
Abstract
Background and Aims:
This study was designed to analyze the feasibility of laparoscopic right posterior sectionectomy compared to laparoscopic right hemihepatectomy in patients with hepatocellular carcinoma located in the posterior segments.
Material and Methods:
The study included patients who underwent either laparoscopic right posterior sectionectomy or laparoscopic right hemihepatectomy for hepatocellular carcinoma located in segment 6 or 7 from January 2009 to December 2016 at Samsung Medical Center. After 1:1 propensity score matching, patient baseline characteristics and operative and postoperative outcomes were compared between the two groups. Disease-free survival and overall survival were compared using Kaplan–Meier log-rank test.
Results:
Among 61 patients with laparoscopic right posterior sectionectomy and 37 patients with laparoscopic right hemihepatectomy, 30 patients from each group were analyzed after propensity score matching. After matching, baseline characteristics of the two groups were similar including tumor size (3.4 ± 1.2 cm in laparoscopic right posterior sectionectomy vs 3.7 ± 2.1 cm in laparoscopic right hemihepatectomy, P = 0.483); differences were significant before matching (3.1 ± 1.3 cm in laparoscopic right posterior sectionectomy vs 4.3 ± 2.7 cm in laparoscopic right hemihepatectomy, P = 0.035). No significant differences were observed in operative and postoperative data except for free margin size (1.04 ± 0.71 cm in laparoscopic right posterior sectionectomy vs 2.95 ± 1.75 cm in laparoscopic right hemihepatectomy, P < 0.001). Disease-free survival (5-year survival: 38.0% in laparoscopic right posterior sectionectomy vs 47.0% in laparoscopic right hemihepatectomy, P = 0.510) and overall survival (5-year survival: 92.7% in laparoscopic right posterior sectionectomy vs 89.6% in laparoscopic right hemihepatectomy, P = 0.593) did not differ between the groups based on Kaplan–Meier log-rank test.
Conclusion:
For hepatocellular carcinoma in the posterior segments, laparoscopic right posterior sectionectomy was feasible compared to laparoscopic right hemihepatectomy when performed by experienced laparoscopic surgeons.
Keywords
Introduction
Although liver transplantation provides the highest probability for definite cure of hepatocellular carcinoma (HCC), liver resection is frequently performed with the goal of decreasing morbidity and prolonging survival. Since the advent of minimally invasive abdominal surgery, laparoscopic liver resection (LLR) has become common in many medical centers around the world (1–6). The feasibility of LLR for HCC has been reported in numerous studies with most showing similar oncological outcomes with few instances of operative bleeding and fast recovery despite longer operation time (7–10).
In 2008, the Louisville Statement noted that major liver resection should be performed by experienced surgeons (11). LLR difficulty levels based on the Iwate criteria were proposed at a conference in Morioka (4, 5). The criteria classified right or left hepatectomy as advanced difficulty with an index of 7. Posterior sectionectomy was classified as expert difficulty. Although right hemihepatectomy removes a considerable amount of liver parenchyma compared to right posterior sectionectomy, the surgical difficulty of laparoscopic right posterior sectionectomy (LRPS) is considered greater than laparoscopic right hemihepatectomy (LRHH).
For HCCs in the posterior segments 6 and 7, right posterior sectionectomy can be an optimal treatment if resection yields adequate free margins. Right posterior sectionectomy is especially valuable when the liver is cirrhotic. Yip et al. (12) published a study comparing the outcomes of right posterior sectionectomy and right hemihepatectomy for HCCs in the posterior segments. However, the feasibility of LRPS for HCC in the posterior segments based on the comparison of its outcomes to LRHH has not been investigated. Therefore, in this study, the feasibility of LRPS and whether it provides similar oncological outcomes as LRHH for HCCs in the posterior segments were analyzed.
