
Abstract
Background and Aims:
Over the past decades, laparoscopic colorectal surgery has become widely used for various indications. Large multicenter studies have demonstrated that laparoscopy has clear advantages over open surgery. Compared to open procedures, laparoscopy decreases perioperative blood loss, post-operative pain, and hospitalization time, but provides equivalent long-term oncological and surgical results. Most studies have been conducted in high-volume institutions with selected patients, which may have influenced the reported outcome of laparoscopy. Here, we investigated the primary outcome of all laparoscopic colorectal resections performed between 2005 and 2015 in a low-volume center.
Materials and Methods:
This retrospective study included bowel resections performed between 2005 and 2015 in the Lapland Central Hospital. Data were retrieved from electronic patient registries, and all operations that began as a laparoscopy were included. Patient records were investigated to determine the primary surgical outcome and possible complications within the first 30 days after surgery.
Results:
During 2005–2015, 385 laparoscopic colorectal resections were performed. Indications included benign (n = 166 patients, 43.1%) and malignant lesions (n = 219 cases, 56.9%). The median patient age was 68 years, and 50.4% were male. The median American Society of Anesthesiologist score was III, and 48.5% of patients had an American Society of Anesthesiologist class of III or IV. The median hospital stay after surgery was 6 days (interquartile range: 3.8). The conversion rate to open surgery rate was 13%. The total surgical complication rate was 24.2%, and re-operation was required in 11.2% of patients. A total of 26 patients had anastomotic leakage, of which 16 required re-operations. The 30-day mortality was 0.8%.
Conclusion:
Our results showed that laparoscopic colorectal surgery in a peripheral hospital resulted in primary outcome rates within the range of those reported in previous multicenter trials. Therefore, the routine use of laparoscopic colorectal resections with high-quality outcome is feasible in small and peripheral surgical units.
Keywords
Introduction
Laparoscopic surgery is currently commonly practiced for treating various diseases that demand a bowel resection. Compared to open surgery, laparoscopy provides reduced intraoperative bleeding, reduced post-operative pain, and allows for shorter hospitalizations after surgery (1, 2). In addition, compared to open surgery, laparoscopy has shown reduced overall morbidity and earlier bowel function (3), with equivalent long-term oncological results (4–6).
Although the overall post-operative morbidity is reduced with laparoscopy, 13%–34% of patients have at least one post-operative complication (1, 7). In addition, previous multicenter trials have reported conversion rates of 4%–15% (8, 9) and for rectal surgery, conversion rates up to 17% were recently reported (5). Re-operations were required in 7%–11% of patients (9, 10) and anastomotic leakage developed in 4%–7% of patients (1, 9).
Enhanced recovery after surgery (ERAS) protocols have been developed to provide further improvements in post-operative treatments and to decrease complications (1, 9). ERAS protocols were also shown to be safe and efficient among older patients (11). Previous trials using ERAS protocols showed a median primary hospitalization of 5–6 days after colorectal resection (1, 8–10), and discharge was safe after the second post-operative day for selected patients with no complications (12). However, re-admission rates were reported to be 13%–14% (8, 10). According to a meta-analysis, the combination of ERAS and laparoscopy decreases hospital stay and major morbidity when compared with open surgery, but the effect on morbidity was due to laparoscopy rather than ERAS (13).
Most randomized trials are multicenter studies performed in high-volume institutes with highly specialized operation units and operative personnel. In addition, different exclusion criteria were used among different trials, such as comorbidity (based on the American Society of Anesthesiologist (ASA) class), the probability of conversion, and age over 80 years (1, 5, 9). These factors may have influenced the reported outcomes of laparoscopic colorectal resections. It can be hypothesized that the surgical results may change, once laparoscopic resections become a common practice in smaller institutions, and when studies include unselected patients.
The Lapland Central Hospital is a small, peripheral teaching hospital in Rovaniemi, in the northern part of Finland with a patient population of about 118,000. The area served by the Hospital is very large with the longest distance from the peripheral villages to the hospital being around 450 km. The Lapland Central Hospital is the only surgical unit in the area and began to perform laparoscopic bowel resections in 2005 and laparoscopic colorectal cancer surgery in 2008. Over the past 5 years, between 50 and 60 laparoscopic colorectal resections have been performed per year.
