
Abstract
Background and Aims:
The aim of this study was to evaluate the long-term (5-year follow-up) results of laparoscopic sleeve gastrectomy in terms of weight loss and obesity-related comorbidities, as well as the risk factors associated with postoperative nutritional deficiencies.
Material and Methods:
The first 99 consecutive patients who underwent laparoscopic sleeve gastrectomy for the treatment of morbid obesity between October 2008 and August 2011 at Tartu University Hospital were followed prospectively in cohort study. The outpatient hospital follow-up visits were conducted at 3 months, 1 year, and 5 years postoperatively. At 5 years, the follow-up rate was 90.9%; 86 laparoscopic sleeve gastrectomy patients were included in final analysis.
Results:
The mean excess weight loss (%EWL) was 44.3% ± 13.0%, 75.8% ± 23.1%, and 61.0% ± 24.3% at 3 months, 1 year, and 5 years, respectively. A linear association between preoperative weight and weight at 5 years was found. Remission rates at 5-year follow-up for type 2 diabetes, hypertension, dyslipidemia, and obstructive sleep apnea were 68.8%, 32.7%, 27.4%, and 61.5%, respectively (all p < 0.05). There was a statistical difference (p < 0.05) in the dynamics of triglyceride, low-density lipoprotein, and high-density lipoprotein level at 5-year follow-up but the level of total cholesterol did not show significant improvement. The risk for cumulative iron, vitamin B12 deficiency, and anemia was 20%, 48%, and 28%, respectively.
Conclusion:
In conclusion, laparoscopic sleeve gastrectomy ensured long-term excess weight loss 61.0% at 5 years. Laparoscopic sleeve gastrectomy has a long-term effect on significant improvement in the median values of triglycerides, low-density lipoproteins, and high-density lipoproteins, but not on total cholesterol levels. There is a risk of postoperative vitamin B12 and iron deficiency.
Introduction
According to the World Health Organization, there are more than 600 million obese adults in the world and bariatric surgery is currently the most effective treatment for severe obesity (1, 2).
Sleeve gastrectomy was initially used as the first stage of the duodenal switch procedure in morbidly obese patients. Since the beginning of this century, due to the development of endoscopic surgery and good short-term results, laparoscopic sleeve gastrectomy (LSG) has gained popularity as a single weight loss procedure. In 2013, LSG was the second most common bariatric procedure in Europe after laparoscopic Roux-en-Y gastric bypass (LRYGB) (3). According to the ASMBS, LSG has been the most popular bariatric procedure in the Unites States since 2014 (4).
The postoperative results of LSG are comparable to those of LRYGB regarding weight loss and resolution of comorbidities (5–7). A systematic review by Switzer et al. (6) demonstrated resolution of T2DM in 60.8% of LSG patients (n = 402) at 5-year follow-up. Dicker et al. (7) compared LSG with LRYGB and laparoscopic banding and found a 54.4% resolution rate for T2DM at 5-year follow-up with no statistical long-term difference between the groups. Salminen et al. (5) also found no significant difference in diabetes remission at 5 years between the LSG and LRYGB groups. Weight loss has been found to be the strongest predictor of diabetes remission after bariatric surgery (6). Older age, higher baseline HbA1c and treatment with insulin are considered negative prognostic factors for remission (7).
Long-term results about the influence of LSG on lipid metabolism have not been thoroughly investigated and the results are varying. Rawlins et al. (8) published a 46.9% prevalence of preoperative dyslipidemia (23/49) with a 5-year resolution rate of 100%, Alexandrou et al. (9) reported an 84% prevalence of dyslipidemia with an 80% of resolution rate at 5 years in LSG patients. In their Updated Systematic Review and Meta-analysis, Chang et al. (10) reported 28% patients having dyslipidemia, with a remission rate of 76% for randomized controlled trials and 68% for observational studies.
Nutrient deficiencies have been shown to occur after all types of bariatric surgery. Moize et al. (11) found no significant long-term differences in nutritional deficiencies between the LSG and gastric bypass groups. The aim of this study was to evaluate the long-term (5-year follow-up) results of LSG in terms of weight loss and obesity-related comorbidities, as well as the risk factors associated with nutritional deficiencies.
Materials and Methods
This is a prospective cohort study of the first 99 patients who underwent LSG for the treatment of morbid obesity between October 2008 and August 2011 at Tartu University Hospital. All patients fulfilled the criteria for bariatric surgery: each had a body mass index (BMI) of >40, or >35 with certain obesity-related comorbidities. The patients were followed prospectively with planned outpatient hospital visits at 3 months (limited data package collected), 1 year, and 5 years postoperatively. The 2-, 3-, and 4-year follow-up visits were assigned to the family doctor.
