
Abstract
Background and Aims:
As conducting the regular trauma team simulation training is expensive and time-consuming, its effects must be explored. The objective was to evaluate the efficacy of a structured 2-h in situ multiprofessional trauma team simulation training course on non-technical skills.
Materials and Methods:
This prospective study comprised 90 trauma teams with 430 participants. The structured, 2-h course consisted of an introductory lecture and two different simulations with debriefings. Data were collected using a pre–post self-assessment questionnaire. In addition, the expert raters used the T-NOTECHS scale.
Results:
The following non-technical skills improved significantly among both medical doctors and nurses: knowledge of the trauma resuscitation guidelines, problem identification, decision making, situation awareness/coping with stress, communication and interaction, time management, being under authority, and confidence in one’s role in a team. The teams improved significantly in leadership, cooperation and resource management, communication and interaction, assessment and decision making, and situation awareness/coping with stress.
Conclusion:
A short, structured 2-h in situ trauma team simulation training course is effective in improving non-technical skills.
Keywords
Introduction
Emergency trauma management is a complex, time-critical enterprise requiring a multidisciplinary health care team comprised of highly trained medical professionals. It poses a unique challenge to the health care system as casualties presenting within the first 2 h of injury represent the population with potentially preventable disability and death. This group of patients can be helped through expert trauma management, such as a dedicated trauma team (1).
The primary aims of the trauma team are to rapidly resuscitate and stabilize the patient, treat the patient holistically and humanely, prioritize and determine the nature and extent of the injuries, and prepare the patient for transport to the site of definitive care according to the predetermined protocol (2, 3).
Trauma teams are important parts of the optimal care of severely injured patients, and they have been shown to reduce the time taken for resuscitation, clinical and radiological diagnostics as well as time to emergency department discharge and transfer to the operating room (3, 4).
Non-technical skills (NTS) are seen as an important contributor to reducing adverse events and improving medical management in health care teams (5). Better teamwork and non-technical performance are associated with significant decreases in disposition time, which is an important marker of quality in acute trauma care (6). Positive reactions to simulation-based training of NTS have been found, and especially its strengthening effects on teamwork and communication (7–11).
As conducting the trauma team simulation training is expensive and pulling staff from their clinical tasks is time-consuming and requires special arrangements, the effects of the simulation training course must be explored to be able to show the efficacy of the course and to develop further the format of the course. Durations of reported trauma team simulation training courses vary from 30 min to 3 weeks (11). Studies with short simulation training course (⩽4 h) and large research data were not found. Also, evaluation methods of learning vary considerably between trauma team simulation training courses (11).
The aim of this study was to evaluate the effects of a short, structured 2-h in situ trauma team simulation training course on NTS in a large research material using two assessment methods. We integrated both self-assessment and validated expert rater assessments (T-NOTECHS) to increase validity of the results (12).
Materials and Methods
Setting and Trauma Team Simulation Training Course
We started conducting computerized patient simulator–based multiprofessional trauma team simulation training regularly in 2009 in the Central Finland Health Care District. Our Center of Medical Expertise is an accredited Center by the Network of Accredited Skills Centres in Europe (NASCE). In our hospital, simulation training is used as a regular teaching and learning method to improve and maintain the team’s performance. This trauma team simulation training is developed for specialists and residents, and trauma and other nurses working in the emergency department, intensive care unit (ICU), and post anesthesia care unit. Minimally, the trauma team includes a surgeon, an anesthesiologist, a radiologist, a trauma nurse, and another nurse as an anesthesiologist’s working pair. The surgeons, anesthesiologists, and nurses participate in the training once a year.
The educational goals of the course are in improving the team members’ knowledge of the trauma resuscitation guidelines, problem identification, assessment together with decision making, situation awareness/coping with stress, teamwork/cooperation and resource management, communication and interaction, time management, being under authority, and confidence of one’s own role in a team. Team leaders’ experiences of their leadership, workload distribution, and conflict resolution are also of interest. The aim of the simulation training is to enhance the effectiveness of team performance by practicing these focus areas.
