
Abstract
Background and Aims:
Laparoscopic sleeve gastrectomy (SG) has massively increased in numbers over the last decade and is the most frequently performed bariatric procedure worldwide today. The aim of this review is to evaluate SG in terms of weight loss and resolution of comorbidities, based on data gained from the latest long-term studies available.
Material and Methods:
This review includes the results of any long-term studies on SG available at this point as well as a selection of short- and mid-term studies.
Results:
There are only a handful of studies on sleeve gastrectomy with long-term follow-up available at this point. Conversion rates in these long-term studies amount to up to one-third of their cohorts; however, excess weight loss in patients maintaining their sleeve is over 50%. Results on the resolution of comorbidities vary among the studies available today.
Summary:
Sleeve gastrectomy is a valid bariatric method but one has to be aware of its limitations.
Keywords
Background and Aims
Sleeve gastrectomy (SG), the most commonly performed bariatric procedure worldwide today, is still to be considered a rather new method within a field that is quite young itself—compared to other areas of general surgery: the first bariatric procedure performed on a patient was Kremen and Linner’s jejunoileal bypass in 1954 (1). While vertical banded gastroplasty and Magenstrasse and Mill may be considered predecessors of SG by some, others might argue that it was newly developed as part of biliopancreatic diversion and then became a standalone procedure (2,3).
During the early years of SG as independent method, in the early 2000s, it was a two-step procedure: super-obese patients with a body mass index (BMI) over 50 kg/m2 had SG first and then a malabsorptive method after losing a considerable amount of weight—which usually happened after a year, approximately (4). Today, SG is thus a solely restrictive procedure and indicated for patients with a BMI of over 40 kg/m2, or 35 if they suffer from a comorbidity as well, and does not typically include a second step (5).
SG overtook Roux-en-Y gastric bypass (RYGB) as the most common bariatric procedure worldwide in 2014. It may be argued that SG has supplanted adjustable gastric banding, the number 1 bariatric procedure of the 1990s, which is practically obsolete in many countries today (6).
SG is now more than 15 years old and has been acclaimed by a considerable number of short- and mid-term studies as highly effective method for excess weight loss and cure of comorbidities. However, the latest studies on SG’s outcome, which include follow-ups of 8 years or more, do evaluate the procedure more controversially, which has caused a highly interesting discussion of its true merits among the researchers (7–11). The aim of this review, therefore, is to evaluate SG in terms of weight loss and resolution of comorbidities, based on data gained from the latest long-term studies available.
Material and Methods
This review includes the results of any long-term studies on SG available at this point as well as a selection of short- and mid-term studies. The latter were chosen by relevance to this review’s focus as well as by the studies’ design and time/place of publication. Thus, preference was generally given to rather recent studies, randomized controlled trials, studies with large cohorts, and studies published in highly rated journals. The search for studies was performed on PubMed database using the keywords “sleeve gastrectomy” or “gastric sleeve.”
Results
Weight loss
Weight loss after SG should be discussed based on the quite varying results of studies with different lengths of follow-up periods available (Table 1).
Review of selected literature on short-, mid-, and long-term outcome of SG.
