
Abstract
Background and Aims:
The Swedish National Patient Insurance Company (LÖF) can compensate patients who believe they have been exposed to an avoidable injury or malpractice in healthcare. Its register covers 95% of Swedish healthcare providers.
Material and Methods:
Data on patients operated for primary or incisional ventral hernia in Sweden between 2010 and 2015 and who had filed a claim, were retrieved from LÖF. A total of 290 cases were identified and included. Files include a copy of records, relevant imaging, and an expert advisor’s opinion.
Results:
Inadvertent enterotomy occurred during 25 repairs and in these cases, laparoscopic repair was clearly overrepresented (p < 0.001). Complications related to the surgical site (infection and ugly scar) were predominantly related to open repairs (p < 0.001). Twenty percentage (57/290) of the claims were directly related to an anesthetic mishap. Univariate ordinal regression showed that the odds of receiving a high reimbursement was significantly increased if laparoscopic repair was performed p < 0.001 (odds ratio: 0.37; 95% confidence interval: 0.21–0.65). Sixty-three percentage of claims were filed by women.
Conclusion:
Inadvertent enterotomy is overrepresented, and the probability that a claim filed for an avoidable injury leads to high reimbursement is greater if laparoscopic repair is performed rather than open ventral hernia repair. The high amount of injuries related to general anesthesia during umbilical hernia repair may be reduced with an increased proportion executed in local anesthesia.
Keywords
Introduction
Historically, hernia surgery research has mostly focused on outcomes such as recurrence and infection. The patient’s own perception of the value and quality of repair and perioperative care remains largely untouched and constitutes an interesting field of exploration that could potentially provide us with unique information. Apart from the use of questionnaires, a valuable source of information on patient opinion is malpractice claims and patient injuries registered with insurance companies. Resources and systems used to investigate avoidable injuries and malpractice claims differ between countries (1, 2).
In Swedish healthcare, all caregivers sign a compulsory patient insurance to protect the patient in case of an avoidable injury during care. The insurance compensates patients, who experience an avoidable injury, for losses that are not compensated by the social insurance system.
All 21 Swedish county councils and regions (10 million inhabitants) have assigned their patients insurance at The Swedish National Patient Insurance Company (LÖF). LÖF’s claim-register covers 95% of all healthcare provided in Sweden. The missing 5% constitutes of private caregivers who have signed their patient insurance with other insurance companies. Annually 16,000 claims are received of which about 40% are compensated. All claims received are stored in a claims database, which today covers over 180,000 entries.
Gender differences in medical treatment and treatment outcome have been reported in numerous fields such as cardiology and nephrology (3, 4), and it is known that more damage claims are filed by women. Claims of malpractice leading to adverse outcome after surgery may be an indicator of substandard care and thus poorer surgical outcome (for women).
Ventral hernia repair is one of the most common procedures in general surgery (3). Over the last decade or so, ventral hernia repair has primarily been performed using prosthetic mesh repair (4). Since the introduction of laparoscopic ventral hernia repair by LeBlanc in 1993, the endoscopic method has increased in popularity and has become widespread internationally (5). Numerous systematic reviews and meta-analyses have been published presenting the evidence regarding the best possible management of ventral hernia repair (3, 6, 7); yet there is still no consensus on the optimal treatment of abdominal wall hernia. Current evidence is too sparse to claim superiority of one method over another, and the heterogeneity of abdominal wall hernias and the lack of standardization of procedures make series difficult to compare.
Several series emphasize the advantages of laparoscopic repair in terms fewer infections and faster return to normal activities (3, 6, 7), while more interesting outcome variables such as intra-abdominal mesh-related complications and long-term risk for recurrence are less well-described (8). Some papers argue that the risk for undetected inadvertent enterotomy increases when using the laparoscopic approach (9). The vast number of products competing on the market and the paucity of monitoring of events after surgery increases the risk of using inferior products and methods, ultimately affecting the patient (8).
A recently published paper linked the Swedish Groin Hernia Register with LÖF records and compared registered data with claims filed. They concluded that risk factors for filing a damage claim after groin hernia repair were acute surgery, operation for recurrence, sutured repair, and general anesthesia (10).
The aims of this study were to investigate trends and patterns of injury claims due to malpractice or errors in ventral hernia surgery, and to identify cases where errors were potentially avoidable. We also explored the possibility of gender differences regarding the frequency of injury claims after ventral hernia repair.