The structured 2-h trauma team simulation courses were conducted in a real hospital environment (“in situ”) in Central Finland Hospital Emergency Department. The participants acted in their real-life professional roles.
After we obtained institutional review board approval to conduct this study, we started data collection. The data were collected prospectively between October 2013 and May 2016 anonymously using a pre–post self-assessment questionnaire and T-NOTECHS scale filled in by two expert raters (S.L. and nurse-teacher). There were 90 teams, 180 simulations, and 430 participants. It is recommended in our hospital that the professionals participate in the trauma team simulation course annually, so only 27% (n = 116) of the participants under study were first-timers.
The 2-h trauma team simulation course included clarifying the method (10 min), an introductory lecture (10 min), taking the roles (10 min), first simulation (15 min), debriefing (30 min), second simulation (15 min), and debriefing (30 min). The simulations were video recorded for the debriefings. The recordings were deleted afterward. The simulated patient scenarios were changed twice a year and the 2-h simulation training included two different patient scenarios. The topics of the introductory lectures and simulated scenarios are described in Supplement 1.
The main instructor (S.L.) of the simulation training is a senior anesthesiologist and an intensivist. He has a special competency as a medical educator and in emergency medicine from Finnish Medical Association. He is an Advanced Trauma Life Support (ATLS) provider and has participated in the Finnish basic course of the simulation instructor and the European Trauma Course (ETC). Two nurse-teachers (anesthesia nurses) worked as his working pair (one at a time). They acted as simulator pilots. Nurse-teachers have also participated in the Finnish basic course of the simulation instructor. A member of the team is also an assistant, who technically conducts the simulations. Three different computer-based patient simulators were used: an infant (SimNewB™, Laerdal), a 6-year old boy (MegaCode Kid™ Vital Sim, Laerdal), and an adult (HAL S3201, Gaumard, Nordic Simulators Oy).
Instruments
The self-assessment questionnaire included two pages: page 1 (questions 1–8) was filled in before the simulation training course. In page 1, there were six background questions: (1) age, (2) gender, (3) occupation, (4) working experience in years in a present duty, (5) participation times to a trauma team simulation course, and (6) participations times to real-life trauma team resuscitation.
In question number 7, participants were asked to evaluate how much their real-life trauma resuscitation–related domains need improvement. The following domains were evaluated: (7a) knowledge (textbook knowledge and guidance), (7b) skills (hands-on skills), and (7c) attitudes (acting as agreed).
Participants’ perceptions of their real-life trauma resuscitation–related skills and their levels (question number 8) were examined. The NTS of interest were (8a) knowing the trauma resuscitation guidance, (8b) problem identification, (8c) decision making, (8d) situation awareness/coping with stress, (8e) teamwork/cooperation, (8f) communication and interaction, (8g) time management, (8h) being under authority, and (8i) the confidence of the own role in a team. In addition, the team leaders were asked to answer the following three extra questions: (8j) leadership, (8k) workload distribution, and (8l) conflict resolution.
Page 2 (questions 9 and 10) was filled in immediately after the training. Question number 9 was identical with question number 7, and question number 10 was identical with question number 8.
The answers to question numbers 7 to 10 were given using the 5-point Likert-type scale (1 = I need a lot, 5 = I don’t need at all).
The modified NTS (NOTECHS) scale for trauma (T-NOTECHS) was used to assess teamwork skills of multidisciplinary trauma resuscitation teams. T-NOTECHS is based on a psychometrically sound teamwork rating tool for operating room teams. It is based on five behavioral domains, illustrated with exemplar behaviors. These domains are leadership, cooperation and resource management, communication and interaction, assessment and decision making, and situation awareness/coping with stress. T-NOTECHS is a tool on the basis of these behavioral domains that could serve to evaluate trauma teams. It uses a 5-point Likert-type scale (range: 1–5 points). In general, “1” indicates the team did not demonstrate this teamwork behavior, and “5” indicates flawless teamwork. The total score ranges from 5 to 25 (12).