Methods
Patients and data
Data of patients who underwent LRPS or LRHH for HCC in posterior segments 6 and 7 from January 2009 to December 2016 at Samsung Medical Center were analyzed. Patients who had HCC in segment 5 or 8 were excluded. Patient data were reviewed from our prospectively updated HCC database. Data on demographics, pathology, surgery, and clinical course were reviewed. All three surgeons who performed LLR were experienced and specialized in hepatopancreatobiliary surgery and liver transplantation. Whether the tumor was in the posterior segments and whether LRPS was feasible for the patient were determined by reviewing radiographic images.
In our center, the treatment modality is discussed among a multidisciplinary team including hepatologists, interventionists, radiologists, and medical oncologists. Whether to perform surgery and the extent of liver resection are also discussed based on the patient’s general condition, liver cirrhosis, and tumor size and location. The final decision whether to perform LRPS or LRHH is made by the operating surgeon.
Statistical Analysis
To minimize the potential of selection bias, we matched patients in the LRPS and the LRHH groups using 1:1 propensity score (PS) matching. The caliper was set at 0.2 and matched without replacement using the nearest neighbor method (13). PS represents the probability of each patient being assigned to LRPS or LRHH based on the covariables (14). PS was calculated using a multivariate logistic regression model including background characteristics of patient demographic conditions and tumor progressiveness. Variables included age, sex, HCC etiology, American Society of Anesthesiologists (ASA) score, disease status, number of tumors, tumor size, liver cirrhosis, and microvascular invasion. Standardized mean differences (d, as an absolute number) were calculated to provide a more reliable estimate of group divergence. Standardized mean differences less than 0.1 were regarded as successful adjustments representing very small differences; values between 0.1 and 0.3 indicated small differences, values between 0.3 and 0.5 indicated moderate differences, and values above 0.5 indicated considerable differences (15).
Primary endpoints were operative result comparison of open conversion rate, operation time, transfusion, margin status, intensive care unit (ICU) admission, days between surgery, and discharge and postoperative complications between the two groups. Patients were discharged when they could eat a normal diet, endured postoperative pain with oral analgesics, and had no postoperative complications. Secondary endpoints were differences in disease-free survival and overall survival between the two groups. Baseline characteristics, preoperative histories, laboratory tests, and pathology data were also compared between the two groups, both before and after PS matching, to ensure matching quality. Numerical variables were compared using Student’s t-test and expressed as means ± standard deviation when they showed normal distribution or compared using Mann–Whitney test and expressed as median (interquartile range) when they did not. Categorical variables were compared using the Chi-square test, Fisher’s exact test, or linear-by-linear association. Kaplan–Meier survival with log-rank test was used to analyze differences in disease-free survival and overall survival between the groups. A two-tailed P-value < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS 20.0 (SPSS Inc., Chicago, IL). This study was approved by the Institutional Review Board of Samsung Medical Center (IRB No. 2017-11-065).
Results
During the study period, 98 patients underwent LLR for HCC located in the posterior segments; 61 received LRPS and 37 LRHH. After PS matching, 30 patients were assigned to each group. Comparisons of baseline characteristics, preoperative histories, laboratory tests, and pathology data between the two groups before and after PS matching are summarized in Table 1. No differences were observed before or after PS matching between the LRPS and LRHH groups in sex, age, body mass index, HCC etiology, ASA classification, history of major operation of the upper abdomen, disease status, all laboratory test results, location and number of tumors, cirrhosis, microvascular invasion, portal invasion, and intrahepatic metastases that indicate satellite nodules. Only tumor size differed significantly between the groups before PS matching (P = 0.035). The LRPS group had a mean tumor size of 3.1 ± 1.3 cm and the LRHH group had a mean tumor size of 4.3 ± 2.7 cm. After PS matching, the LRPS group had a mean tumor size of 3.4 ± 1.2 cm and the LRHH group had a mean tumor size of 3.7 ± 2.1 cm (P = 0.483). The standardized mean difference between the groups for tumor size was 0.233. Most variables showed increased P-values after PS matching and standardized mean differences less than 0.2, except for prothrombin time (international normalized ratio), which had a P-value of 0.148 and a standardized mean difference of 0.411. All patients included after PS matching had Child–Turcotte–Pugh class A disease. The only patient with class B disease was excluded from the matching process.
