
Abstract
Background and Aims:
Simulation-based training in laparoscopy can improve patient safety and efficiency of care, but it depends on how it is used. Research in medical education has moved from demonstrating transferability of simulation training to the operating room to how to best implement it. This study aims to investigate how simulation-based training in laparoscopy has been implemented Scandinavia.
Material and Methods:
An online survey was sent out to medical doctors at surgical, gynecological, and urological departments at 138 hospitals in Denmark, Norway, and Sweden. The questionnaire included questions on respondents’ baseline characteristics, opinions, access, and actual use of simulation-based training in laparoscopy.
Results:
In total, 738 respondents completed the survey. Of these, 636 (86.2%) of respondents agreed or strongly agreed that simulation-based training in laparoscopy should be mandatory. A total of 602 (81.6%) had access to simulation-based training in laparoscopy. Of the total 738 respondents, 141 (19.1%) were offered structured training courses, 129 (17.5%) were required to reach a predefined level of competency, and 66 (8.9%) had mandatory courses in laparoscopy. In all, 72 (9.8%) had never used simulation-based training in laparoscopy.
Conclusion:
An implementation gap in laparoscopic simulation-based training still exists in Scandinavia. Simulation equipment is generally available, but there is a lack of structured simulation-based training.
Keywords
Introduction
Minimal invasive surgery and laparoscopy, in particular, has become the first choice for most operative procedures today (1). However, laparoscopy requires a unique set of skills to master the technique. Simulation-based training is an effective method of acquiring these (2, 3). Simulation training has shown to be transferable to the clinical setting and has the potential of improving patient safety and efficiency of care (4, 5). The beneficial effects of simulation-based training are, however, dependent on how it is implemented (6, 7). As we know that simulation training is effective, research in medical education has moved from demonstrating the effect of simulation training to exploring how to best integrate simulation training in current surgical training curricula (8). When including simulation-based training in surgical curricula, it should be based on proficiency-based learning and deliberate practice (8, 9).
Despite the mounting evidence supporting simulation training in laparoscopy, simulation training is only mandatory in few countries (10, 11). Furthermore, there is a global lack of access to simulation-based training, and surgeons’ access to simulation equipment is far from sufficient (12). Therefore, most surgical trainees still develop their skills by practicing on patients during supervised procedures (12). However, operating on patients without practicing beforehand is becoming unacceptable, to both the general public and the surgical societies (7). There has been an increased focus on implementing simulation training in laparoscopy as a part of the surgical curriculum for several surgical specialties (13). Previous studies have tried to explore the use of simulation-based training in laparoscopy (12). However, the use of simulation-based training as a part of surgical training is still unclear. The study objective was to get an overview of how simulation-based training in laparoscopy has been implemented in Scandinavia.
Material and Methods
Respondents
To explore how laparoscopic simulation training is implemented in Scandinavia, we aimed to include at least 600 respondents from Denmark, Norway, and Sweden, 200 from each country. We included medical doctors from departments of general and gastrointestinal surgery, gynecology, and urology. Both female and male respondents were included and respondents with different levels of proficiency in laparoscopic surgery. There were no age limits. Respondents who had only partially completed the survey when data collection ended were excluded.
Survey Development
We developed the survey in English using an online survey tool, SurveyXact (Ramboll, Copenhagen, Denmark). The survey was constructed using recommendations for developing surveys in healthcare (14). The questionnaire provided descriptive information on the respondent, such as demographics, specialty, and surgical experience together with questions regarding their opinions, access, and actual use of simulation-based training in laparoscopy. Using a 5-point Likert scale, respondents were asked to choose which level they agreed on statements regarding the importance of simulation-based training in laparoscopy. They were also asked if the training was structured in accordance with educational principles of deliberate practice and proficiency-based learning.