Author 1 (E.R., Educational designer) introduced the T-NOTECHS to two raters, and concepts of behavior rating and specific features of this tool were discussed before commencing assessment. The main instructor (S.L.) and nurse-teacher acted as expert raters, and they conducted the assessments in a real time, immediately after the simulations.
Statistical Analysis
The data were analyzed with the SPSS, version 23.0 (SPSS, Inc., Chicago, IL, USA). The results were presented as frequency and percentage distributions. The averages used were the mean and the median. Measures of dispersion used were standard deviation and interquartile range (IQR). Paired-samples t-test as a statistical analysis method was used. A p value of less than 0.05 was considered significant.
Interrater reliability between the expert raters was calculated using intraclass correlation coefficients (ICCs). ICC can be interpreted as follows: 0–0.2 indicates poor agreement, 0.3–0.4 indicates fair agreement, 0.5–0.6 indicates moderate agreement, 0.7–0.8 indicates strong agreement, and >0.8 indicates almost perfect agreement.
Results
Over half of the participants (total N = 430) were female (58%). The participants’ age varied between 20 and 63 years (mean = 37 years). The occupations were as follows: an anesthesiologist (20%), a surgeon (19%), a pediatrician (1%), an emergency medicine physician (6%), a radiologist (1%), a nurse (50%), and other (3%). The mean working experience in a present duty was 8 years (median = 4.9). The median participation time to course was 3 times (IQR = 1–6) and to real-life trauma team resuscitation situation was 5 times (IQR = 1–10).
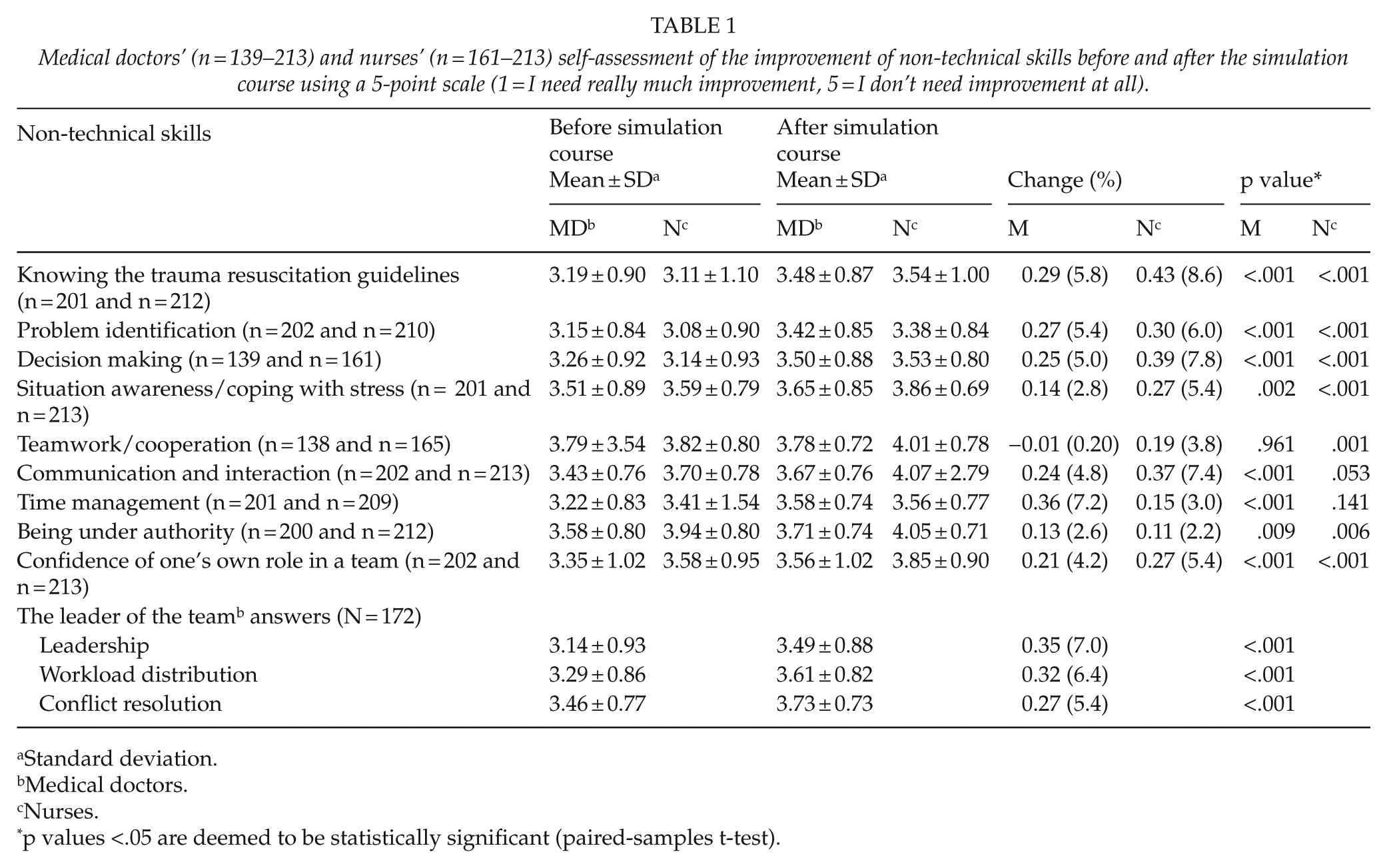
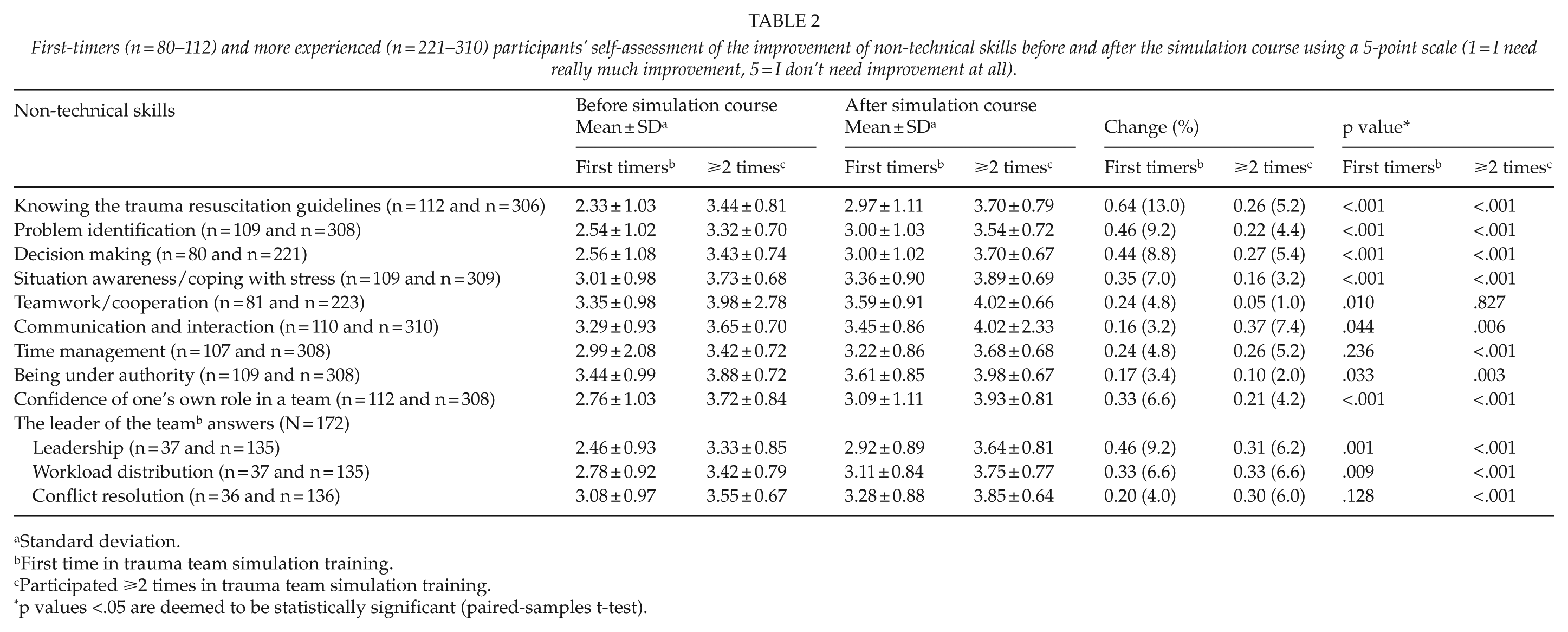
Table 1 describes the self-assessment of the skill levels related to NTS before and immediately after the trauma team simulation course of different professional groups using a 5-point scale. Table 2 shows perceived NTS-related skill levels among first-timers and more experienced participants in the trauma team simulation course.