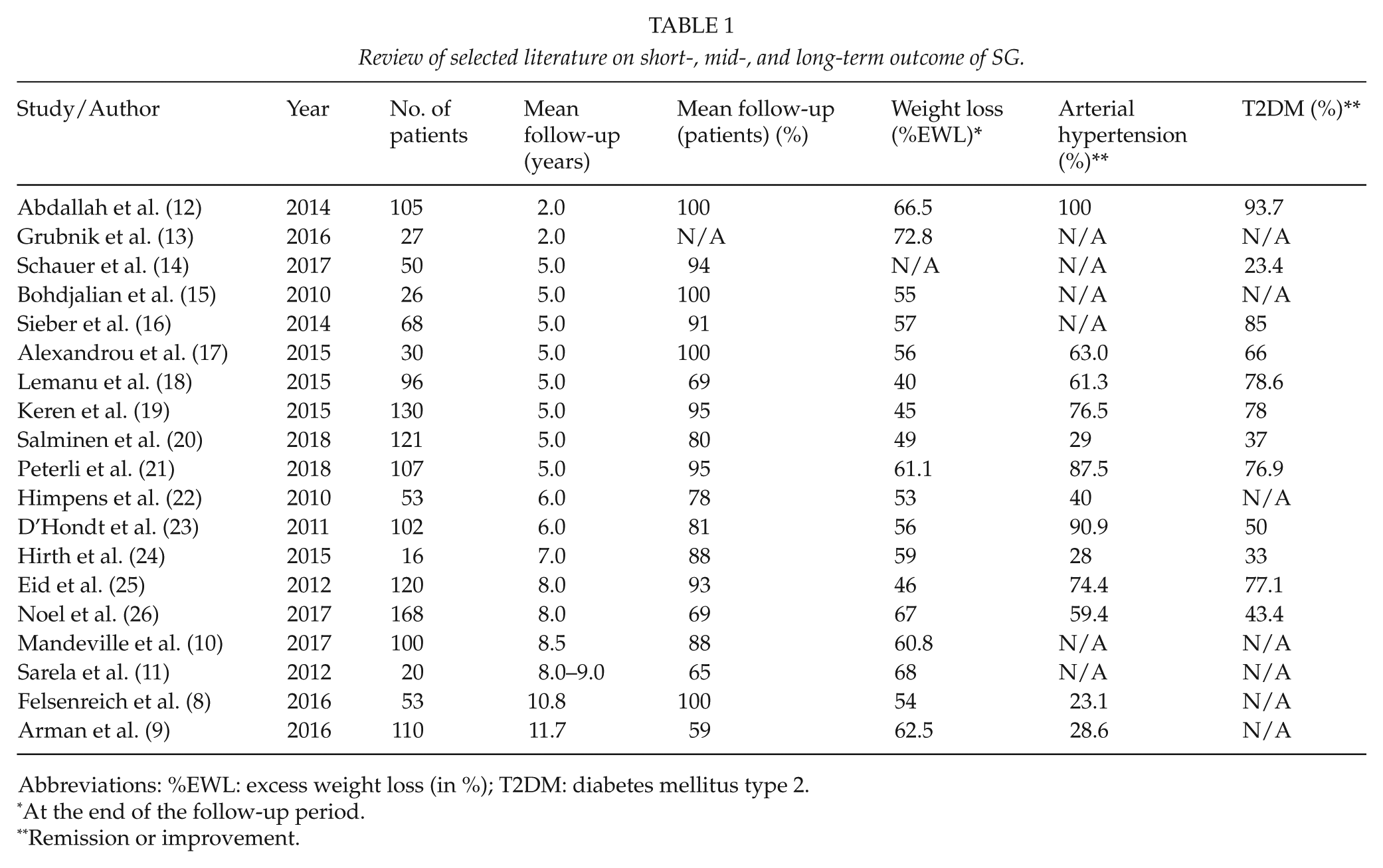
Abbreviations: %EWL: excess weight loss (in %); T2DM: diabetes mellitus type 2.
At the end of the follow-up period.
Remission or improvement.
The results of short-term studies (follow-up periods of 1–3 years) on SG are quite similar to one another in that they depict an excellent outcome in terms of excess weight loss (%EWL). Grubnik et al. (13), for example, in a randomized controlled trial found a high %EWL of 78.9% 2 years after SG.
Mid-term studies’ (follow-up of 4–7 years) results are less homogeneous: many still find decent amounts of %EWL, however, some also show a slight weight regain from nadir weight compared to short-term results (23,24). Three studies with follow-up periods of 5 years and small study cohorts between 26 and 68 patients showed a %EWL between 55 and 57 (15–17). Two studies with larger cohorts of 96 and 130 patients only found %EWL of 40 and 45, respectively, after 5 years (18,19). Furthermore, two prospective randomized studies comparing RYGB and SG with a follow-up of 5 years have been published recently. First, no significant difference in excess weight loss was found comparing SG and RYGB (49% vs 57%) in the SLEEVEPASS study including 240 patients and an 80% follow-up rate (20). Second, the SM-BOSS study showed that the peak excess BMI loss was reached 2 years after SG (74.7%) and had decreased by the end of the fifth year to 61.1%. Plus, no significant difference was found between SG and RYGB in terms of excess BMI loss (21).
