finnish TESS and the MSTS versions were adopted.
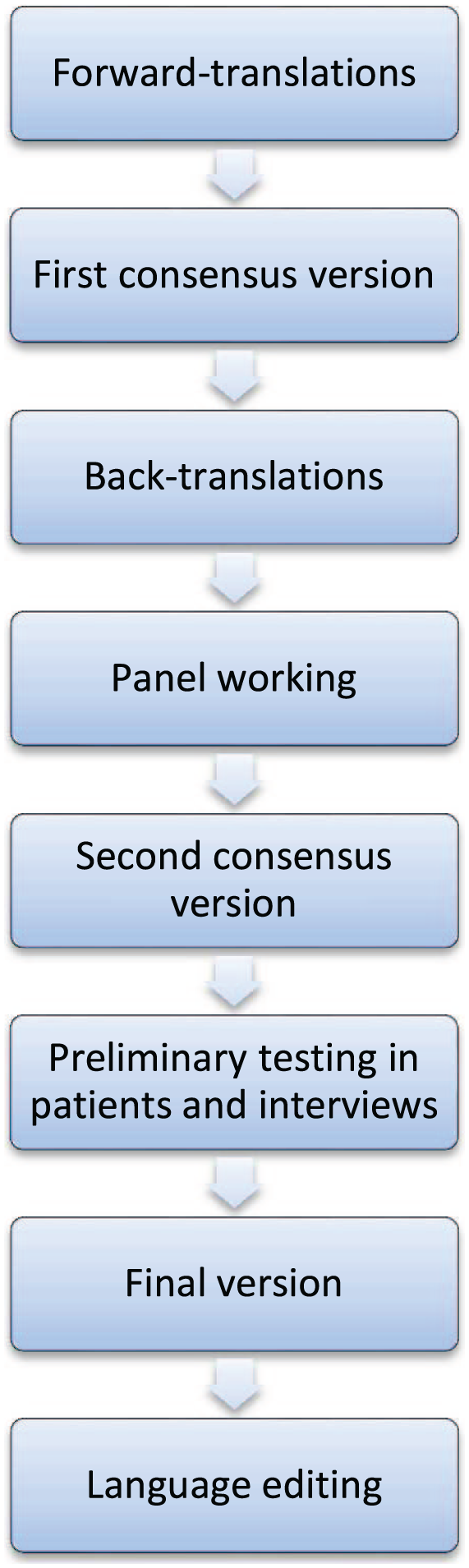
Translation and cultural adaptation process.
Statistical Analysis
Demographic, clinical, surgical, and oncological outcome results are reported as means, standard deviations, and ranges. The maximum and minimum values were assessed as a part of a reliability assessment. Correlations between the MSTS and the TESS were analyzed using Spearman’s correlation coefficients. MSTS scores were converted into percentages to conduct this analysis. Analyses were performed with SPSS 21 (SPSS Inc., Chicago, IL, USA).
Results
Translation and Testing of Questionnaires
Some linguistic discrepancies were observed in the translation process. A few translation differences and cultural issues were observed between translations. For example, the TESS question on “participating in sexual activities” was changed in the second consensus version, as back translations produced results focused too much on the act itself. The linguistic and cultural aspects of selected changes at the various stages of the translation and cultural adaptation process are presented in the supplementary material.
All 19 patients who were invited agreed to participate in the study. No problems or difficulties were reported in using and completing the Finnish versions of the TESS and MSTS questionnaires.
Questionnaire Assessment
In the TESS instrument, there was a slight ceiling effect as 5/19 patients received the maximum score. In the MSTS score, 1/19 patients scored the maximum, indicating minimal item redundancy. There were no minimum points in either of the instruments. The Spearman correlation coefficient was 0.588 (p = 0.008), indicating strong correlation between the two instruments.
Clinical Outcome
A total of 19 lower-limb STS patients surgically treated between 2002 and 2015 met the inclusion criteria and participated in the study. All patients had undergone limb-sparing tumor resection, except in one case of lower-leg rotationplasty. In rotationplasty, the lower leg is rotated 180 degrees and reattached to the femur following resection of the knee joint for a distal femoral STS.
The follow-up period ranged from 6 months to 12 years and 10 months (average 2 years and 11 months, median 1 year and 11 months). Data on demographics, tumor histology, surgical and oncological treatment, complications, and oncological outcome were collected from patient records (Tables 1 and 2).