The collected data comprised demographics, weight, BMI, prevalence of comorbidities, duration of operation, complications, reoperations, use of vitamins/microelements, and blood sampling. The data collected at follow-up visits at 1 year and 5 years postoperatively were weight, reported minimal postoperative weight, resolution or improvement of comorbidities, occurrence of anemia and other pathological changes in blood tests, vitamin and microelement usage. Cumulative deficiency of vitamins and microelements was evaluated and defined as abnormal blood test results at 1-year or 5-year follow-up or history of using iron or vitamin B12 supplementation additionally to multivitamins. This study was approved by the Ethics Committee of the University of Tartu (study no. 12089) and written informed consent was obtained from all patients.
Comorbidities
Diabetes was defined as previous diagnosis and treatment, as reported by the patient, or preoperative glycohemoglobin ⩾6.5% (12). Postoperative remission of T2DM was defined as discontinuation of all medications for diabetes, as reported by the patient, and HbA1c < 6.5%. Hypertension was defined as previously diagnosed hypertension, treated with antihypertensive medication, as reported by the patient. Remission from hypertension was defined as discontinuation of medication and improvement was defined as lowering the dosage of antihypertensive medication. Patients who reported symptoms like snoring and excessive daytime sleepiness were referred for polysomnography at the Sleep Medicine Center at Tartu University Hospital where moderate OSA was diagnosed at AHI (apnea–hypopnea index) 15–30 and severe OSA was diagnosed at AHI > 30 (13). Remission of OSA was defined as discontinuation of treatment with CPAP (continuous positive airway pressure therapy), and improvement was defined as subjective relief of symptoms as reported by the patient. Dyslipidemia was diagnosed when total cholesterol level was higher than 5.2 mmol/L (>200 mg/dL), low-density lipoprotein (LDL) level > 4.14 mmol/L (>160 mg/dL), triglyceride (TG) level > 2.26 mmol/L (>200 mg/dL), or high-density lipoprotein (HDL) level lower than 1.04 mmol/L (40 mg/dL) for men and <1.3 mmol/L (<50 mg/dL) for women (14). Systematic data on proton pump inhibitor (PPI) usage were not collected.
Surgical Technique
All LSG operations were performed by two surgeons (T.S. and T.T.) who used the standardized laparoscopic technique; there were no conversions. The greater curvature was dissected using an ultrasound scalpel. Bougie size was 32–35 Fr (40 Fr for the first three patients Resection started 3 cm from the pylorus. No stapler line enforcement or oversuturing was used. The methylene blue test was employed to discover leakages. The specimen was removed via a 12 mm trocar on the left side.
Altogether 20 simultaneous operations were performed on 19 patients. In 17 patients, laparoscopic cholecystectomy was undertaken because of cholelithiasis found on a preoperative abdominal ultrasound. Three herniotomies were performed due to umbilical hernia. One patient underwent both herniotomy and laparoscopic cholecystectomy. This study involves patients operated during the learning curve of the surgeons and the bariatric center.
Perioperative Complications
For the 99 operations, there were no conversions and mortality rate was 0%. During the first 30 postoperative days, two patients (2%) underwent reoperation: a laparoscopic drainage of a subdiaphragmal abscess on the third postoperative day in one case, and a laparotomy for small bowel injury on the operating day in the other case. There were two rehospitalisations (2%) during the first 30 postoperative days. Two days after discharge from the hospital, a patient was readmitted with stapler line leakage which was treated conservatively. Three weeks after discharge, another patient was diagnosed with thrombosis of the portal and superior mesenteric veins, which was treated with anticoagulation. The overall leakage rate was 2% (2/99).
Postoperative Nutrition And Deficiencies
Postoperatively, the patients were recommended to regularly take multivitamins containing at least 200 µg of folic acid (100% Recommended Dietary Allowance [RDA]), 14 mg of iron (100% RDA), 1 µg of vitamin B12 (40% RDA), and Zn, Se (e.g. Apovit®). Data were collected about multivitamin usage and additional replacement therapy during the 5-year postoperative period as prescribed by the surgeon or the general practitioner.
Cumulative deficiencies were defined as abnormal blood test results at 1-year or 5-year follow-up or history of using additional iron or vitamin B12 supplementation. Anemia was defined as hemoglobin level lower than 117 g/L in women and lower than 134 g/L in men. Vitamin B12 deficiency was defined as vitamin B12 level lower than 145 pmol/L. Ferritin deficiency was defined as ferritin level below 30 µg/L in men and below 13 µg/L in women. Protein deficiency was defined as serum protein level below 64 g/L (reference values set by the United Laboratories of Tartu University Hospital).
