
Abstract
Background and Aims:
Small-bowel obstruction is a frequent cause of hospitalization. The condition is potentially life-threatening, causing many admission days and is a heavy burden socioeconomically. Patients with small-bowel obstruction may develop abdominal free fluid and the quality of this fluid may be predictive of worse outcomes. Our aim was to examine whether the presence of free fluid and its density, measured on computed tomography scans, was associated with severe complications and mortality postoperatively.
Materials and Methods:
Patients admitted to the Department of Surgery, Zealand University Hospital with a diagnosis of small-bowel obstruction between January 2010 and December 2015 were included. Medical records were reviewed and preoperative computed tomography scans were examined. A radiologist blinded to the outcomes reviewed all Hounsfield unit values of the free fluid. The primary outcomes evaluated were odds ratios of the severity of complications and hazard ratios of 30- and 90-day mortality postoperatively.
Results:
A total of 289 patients were included. Analyses revealed an adjusted odds ratio of 1.03 (95%confidence interval = 0.93–1.15) between the presence of free fluid and postoperative complications and an adjusted hazard ratio of 1.28 (95% confidence interval = 0.80–2.05, p = 0.30) of the 30-day mortality in this patient group. Furthermore, the analyses revealed an adjusted odds ratio of 1.22 (95% confidence interval 0.98–1.52) between the density of the free fluid > 20 Hounsfield unit and postoperative complications and an adjusted hazard ratio of 0.85 (95% confidence interval = 0.28–2.63, p = 0.78) of the 30-day mortality.
Conclusion:
No significant correlation was found between the presence of free fluid nor its density in regard to postoperative complications or mortality in patients with small-bowel obstruction.
Keywords
Introduction
Small-bowel obstruction (SBO) is a frequent cause of hospitalization worldwide and 20% of all admissions with acute abdominal pain are due to SBO (1). The condition is potentially life-threatening, causing many admission days and is a heavy burden socioeconomically (2).
Emerging evidence suggests that patients with SBO may develop free fluid in the abdomen. An experimental study showed that the volume of fluid increases the longer the obstruction has persisted, and decreases after surgery (3). Other studies found that free fluid is a significant predictor to identify the SBO patients who may need early surgical intervention, in order to prevent postoperative adverse events (4 –6). Furthermore, studies have shown that the interval from the onset of the symptoms to surgery affects patients’ postoperative recovery, suggesting that late surgical intervention defined as a delay in surgery for more than 24–48 h, induces longer hospitalization (7, 8), higher infection rates postoperatively (9), and higher mortality (8 –10).
Thus, a delay in surgery is proven to increase the volume of the free fluid, and complication and mortality rate postoperatively.
Hounsfield unit (HU) is a measure of the density of various tissues in the body and is assessed on computed tomography (CT) scans. Even small density changes can be detected with the HU, and the method is a reliable tool to differentiate between liquids, even if the protein concentration has changed slightly.
Some studies have shown a correlation between free fluid density over 20 HU and infection of the fluid (11, 12). If the free fluid is infected, it is believed to exacerbate the prognosis of the patients and the complication and mortality rates are likely to rise (13). The hypothesis is that the presence of free fluid in the abdomen and density over 20 HU in patients with SBO increases the risk of developing postoperative complications, which may increase the mortality rate.
To our knowledge, no published studies have examined the correlation between the presence of free fluid and postoperative complications in the SBO population. This relationship may be important to investigate in order to develop therapeutic strategies to prevent complications in the future.
The aim of this study was to examine whether the presence and the density of free fluid was associated with severe complications and mortality postoperatively.
Materials and Methods
All patients admitted to the Department of Surgery, Zealand University Hospital between 1 January 2010 and 31 December 2015, with a diagnosis of SBO, were included in the study. Medical records were reviewed and only patients above 18 years of age, who underwent surgical intervention and with preoperative CT scan, were included in the study. From the medical records, information regarding age at admission, gender, body mass index (BMI), tobacco use (smoking pack years), alcohol consumption (average drinks of alcohol per week), American Society of Anesthesiologists Score (ASA score), date of surgery and operative findings were obtained. Furthermore, information about the postoperative period, complications, and mortality were obtained.