Descriptive characteristics.
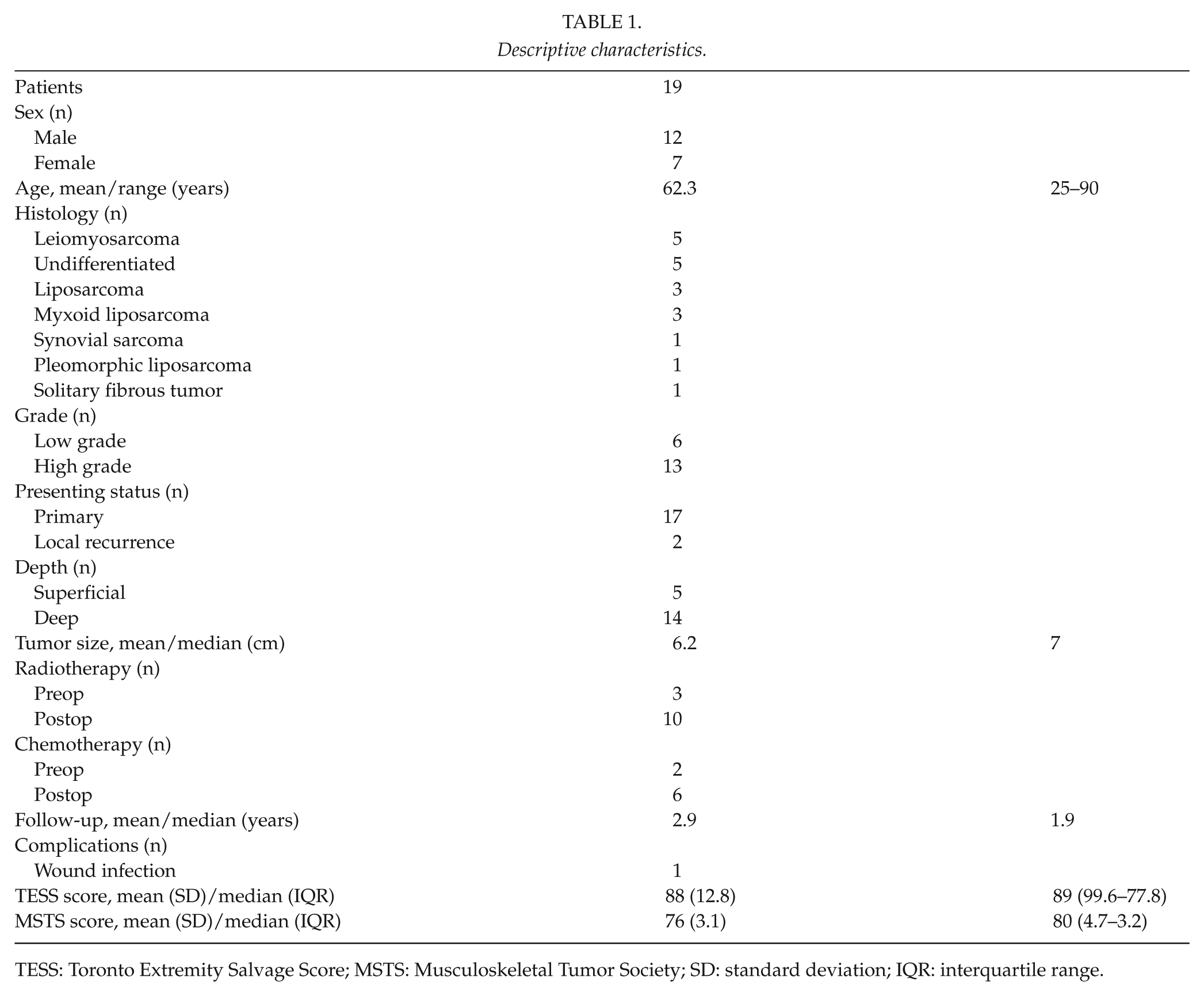
TESS: Toronto Extremity Salvage Score; MSTS: Musculoskeletal Tumor Society; SD: standard deviation; IQR: interquartile range.
Surgical and functional outcomes.