The purpose of this study was to examine the primary outcome of laparoscopic colorectal resections in this low-volume institution.
Methods
Patients and data collection
The operative records for laparoscopic bowel resections performed in the Lapland Central Hospital are stored in a prospectively maintained database. We retrieved records for the resections performed between December 2005 and December 2015 from the electronic patient registry. All colorectal resections that began as a laparoscopy were included in this study. Operative records were used to determine a perioperative ASA score. We also reviewed patient records to determine the index hospital treatment period and to identify any possible re-admissions within the first 30 days after the operation. Furthermore, we identified all possible re-admissions within 30 days after re-discharge. All radiologically diagnosed intra-abdominal abscesses near the anastomosis site were recorded as anastomotic leakages.
Surgical Procedures
Preoperative mechanical bowel preparation was performed with 4 L of a bowel cleansing agent for all patients, except those with a right-side hemicolectomy or ileocecal resection; the latter patients received no preoperative preparation. All patients without allergies received a single dose of cefuroxime, based on body mass index (BMI; 1.5 g for BMIs under 30 kg/m2 or 3.0 g for BMIs over 30 kg/m2), and 1.0 g metronidazole during induction of general anesthesia. Patients with an allergy to cefuroxime or metronidazole received other, individually prescribed antibiotic prophylactic medications. Trocar placement was based on preoperative planning and the preferences of the surgeon. Bowel anastomosis was performed and a specimen was removed through the extension of the umbilical trocar incision or through a separate incision made to the right or left lower abdominal quadrant, depending on the operative site. To prevent post-operative thromboembolic episodes, all patients received mini-heparin treatments, which were begun at 6 h from the end of the operation, unless the surgeon decided otherwise. Anticoagulation treatment was discontinued after 4 weeks in patients treated for malignant disease and was discontinued once the patient was fully mobilized in patients treated for non-malignant disease.
Perioperative Care Protocol
An ERAS program was implemented in all cases, unless the operating surgeon decided otherwise. The ERAS protocol included a preoperative carbohydrate drink, removal of the nasogastric tube after the operation, early oral feeding, active mobilization, and discharge after the patient could tolerate fluids and a soft diet, and when adequate pain relief could be achieved without intravenous drugs. Outpatient visits were only planned in mandatory cases, and no routine post-operative controls were planned, except surgical cancer surveillance as indicated.
Statistical Analysis
Statistical analyses were performed with IBM SPSS Statistics 23.0 (IBM corp., Armonk, NY). Group statistics for continuous variables were calculated with SPSS, and group comparisons were performed with the Mann–Whitney U test due to its skewed distribution. A Cox proportional hazards model with backward selection was used for multivariate analyses with the following covariates: ASA class (I–II/III–IV), conversion, operative site, indication (cancer/benign), and primary enterostomy.
Results
Patient information
The patient demographics are presented in Table 1. The median age was 68 years (interquartile range (IQR): 17). A higher proportion of patients had cancer (n = 219, 56.9%) compared to those with benign disease (n = 166, 43.1%). The benign indications for bowel resection included recurrent diverticulitis (n = 91), adenomas (n = 50), inflammatory bowel disease (n = 19), endometriosis (n = 3), and three patients with other benign lesions. We found a clear difference in operative indications between genders. Bowel resections were performed to treat cancer in 50.8% of females and 62.9% of males. The median BMI was 27 kg/m2 (IQR: 6) for female and 26 kg/m2 (IQR: 5) for male.
Demographic and operative data of patients.