Recently published long-term studies (8+ years of follow-up) have found similar numbers in terms of %EWL. Mandeville et al. (10) in a study of 100 patients report a %EWL rate of 60.8 at a mean 8.5 years after SG, Felsenreich et al. (8) state 54% after a mean 10.8 years and 53 patients, and Arman et al. (9), in the study with the longest follow-up of a mean 11.7 years published so far, found 62.5% in 110 patients.
An important point that needs to be made when considering long-term studies’ weight loss results is that, while %EWL does not further decrease in any substantial way, the conversion rate is between 20% and 35% (8–11). Thus, for complete %EWL results one would have to include converted patients’ %EWL at the time of conversion into these numbers as well.
In terms of technique, it is important to add that while in SG’s early days the resection was started opposite the crow’s foot, about 6 cm above the pylorus (27), it is common to resect the entire antrum today, which, as Yormaz et al. (28) point out, affects weight loss success. In their retrospective study they compared the outcome of patients who had had SG with antrum resection (2 cm distance to the pylorus) and patients who had not (6 cm distance to the pylorus). At 2 years, patients with antrum resection had lost significantly more weight (%EWL: 68.7 vs 61.5). Similarly, a prospective randomized study compared two groups of patients who had SG with antrum resection, one at 2 cm and the other at 6 cm distance to the pylorus. After 2 years, the %EWL was significantly higher in the first group (71.8% vs 61%, p = 0.003). The complications rate in this study was not significantly different in both groups (12).
Resolution of Comorbidities
As studies have shown, arterial hypertension and T2DM are common comorbidities with SG. (Other comorbidities (e.g. sleep apnea, hyperlipidemia) will not be discussed here since there is not enough data available at this point.) The results vary considerably according to the length of the studies’ follow-up. It is also important to note that the number of long-term studies on comorbidities and their improvement is quite limited even now. (Table 1)
Chuffart et al. (29) report a remission rate of arterial hypertension of 28% at 5+ years after SG. Both, the SLEEVEPASS and the SM-BOSS study also looked into the resolution/improvement of comorbidities at 5 years. In the former, the resolution/improvement rates of T2DM and arterial hypertension are 37% and 29%, while they are higher in the latter (76.9% and 87.5%) (20,21). In a study with a follow-up of 11+ years, Arman et al. have examined the remission of comorbidities and found that preoperative arterial hypertension was resolved or at least improved in 28.6% (two out of seven) of their patients, while one patient had developed it de novo (9). Similar results can be found in Felsenreich et al.’s (8) study with a follow-up of 10+ years: an improvement of arterial hypertension was found in 23.1% of their subjects. The authors of both studies were not able to evaluate the development of T2DM due to the low number of patients with T2DM in their cohorts.
Aminian et al. (30) found that, comparing results at <2 years and >5 years of patients with T2DM, remission of diabetes had decreased from 41% to 26%. About 44% of patients with initial T2DM remission had experienced relapse. Schauer et al. (31) observed T2DM remission (Hba1c ⩽ 6.5%) in 47% of their patients at 3 years after SG. In an update at 5 years after SG they found T2DM remission (Hba1c ⩽ 6.5%) in 36% of their patients (14) These data show that several patients in this study experienced T2DM relapse between 3 and 5 years after SG, however, the participants had started at a high Hba1c level of 9.5% preoperatively.
However, a long-term study with a follow-up of 8 years and a large cohort (120 patients) showed rather high remission rates for both T2DM (74%) and arterial hypertension (77%) (25).
Gastroesophageal Reflux Disease and Barrett’s Esophagus
When looking at the outcome of SG in terms of reflux, one may notice that short-term studies report an improvement (or even remission) of reflux symptoms in many of their patients, which may very well be caused by a decrease of intra-abdominal pressure as patients lose large amounts of weight (32–35). Spivak et al. (35), for example, were able to show in a study comparing the use of different bougie sizes for SG that reflux was cured in 73.7% of patients, who had had preoperative reflux, after 1 year. Chiu et al. (32) analyzed 15 studies with follow-ups between 6 and 60 months after SG in a systematic review and found that 4 of them reported higher rates of reflux and 7 showed improvement of reflux (the results of 4 studies were not relevant).