Medical doctors’ (n = 139–213) and nurses’ (n = 161–213) self-assessment of the improvement of non-technical skills before and after the simulation course using a 5-point scale (1 = I need really much improvement, 5 = I don’t need improvement at all).
Standard deviation.
Medical doctors.
Nurses.
p values <.05 are deemed to be statistically significant (paired-samples t-test).
First-timers (n = 80–112) and more experienced (n = 221–310) participants’ self-assessment of the improvement of non-technical skills before and after the simulation course using a 5-point scale (1 = I need really much improvement, 5 = I don’t need improvement at all).
Standard deviation.
First time in trauma team simulation training.
Participated ⩾2 times in trauma team simulation training.
p values <.05 are deemed to be statistically significant (paired-samples t-test).
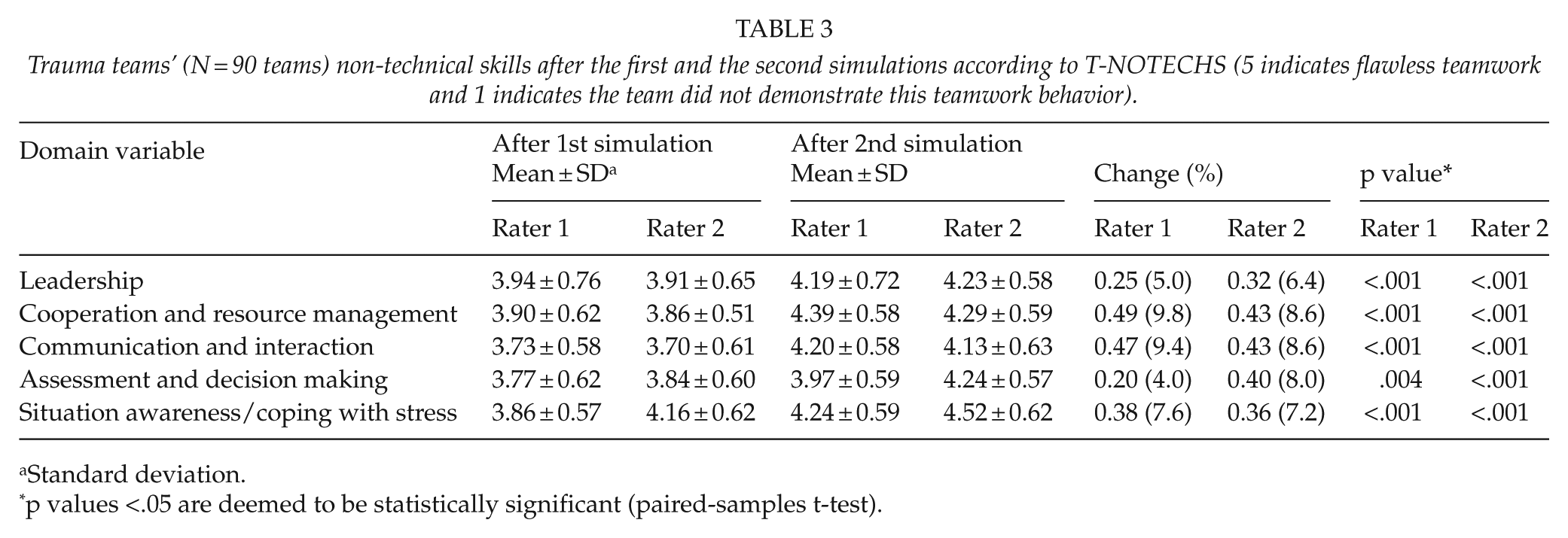
Table 3 demonstrates the trauma teams’ (N = 90 teams) NTS according to the T-NOTECHS scale after the first and the second simulations as evaluated by two expert raters.