Comparison of baseline characteristics, preoperative clinical presentation, laboratory blood tests, and pathological characteristics between the laparoscopic right posterior sectionectomy group and the laparoscopic right hemihepatectomy group before and after propensity score matching.
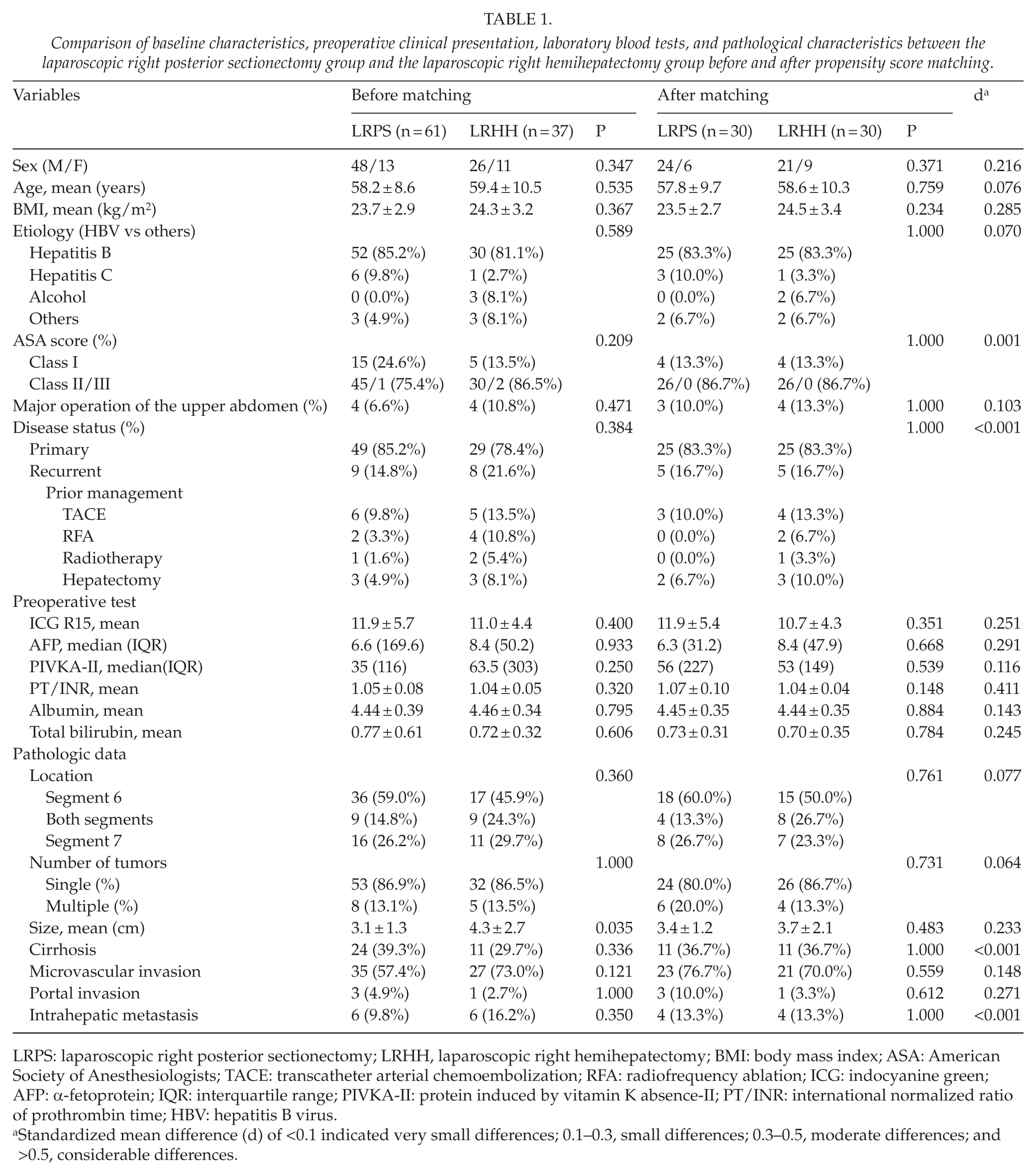
LRPS: laparoscopic right posterior sectionectomy; LRHH, laparoscopic right hemihepatectomy; BMI: body mass index; ASA: American Society of Anesthesiologists; TACE: transcatheter arterial chemoembolization; RFA: radiofrequency ablation; ICG: indocyanine green; AFP: α-fetoprotein; IQR: interquartile range; PIVKA-II: protein induced by vitamin K absence-II; PT/INR: international normalized ratio of prothrombin time; HBV: hepatitis B virus.