Material And Methods
Patients And Methods
This was a retrospective cohort study. Data were retrieved from the LÖF database on patients who had filed a claim after undergoing surgery for primary or incisional hernia in Sweden between 2010 and 2015. Search terms in the LÖF database were ICD10 diagnosis codes regarding ventral hernia (K42, K43, K45, and K46) and associated surgical procedure codes (JAD, JAF, JAE, JAG). In all, 380 patients were identified. Data were validated by comparison with patient records. After exclusions, 290 patients were included in the final database. A flowchart diagram describing inclusion and exclusion of patients is presented in Fig. 1.
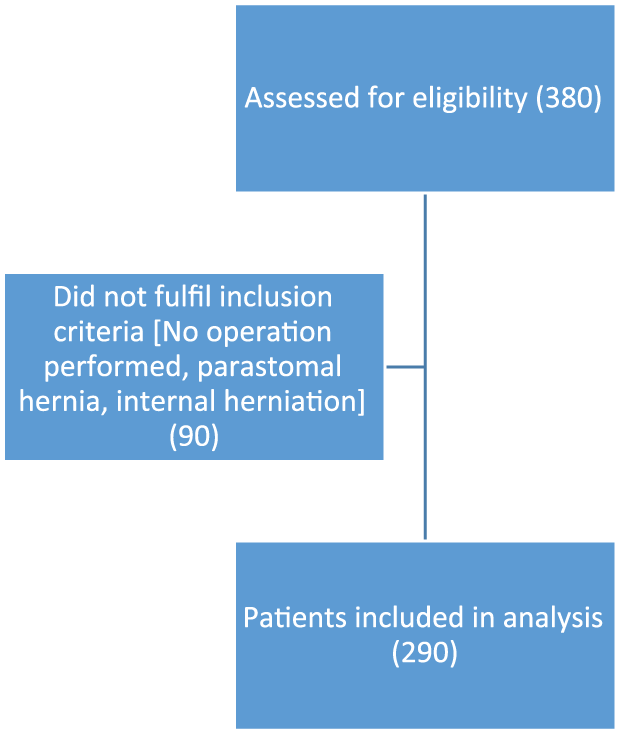
Flowchart of patients included.
To be able to interpret the relationship between the number of claims and the total number of repairs performed, we collected data of ventral hernia procedures between 2004 and 2014 from the Patient registry run by the Swedish National Board of Health and Welfare. Around 68,000 ventral hernia repairs were executed during this period, of which approximately 4100 were laparoscopic repairs. The proportion of laparoscopic repair in the nation was thus around 6% during these years. Annually, approximately 6800 procedures are recorded, which means that less than 1% of procedures leads to a claim.
The definition of “avoidable” in the Swedish patient insurance is a situation where an experienced specialist in the same field of surgery would have chosen another treatment or procedure, or performed the procedure in some other way, whereby the injury could have been avoided. An experienced medical advisor makes this assessment for LÖF. If he or she considers the injury more likely avoidable than not, the claimant is granted compensation.
When LÖF receives a damage claim, all medical records related to that event are retrieved. From these medical records, we were able to collect detailed information of each case included in this study, including details regarding type of surgical repair, habitual parameters, comorbidity, and the final assessment of the expert medical advisor.
The severity of the injury is classified in terms of medical invalidity, as stated in official tables of medical invalidity. For this study, degree of medical invalidity was grouped in six levels shown in Table 1. The level of compensation is based on a legal liability basis, that is, that the level of compensation is the same as if the claim was to be tested in a court of law. Compensation may be granted for adverse events leading to loss of income, expenses, and suffering. Compensation is also granted for permanent invalidity, future loss of income, future expenses, and death.
Showing numbers of claims, open or laparoscopic repair, and the level of reimbursement according to the Swedish National Patient Injury Insurance (LÖF) scale.