Mid- and long-term studies, however, show an increase in patients needing proton pump inhibitors (PPIs) and severe reflux symptoms that often stem from de novo reflux (22,36,37). Boza et al. (38), for example, found new-onset reflux in 26.7% of their SG patients after 5 years in a study of 161 patients with a follow-up rate of 70%. Himpens et al. (22) studied 53 SG patients at a follow-up of 6+ years and 21% were suffering from new-onset reflux at that point. A reason for de novo reflux at this stage may be an increased intra-abdominal pressure caused by weight regain, which often also leads to hiatal hernia development and/or intra-thoracic migration of the sleeve, which is a high-pressure system (7).
Studies focusing on SG combined with intra-operative hiatal hernia repair report better short-term results considering reflux (37,39,40). Some authors argue that hiatal hernia detection in preoperative gastroscopies is overestimated and advocate a combination of SG with hiatoplasty as standard procedure (33,41). In a study on SG with hiatoplasty including 378 patients, 15.8% of whom had had reflux preoperatively, Soricelli et al. (40) found a remission of reflux symptoms in 73.3% after 18 months. Daes et al. (33), combining SG with hiatoplasty as well, published a study of 382 patients and 6–22 months follow-up. Hiatoplasty in this study was performed in case hiatal hernia was found intraoperatively and 94% of their patients with preoperative reflux were cured. However, the results of long-term studies based on this method have yet to be published and will certainly be a very interesting contribution to the discussion of SG.
Barrett’s metaplasia has been found as consequence of chronic reflux in a small number of studies at this point. Genco et al. (42) in a study with a mean follow-up of 58 months after SG report newly diagnosed Barrett’s metaplasia in 17.2% of their patients. Felsenreich et al. (7) found Barrett’s metaplasia in 15% at 10+ years after SG. Interestingly, both studies did not find any significant correlation between reflux symptoms and Barrett’s metaplasia, which shows that patients without symptomatic reflux may be at risk of developing Barrett’s as well. In a case report Wright et al. (43) have described the incidence of adenocarcinoma of the esophagus 5 years after SG. However, Gagner (44) argues that Barrett’s esophagus need not be an absolute contraindication to SG based on the fact that, even after 25 years of applying this method, no adenocarcinoma have been reported after duodenal switch (SG is part of this procedure).
As the discussion of these studies shows, there is no consensus among authors whether to exclude patients with preoperative reflux from SG. The occurrence of Barrett’s metaplasia after SG has been reported by a small number of mid- and long-term studies only recently. Therefore, the discussion on how to treat patients with preoperative Barrett’s metaplasia has yet to be concluded.
Further (long-term) studies are necessary to determine whether hiatal hernia may be considered a (relative) contraindication to SG. In case of preoperative hiatal hernia authors generally agree that hiatoplasty must be added to the procedure to achieve an improvement or even remission of gastroesophageal reflux disease (GERD).
Preoperative gastroscopies are advisable for all patients as GERD, hiatal hernia, and Barrett’s esophagus may be diagnosed this way. Postoperative gastroscopies at regular intervals are recommended as part of a post-SG scheme at bariatric centers in order to detect GERD and its further ramifications, such as Barrett’s esophagus, especially in patients without clinical reflux (7). Georgia et al. showed in a recent study comparing SG patients’ DeMeester scores pre- and postoperatively that they were 2.5 times higher after the procedure. Thus, 24 h pH-metries are recommended for SG patients in order to detect GERD at an early stage (45).
Reoperations and Complications
An analysis of different studies shows that the conversion rate after SG rises with the length of the follow-up period due to different reasons. Alexandrou et al. (17), for example, studied 30 SG patients and report that 5 (16.7%) of them had been converted to RYGB by 5 years. By comparison, conversion rates in long-term studies are noticeably higher. Studies with follow-ups between 8 and 9 years found conversion rates of 29.5% and 20%, respectively (10,11). In studies with over 10 years of follow-up, authors report 25% and 37% (8,9).