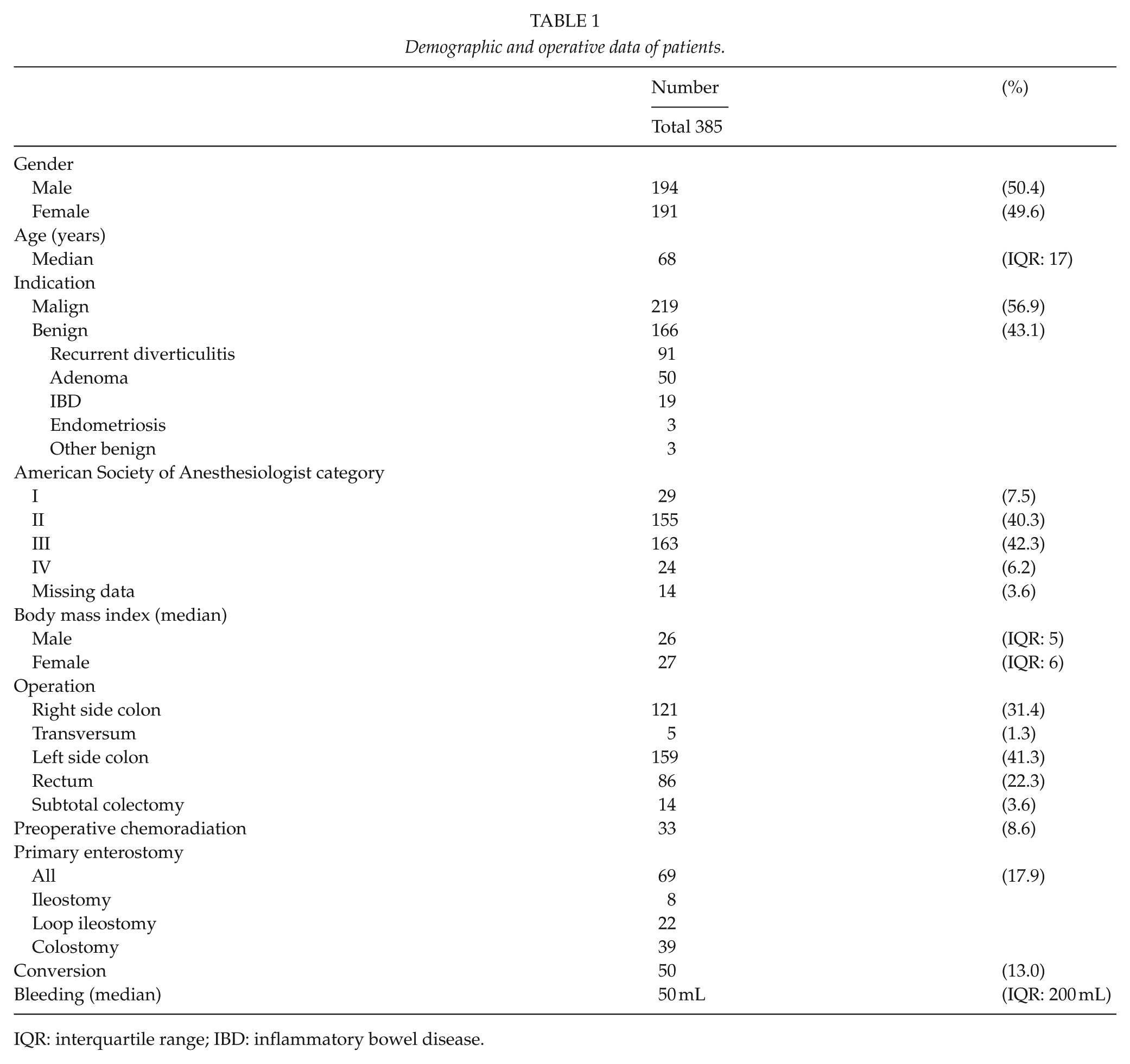
IQR: interquartile range; IBD: inflammatory bowel disease.
Operations
Between 2005 and 2010, the rate of laparoscopic bowel resections increased from 2% to 80% and has subsequently varied between 75% and 85% (Fig. 1). Among all 385 operations, 31.4% were right-side colonic (ileocecal resections or right-side hemicolectomies), 1.3% were colon transversum resections, 41.3% were left-side colon resections, 22.3% were rectal resections, and 3.6% were total or subtotal colectomies. Majority of operations (314 operations, 81.6%) were performed by three experienced colorectal surgeons each with more than 10 years of specialist experience, 41 operations (10.6%) were performed by two colorectal specialists with less than 10 years of specialist experience, and 30 (7.8%) operations were performed by surgical residents under specialist supervision. A total of 33 patients (8.6%) treated for rectal cancer had preoperative chemoradiation. Of the 69 patients (17.9%) who received primary enterostomies, 22 were loop-ileostomies, 8 were end ileostomies, and 39 were end-colostomies. Median operative bleeding was 50 mL (IQR: 200).