Statistics
The data were analyzed using the Statistica® version 13 software package. Continuous variables were presented as mean values with standard deviation, data with a non-normal distribution were presented as medians with the lower and upper quartiles, and nominal variables were presented as relative frequencies. Comparison between the groups was performed using the Student t-test for continuous variables, and the z-test for relative frequencies. McNemar’s test was employed to analyze significance of resolution of comorbidities. The non-parametric Wilcoxon Sign test was used for assessing differences between the biomarkers preoperatively versus 5 years. Multiple backward stepwise linear regression was used to evaluate factors predicting %EWL at 5 years. Multiple logistic regression was performed to evaluate risk factors for weight loss failure and cumulative ferritin, vitamin B12 deficiency, or anemia. The evaluated factors for predicting EWL% at 5 years and risk factors for weight loss failure were patient age, preoperative weight, gender, occurrence of T2DM (type 2 diabetes mellitus), hypertension, dyslipidemia, and OSA (obstructive sleep apnea). The risk factors evaluated for cumulative vitamin B12 or ferritin deficiency or anemia were age, preoperative weight, preoperative level of hemoglobin, preoperative level of vitamin B12, preoperative level of ferritin, and %EWL at 5-year follow-up. Receiver operating characteristic (ROC) curve analysis was performed to find a cut-off point for preoperative vitamin B12 level predicting long-term vitamin B12 deficiency. All statistical tests were two-sided and p ⩽ 0.05 was considered significant.
Results
Patient Characteristics
The basic demographics and prevalence of concomitant diseases of the 99 operated patients and of the 86 analyzed patients are presented in Table 1. The 5-year follow-up rate was 90.9% (90 patients out of 99). Eight patients lost to follow-up were not reachable via the provided contact data and one patient had died (from cerebral infarction 3 years after bariatric surgery). In addition, four patients who had undergone a bariatric reoperation were excluded from analysis. All four patients had received LRYGB 3 to 4 years after LSG: two due to weight regain, one for severe reflux disease, and one for both reasons. Final analysis was based on 86 “pure” LSG cases with the mean 5-year follow-up at 62 months (range: 55–75 months). Calculation of weight loss failure includes three patients who were reoperated for weight regain.
Demographic data of the 99 LSG patients and of the 86 included in final analysis.
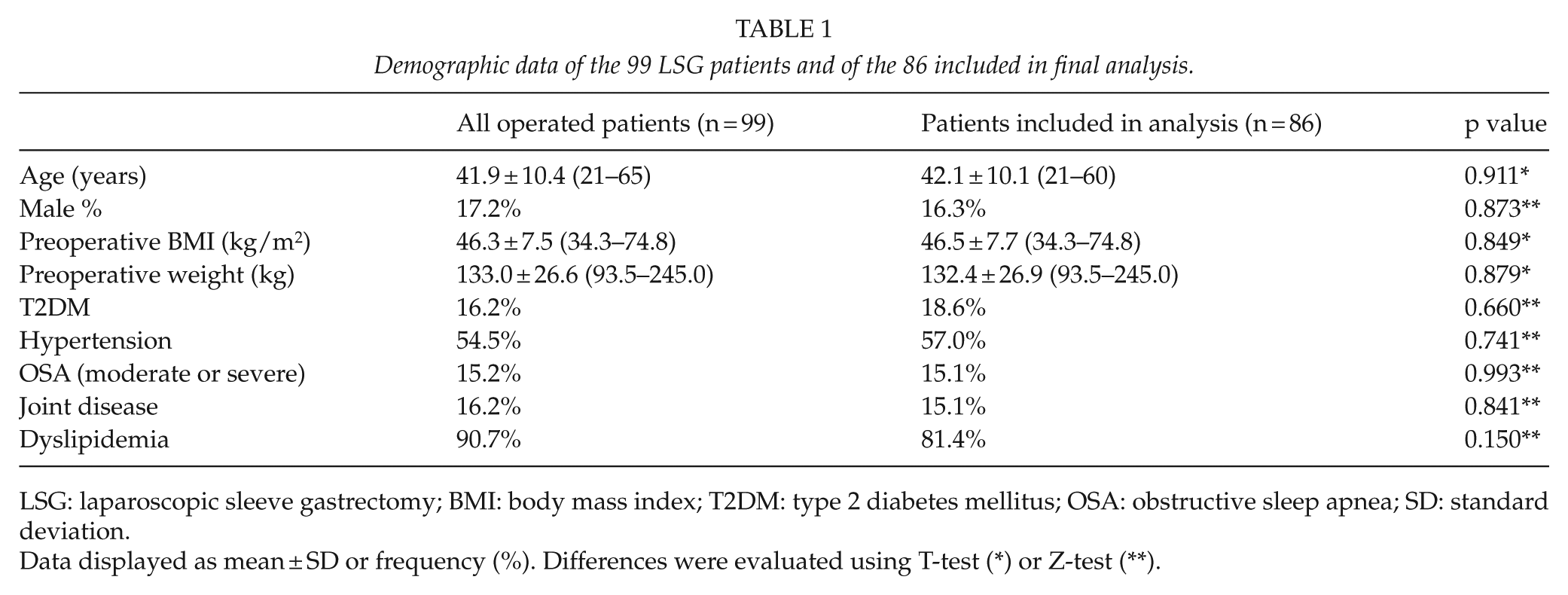
LSG: laparoscopic sleeve gastrectomy; BMI: body mass index; T2DM: type 2 diabetes mellitus; OSA: obstructive sleep apnea; SD: standard deviation.