Bohdjalian et al. (15) found that 15.4% of their SG patients had had conversions (to RYGB) 5 years after SG. 3.8% of these patients were converted because of reflux and 11.5% due to weight loss failure. Both issues will be discussed separately in the following sections.
GERD
There are several options available for converting patients who suffer from reflux. They may be converted to RYGB (combined with hiatal hernia repair if necessary) or may receive a Linx® ring device (46). However, the latter procedure may still be considered experimental—there are no long-term results or studies including larger cohorts available at this point. For patients with remnant fundus or unformed sleeve, detected via gastroscopy or 3D volumetry, a re-sleeve procedure may be an option (47–49).
Patients diagnosed with Barrett’s metaplasia may—according to the guidelines published by the American Society for Gastrointestinal Endoscopy (ASGE)—have a surveillance gastroscopy after 1 year, then periodic gastroscopic check-ups every 5 years (50).
In case of Barrett’s dysplasia, ablation therapy has been recommended in literature (51). If patients suffer from severe reflux as well, they are suggested to take PPIs to alleviate reflux symptoms (52) or may be converted to RYGB instead (53,54).
Weight Regain
The question of how to treat patients with weight regain after SG has been discussed among authors in recent years. For example, Homan et al. have published a study comparing conversion to RYGB to biliopancreatic diversion with duodenal switch. While their group of patients that were converted to biliopancreatic diversion with duodenal switch showed better weight loss results (with a median excess weight loss of 59%) than those converted to RYGB (23%), the authors conclude that a conversion to RYGB was better suitable for patients who suffered from GERD or dysphagia instead of weight regain (55). Also, comparing patients converted to RYGB due to weight regain to those without conversion at 10+ years after SG, Felsenreich et al. (8) were able to show that both groups had similar %EWL results (52.8 vs 52.5%). One may conclude that RYGB is only mildly effective in achieving good weight loss results as a conversional procedure and that procedures involving a stronger malabsorptive element (e.g. biliopancreatic diversion with duodenal switch, Fig. 3) may be more successful options. Single anastomosis duodeno-ileal bypass with SG (=SADI-S, Fig. 1) and single-anastomosis gastric bypass (Fig. 2) are possible alternatives to biliopancreatic diversion with duodenal switch. However, as both are still “new” procedures, there is currently no reliable data available on their performance as conversional methods after SG.
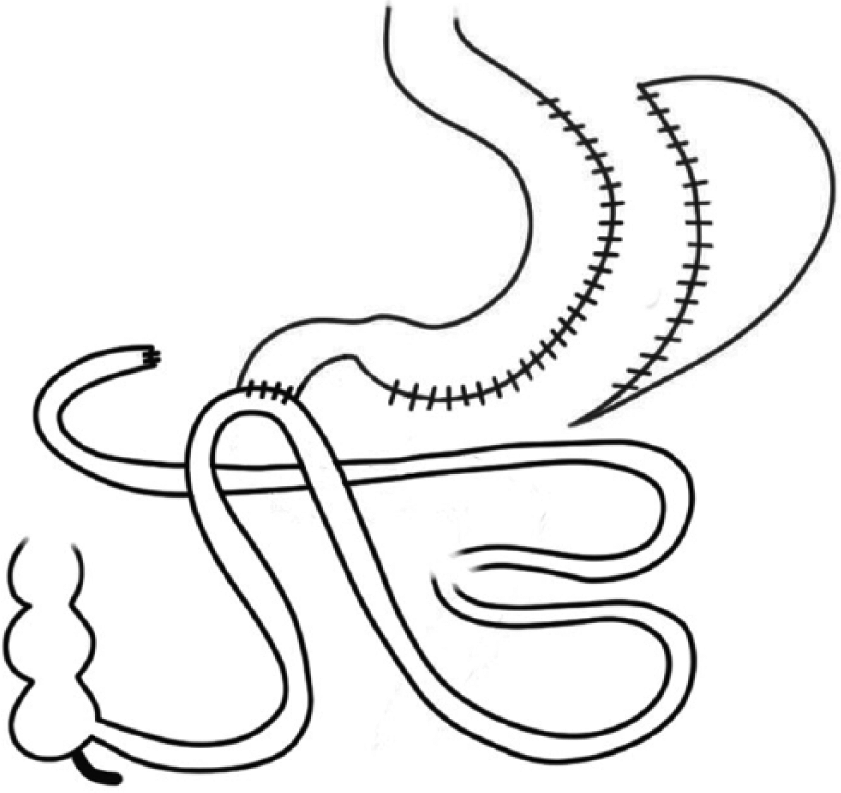
SADI-S (Single-anastomosis duodeno-ileal bypass with sleeve gastrectomy).