The postoperative complications were assessed by the Clavien–Dindo classification, and the complications were graded in eight groups based on the severity: 0—no complications; 1—any deviation from the normal postoperative course without the need for pharmacological treatment or surgical, endoscopic, and radiological interventions; 2—requiring pharmacological treatment, including blood transfusions; 3a—requiring surgical, endoscopic, or radiological intervention, but not under general anesthesia; 3b—same as 3a, but with intervention under general anesthesia; 4a—single organ dysfunction requiring intensive care management; 4b—same as 4a, but multiorgan dysfunction; and 5—death of the patient (14).
Patients were classified into two groups depending on the severity of the postoperative complication, based on the Clavien–Dindo score. None or minor complications were defined as Clavien–Dindo score of 3a or less, while major complications were defined as a score of 3b or above.
A radiologist blinded to the outcomes examined all CT scans. The HU values of the free fluid were measured by studying the axial, coronal, and sagittal planes. Free fluid was defined as an abnormal accumulation of fluid in the abdominal cavity. No volume limitation was set. The measurements were taken in three different areas within the fluid. In cases with sparse volume of the abdominal fluid, three readings were taken from the same area. The highest value was used in the statistical analyses.
The study cohort was divided into two groups according to whether or not the patients had free fluid inside the abdomen at the time of diagnosis. Furthermore, the group with abdominal free fluid was subdivided based on whether or not the highest value of the measured HU was under or above 20 HU (11, 12).
The primary outcomes were the severity of postoperative complications, none or minor versus major complications, assessed by logistic regression, and the 30- and 90-day mortality were estimated using the Kaplan–Meier estimator with a log-rank test as well as a Cox regression model. The analyses were adjusted for age at diagnosis, gender, use of tobacco, alcohol consumption, and ASA score. The results were presented with a hazard ratio (HR). A p value ≤ 0.05 was considered as statistically significant.
The study was approved by The Danish Patient Safety Authority (journal-no 3-3013-1508/1/) and the Danish Data Protection Agency (journal-no 2008-58-0020). All statistical analyses were performed using the SAS® Proprietary Software 9.4, SAS Institute Inc., Cary, NC USA.
Results
A total of 479 patients underwent surgery due to SBO between January 2010 and December 2015. Of these patients, 190 were excluded based on missing preoperative CT scans (165 patients with preoperative abdominal X-ray, while the remaining 25 patients had no preoperative radiological examinations made). The remaining 289 patients were included in the study cohort.
Review of the CT scans revealed 136 patients with abdominal free fluid and 153 without free fluid. See Fig. 1. The baseline characteristics of the two groups were not significantly different. Data are presented in Table 1. The median age in the group with abdominal free fluid was 68 years (range 18–92) and in the group without free fluid, it was 71 years (range 18–94). The distribution of the patient characteristics regarding gender, BMI, smoking pack years, weekly consumption of alcohol, and ASA score are presented in Table 1.