Survey Distribution
A pilot test was sent out to members of the research group and a few external surgical residents to make sure that the survey was understandable and to help identify possible threats to data integrity. To distribute the survey online, we made primary contact to leading consultants via phone-calls or personal emails who agreed to participate on behalf of their department. We did not use financial incentives (14). We started contacting head of departments on 4 April 2016. The leading consultants received an instructional email with a link to the survey. They were asked to forward the link to all the doctors at their department. Respondents registered their name and email address when they completed the survey. Respondents were informed that only the first author had access to research data and that results would be anonymous. Reminder emails were sent to the leading consultants and directly to respondents who only partially filled out the survey. We sent out reminder emails every month to increase the response rate (14). The study ended on 22 September 2016.
Statistical Analysis
Responses were analyzed and figures were made using descriptive statistics in Microsoft Excel (Microsoft Excel 2016, Microsoft Corporation, Seattle, WA, USA).
Results
Respondents
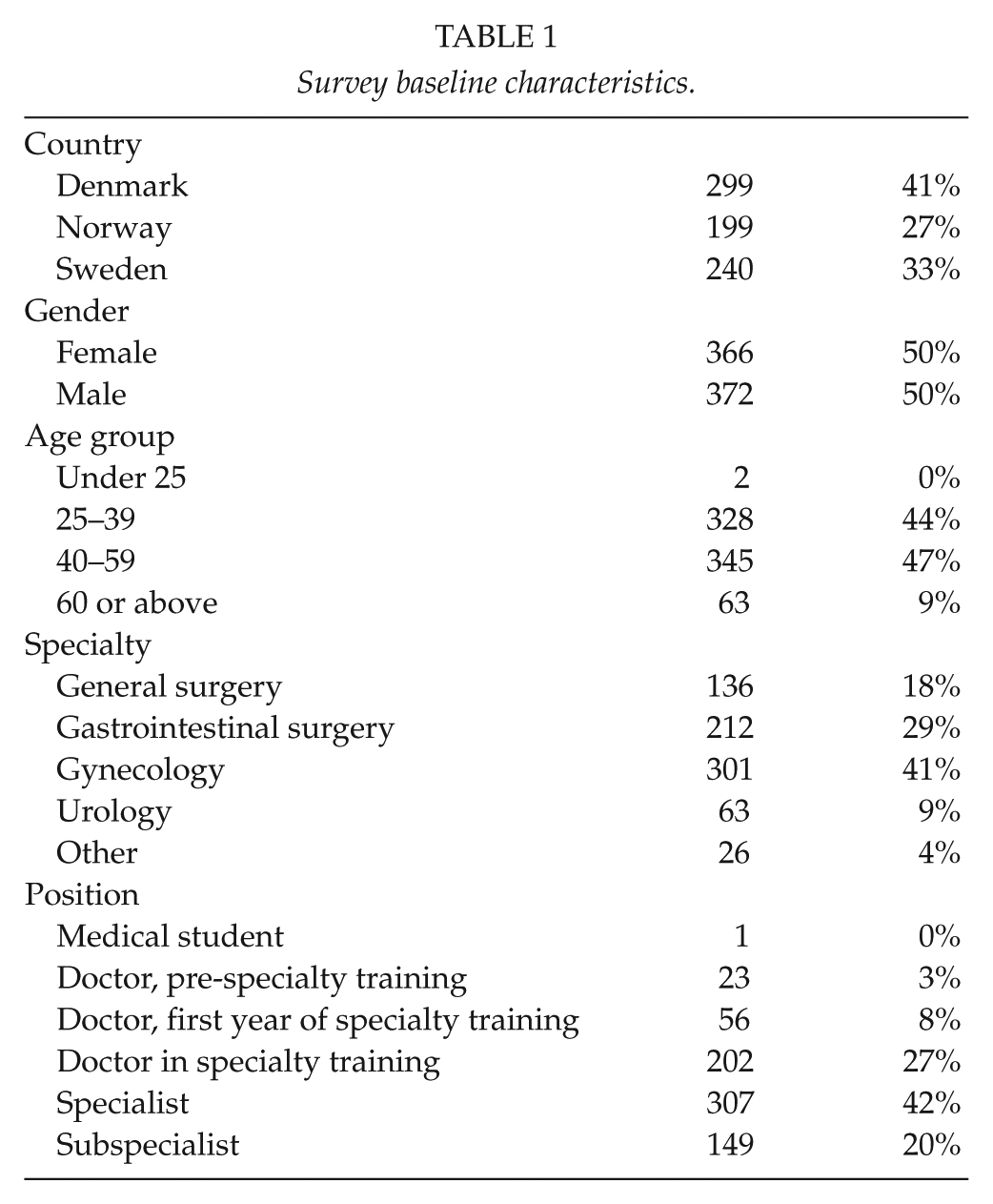
In total, 266 departments in 138 hospitals in Denmark, Norway, and Sweden were contacted. In all, 738 respondents from 128 hospitals completed the survey. All administrative hospital regions in the three countries were represented. Respondents included doctors from departments of general surgery, gastrointestinal surgery, gynecology, urology, and other surgical specialties. One medical student employed at a surgical department also completed the survey. Baseline respondent characteristics are shown in Table 1.