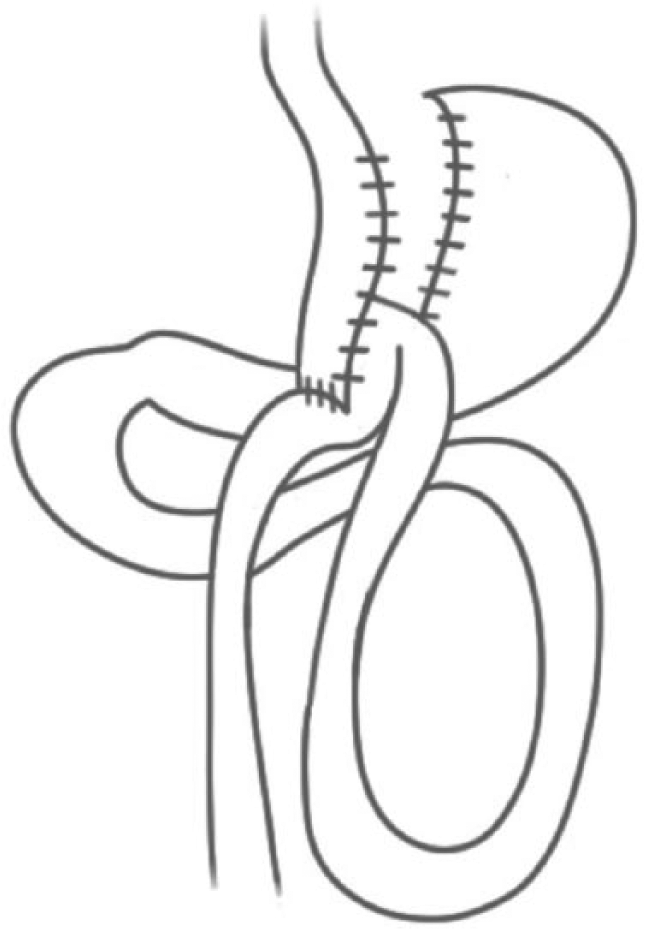
Single-anastomosis gastric bypass (omega loop bypass).
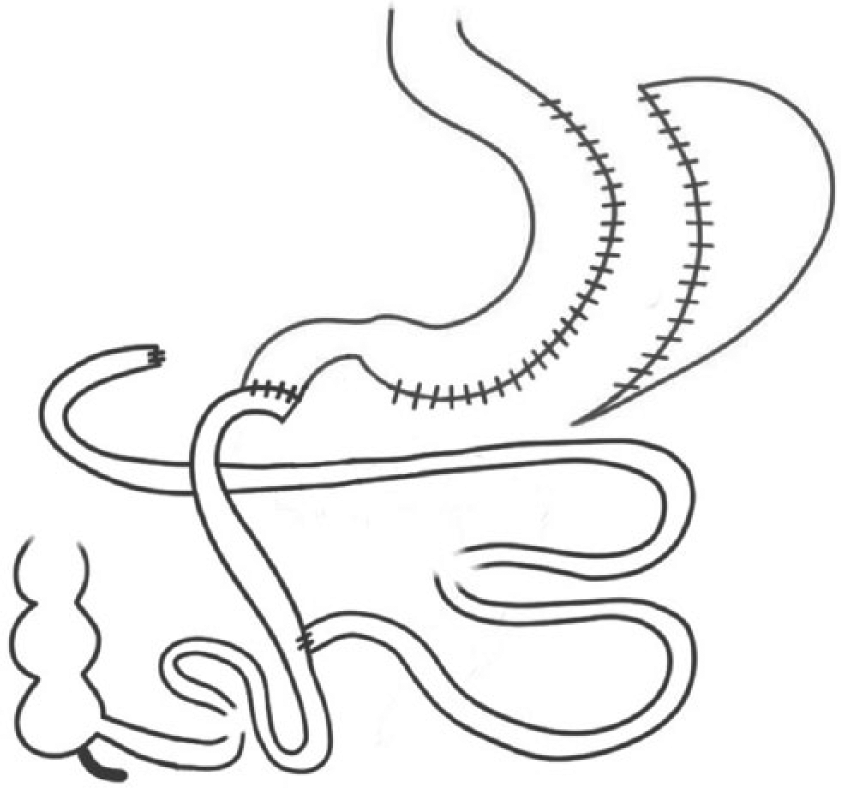
Biliopancreatic diversion with duodenal switch.