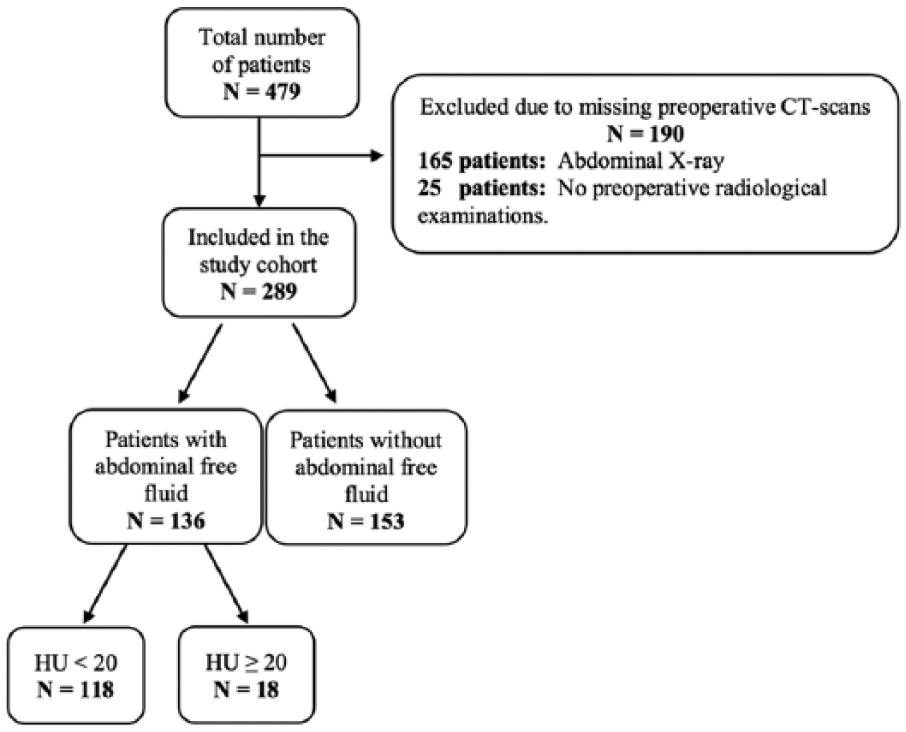
Overview of the study population.
Patient characteristics of the study population, N = 289.
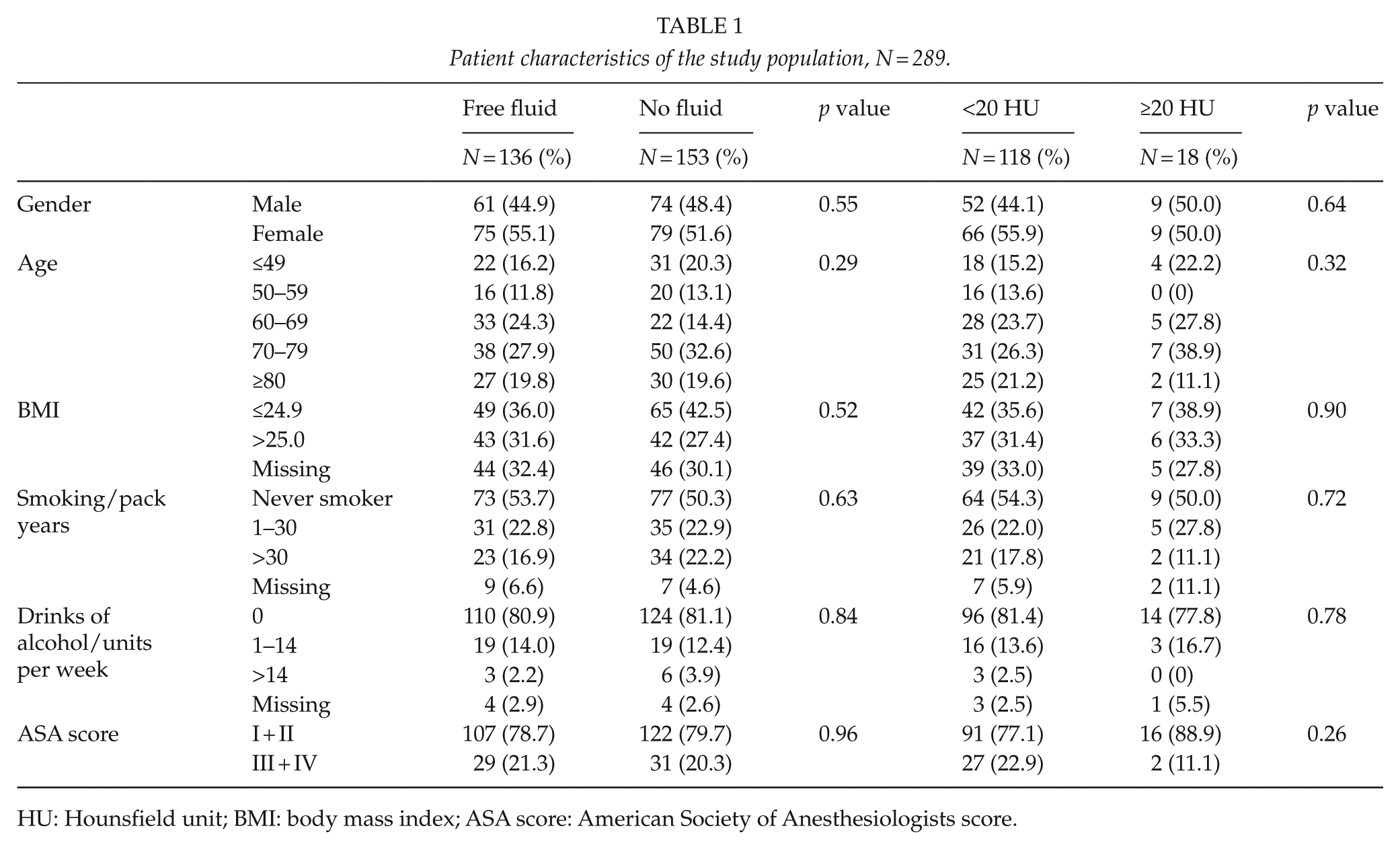
HU: Hounsfield unit; BMI: body mass index; ASA score: American Society of Anesthesiologists score.
Overall, 48% of all surgeries performed in the study population were caused by postoperative adhesions, 15% by tumors, 14% by hernias, 11% by volvulus, 10% by intestinal obstructions (i.e. gallstones and stenosis) and 1% by other causes. The operative findings revealed 30 patients with bowel ischemia and in total 91 bowel resections were performed.
Furthermore, the patients with abdominal free fluid were stratified into two subgroups according to whether or not the HU value measured on the CT scan was below or above 20 HU. The analysis revealed 118 patients with an HU value under 20 HU and 18 patients above 20 HU (see Fig. 1). The median age of the group with an HU value above 20 was 65 years (range 20–96) and 68 years (range 18–92) in the group with an HU value under 20. With respect to the demographics, the statistical analysis showed no significant difference between the groups (see Table 1).
The postoperative complications of the study population are visualized in Table 2. The complications were categorized by the Clavien–Dindo classification for each of the four subgroups of this study. The severity of the postoperative complications appeared not to be correlated to the presence of free fluid inside the abdomen nor the density of the fluid above 20 HU. The logistic regression showed an adjusted odds ratio (OR) of 1.03 (95% confidence interval (CI) 0.93–1.15) in the group with abdominal free fluid and 1.22 (95% CI 0.98–1.52) in the group with HU value above 20. In addition, the univariate and multivariate analyses implied no significant correlation between the presence of abdominal free fluid and the 30- or 90-day mortality. The multivariate analysis showed a 30-day mortality HR of 1.28 (95% CI 0.80–2.05, p = 0.30) in the group with abdominal free fluid. Furthermore, the multivariate analysis revealed a 30-day mortality HR of 0.85 (95% CI 0.28–2.63, p = 0.78) in the group with the density of the free fluid above 20 HU (see Table 3). The 30- and 90-day mortality in the two studies were visualized with a Kaplan–Meier estimator in Figs 2 and 3.
Postoperative complications and mortality of the study population, categorized by the Clavien–Dindo classification, N = 289.