Standardized mean difference (d) of <0.1 indicated very small differences; 0.1–0.3, small differences; 0.3–0.5, moderate differences; and >0.5, considerable differences.
Four patients had a history of major surgery of the upper abdomen in each group before matching. In the LRPS group, one patient had a history of exploratory laparotomy due to hemoperitoneum and three patients had a history of liver resection. In the LRHH group, one patient had subtotal gastrectomy for gastric cancer and three patients had a history of liver resection. All patients had severe adhesion during laparoscopic surgery.
The mean follow-up duration was 32.0 ± 18.2 months (range: 2–95 months).
Primary Endpoint: Operative and Postoperative Results
Table 2 summarizes the comparison of operative and postoperative results between the two groups before and after PS matching. No significant difference in open conversion rate was observed between the LRPS and LRHH groups before or after PS matching. In the LRPS group, two patients who underwent open conversion for bleeding from the inferior vena cava and unidentified mass during laparoscopy were included after PS matching. Patients who experienced conversion due to tearing of the mass, a difficult site for resection, or massive venous bleeding were excluded after PS matching. Exclusion was solely determined by the process of PS matching when occurrence of any complication was not included in the matching process. In the LRHH group, one patient underwent open conversion for bleeding from the tumor capsule that was unsafe for electrocauterization during laparoscopy.
Comparison of operative results and postoperative clinical course between laparoscopic and open right posterior sectionectomy groups before and after propensity score matching.
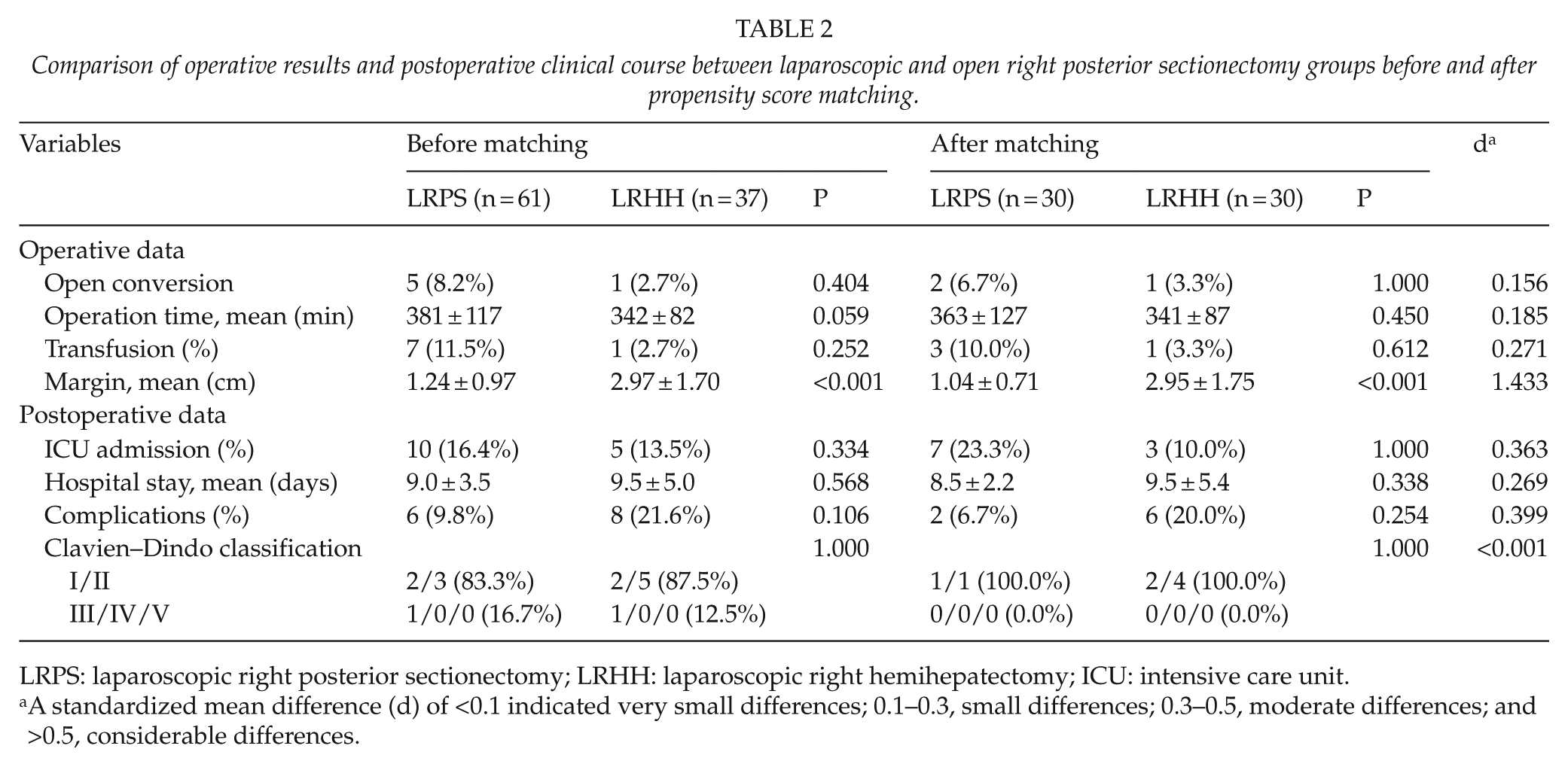
LRPS: laparoscopic right posterior sectionectomy; LRHH: laparoscopic right hemihepatectomy; ICU: intensive care unit.
A standardized mean difference (d) of <0.1 indicated very small differences; 0.1–0.3, small differences; 0.3–0.5, moderate differences; and >0.5, considerable differences.
No significant difference in operation time was observed between the LRPS and LRHH groups before matching (381 ± 117 min in LRPS vs 342 ± 82 min in LRHH, P = 0.059) and after matching (363 ± 127 min in LRPS vs 341 ± 87 min in LRHH, P = 0.450, d = 0.185). No significant difference in transfusion rate was observed (P = 0.252–0.612, d = 0.271) before and after PS matching. Margins were significantly larger in the LRHH group before (1.24 ± 0.97 vs 2.97 ± 1.70 cm, P < 0.001) and after PS matching (1.04 ± 0.71 vs 2.95 ± 1.75 cm, P < 0.001). All patients had a margin status of R0 after resection.