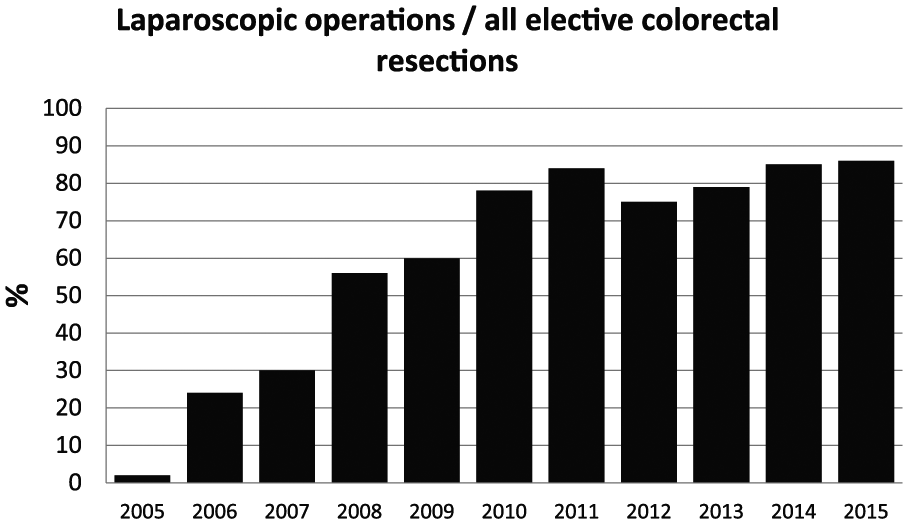
Proportion of laparoscopy in all elective colorectal resections.
Post-Operative Complications
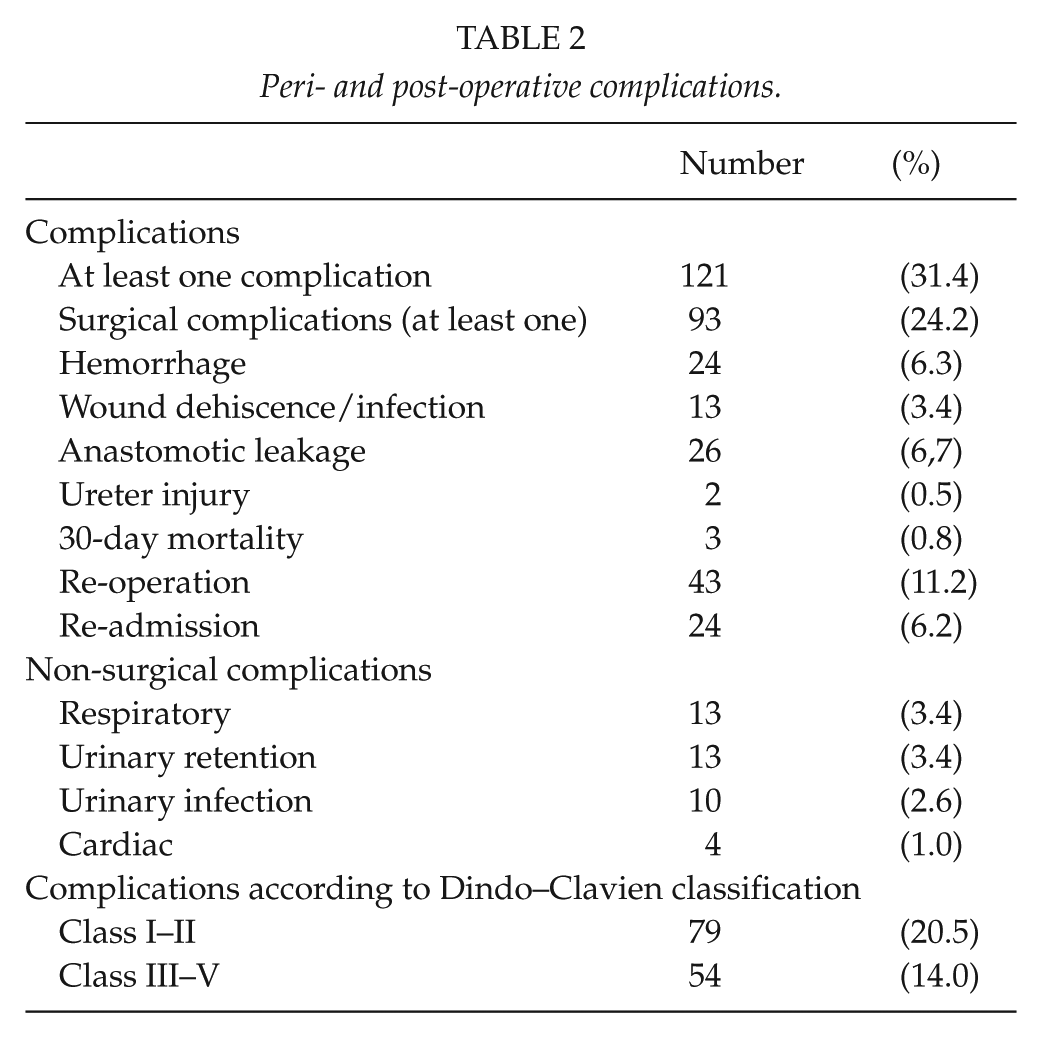
Nearly one-third of patients (n = 121, 31.4%) experienced at least one post-operative complication (Table 2). Surgical morbidity was observed in 93 patients (24.2%). The most common surgical complications were anastomotic leakage (26 patients, 6.7%), followed by hemorrhage (24 patients, 6.2%) and wound dehiscence/infection (13 patients, 3.4%). The most common non-surgical complications were respiratory complaints (13 patients, 3.4%), followed by urinary infection (10 patients, 2.6 %) and cardiac complaints (4 patients, 1.0%). In addition, 13 male patients (3.4% of all patients and 6.7% of male patients) had post-operative urinary retention and required urinary catheterization after discharge (10 patients required long-term catheterization and 3 patients required intermittent catheterization). There were no statistically significant differences in post-operative complications between those patients operated on by experienced specialists, younger specialists, or surgical residents. Over the 10-year study period, fluctuation was seen in yearly complication rates, but these were not statistically significant changes (data not shown).
Peri- and post-operative complications.
Anastomotic Leakage