Data displayed as mean ± SD or frequency (%). Differences were evaluated using T-test (*) or Z-test (**).
Seventy-two out of the 86 patients were female with the mean BMI of 45.1 ± 6.2. The mean BMI of the male patients was 53.7 ± 10.4.
The mean excess weight loss (%EWL) for the 86 analyzed patients was 44.3% ± 13.0%, 75.8% ± 23.1%, and 61.0% ± 24.3% at 3 months, 1 year, and 5 years, respectively (Fig. 1). A mean maximum %EWL of 85.4% ± 25.6% was usually achieved between the first and second postoperative year. Using multiple linear regression, the only predictors for higher 5-year %EWL was lower preoperative weight or BMI (p = 0.002 or p = 0.004, respectively). Fig. 2 shows a linear association between preoperative weight and weight at 5 years (R2 = 0.71). There was no association with age, gender, or prevalence of any comorbidities. Seven patients (7%) underwent a laparoscopic cholecystectomy due to symptomatic cholelithiasis during the follow-up period. Twenty-two patients (22%) underwent an abdominoplasty. There was no postoperative incisional hernia or bowel obstruction.
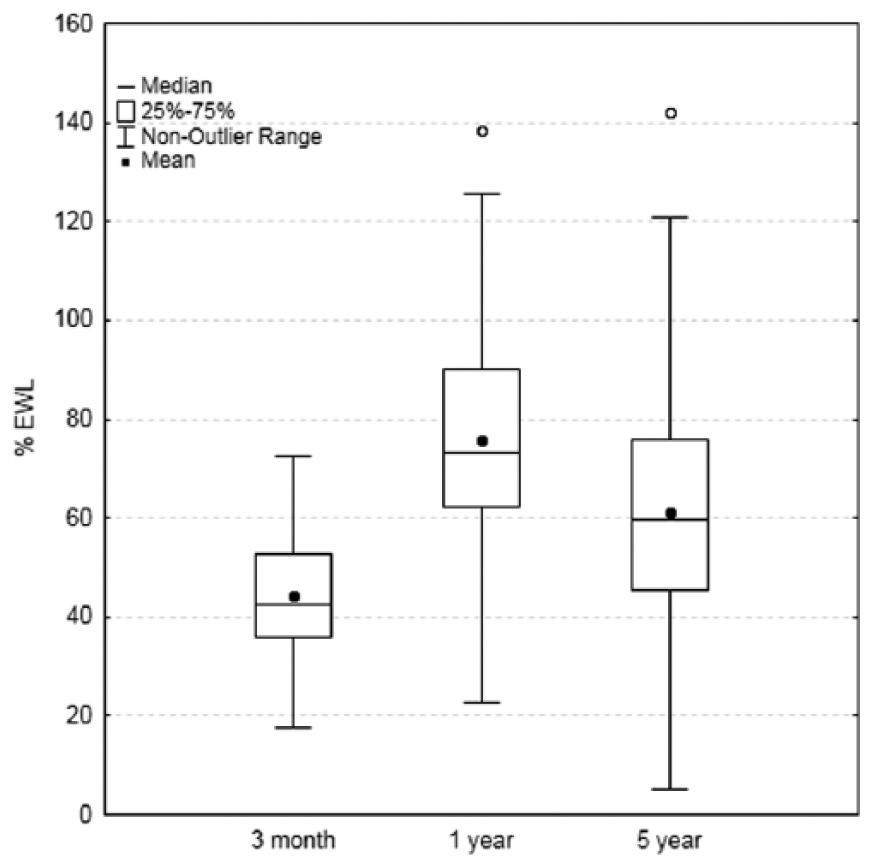
Dynamics of excess weight loss (%EWL) for the 86 analyzed LSG patients.