If patients experience weight regain due to pouch dilatation, revised SG (re-sleeve) may be an effective option. In a study with a follow-up of 20 months, Nedelcu et al.’s (48) patients reached a mean %EWL of 58.5% after revised SG.
Studies have shown that patients suffering from both reflux and weight regain fare best with a conversion to RYGB, combined with hiatal hernia repair if applicable. An intraoperative exploration of the hiatus should be part of every revisional procedure to detect hiatal hernia (53,54).
Late Complications
Complications that may appear during a long-term follow-up after SG include stenoses, reflux and weight regain, the latter of which have already been discussed. Leaks have been commonly described as complications of SG as well, however, they tend to occur at a much earlier stage after the procedure and are thus omitted in the present discussion.
Agnihotri et al. have developed an algorithm for the treatment of stenoses after SG, which includes a series of possible measures that may be taken until resolution is achieved. The various steps suggested are dilation with different diameters, stenting using fully covered metal stents, and conversion to RYGB as last resort (56). Similarly, Manos et al. (57) had good results using balloon dilation and stenting in 18 SG patients with stenoses. Nath et al. (58) found that balloon dilation lead to resolution in 69% of their 352 patients with stenoses in a retrospective cohort study.
Outcome
The outcome of a bariatric procedure very much depends on weight loss success and remission of comorbidities. The Bariatric Analysis and Reporting Outcome Score (BAROS) serves to evaluate the outcome of a bariatric procedure and has been used for SG patients by several studies. The BAROS mainly factors in patients’ quality of life, weight loss success, and remission of comorbidities (59). When comparing the results of different studies, one may observe that BAROS results decrease with the length of the follow-up period. For example, Keren et al. (60) found mean BAROS scores of 7.6 and 6.9 in their two groups of patients at 2.5 years after SG, which denote “very good” results. In a study with a follow-up of 5 years, Lemanu et al. (18) report a “good” outcome (mean BAROS of 3.1). Finally, Felsenreich et al. (8), using BAROS as well, identified a mean score of 2.4 at 10+ years after the procedure, which means “slightly efficient.”
Summary
The aim of this review was to evaluate SG in terms of weight loss and resolution of comorbidities on the basis of data gained from the latest long-term studies available.
Based on the findings of the studies analyzed in this review, it may be concluded that in terms of excess weight loss long-term results are generally satisfying. Results on the resolution of comorbidities vary among the studies available today, so the procedure’s performance in this area cannot be evaluated irrefutably at this point.
However, there is no consensus among authors concerning the issues of GERD and Barrett’s esophagus. Authors argue whether SG is able to improve symptomatic reflux and reduce the risk of developing Barrett’s metaplasia or, on the contrary, if it actually promotes these issues. Thus, the question whether GERD and Barrett’s esophagus should be treated as relative contraindications to SG may not be clearly answered at this point.
In terms of hiatal hernias authors have reported good results combining SG with hiatoplasty. An intraoperative visualization of the hiatus to detect hiatal hernias and adding hiatoplasty to SG if necessary thus seems recommendable.
This review of long-term studies was also able to show that conversion rates after SG are quite high due to different reasons. RYGB as a conversional procedure is considered most successful for patients with reflux in literature. Patients with weight regain are suggested to benefit from a procedure with a stronger malabsorptive element.
Footnotes
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.