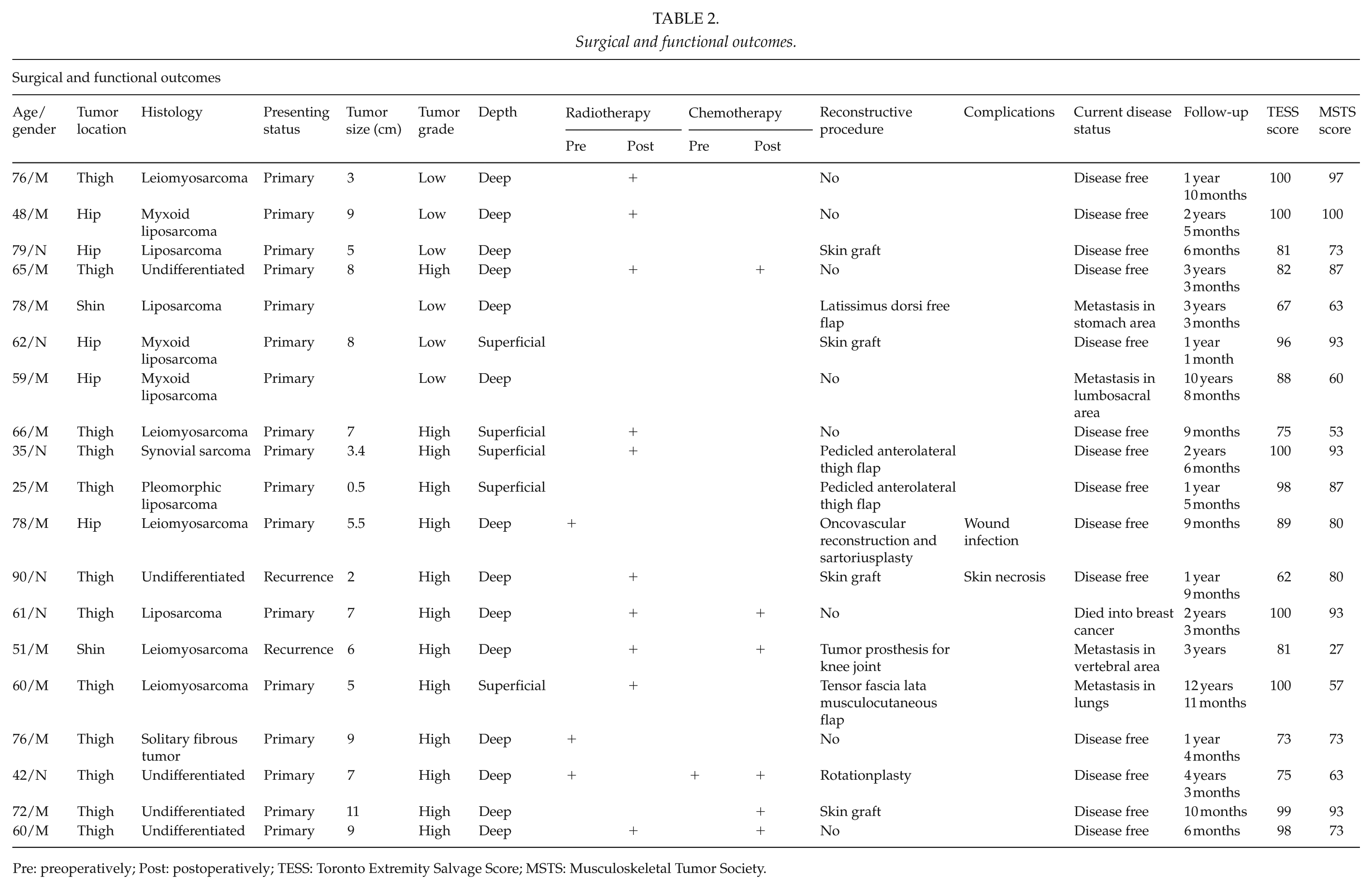
Pre: preoperatively; Post: postoperatively; TESS: Toronto Extremity Salvage Score; MSTS: Musculoskeletal Tumor Society.