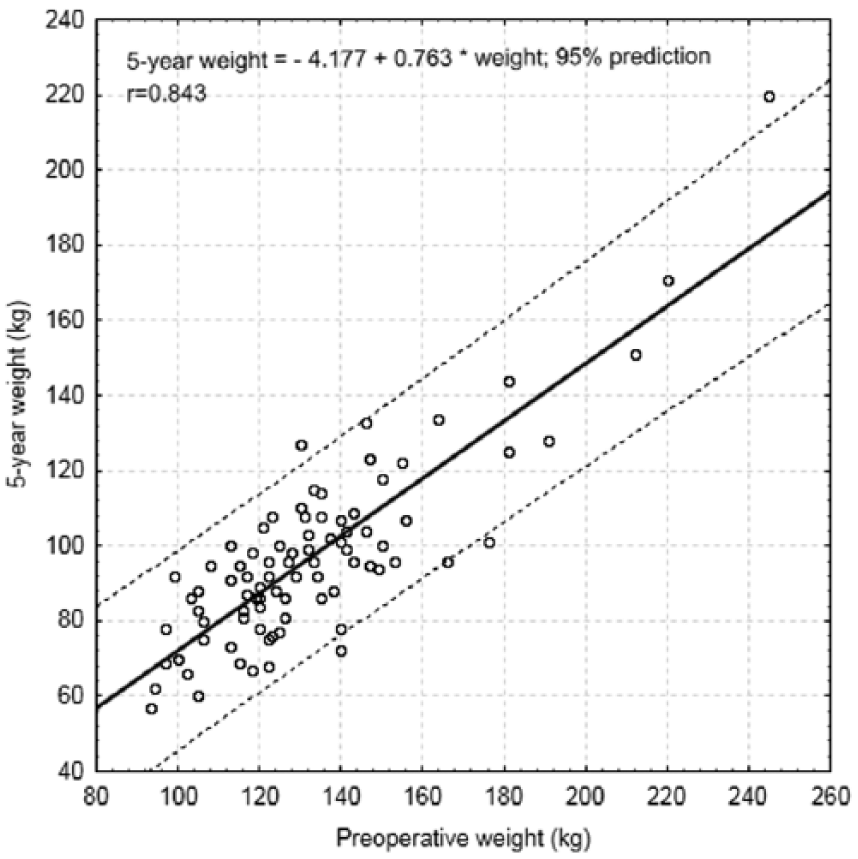
Linear association between preoperative weight and weight at 5 years.
Comorbidities
Twenty-four patients out of the 86 (27.9%) did not have any comorbidities. Prevalences of obesity-related comorbidities are presented in Table 1. All diabetic patients were treated perorally; there were no insulin users. The mean duration of T2DM was 29.7 ± 29.6 months (range: 2–120 months). The median HbA1c (glycohemoglobin) in the diabetic population was 5.9 (5.4–7.8)%. Total cholesterol was over 5.2 mmol/L in 42 patients (48.8%), 31 patients (36.1%) had hypertriglyceridemia, LDL was above the reference value in 26 patients (30.2%), and HDL was below the reference value in 51 patients (59.3%).
Using the McNemar test, we found a statistically significant remission of comorbidities at 5-year follow-up. Of the 16 diabetic patients, 11 (68.8%) achieved total remission (p = 0.003) and 3 (18.8%) showed improvement. The overall median glycohemoglobin level was 5.9 (5.6–6.2)% preoperatively and 5.5 (5.3–5.7)% both at 1 year and 5 years postoperatively (baseline vs 5 years p ≤ 0.001). Remission from hypertension occurred in 32.7% (16/49) (p = 0.002) and improvement occurred in 15 patients (30.6%). Obstructive sleep apnea resolved or improved in eight patients (61.5%, p = 0.013).
Dyslipidemia resolved in 17 patients (27.4%, p = 0.004); there were three de novo cases of dyslipidemia at 5-year follow-up. When comparing the median level of cholesterol preoperatively and at 5 years, there was no statistically signicant change. (Table 3). However, there occurred a statistically significant change in HDL (p ≤ 0.001), LDL (p = 0.045), and TG (p ≤ 0.001).
Postoperatively, at 5-year follow-up, 10 patients reported taking PPIs regularly and 22 patients reported taking them irregularly as needed. Joint disease had resolved in three patients (p = 0.248).
Nutrient Deficiencies
At 5-year follow-up, 50% of the patients (43/86) used vitamins regularly and 14% (12/86) used them irregularly. Of the patients, 34% (29/86) were not using multivitamins, 37% (32/86) of the patients took peroral iron supplements, and 12% (10/86) received intramuscular or peroral additional vitamin B12. In 13% (11/86) of the cases, vitamin D supplements were recommended to patients because of low vitamin D (25-(OH)D3) levels in blood. The statistically significant reduction occurred in preoperative and 5-year hemoglobin, ferritin, and vitamin B 12 median levels (Table 3).
Cumulative anemia was found in 28% (24/86) of the patients. Cumulative ferritin deficiency occurred in 47% (40/86) of the patients. Of the men, 43% (6/14) had ferritin level below 30 µg/L and 47% (34/72) of the women had ferritin level below 13 µg/L. Cumulative vitamin B12 deficiency was found in 20% (17/86) of the patients: in 7% (1/14) of the men and in 22% (16/72) of the women.