Postoperative data did not significantly change after PS matching. Postoperative ICU admission was 16.4% (n = 10) in the LRPS group and 13.5% (n = 5) in the LRHH group before PS matching (P = 0.334). After matching, ICU admission after operation was 23.3% (n = 7) in the LRPS group and 10.0% (n = 3) in the LRHH group (P = 1.000, d = 0.363). Complication rates were not significantly different in the LRHH group (21.6% before matching and 20.0% after matching) and the LRPS group (9.8% before matching and 6.7% after matching) before or after PS matching (P = 0.106–0.254, d = 0.399). The severity of complications categorized by Clavien–Dindo classification grades I/II and III/IV/V was similar between the groups before and after matching (both, P = 1.000).
In the LRPS group, six patients had postoperative complications and two were included after PS matching. A 59-year-old man diagnosed with stable angina before surgery had chest discomfort after the operation. The patient was evaluated with the assistance of cardiologists and had no abnormal findings on electrocardiography, echocardiography, or cardiac markers; the angina spontaneously subsided. A 54-year-old man was diagnosed with trigeminal neuralgia postoperatively after complaining of facial pain. He was evaluated by a neurologist and discharged with conservative care. Postoperative complications in patients excluded after PS matching included percutaneous drainage due to biloma, a drainage tube for bile leakage, and a diuretic prescription for ascites formation. These patients were excluded solely by the process of PS matching, not by intention.
In the LRHH group after PS matching, the following patients were included: three patients with ascites who were prescribed diuretics, a patient with low hemoglobin who was prescribed ferric acid, a patient who had severe scrotal swelling that was managed conservatively, and a patient with dysuria who was further evaluated by a urologist and managed conservatively. In addition, two patients with ascites and one patient with pleural effusion were excluded after PS matching.
Secondary Endpoint: Disease-Free Survival and Overall Survival
Kaplan–Meier survival analysis was performed to estimate disease-free and overall survival of patients. Disease-free survival was 66.5% at 1 year, 45.8% at 3 years, and 42.3% at 5 years. Overall survival was 94.9% at 1 year, 90.8% at 3 years, and 90.8% at 5 years. Kaplan–Meier survival with log-rank test was used to analyze survival differences between the LRPS and LRHH groups. Fig. 1 shows the disease-free survival and overall survival curves of the LRPS and LRHH groups. Based on log-rank test results, disease-free survival rates in the LRPS group (1 year, 63.2%; 3 years, 38.0%; 5 years, 38.0%) and the LRHH group (1 year, 69.8%; 3 years, 53.7%; 5 years, 47.0%) were not significantly different (P = 0.510). Overall survival in the LRPS group (1 year, 96.6%; 3 years, 92.7%; 5 years, 92.7%) and the LRHH group (1 year, 93.2%; 3 years, 89.6%; 5 years, 89.6%) was also not significantly different (P = 0.593). Intrahepatic recurrence was observed in 86.2% of cases (25 of 29 recurrences) and extrahepatic in 13.8% (4 of 29 recurrences). The ratio of metastatic location was not different between the two groups (P = 1.000). In the LRPS group, 13 of 15 recurrences were intrahepatic and in the LRHH group, 12 of 14 recurrences were intrahepatic.