Eight wounds were closed directly and four wounds were closed using split-thickness skin grafts (STSG). In seven patients, tumor resection resulted in defects requiring reconstruction. Two pedicled anterolateral thigh flaps were used and one each of pedicled musculocutaneous tensor fascia latae flap and free latissimus dorsi muscle flap with STSG. One patient underwent vascular reconstruction of the inguinal vessels, and the reconstructed vessels were covered with a sartorius muscle transposition followed by direct skin closure. One patient had above-knee amputation and rotationplasty, which entails reattaching the lower leg to the thigh stump using microvascular technique. One patient required a tumor prosthesis for knee joint reconstruction (Table 2). In total, 14 of 19 patients received oncological therapy (Table 2).
In total, 14 of 19 patients were disease free at a mean follow-up of 2 years and 11 months after surgery (range, 6–51 months). Two patients experienced local recurrence of sarcoma, and five patients had metastasis.
One revision and skin graft in the STSG group was performed due to skin graft loss. One patient suffered from a postoperative wound infection after tumor excision, oncovascular reconstruction, and sartorius muscle transposition. In this case, revision and reconstruction with a gracilis muscle flap was performed.
Functional Outcome
TESS and MSTS results are provided for each patient in Table 2. The overall mean TESS was 88 (standard deviation (SD), 12.8) and the overall mean MSTS score was 76 (SD, 3.1). The overall median TESS was 89 (interquartile range (IQR), 99.6–77.8) and the overall median MSTS score was 80 (IQR, 93–63). In the simple closure group (primary closure or STSG), the average TESS was 88 (range, 62–100) and the average MSTS score was 81 (range, 53–100). In the flap reconstruction group, the corresponding scores were 89 (range, 67–100) and 68 (range, 27–100), respectively.
Discussion
This study revealed that the Finnish versions of the TESS and MSTS questionnaires are suitable and adequate tools for measuring functional outcome in the Finnish population. As no problems or difficulties were reported in this pilot study, the TESS and MSTS questionnaires are recommended for functional outcome studies of lower extremity sarcoma patients in Finland. Functional outcomes varied from moderate to excellent after lower extremity sarcoma treatment in a single academic referral center.
In other studies, functional outcome was good to excellent after lower extremity sarcoma treatment using TESS or MSTS questionnaires (6, 20, 21). In a matched case–control study by Davis et al., 12 patients with amputation were matched with 24 patients treated with limb-preserving surgery for lower extremity primary STS or bone sarcoma patients. The mean TESS for the patients with amputations was 74.5 versus 85.1 for the limb-sparing patients. Only the physical function subscale of the SF-36 showed statistically significant differences, with means of 45.0 (amputation group) and 71.1 (limb-sparing group). The Reintegration to Normal Living for the amputation group was 84.4 versus 97 for the limb-sparing group (20). Another study in Canada reported on the surgical and functional outcome of 154 patients treated for malignant lower extremity STS. Treatment was by medical management in 3 patients (2%), limb-sparing surgery with vascular reconstruction in 9 patients (6%), and limb-sparing surgery without vascular reconstruction in 142 patients (92%). The functional status of patients was assessed using the MSTS score before surgery and at 6 and 12 months after surgery. There were no significant differences in the mean MSTS scores preoperatively, at 6 months, and at 1 year after surgery between the two groups. MSTS values were 27 (preoperatively), 25 (6 months), and 29 (1 year) for limb-sparing surgery with vascular reconstruction; the corresponding values were 28, 31, and 31 for limb-sparing surgery without vascular reconstruction (6). However, the limb-sparing surgery with vascular reconstruction group MSTS was clearly inferior compared with the limb-sparing surgery without vascular reconstruction group (6). It was difficult to interpret the study by Davis et al. (6), which presented the MSTS resultant total maximal score to be 30, but the MSTS values for limb-sparing surgery with vascular reconstruction were 31 at 6 and 12 months postoperatively (16). Recent personal communication has confirmed that an error was made in this study. Conversely, Davidge et al. (22) presented that flap reconstruction was associated with more postoperative impairments in MSTS and activity limitations in TESS, but did not significantly predict postoperative function or health status outcomes compared to primary closure. Saebye et al. (21) studied 128 patients who were treated with limb-sparing surgery for STS. In this study, only primary diseases for upper-limb and lower-limb sarcomas were included. No information about limb-sparing operation types and performed reconstructions was presented. The overall median TESS and MSTS scores were 94 (IQR, 81–99) and 97 (IQR, 77–100), respectively (21). In this study, the mean functional outcome was lower compared with these reports. In this study, most of the STS cases were deep tumors (73.7% of patients), which possibly decreased the overall functional outcome score. In addition, in our opinion, small data sets may be the reason for the observed lower functional outcome results observed in this study.