Using backward stepwise logistic regression, the only risk factors for cumulative anemia or vitamin B12 or ferritin deficiency were lower (but not below the reference value) preoperative levels of vitamin B12 (p = 0.005) and ferritin (p = 0.022). The patient age, weight, preoperative level of hemoglobin, and 5 years %EWL were non-significant risk factors. The analysis of the ROC curve yielded a cut-off point of 255.7 pmol/L for vitamin B12, meaning that the patients whose preoperative vitamin B12 level is lower than the cut-off value are more predisposed to postoperative vitamin B12 deficiency, sensitivity was 0.94 (95% confidence interval (CI) 0.70–1.00), and specificity was 0.71 (95% CI: 0.58–0.82).
Weight Loss Failure
Failure rate (%EWL < 50%) was 36% (32/89) at 5-year follow-up, including three reoperated patients. Six patients did not achieve sufficient weight loss and 26 patients out of 32 who had achieved sufficient weight loss at 1-year follow-up had regained weight at 5-year follow-up. The average weight regained between the first and the fifth postoperative year was 18.5 kg (range: 4–36 kg). Inclusion of the nine patients lost to follow-up as failures would have yielded a failure rate of 41.4% (41/99).
Logistic regression for predicting weight loss failure (%EWL < 50%) revealed hypertension as a statistically significant risk factor (p = 0.047) (Table 2). Hypertension remained a significant risk factor for weight loss failure when backward stepwise regression was used (p = 0.013).
Risk factors for weight loss failure (5-year %EWL < 50%).
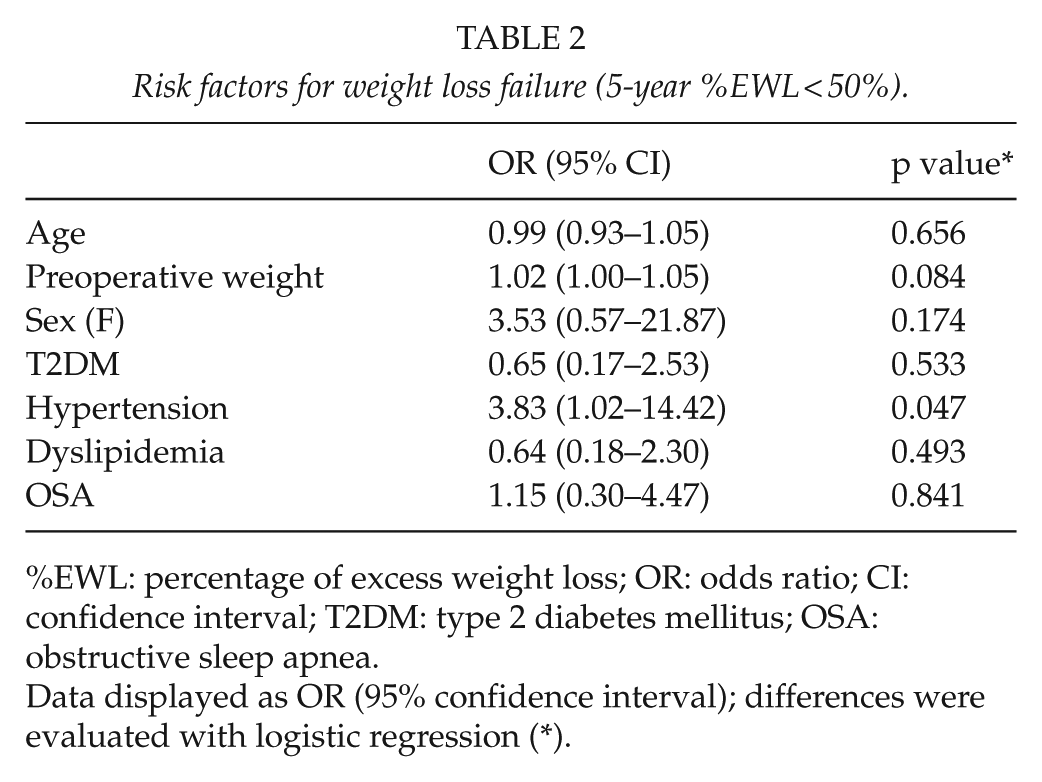
%EWL: percentage of excess weight loss; OR: odds ratio; CI: confidence interval; T2DM: type 2 diabetes mellitus; OSA: obstructive sleep apnea.
Data displayed as OR (95% confidence interval); differences were evaluated with logistic regression (*).
Discussion
Despite the increasing popularity of LSG, reliable data about long-term results are still limited. Most of the published studies include a small number of patients with follow-up rates less than 80%. In this study, the follow-up rate was 90.9%.