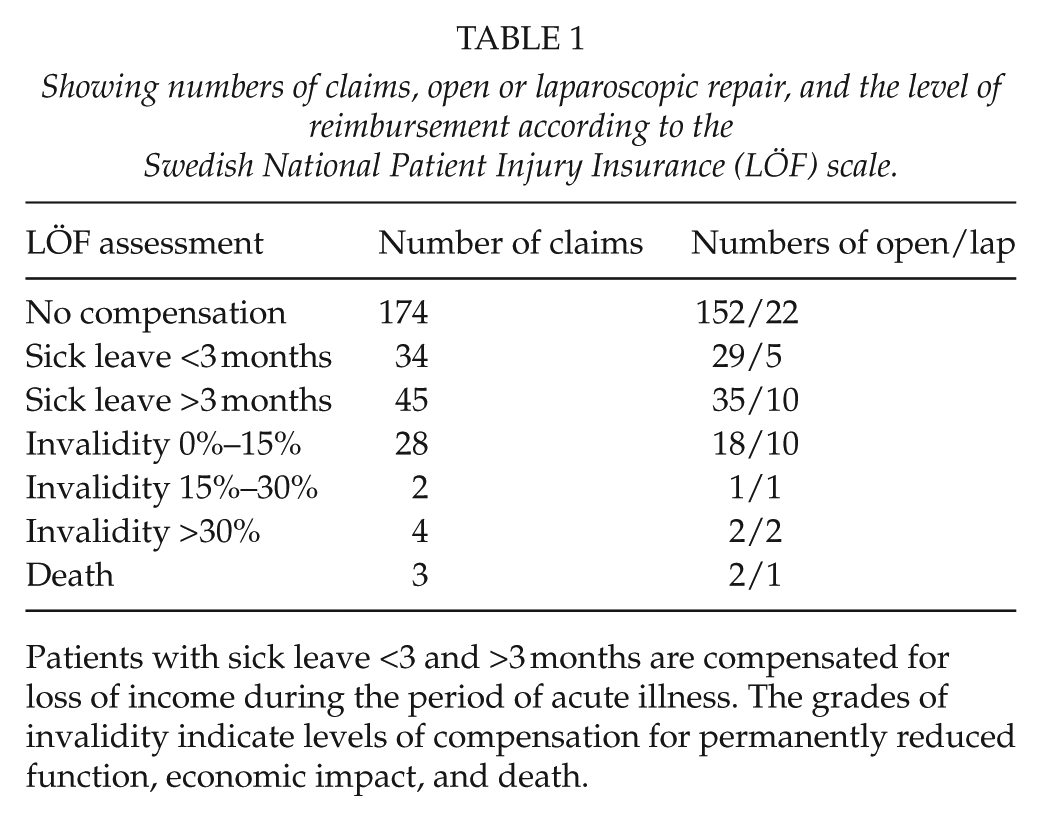
Patients with sick leave <3 and >3 months are compensated for loss of income during the period of acute illness. The grades of invalidity indicate levels of compensation for permanently reduced function, economic impact, and death.
The primary endpoint was to identify patterns in hernia surgery related to severe avoidable injuries. The secondary endpoint was to investigate gender differences in terms of frequency of claims. The study was approved by the Regional Ethics Review Board in Umeå (Dnr 2016/202-31).
Statistical Methods
Patient data were registered in an Access® database (Microsoft Corp.). Statistical analysis of the data was performed using Statistica version 12 (Statsoft, Tulsa, OK, USA). Statistical significance was tested by chi-square analysis where a p value < 0.05 was regarded as significant.
Ordinal regression analysis was performed to analyze the risk of patient injuries using the six groups of medical invalidity as dependent variable. Grading of the injury was considered as a scale of groups forming an ordinal scale rather than a continuous quote scale. Open and laparoscopic surgery as well as gender and age were tested as independent variables.
Results
The number of patients assigned to each medical invalidity category is shown in Table 1. Forty percentage of patients filing a claim received compensation. In the “no compensation” group, LÖF did not consider the complication to be avoidable.