Survey baseline characteristics.
Opinions of Simulation-Based Training
There was a high level of agreement among respondents to integrate simulation training in laparoscopy to surgical practice (Fig. 1). In all, 636 (86.2%) respondents reported that they agreed or strongly agreed that simulation training should be mandatory. Furthermore, 469 (63.6%) agreed or strongly agreed that surgical trainees should pass a test on a simulator before being allowed to operate on patients.
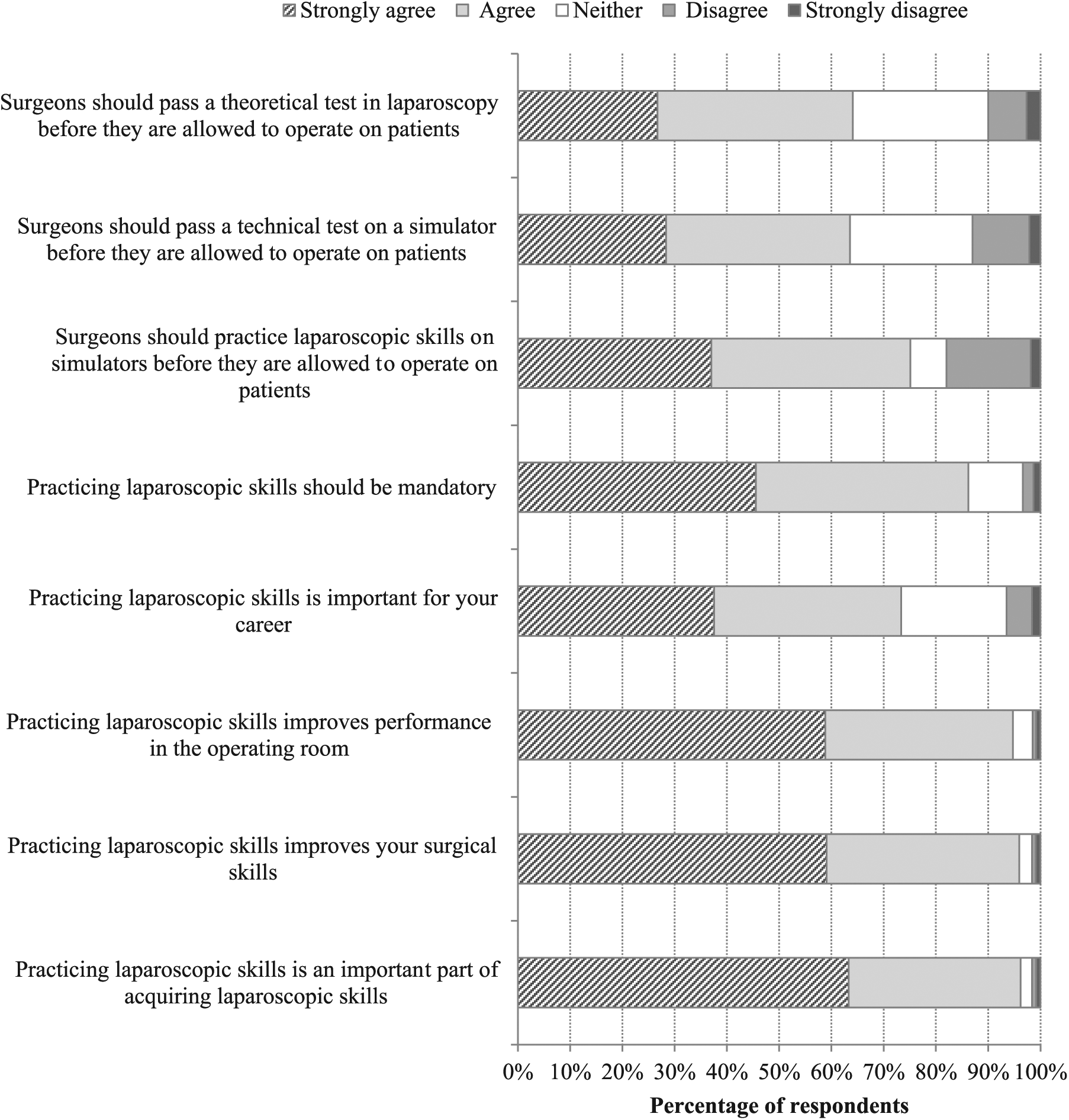
Opinions on simulation-based training in laparoscopy.
Access to Simulation-Based Training
In total, 602 (81.6%) reported that they had access to simulation-based training in laparoscopy and 136 (18.4%) reported that they did not have access. In total, 550 (74.5%) had access to training in a skills lab and 219 (29.7%) had access to training off-site. Out of this, 167 respondents had access both