The median interval between the operation and the diagnosis of anastomotic leakage was 5.5 days (IQR: 6.0). Of the 26 patients with an anastomotic leakage, 13 patients received operations on the left colon, 6 on the right colon, 6 on the rectum, and 1 had a subtotal colectomy. Of the six patients operated for rectal disease, three had received preoperative chemoradiation. To treat the anastomotic leakages, 16 patients underwent re-operations (of these, 2 were treated with an endoscopic vacuum-assisted closure), 4 patients required radiology-assisted drainage, and 6 patients received conservative treatments with antibiotics. All 16 patients who required re-operations for treating an anastomotic leakage were diagnosed before discharge. Of the other 10 patients, 4 were re-admitted due to leakage, and 2 of these required radiology-assisted drainage.
Re-Operation
Of the total 385 patients, 43 required re-operations (11.2%). Re-operations were mostly performed with open surgery (81.4%), whereas laparoscopy was used in only one case (2.3%). In total, 16.3% of re-operations were wound revision without opening the deep fascia. The most common indication for a re-operation was anastomotic leakage (n = 16 operations), followed by the need for an enterostomy revision (n = 10) and wound dehiscence or infection (n = 8). Three patients received re-operations for intra-abdominal bleeding, two for an iatrogenic ureter injury, one for an iatrogenic bowel perforation, one for a ventral hernia, and one for prolonged ileus. In addition, two patients received re-operations based on computer tomography detection of a suspected leakage, but the operation revealed an intact anastomosis. Re-operations led to an enterostomy in 10 cases; of these 5 were loop-ileostomies and 5 were end-colostomies (Hartmann’s procedure).