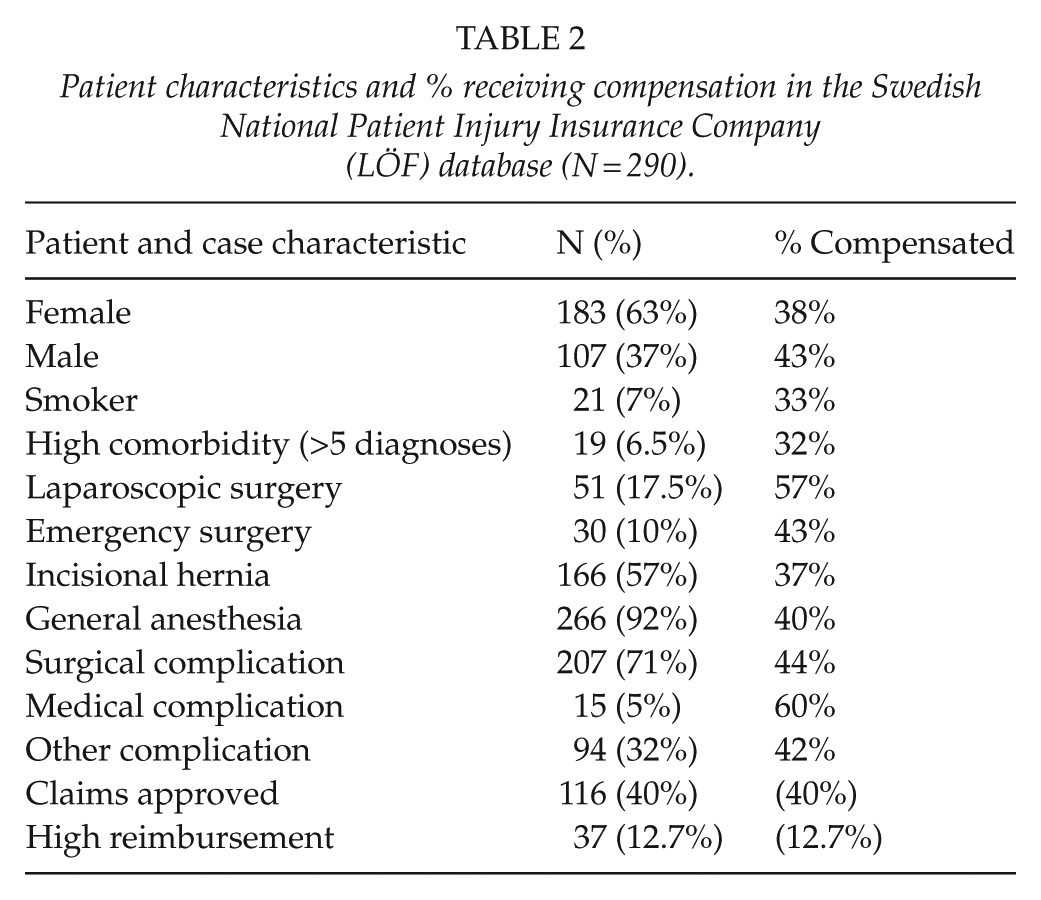
A total of 290 claims filed between 2010 and 2015 were eligible for analysis, and of these, 63% were filed by females. Among the patients filing a claim, 92% were operated under general anesthesia and 57% were incisional hernia repairs. Median age was 62 years. Basic characteristics of the patients are shown in Table 2.
Patient characteristics and % receiving compensation in the Swedish National Patient Injury Insurance Company (LÖF) database (N = 290).
Claims due to a surgical complication were filed in 207 cases. Twenty-six patients claimed both surgical and other/medical complications in the same suit making the total number of complications higher than 290. Table 3 shows the frequency and type of surgical complications involved, the most common being surgical site infection, poor cosmesis, recurrence, pain, and inadvertent enterotomy. Inadvertent enterotomy occurred during 25 repairs, and laparoscopic repair is clearly overrepresented in this group (p < 0.001). Deep infection with abscess was seen in two patients, one after a laparoscopic procedure and one after an open. Complications related to the surgical site (infection and ugly scar) were predominantly associated with open repair (p < 0.001). Nine patients who had an open repair filed a claim because of seroma formation, while this complication was not reported after laparoscopic repair.
Surgical complications, numbers, open and laparoscopic repair, and % patients compensated.