Functional outcome after amputation for sarcoma has been shown to be inferior compared to that of patients treated with limb-sparing protocols (20, 23, 24). However, in a meta-analysis including six high-quality studies, Mei et al. (25) reported that amputation and limb-sparing surgery provided similar functional outcome and quality of life for patients with osteosarcoma. Malek et al. (26) demonstrated improved functional outcome results in above-knee amputations compared to limb-salvage patients for aggressive musculoskeletal tumors around the knee. Reintegration to Normal Living Index scores was higher in the limb-sparing surgery group compared to amputation, but TESS values were similar in both groups (26). Ladlow and colleagues examined 100 procedures in a retrospective study of rehabilitation outcomes from a UK military complex trauma rehabilitation center (36 unilateral amputations, 43 bilateral amputations, and 21 single-limb salvages). The unilateral amputation group walked significantly further in 6 min (564 ± 92 m) than the limb-salvage group (483 ± 108 m) and the bilateral amputation group (409 ± 106 m). In addition, the limb-salvage group was less capable of running independently compared with all amputee groups. One explanation for the functional advantage in the amputation groups over the limb-salvage group is recent advances in prosthetic design and technology (27, 28). It is noteworthy that the study only presented data on functional results. Only one amputation patient was included in our study; this patient additionally underwent primary rotationplasty. While functional outcome was lower than overall TESS and MSTS results, comparison is difficult.
To investigate functional outcome in Finnish STS patients, we used (according to well accepted guidelines) translated, culturally adapted, and linguistically validated Finnish versions of TESS and MSTS outcome measures. This is a strength of this study. The results showed that the pre-final versions of the questions could change during the translation process. There were some difficulties encountered in the translation process. These discrepancies were duly addressed by the steering group. This reflects the essence of the adaptation of the multi-step translation process and the content of the form to the culture. The results are presented together with preliminary psychometric analyses for floor and ceiling values and convergent validity. The main weakness of this pilot study is that few patients were included in the analysis. Also, no data on preoperative functional outcome was available due to study design. In addition, a wide variety of reconstructive methods were used for the patients that required reconstruction after limb-sparing resection. Prospective study settings with at least two different time points would have provided data on the change in outcomes. However, a prospective design was not considered as an option in this pilot study; this study was planned as a cross-sectional study.
Future research directions include functional outcome and health-related quality-of-life assessment of lower extremity sarcoma patients after limb salvage in a larger cohort in Finland. Future studies should also include data on preoperative functional outcomes and a control group. In addition, future research should determine if there is any change in the functional outcomes during a long-term follow-up period.
Conclusion
Treatment of lower extremity STS is challenging. Depending on the extent of the defect, treatment options may include need for reconstructive procedures. The present pilot study shows that the translated TESS and MSTS questionnaires are suitable and adequate instruments for measuring functional outcome of lower extremity STS patients in the Finnish population. Functional outcomes vary from moderate to excellent after treatment. Previous studies have found that functional outcome after amputation for sarcoma is inferior or comparable to that of limb-salvage surgery. In lower-limb STS patients, decreased functional outcome is expected after limb-salvage surgery with microvascular reconstruction, possibly because this reconstruction method is often used for extensive defects.
Supplemental Material
Supplementary_material_(1) – Supplemental material for Functional Outcome After Lower Extremity Soft Tissue Sarcoma Treatment: A Pilot Study Based on Translated and Culturally Adapted Measures
Supplemental material, Supplementary_material_(1) for Functional Outcome After Lower Extremity Soft Tissue Sarcoma Treatment: A Pilot Study Based on Translated and Culturally Adapted Measures by G. Kask, I. Barner-Rasmussen, J. Repo, C. Blomqvist and E. Tukiainen in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
We would like to thank Saara Haapasaari for her contribution in data collection. This study was performed in accordance with the Helsinki Declaration as revised in 2013.
Data Statement
All data are available from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful for financial support from the Competitive Research Funding of Helsinki University Hospital and the Finnish Cancer Society. The funding sources had no involvement in conducting the research or preparation of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.