Trauma teams’ (N = 90 teams) non-technical skills after the first and the second simulations according to T-NOTECHS (5 indicates flawless teamwork and 1 indicates the team did not demonstrate this teamwork behavior).
Standard deviation.
p values <.05 are deemed to be statistically significant (paired-samples t-test).
Interrater Reliability for T-Notechs
The interrater agreement between the two raters for T-NOTECHS after the first (n = 90) and second (n = 90) simulations was fair (ICC = 0.30). When combining all the simulations (N = 180), the ICC was 0.41.
Discussion
Our study demonstrated that a short, structured 2-h in situ multiprofessional trauma team simulation training course is effective and improves skill levels related to NTS among both specialist doctors/residents and nurses/nurse students.
According to the self-assessments, all NTS improved statistically significantly among all participants, with the exceptions of teamwork/cooperation among specialists and residents, and time management among nurses/nurse students. Teamwork/cooperation was rated highest both before and after the simulation course by the specialists and residents, which may explain why it did not improve during the course. The ratings on leadership, workload distribution, and conflict resolution by team leaders (N = 172) improved (p < .001).
Some differences were observed between the professional groups. Specialists and residents mostly improved in time management, knowledge of the trauma resuscitation guidelines, and problem identification. Nurses and nurse students mostly improved in knowledge of the trauma resuscitation guidelines, decision making, and communication and interaction.
The self-assessments of personnel participating for the first time in a trauma team simulation course showed statistically significant improvements in all NTS except time management. Before the simulation course, the level of knowhow of the first-timers was lower in all NTS when compared to the levels of those who had previously participated ⩾2 times in a trauma team simulation course. After the course, the first-timers’ perceptions of their skill levels remained lower in all NTS compared to the levels of the more experienced team members: the first-timers’ mean scores were 0.37 to 0.84 points lower than the means of their more experienced colleagues. This indicates both the efficacy of the simulation training course and the need for regular simulation training.
According to the two expert raters’ assessments (T-NOTECHS), the teams’ leadership, cooperation and resource management, communication and interaction, assessment and decision making, and situation awareness/coping with stress improved statistically significantly as a result of the simulation training. The positive change in means varied between 4%–10% (Rater 1) and 6%–9% (Rater 2). The mean scores of the two raters after both the first and second simulations were in good agreement.
Furthermore, the self- and two expert raters’ assessments were in good agreement, which improves the validity of the study.
Relation to Previous Literature
In a systematic review, Gjeraa et al. (11) explored the efficacy of simulation-based trauma team training of NTS and found that a significant effect on learning after training. Knowledge and skills improved after training in all the studies that evaluated the effect of training on learning. However, all these studies included a moderate to high risk of bias. NTS training duration varied from 30 min to a couple of days; however, in two studies, the simulation training was conducted for 10 to 14 days and over 3 to 4 weeks (7, 11, 13).
Gjeraa et al. (11) also found that the methods used in the trauma team simulation training of NTS varied considerably. These included, for example, pre-reading of handbooks, didactic sessions, online training, case-based discussions and skill stations as well as team-training sessions with team exercises and debriefing situations with video recordings of the simulations. This diversity of methods hinders comparison of research results.