in a skills lab and off-site. Box-trainers and virtual reality simulators were the most frequently available training modalities (Fig. 2). Out of the 219 respondents that had access to off-site training, this was either at work (122, 55.7%), at home (67, 30.6%), at another hospital (46, 21.0%), or other (33, 15.1%). Overall, 141 (19.1%) of respondents were offered structured training courses, 129 (17.5%) were required to reach a predefined level of proficiency, and 66 (8.9%) had mandatory courses in laparoscopy.
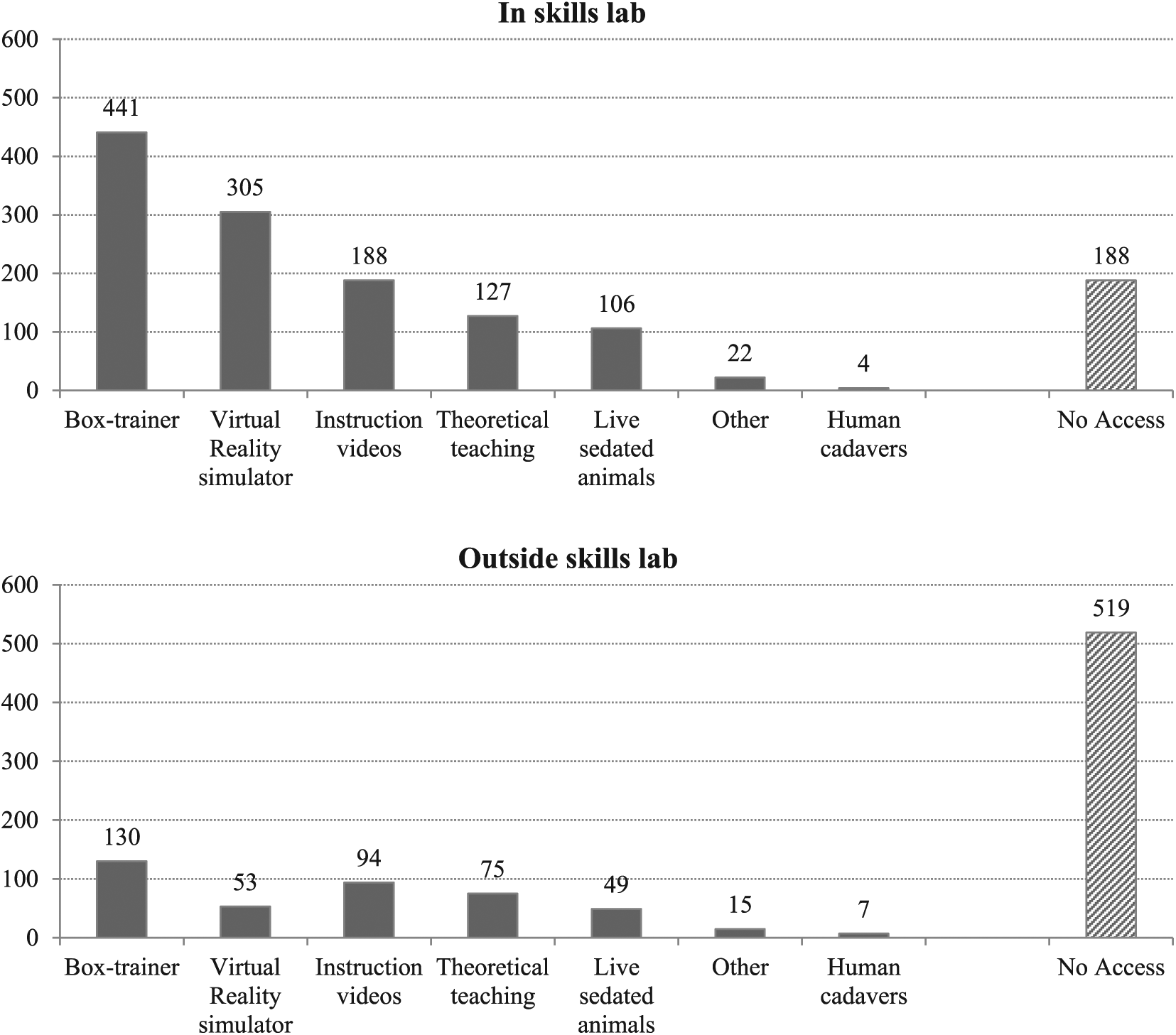
Available training instructions in laparoscopy.
Actual Use of Simulation-Based Training
A total of 666 (90.2%) respondents reported that they practiced laparoscopic skills and 72 (9.8%) respondents had never used any kind of simulation-based training in laparoscopy. The respondents that had practiced were asked whether they have done this in a skills lab, off-site, or both. In total, 630 (85.4%) had practiced laparoscopic skills in a skills lab and 334 (45.3%) had practiced off-site. Out of this, 298 (40.4%) had used simulation-based training in laparoscopy both in a skills lab and off-site. Overall, 13 (1.8%) and 16 (2.2%) respondents practiced their laparoscopic skills on a weekly basis in a skills lab and off-site, respectively, and 390 (52.8%) respondents practiced laparoscopic skills in a skills lab once or less than once a year. The majority of training sessions lasted for 1 h or less (398, 59.8%). An overview of respondents training patterns; session frequencies and durations, can be found in Fig. 3. Respondents that had not practiced laparoscopic skills were asked about the reasons for not practicing. Besides no skills lab available, lack of time was the most frequent reason for not using simulation-based training for laparoscopic skills acquisition.