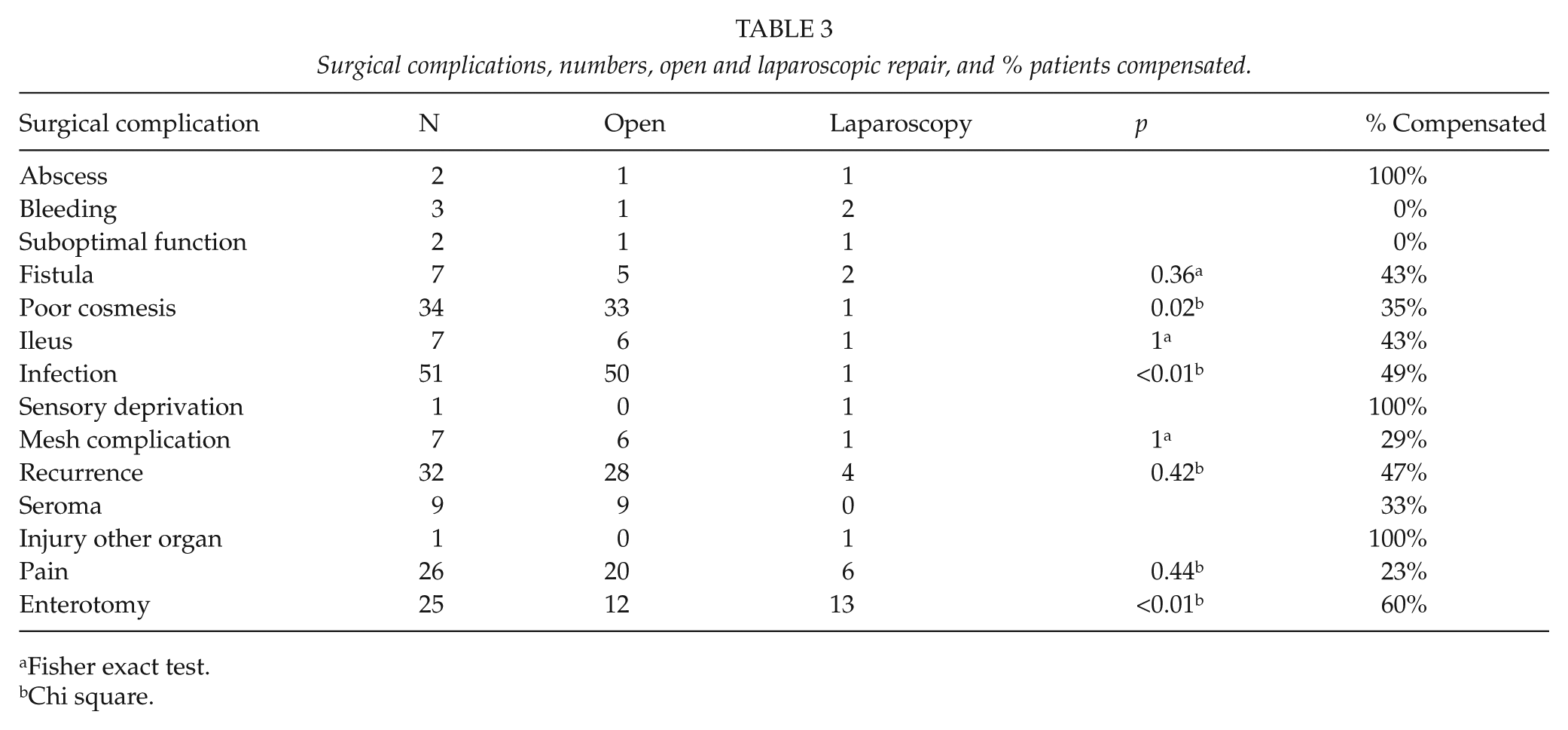
Fisher exact test.
Chi square.
Explantation of the mesh was the basis of fourteen claims; twelve after open repair and two after laparoscopic repair. Negative exploration, missed hernia, and abdominal rectus diastasis-related problems were filed in 19 cases: fifteen women and four men. Female patients filed 28 of 33 (85%) claims due to poor cosmetic result (p = 0.006).
Claims other than surgical or medical complications are here stated as “other complication.” An interesting group comprises 57 cases involving an anesthetic mishap. These cases included 14 women and 6 laparoscopic procedures. The mishaps reported included: suboptimal preparation leading to decubitus; nerve damage related to overextended joints; spinal cord bleeding after epidural anesthesia; and patients falling to the floor during transportation. The major mishap category was dental injuries (32 cases of 57). In all, 20% (57/290) of claims filed were directly related to anesthesia.