30-Day Mortality
The 30-day mortality was 0.8% (three patients). One patient had an iatrogenic bowel perforation, which was diagnosed and re-operated on the second post-operative day. The patient died on the 14th post-operative day due to secondary peritonitis, despite repeated laparotomies and intensive care. A second patient received an operation for a diagnostic ileocecal resection to treat end-stage cancer with multifocal liver metastases, but no intraluminal tumor observed in the colonoscopy. In addition, one patient at high risk due to preoperative liver dysfunction received an operation for right-side colon carcinoma; an intraoperative liver biopsy revealed liver cirrhosis and suspicion of an alpha-1-antitrypsin deficiency. The patient died on day 12 due to liver dysfunction.
Hospitalization And Re-Admission
The median length of stay for the primary hospitalization in the entire study group was 6 days after surgery (IQR: 3.5), and the distribution is presented in Fig. 2. The geographical region of residence (Rovaniemi vs other municipalities) had no effect on the length of stay for the primary hospitalization. Patients who received operations for cancer had significantly longer hospital stays than patients who received operations for benign indications (median 6 vs 4 days, p < 0.001; Table 2). In addition, patients with ASA class III–IV had significantly longer hospital stays (median 6 days, p = 0.036) than patients with ASA class I–II (median 4 days). Patients with primary enterostomies had significantly longer hospital stays than patients without enterostomies (8 vs 5 days, p < 0.001). Conversion also significantly affected the length of hospitalization; the median hospital stays for those without and those with conversions were 5 and 7 days, respectively (p < 0.001). The multiple regression analysis showed that only an ASA class of III–IV, a conversion, and a primary enterostomy were independent risk factors for a prolonged primary hospital stay. The median primary hospitalization for patients without post-operative complications was 4 days.
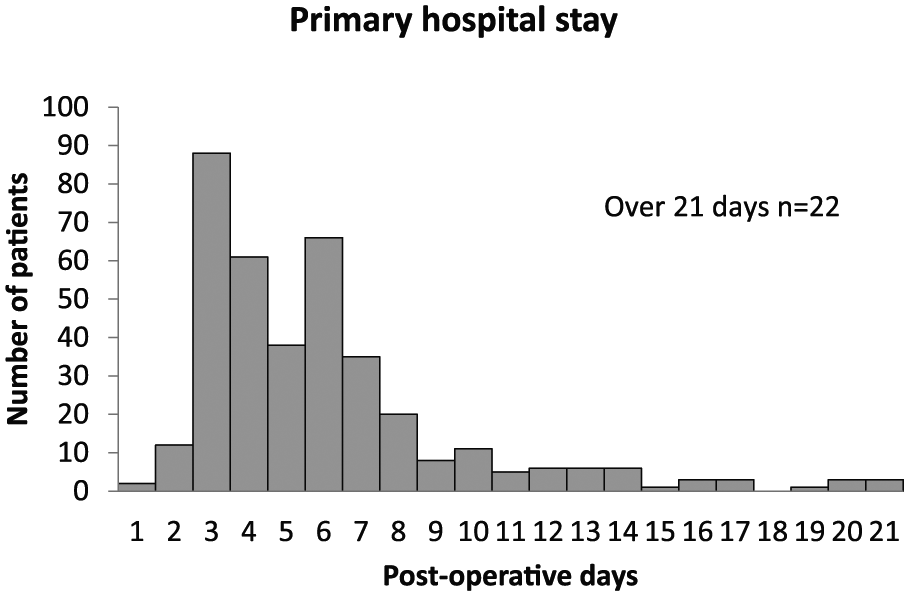
Primary post-operative hospital stay.
Out of 385 patients, 54 (median age 77 years, median ASA class III) were discharged to local, general practitioner-driven hospitals, because their overall condition required prolonged hospitalization. In this group, the median primary hospitalization time was 8 days after surgery. Most of these patients (n = 40, 74%) lived outside Rovaniemi (more than 85 km from a surgical unit). The other 345 patients were discharged as out-patients.
Of the 385 patients, 23 were re-admitted (6.2%), and the most common reasons for re-admission were intra-abdominal abscess (five patients) and melena (four patients). The median length of hospitalization after re-admission was 5 days. The median time to re-admission was 6 days after discharge and 12 days after the index operation. One patient received a re-operation after re-admission for ileostomal stricture; the others were treated conservatively. Three patients were re-admitted twice due to intra-abdominal abscesses. The median total hospitalization time (primary hospitalization + re-admission) was 6 days (IQR: 4.0).