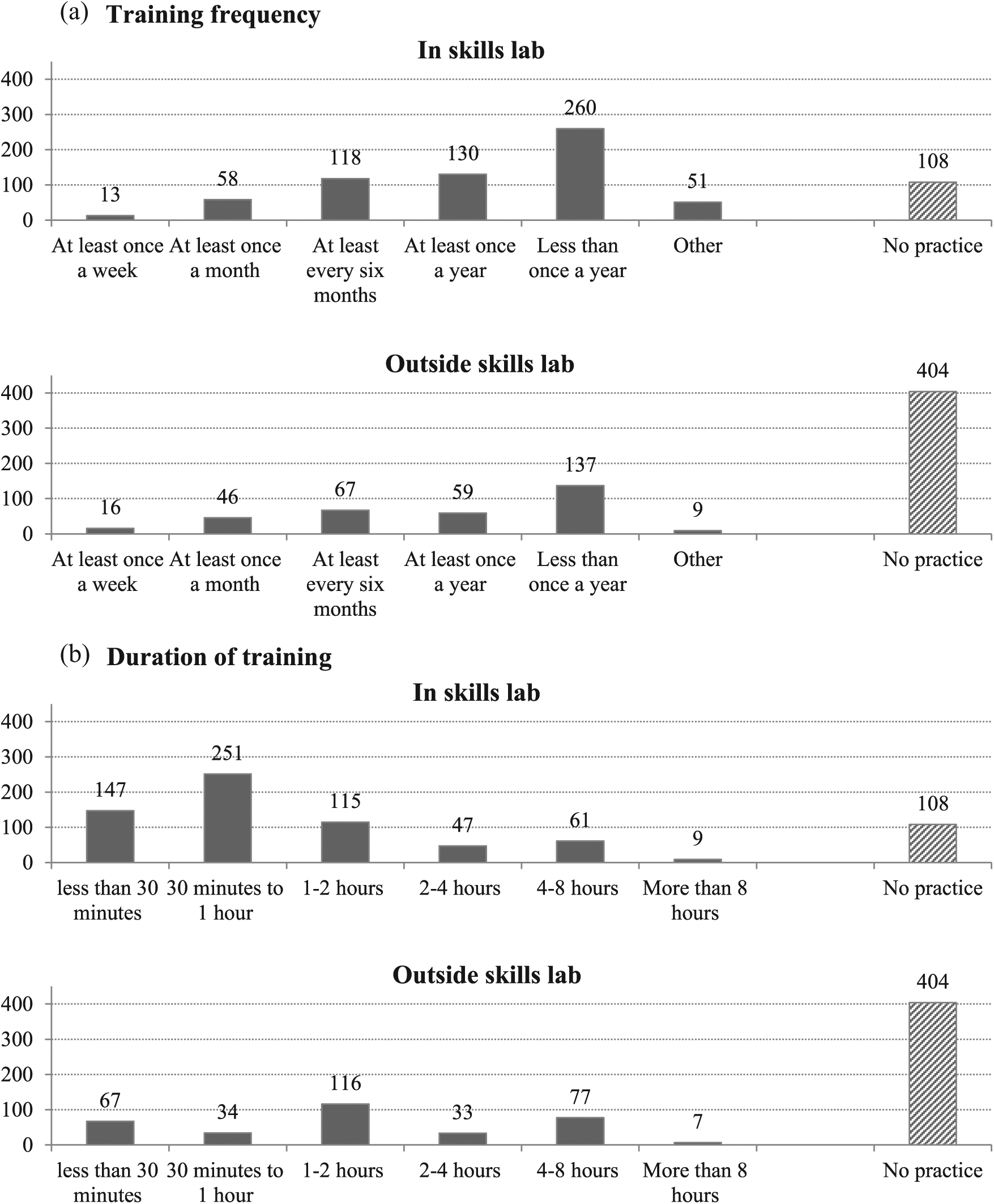
Overview of training patterns.
Discussion
To investigate the implementation of simulation-based training in laparoscopy in Scandinavia, we used a survey tool to map the opinions on, access to, and actual use of laparoscopic simulation. In total, 738 respondents from 128 different hospitals in Denmark, Norway, and Sweden completed the survey. Respondents agree that surgical simulation is important for acquiring laparoscopic skills and should be mandatory. Even though the majority of our respondents had access to simulation training, they did not practice very often, and training did not follow recommended educational principles.