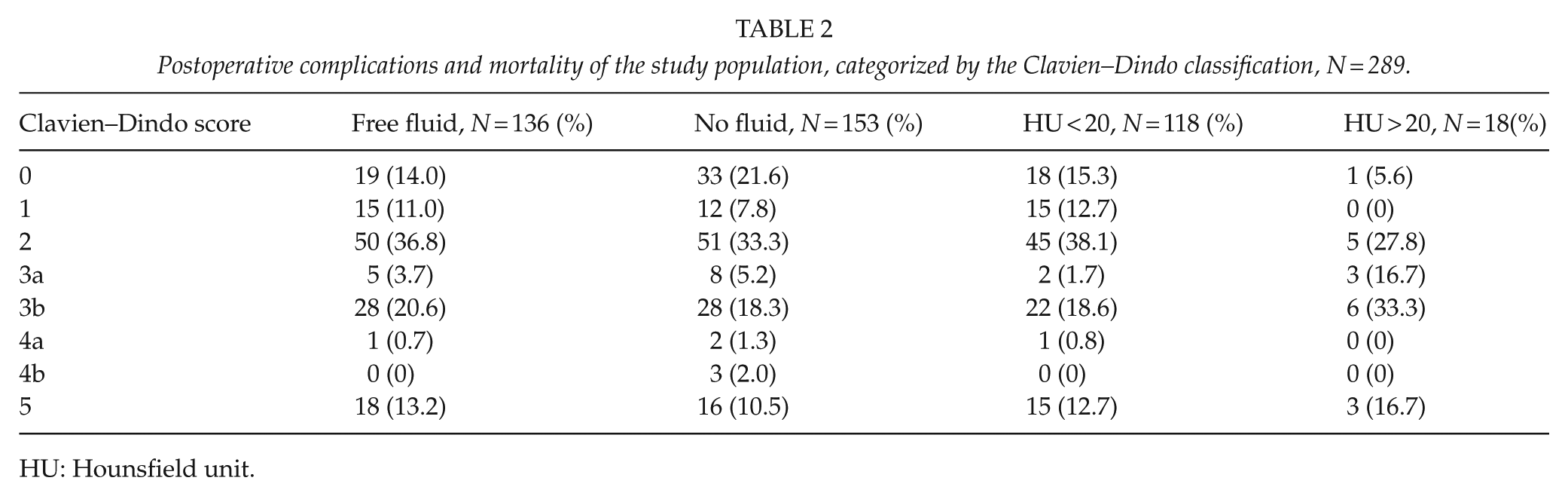
HU: Hounsfield unit.
30- and 90-day survival hazard ratios and complication rates presented with odds ratios.
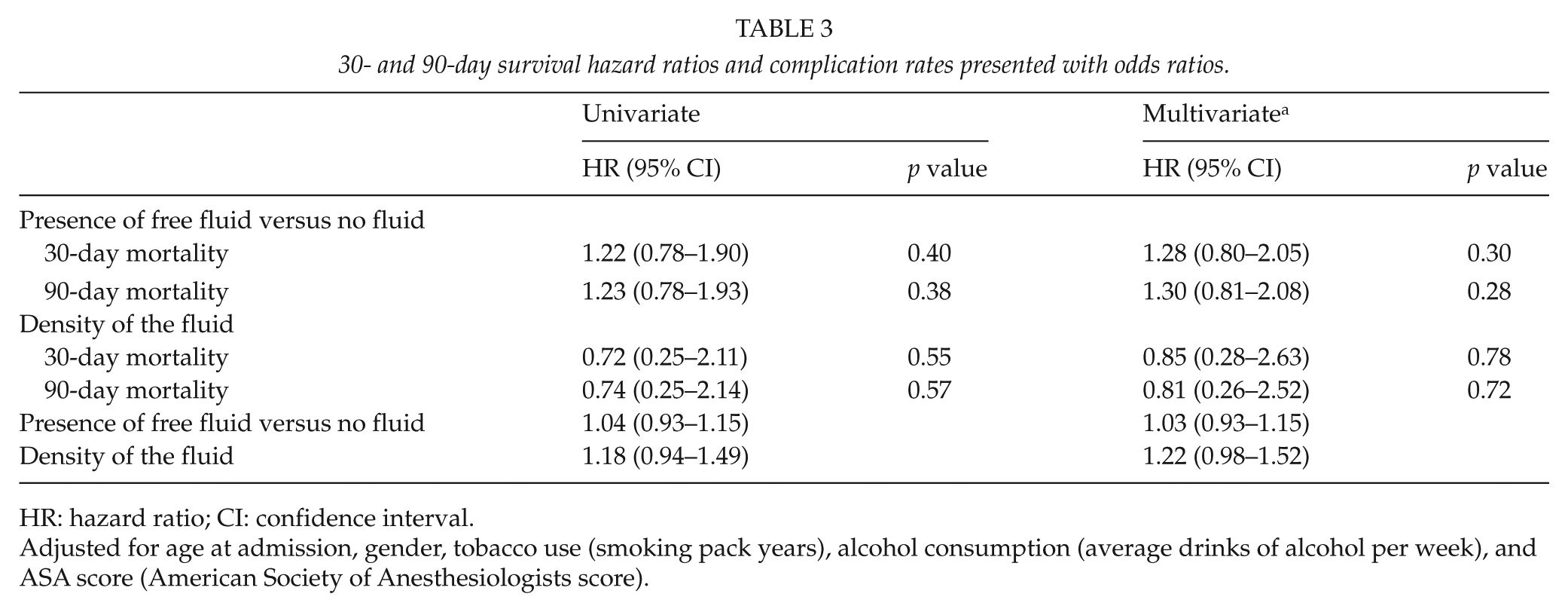
HR: hazard ratio; CI: confidence interval.
Adjusted for age at admission, gender, tobacco use (smoking pack years), alcohol consumption (average drinks of alcohol per week), and ASA score (American Society of Anesthesiologists score).
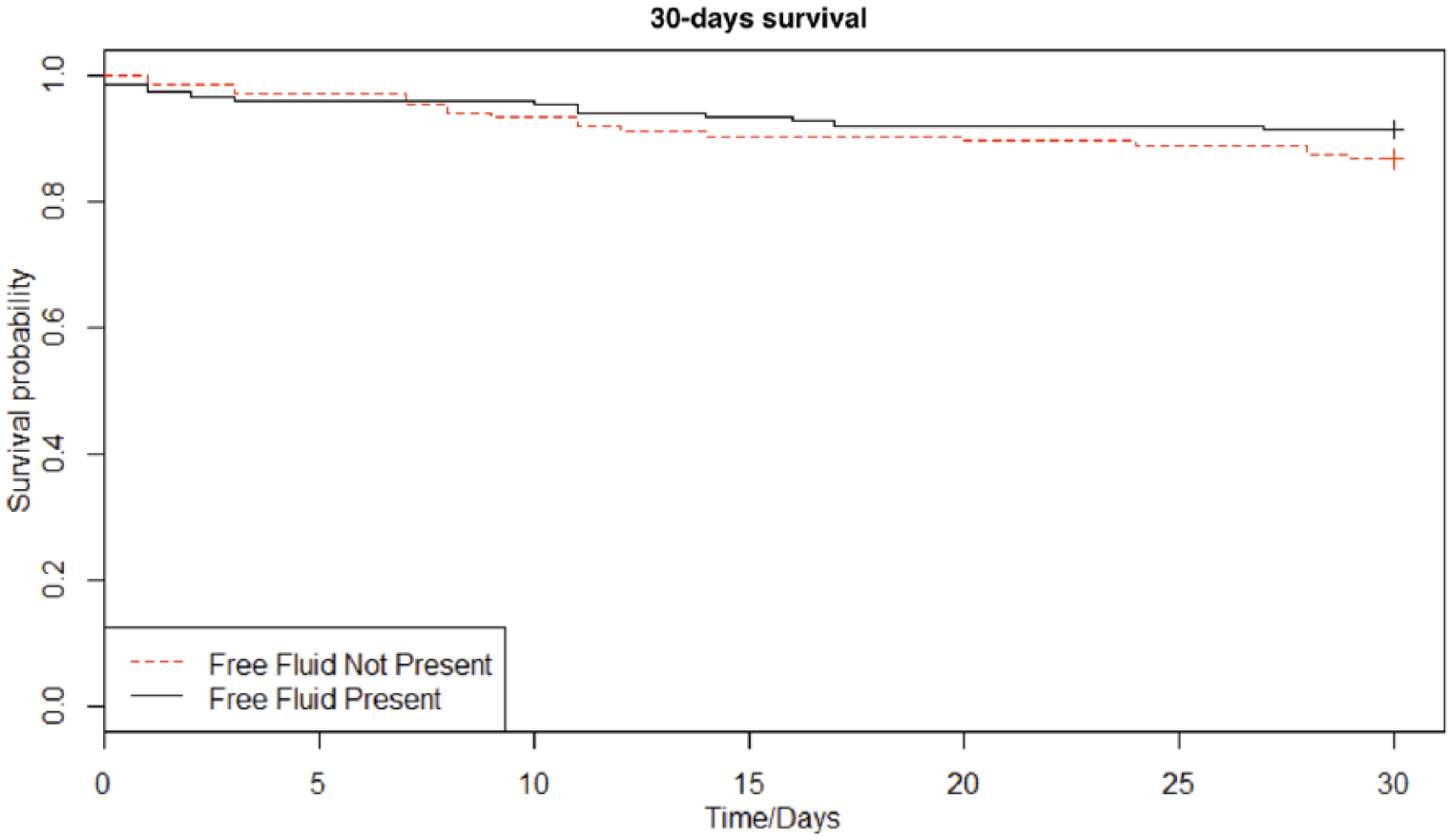
Kaplan–Meier curve on 30-day survival.
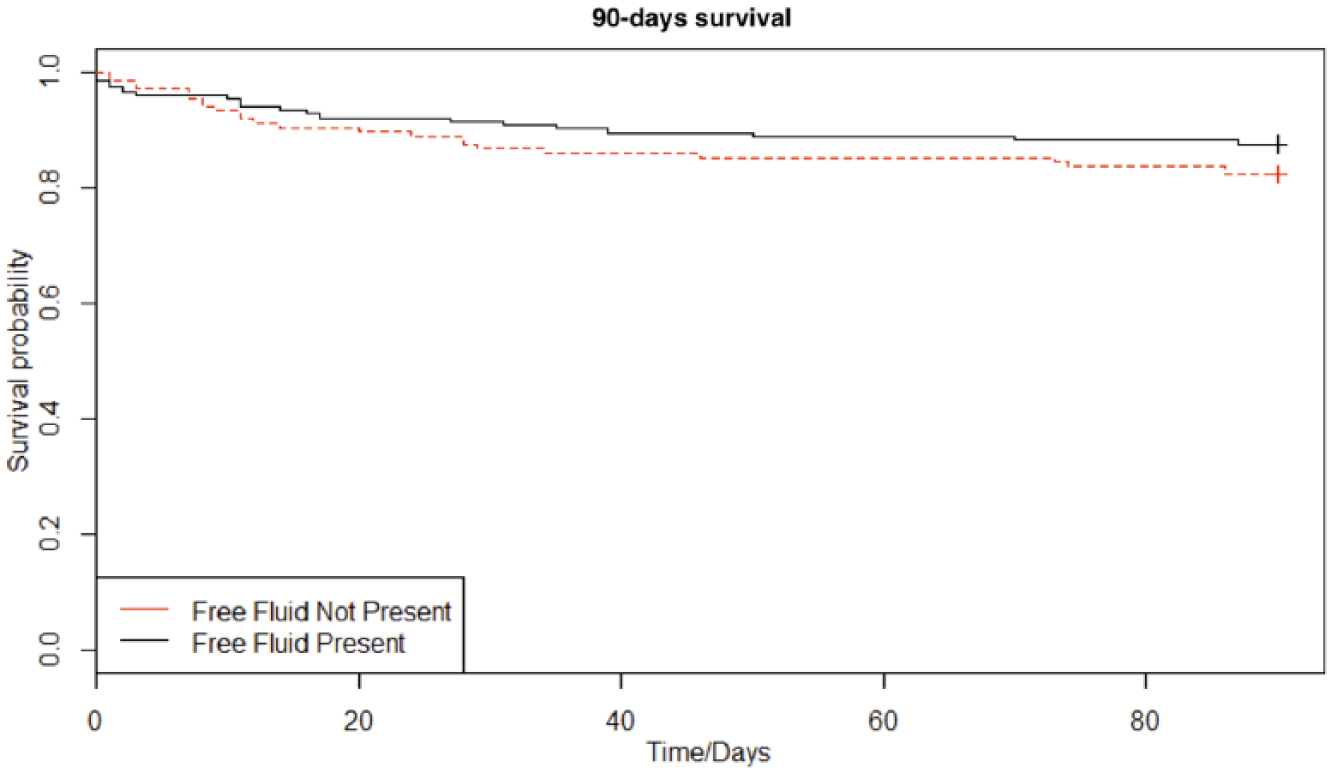
Kaplan–Meier curve on 90-day survival.
Discussion
This study revealed no significant correlation between the presence of abdominal free fluid, nor the density and postoperative complications, and 30- and 90-day mortality in patients with SBO.