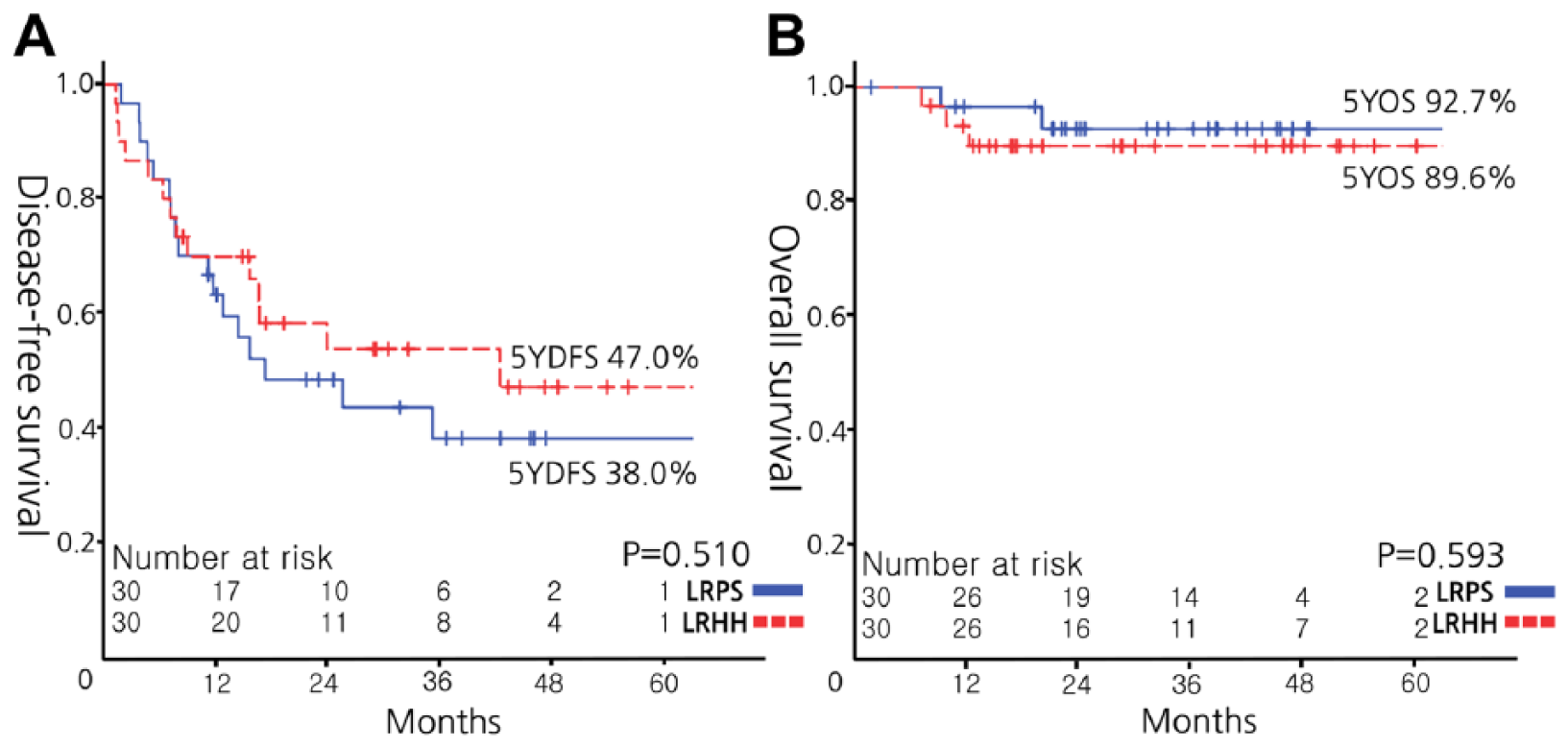
A) Disease-free survival curves and B) Overall survival curves of patients in the laparoscopic right posterior sectionectomy group and the laparoscopic right hemihepatectomy group.
Discussion
Since the introduction of minimally invasive liver surgery, the boundaries of laparoscopic surgery have gradually extended (1, 6, 16–18). Minor resections such as wedge resection or left lateral sectionectomy have been achieved by laparoscopic surgeons (19). Based on the 2008 Louisville Statement and its revision in Morioka, lesions in the posterior segments are considered challenging and should be performed by experienced surgeons (11). Although LRHH can be a significant burden for patients because a large amount of liver parenchyma is removed, LRPS can be problematic for surgeons due to its surgical difficulty (4). For HCCs in the posterior segments, LRHH can be an option when the liver can handle the stress and LRPS does not guarantee sufficient margin clearance. However, HCC patients usually have a fibrotic or cirrhotic liver, necessitating the preservation of as much normal parenchyma without HCC as possible. In these situations, LRPS is more appropriate than LRHH for preserving the liver parenchyma with no HCC. Surgical decisions should be made by surgeons on a case-by-case basis. However, since surgical, clinical, and oncological outcomes of LRPS and LRHH for posterior segment HCCs have not previously been compared, we conducted this study to analyze the differences between LRPS and LRHH for those specific patients.