The mean age and the male:female ratio for the patients of this study are comparable to the corresponding indicators reported in the long-term results of other studies (5, 15–17). The mean preoperative BMI in our study is 46.5 ± 7.7, which can be considered an average preoperative characteristic according to a review by Diamantis et al. (18) The 61.0% EWL at 5 years in our study is consistent with and even slightly higher than that reported in most long-term studies (49.0%–62.9%) (5, 8, 18–22). According to the Reinhold criteria (%EWL higher than 50%), the success rate at 5 years was 64% (23). This result is comparable with other published data of success rate 42%–68% (8, 24, 25). The only predictor for long-term %EWL in this study was preoperative weight (or BMI based on weight).
Like other authors, we also noted weight regain between the first and the fifth year (Fig. 1) (19, 20, 22). Himpens et al. (22) suggested that the cause of weight regain could be hyperactivity of the previously silent ghrelin-producing cells and formation of a “neofundus.” A removed gastric volume of <500 mL could be a predictor of failure (26). Patient behavior and dietary choices are, too, contributors to weight regain. It has been noted that better patient support may lead to more lasting long-term results (27).
We found hypertension to be a significant risk factor for predicting weight loss failure; backward stepwise regression confirmed the result. Patients with hypertension had 3.8 times higher odds to have weight loss failure. This finding has not been reported before and needs to be further investigated on a larger number of patients.
Although the preferred surgical intervention for diabetic patients at our hospital is LRYGB, 18.6% of the LSG patients in this study had T2DM; of these patients, 68.8% achieved total remission at 5-year follow-up and, additionally, 18.8% showed improvement. Abbatini et al. (28) reported T2DM remission in 76.9% of the small number of patients (n = 13) 5 years after LSG and found a cut-off point of diabetes duration of 10 years to be a significant prognostic factor for failure.
The LSG patients studied by us used only peroral T2DM treatment, the mean duration of their disease was 29.7 months and the median preoperative HbA1c was 5.9%. These factors could have contributed to the relatively high resolution of T2DM at 5-year follow-up. Also, it should be noted that the literature offers different definitions (HbA1c references) of T2DM diagnosis and resolution (6, 14).
Likewise, dyslipidemia has heterogenous definitions in the literature. Brethauer et al. (14) published a guideline for standardizing outcome reporting in bariatric surgery, which includes a definition of hyperlipidemia that fits the definition adopted in this study.
Compared to the literature data, the LSG patients in our study had high preoperative rate (81.4%) of dyslipidemia (5, 8–10, 29, 30). The high levels of total cholesterol in 48.8% of the patients and the low levels of HDL in 59.3% can be attributed to that circumstance. Notably, there was a statistically significant improvement in the median levels of HDL, LDL, and TG at 5-year follow-up compared to the baseline values but no statistically significant change in total cholesterol levels. Golomb et al. (31) found no significant difference in the change of total cholesterol, LDL, HDL, or triglyceride levels preoperatively versus 5 years. In contrast, Peterli et al. (30) found a statistically significant change in total cholesterol, HDL, and TG levels at baseline versus 5 years after LSG.
A major controversial issue in sleeve gastrectomy is the risk of reflux disease. Of the patients, 32/86 (37%) used PPI at 5-year follow-up. Unfortunately, no adequate data for preoperative PPI usage were collected. The high percentage of PPI users among the LSG patients at long-term follow-up points out the need for careful preoperative evaluation and patient selection. In addition, three patients underwent bariatric reoperation due to reflux disease (one patients also had a weight regain).
The patients of the present study were recommended to take lifelong multivitamin supplements postoperatively. At 5-year follow-up, only 50% (43/86) of them used vitamins regularly. A similar result (54% of regular vitamin users) was described by Gillon et al. (32), which illustrates low long-term adherence to supplementation.
As noted by other authors, it is difficult to compare studies on nutritional deficiencies due to different approaches to postoperative vitamin and mineral supplementation prescribed by surgeons. Some patients receive supplementation because of detected low levels of minerals or vitamins (e.g. vitamin B12, iron, folate). To take account of all deficiencies, we analyzed the patients taking vitamin B12 or iron supplementation, in addition to regular multivitamins, as cumulatively deficient. The risk factors for cumulative anemia or for vitamin B12 or ferritin deficiency were lower preoperative levels of vitamin B12 and ferritin. We found a statistically significant decrease in the ferritin levels between the preoperative value and the value at 5 years (Table 3). There was no significant difference in the prevalence of nutritional deficiencies at 5 years between the regular and irregular multivitamin users, and the patients who did not take multivitamins. The authors would like to point out that during the study period, the recommended use of multivitamins did not ensure a sufficient amount of vitamin B12 or iron. In the recent 2017 Nutritional Guidelines by ASMBS (American Society for Metabolic and Bariatric Surgery), the recommended dose of vitamin B12 after bariatric surgery is 350–500 µg daily and the recommended iron dose after sleeve gastrectomy is 45–60 mg daily (33). Our findings support the need for adequate vitamin B12 and iron replacement, especially in patients with lower preoperative levels of vitamin B12 and ferritin.