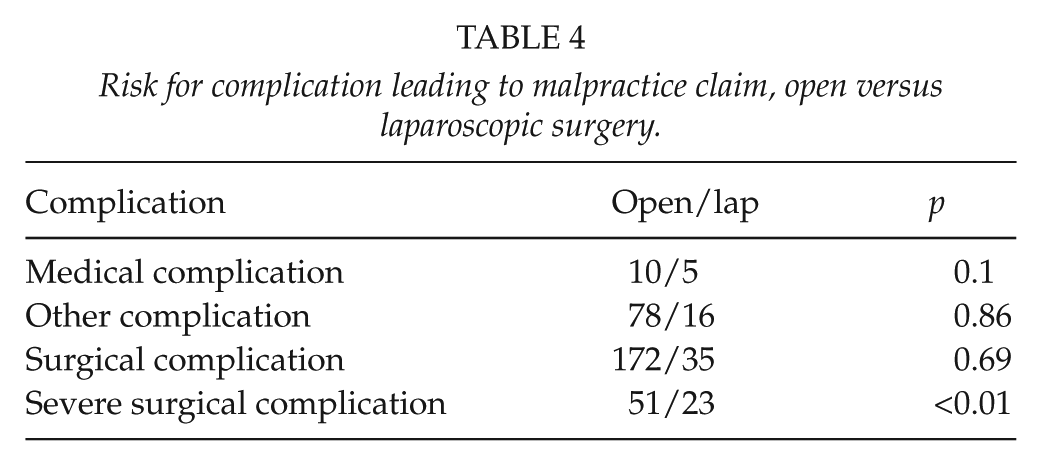
The risk of a severe surgical complication leading to a claim was significantly increased in patients undergoing laparoscopic repair (Table 4). “Severe surgical complication” is here defined as bleeding, inadvertent enterotomy, fistula, ileus, recurrence, and other visceral injury.
Risk for complication leading to malpractice claim, open versus laparoscopic surgery.
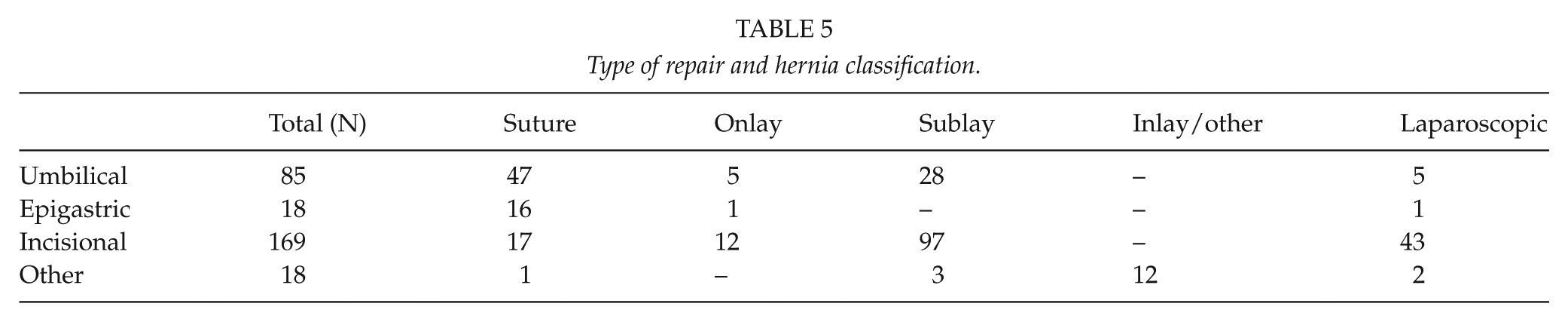
Hernia classification, type of repair and number of patients in each group are found in Table 5.
Type of repair and hernia classification.
There were no significant differences between open and laparoscopic surgery in terms of risk for medical, mild surgical, or other complication in this material. The open approach was used in 50 cases with infection, while the laparoscopic technique accounted for one case. There were 33 claims for an ugly scar using the open approach and one after laparoscopic repair.
Seventy-four patients filed a claim after a simple umbilical hernia repair (K42.9); 46 were sutured repairs of which four were operated under local anesthesia. Ten of the 42 patients operated under general anesthesia filed a claim for injury directly related to anesthesia (dental injury during intubation, etc.).
Univariate ordinal regression analysis compared with open repair with the six classes of medical invalidity as dependent variable showed that the odds of being granted higher reimbursement was significantly greater in cases of laparoscopic repair p < 0.001 (odds ratio (OR): 0.37; 95% confidence interval (CI): 0.21–0.65). Since no significant impact was found for independent patient variables such as gender and age, we did not perform multivariate analyses.
The hernia patients included in this study attended surgical units at all kinds of hospitals. A total of 118 patients were operated at a district hospital, 92 at a county hospital, 32 at a private hospital, and 48 at a university hospital. All types of hospitals performed both open and laparoscopic surgery.
Discussion
The probability that a filed claim due to an avoidable injury after ventral hernia repair will lead to high reimbursement (i.e. a more serious injury) is greater if the operation was performed laparoscopically. Inadvertent enterotomy was clearly overrepresented in the laparoscopic repair group. These results are in agreement with those of a Finnish study reporting patient injuries after ventral hernia repair (9) and data from the Danish hernia database (8).