Our study used PS matching to minimize differences in baseline characteristics between the LRPS and LRHH groups. Tumor size was significantly larger in the LRHH group (P = 0.035; Table 1). This result was not surprising because surgeons may decide to perform right hemihepatectomy for large tumors to acquire a sufficient free margin. Since right posterior section is a rather narrow space, large tumors are likely in close proximity to the right hepatic vein. Large HCCs can also be more progressive than smaller HCCs and consequently could have led to poor prognosis in the LRHH group. Therefore, we considered tumor size the main factor affecting the decision to perform LRPS or LRHH. Our intention in matching patients with variables including tumor size was to eliminate potential biases that could be reflected in concurrent analyses. As a result, tumor size was similar between the LRPS and LRHH groups (3.4 ± 1.2 vs 3.7 ± 2.1 cm, P = 0.483, d = 0.233).
After PS matching, only margin size was persistently larger in the LRHH group (2.95 ± 1.75 cm) than the LRPS group (1.04 ± 0.71 cm, P < 0.001, d = 1.433). Margins were likely to be larger in the LRHH group since patients had HCC in the posterior segments. Nevertheless, every patient underwent R0 resection with no positive margins. Right posterior sectionectomy has smaller margins but preserves parenchyma, while right hemihepatectomy has larger margins but sacrifices parenchyma. Oncological outcomes did not differ between the two procedures.
The postoperative course, which reflects normal recovery from surgery, did not significantly differ between the two groups. Although all patients had grade I or II complications based on Clavien–Dindo classification, most postoperative complications (five of nine before PS matching, three of six after PS matching) were posthepatectomy ascites that necessitated the use of diuretics, reflecting the large amount of liver parenchyma lost. All patients recovered to normal daily activities but were discharged on oral diuretics.
Performing LRPS or LRHH should be decided by surgeons who consider the size and location of tumors combined with the imaginary resection plane and the objective assessment of liver function. When the tumor is located near the right hepatic vein, performing an anatomical LRPS reduces the patient’s chance of clearing the tumor completely from his or her liver. In these situations, surgeons can choose to perform an extended LRPS including the right hepatic vein or an anatomical LRHH. Our data showed that LRPS could be performed safely with similar oncological outcomes to LRHH. Therefore, LRPS should be considered as a first option for tumors in the posterior segments. However, the learning curve for LRPS remains challenging for surgeons.
The limitation of this study is mainly the retrospective design. Although PS was matched in this study, matching the surgeons’ intention equally was difficult. While tumor and liver function were matched between the groups, the distance from the imaginary resection plane may have influenced the surgeon’s decision. However, precisely measuring the distance from the right hepatic vein and objectively adjusting the data to diminish the selection biases made by the surgeon in the past is difficult. Because laparoscopy has only been adopted recently, the mean follow-up period was relatively short. More than half of the patients (n = 35, 58.3%) had a follow-up period of less than 36 months. Long-term follow-up data would be more valuable for identifying the oncological safety of LRPS compared with LRHH. The high overall survival reflects the short follow-up period while also reflecting the improved survival provided by the advancement in treatment modalities. The small number of patients included in the study is also a limitation. The statistical power could have been improved with more patients involved. However, by matching patients and thus reducing possible selection biases, our data are relevant. Most importantly, delicate procedures for obtaining proper surgical margins can be achieved with laparoscopy when right posterior sectionectomy is compared to right hemihepatectomy. Similar oncological outcomes were achieved with open surgery or laparoscopy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was carried out with the support of the “Cooperative Research Program for Agriculture Science & Technology Development (Project No. PJ01100202),” Rural Development Administration, Republic of Korea.