Dynamics of the median values of biochemical parameters in the LSG patients.
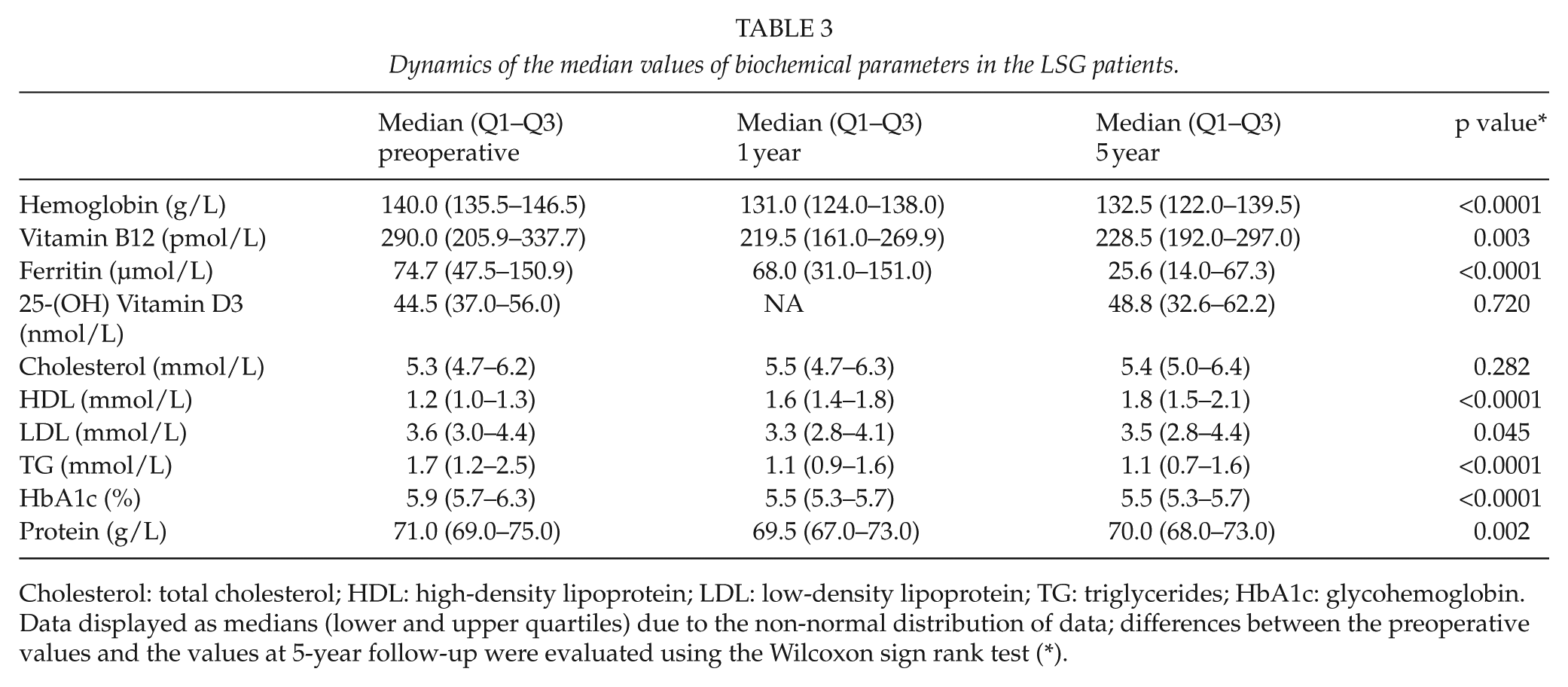
Cholesterol: total cholesterol; HDL: high-density lipoprotein; LDL: low-density lipoprotein; TG: triglycerides; HbA1c: glycohemoglobin.
Data displayed as medians (lower and upper quartiles) due to the non-normal distribution of data; differences between the preoperative values and the values at 5-year follow-up were evaluated using the Wilcoxon sign rank test (*).
Protein deficiency was found in nine patients (10%); however, in all cases, it was mild and clinically not relevant.
Patients were followed at 3 months, 1 year, and 5 years postoperatively. High nutrient deficiency rate found in this study supports the need for frequent follow-up vistis as suggested in most guidelines.
In conclusion, LSG ensured a long-term %EWL of 61.0% at 5 years and a resolution rate of 68.8% for T2DM. LSG has a long-term effect on significant improvement in median values of TG, LDL, and HDL but not in total cholesterol levels. A linear association between preoperative weight and weight at 5 years was found. There is a risk of cumulative postoperative vitamin B12 and iron deficiency.
Footnotes
Ethical Approval and Informed Consent
This study was approved by the Ethics Committee of the University of Tartu (study no. 12089) and written informed consent was obtained from all the patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Trial Registration
ClinicalTrials.gov Identifier: NCT03467581.