Complaints regarding the surgical site were relatively common after open repair in this material, stressing the importance of hernia site complication as a key factor in damage claims. These complications were unusual following laparoscopic repair. Similar outcome results have been published in several clinical trials (6). However, such data do not quantify the patient’s suffering. The present material reveals complications that are deemed avoidable and where the effects on the patient’s quality of life have been evaluated by an expert advisor. It is of great importance to stress the difference between a life-threatening complication such as intestinal damage, and the experience of poor cosmesis.
Seroma is a common complication after both open and laparoscopic repair, but no claim because of seroma after laparoscopic repair was found in the LÖF database. Since seroma formation is so common after laparoscopic repair, it is possible that most surgeons prepare the patient for this complication, increasing the patient’s tolerance.
The fact that women were overrepresented in this material might reflect poorer surgical management of the female patient. In the Danish ventral Hernia database, umbilical hernia operations are predominantly performed on men, and epigastric hernia operations are evenly distributed between the sexes (11). If these figures apply to Sweden, then the proportion of operations being performed on women would not explain the difference in the numbers of men and women filing claims.
It is impossible to separate the consequences of anesthesia from surgical research. Twenty percentage of claims filed in this material were due to complications directly related to general anesthesia. The majority of repairs in this material are only suitable for general anesthesia, but an exception is the sutured umbilical hernias. An experienced surgeon should have no trouble in suturing small hernias under local anesthesia. Little has been published on the advantages of local anesthesia in umbilical hernia repair, but this is well established in groin hernia repair (12, 13). It seems reasonable to believe that an increase in the number of umbilical hernia repairs executed under local anesthesia would lead to a decrease in the number of events directly related to general anesthesia.
Negative exploration for suspected hernia or missed hernia are events that could be prevented by better preoperative work-up. Careful clinical examination, radiology in selected cases and sufficient knowledge of the anatomy of the abdominal wall would probably prevent this happening. There are very few papers regarding this issue in the literature but it is frequently discussed with regard to occult groin hernias (14).
Explantation of the mesh used for hernia repair was performed in 14 patients due to infection, resulting in a total abdominal wall catastrophe in some cases, significantly reducing the patient’s quality of life and severely impairing abdominal wall function. A thorough knowledge of the various biomaterials available and their properties is essential. It is of utmost importance to consider the risk of infection, and to choose an implant that may be left in situ and treated conservatively in the case of early infection (16). After carefully reviewing the patients’ records, we believe that most of these mesh explantations were unnecessary.
This material is entirely based on records from patients that have filed a claim. A weakness of this study is therefore that we cannot assess complications that patients have chosen not to report. However, our main ambition was to highlight hernia repair problems from the patient’s point of view, thereby contributing to our understanding of this sparsely described aspect of surgical complications.
Since the material is based on a retrospective cohort, one can argue that there is a considerable risk of selection bias, and comparison between open and laparoscopic repair is hazardous. This is a valid argument and we clearly do not suggest superiority of one method. Our ambition is rather to explore method-related patterns.
It is also important to understand that the patient insurance system does not reflect the prevalence of surgical complications. An accepted method of repair associated with a high complication rate of some kind is unlikely to lead to a claim resulting in compensation since it is considered an expected consequence of the procedure rather than a sign of poor care.
Material based on damage claims, as in this study, does not always lend itself to statistical analysis. After reading more than 290 claims, it is clear that the patient’s perception of quality of care is a reflection of his or her preoperative expectations. This stresses the importance of information and a good relationship between patient and surgeon if one is to achieve optimal satisfaction (17, 18).
Patient satisfaction after surgery is an interesting field of research potentially leading to unique results. The current material reflects a population of 10 million Swedish inhabitants over a period of 6 years, thus constituting one of the largest controlled materials yet published on patient injuries in the modern era of ventral hernia repair.
Footnotes
Acknowledgements
The authors thank LÖF and Pelle Gustavsson for their support and for making this study possible. The authors also acknowledge Thyra Löwenmark for statistical guidance and Peter Cox for linguistic revision.
Ethical Approval
The study was approved by the Regional Ethics Review Board in Umeå (Dnr 2016/202-31).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Visare Norr (VISARENORR552961) and by regional agreement between Umeå University and Västerbotten County Council (VLL-675981).