Opinions on Simulation-Based Training
Our results illustrate a high level of agreement in the opinions of simulation-based training in laparoscopy. Respondents agreed that simulation-based training should be mandatory. There is, however, a gap between the strong opinions in favor of including surgical simulation in laparoscopy as a compulsory part of surgical training and the actual use of simulation training. It has been proposed that simulation-based training in laparoscopy is most effective when integrated as a mandatory requirement in surgical training (15, 16). Our results confirm that the implementation of mandatory laparoscopic skills training as part of surgical curriculums still remains a problem in Scandinavian countries.
Access to Simulation-Based Training
When asked about access to training, 550 (74.5%) and 219 (29.7%) responded that they had access to practice laparoscopy in a skills lab or off-site, respectively. Both numbers are higher than compared to previous reports where the largest reported numbers for access to a simulator in a skills lab and off-site is 47% and 20%, respectively (2,12,17). However, a Dutch study from 2015 reports that 48%, 66.7%, and 69% of urology, general surgery, and gynecology residents, respectively, had access to laparoscopic simulation training in a skills lab (18). In addition to obvious advantages to off-site training such as increased availability and cost-effectiveness (19), we believe that the amount of research in the field of surgical simulation has contributed to the high availability to training. Furthermore, this also fits well with the increasing political pressure to increase the availability of simulation training in order to increase patient safety (7).
Use of Structured Skills-Training
In our study, there is a gap in the use of simulation training in laparoscopy compared to the availability where only 13 (1.8%) respondents practice laparoscopic skills in a skills lab and 16 (2.2%) practice off-site on a weekly basis. These tendencies have also been described in other studies (12, 17, 18). In one of the reports only 19% had practiced laparoscopic skills on a simulator for more than 6 h the preceding year and 46% had not used one at all (12). Another report states that the majority (66%) had used a simulator for less than 3 h during the preceding year (17).
In our study, only 66 (8.9%) of the total study population attended mandatory courses in laparoscopy. This could suggest that how and when people train is not only depending on availability but also more on the curricular requirements (19). A laparoscopic training curriculum should include requirements based on proficiency-based training (6). Proficiency-based training includes assessment and testing and has been recommended for laparoscopic simulation training (9). In our study, most training activities was not structured nor organized according to principles of proficiency training as only 141 (19.1%) of respondents were offered structured training courses and 129 (17.5%) were required to reach a predefined level of proficiency. One of the studies cited above report that 10.7%, 15%, and 37.2% of trainees, depending on surgical specialty, were required to practice until proficiency on a simulator (18). Another educational principle which has been recommended for laparoscopic simulation training is that of distributed practice (6, 19). In distributed practice, opposed to massed practice, trainees distribute their training sessions. This has shown to be effective in laparoscopic procedural skills training (20). In our study, there was in fact a tendency toward using shorter training sessions relative to that found in previous literature where majority of training sessions were longer than 1.5 h (18). We found quite the opposite that the majority (398, 59.8%) reported that the most common duration of their training sessions lasted for 1 h or less. This could be a result of an increased focus on implementing educational principles in laparoscopic simulation training, or simply due to lack of time to train as repeatedly illustrated in both the current and previous studies (12, 17, 18).
Limitations
The survey was developed using guidelines for improving response rate and reducing biases (14). Conducting surveys of physicians is, however, challenging, and response rates are normally 10% lower than other surveys (21, 22). Because the survey was sent out as part of an email and respondents registered when participating in the survey, we were not able to detect the exact response rate. However, choosing this method allowed us to include 738 medical doctors, which is more than in similar studies (12, 18). Of the 1919 specialists and doctors in specialization in Norway in surgery, gynecology, and urology, we included 198, which corresponds to 10.3% (23). The latest report from Denmark states there were 1334 medical doctors in total in general surgery, gynecology, and urology in 2013 (24). We collected responses from 298 (22.3%) of them. It is important, however, to consider that there are also medical doctors working as locums in non-training positions at the hospital departments which would falsely increase our response rate. There is also a potential selection bias if the department leader did not forward the survey to all department doctors, although they were carefully instructed to do so.