Trauma teams are typically assembled on an ad hoc basis for individual trauma resuscitation events. Research has shown that the NTS required by a trauma team are difficult to maintain (14). In the study by Roberts et al. (15), the changes in team behavior and communication induced by simulation-based training were maintained after a 3-week interval. Hunziker et al. (16) found that brief leadership instructions improved cardiopulmonary resuscitation in a high-fidelity simulation, and that the improvement was maintained at the 4-month follow-up. These results support the idea that trauma team members who are not routinely exposed to treating trauma victims need to be regularly trained to assess and manage these patients. Our short 2-h trauma team simulation training course includes all these significant factors: training is regular and structured, multiprofessional teams are assembled on an ad hoc basis, and the simulation is conducted in situ in the emergency department. This may explain the efficacy of our course.
The changes in our study were statistically significant in most of the target NTS. In the self-assessments, the biggest improvement was among first-timers in knowledge of the trauma resuscitation guidelines: the post-course mean improved by 0.64 points (13%). The score improvement in the T-NOTECHS scale varied between 0.20 and 0.49 (4%–10%) across the two raters. A potential explanation for the relatively small change in the score is that the NTS levels were already high at baseline, as most of the participants had previous experience of participating in a trauma team simulation training course as well as in real-life trauma resuscitations. However, 27% (n = 116) were first-timers in a trauma team simulation course and 22% had never participated in a real-life trauma team resuscitation.
Limitations and Advantages of The Study
A limitation of the present study was that the video recordings of the simulations were utilized only during the debriefings. Video recordings as research material would enable an independent assessment of the person’s or team’s performance. However, trauma team simulation training in our hospital is used as a regular teaching and learning method, and not to evaluate team competence. Another important aspect is to protect participant anonymity and the confidentiality of the training.
Two expert raters were present in all simulations to avoid single-source bias and to increase the validity of the study. The raters were experienced in both real-life trauma team working and as simulation instructors.
The minimal important change in the T-NOTECHS remains undetermined. Our research setting does not enable us to evaluate the clinical significance of the observed improvement in NTS.
An advantage of the T-NOTECHS is that it is an internationally used validated scale that has been modified specifically for evaluating trauma teams’ NTS. Its interrater reliability is from fair to moderate (12, 17, 18). In the study by Pucher et al. (6) using T-NOTECHS, the interrater reliability scores were not reported. However, significant improvements in T-NOTECHS scores after teamwork training, and their correlation with clinical parameters in simulated and actual trauma resuscitations, indicate the clinical relevance of the tool (12).
In our study, the interrater agreement between the two raters for T-NOTECHS after the first (n = 90) and second (n = 90) simulations was fair (ICC = 0.30). After combining all the simulations (N = 180), the ICC was 0.41. Our results are consistent with those of a prior study using T-NOTECHS, which reported fair interrater reliability (0.44) for a real-time assessment of simulated resuscitation (12). The two raters may focus on different behaviors within the team, while real-time assessment presents a further challenge to the assessment situation. This issue warrants more investigation.
Other advantages of this study are the large research data, and the use of two different assessment methods and two expert raters. These factors increase the relevance of the data, and improve the validity of the study, especially as the assessments produced by the two methods were in close agreement.
Conclusion
A short, structured 2-h high-fidelity in situ multiprofessional trauma team simulation training is effective in improving NTS in hospital trauma teams as evaluated both by self-assessment and by two expert raters. Further investigation is required to explore the clinical effects of the 2-h trauma team simulation course.
Supplemental Material
Supplement_1 – Supplemental material for Short 2-H in Situ Trauma Team Simulation Training Effectively Improves Non-Technical Skills of Hospital Trauma Teams
Supplemental material, Supplement_1 for Short 2-H in Situ Trauma Team Simulation Training Effectively Improves Non-Technical Skills of Hospital Trauma Teams by E. Rosqvist, S. Lauritsalo and J. Paloneva in Scandinavian Journal of Surgery
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This research has obtained institutional review board approval to conduct this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.