Discussion
Laparoscopic colorectal surgery has become common in high-volume centers, and the primary outcome results have demonstrated a clear advantage over open surgery without compromising oncological results. Laparoscopy decreases post-operative complications and allows for a shorter hospitalization time after surgery.
Our demographic data suggested that patients in low-volume institutions are somewhat older, and they may also have more comorbidities than patients in international trials. In various multicenter trials, the percentage of patients with classes ASA III and IV has been between 18% and 40%, partly due to the exclusion of patients with comorbidities (1, 9). In our data, these patients represented 48.5% of all patients, which indicated that we studied an unselected, aged patient population.
In this study, the conversion rate was 13%, which was in the range recently reported by high and medium volume centers (8, 9, 14). We observed low numbers of intraoperative severe complications, including two ureter injuries, two iatrogenic bowel injuries, and two intra-abdominal hemorrhages. The 30-day mortality was low, as expected; only one patient died due to surgical error, while two others died after the difficult decision on whether to operate on a patient with terminal disease. In both cases, the potential risks were known and were fully discussed with the patient during the decision-making process.
Despite the minimal invasiveness of laparoscopy, bowel resections in a mixed patient population represent high-risk surgery, with a total complication rate that has been reported to be as high as 30%–34% (1, 9). In our data, 93 patients (24.2%) had at least one surgical complication, and the total complication rate was 31.4%. One indicator of surgical quality is the anastomotic leakage frequency, which typically varies from 4% to 9%, in mixed colorectal studies (8, 9, 14) and from 8% to 13% in laparoscopic rectum surgery (5, 15). In our data, 26 (6.7%) patients had anastomotic leakage, and 16 of these required operative treatment. The number of re-operations we observed (11.2%) was somewhat larger than reported in various trials, but similar to those reported recently (1, 10).
Despite the high age and comorbidity rate of our patient population, the median length of hospitalization was in the range reported in various trials conducted in high-volume centers. Shorter hospitalization periods (3 days median stay after surgery) have, however, been reported (12). In Finland, similar shorter primary hospital stay has been demonstrated in cases in which re-admission did not occur. However, the total median hospital stay during the index admission and the readmission-related days were 5–6 days after laparoscopic bowel resection (16, 17). The hospitalization time we observed may have been partly influenced by the long geographical distances within our hospital district. Once discharged, some patients may have had a higher threshold for choosing a re-evaluation if problems occurred. An early discharge was therefore not our primary concern. The total hospitalization time was unknown in 54 patients who were discharged to local hospitals. However, their median hospitalization in our institution was 8 days; therefore, their prolonged hospitalization would not have affected the median hospitalization time reported here.
The re-admission rate was 6.2%, which figure is also within the range previously published (14, 17). The median time interval between discharge and re-admission was 6 days; with only five patients being re-admitted within the first 3 days. Therefore, longer hospitalization times would not have significantly affected the re-admission rate. Of the 26 anastomotic leakages, 22 were diagnosed before discharge, and no re-operations were required for anastomotic leakage after discharge. According to these results, an earlier discharge might have been possible, as indicated in previous trials. Whether earlier discharges can be achieved in the conditions of our hospital district remains to be seen in the future.
Long-term oncological results are needed in order to justify laparoscopic surgery for colorectal cancer, and the absence of these is one of the main limitations of our study. However, the primary aim of this study was to report short-term outcomes after laparoscopic surgery in a low-volume hospital.
Taken together, our findings have shown that, despite the somewhat higher median age and comorbidity rate of our patient cohort, laparoscopic colorectal resection appeared to be a safe treatment in this low-volume center with extreme distances. We observed anastomotic leakage frequencies, re-operation rates, hospitalization times, and overall complication rates within the ranges of those reported in international trials conducted in high-volume institutes. It can therefore be concluded that high-quality laparoscopic colorectal surgery is feasible in small, peripheral clinics.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Thelma Mäkikyrö Foundation (H.H.), and the other authors have not received any specific grant from any funding agency in the public, commercial, or not-for-profit sectors.