To ensure questions were relevant to the population, we conducted a pilot study with doctors from the research center. They received the same email as our respondents, and after completing the survey, the first author went over the survey to identify potential misinterpretations and threats to data integrity. Yet, it is likely that the response rate could be increased both by allowing anonymous participation and contacting each medical doctor individually (14).
Recommendations
The costs of simulators have been a key criticism of simulation-based training (25). This has led to an increased focus on developing affordable and more accessible training modalities such as box-trainers which are both affordable, portable, and accessible (26). Box-trainers have shown to be effective and even favored by trainees when compared to virtual reality simulators (27). However, we found that medical doctors still do not practice their laparoscopic skills even though they have access to such box-trainers. How do we get these medical doctors to train? We suggest that the first step is to make laparoscopic simulation training mandatory (16). Currently, training requirements vary in the Scandinavian countries both between the individual countries and the different specialties. In Denmark, simulation-based training is seen as an important training modality in the acquisition of surgical skills in all three specialties, and all trainees attend one mandatory skills course in basic laparoscopy on sedated pigs during their specialty training. However, it is only gynecologists who are required to pass a procedural test on a virtual reality simulator. In Sweden, a simulation-based course is offered and a test exists; however, simulation-based training is not a mandatory requirement to become a specialist. In Norway, official requirements for residents in surgery and urology include participation in a mandatory laparoscopic skills course on box-trainers and sedated pigs, but there is no practical test. For gynecologists in Norway, mandatory simulation-based training is not required as part of their specialty training. Thus, the use of simulation-based training in laparoscopy in Scandinavian countries is to a high degree up to each hospital, department, and even trainees. This is also reflected in the findings of this study, as only 66 (8.9%) of the total study population attend to mandatory training courses. In addition, our results show that the majority support compulsory training courses in laparoscopy and we believe that implementing such training courses would be positively received among surgical trainees. Duty hour requirements in the Scandinavian countries are low, which lead to a reduced operative experience (28). Less time in the operating room may be overcome by simulation-based training without compromising patient safety (29). Implementing mandatory simulation-based training may also reduce the number of errors during surgery (30). Reducing errors increases both patient safety and can reduce costs. All these factors should be powerful motivators for implementing mandatory simulation training.
Despite the advantages of implementing mandatory training, mandatory training alone is not enough to ensure the acquisition of laparoscopic skills. In addition to available training facilities, we are dependent on both motivated trainees and commitment from faculty in order to implement a successful laparoscopic skills curriculum (6). The surgical curricula also need to be based on sound educational principles (6, 20). Instructional design of training courses should allow for several training sessions a week, training until proficiency, feedback, and the use of evidence-based assessment tools (8, 9, 11). The implementation of a such a course in laparoscopy has been shown to be feasible at Copenhagen Academy for Medical Education and Simulation and is mandatory for all gynecological residents in Denmark.
Conclusion
There is an implementation gap in surgical simulation in laparoscopy in Scandinavia. Laparoscopic surgeons across different specialties agree that simulation-based training should be mandatory before operating on patients under supervision. Furthermore, there is need for research on how to improve implementation of simulation-based training in laparoscopy.
Footnotes
Acknowledgements
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request. Equipment was provided by Copenhagen Academy for Medical Education and Simulation, Capital Region, Copenhagen, Denmark.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr E.T. reports non-restricted educational grants from Johnson & Johnson during the conduct of the submitted work. K.F., Dr I.G., and Dr L.K. have no conflicts of interest or financial ties to disclose.
Ethical Approval
The Regional Ethics Committee in Denmark decided that ethical approval was not required in accordance to Danish regulations (H-4-2014-090). Ethical approval from Norway and Sweden was not needed. The study was also reported to the Danish data protection agency (REG-77-2014) as the study was conducted in Denmark, which was sufficient to allow for data collection in Sweden and Norway as well.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Anita and Tage Therkelsens Fond, Knud and Edith Eriksens Mindefond, Else and Mogens Wedell-Wedellborgs Fond, and the University of Copenhagen.
Informed Consent
Participation was voluntary and did not involve patients. Respondents gave their written informed consent when responding to the instructional email.