Free fluid in the abdomen may develop during SBO. Some studies have examined the importance of the fluid (3 –6, 15) and a study in a rat model (3) has shown that the liquid volume increases with prolonged duration of the obstruction. An increase in intraluminal tension compromises the bowel microcirculation, which causes edema in the bowel wall. This impairs the bowel’s capability to reabsorb fluids from the extra luminal space, which explains why the liquid volume increases by time. Other studies have examined the importance of time from onset of the symptoms to surgical intervention, in relation to the postoperative recovery. It is believed that a delay in surgery over 24–48 h increases the complication and mortality rates (7 –10), but no prior studies have examined the physiological changes that cause these adverse events. This field may be important to investigate in order to develop therapeutic strategies to prevent complications in the future.
It is a well-known theory that intestinal obstruction causes translocation of bacteria from the intestinal lumen to the mesenteric lymph nodes (16) and other organs (17). Bacterial translocation is associated with an increase in the risk of complications, especially infections (18). Other studies (11, 12) have shown that the density of the free fluid, measured with an HU value on CT scans, is correlated to infected fluid. These studies suggest that an HU above 20 is associated with a high risk of infection in the fluid.
Therefore, if bacterial translocation results in migration of bacteria from the intestinal lumen, the bacteria could potentially spread to the free liquid as seen in SBO patients. This would lead to a higher density of the abdominal free fluid, which potentially could increase the complication rate.
However, this study showed no detectable significant correlations between the density of the fluid and complications. Furthermore, the study detected no significant associations between the density and the short-term survival.
There were some limitations to this explorative study. This study is limited by its retrospective design, resulting in a restriction on the data obtained. Minor complications may have been under- or misreported in the medical records. The interval from the onset of SBO symptoms to surgery is an important predictor of the postoperative outcomes. Due to lack of registration in the medical records, the duration of the symptoms was not assessable, and the factor was excluded from the analysis. There is a potential selection bias in the study population. Some patients may have had peritoneal reaction clinically, or may have been hemodynamic unstable and thus operated before a CT scan was made. These patients might have had a larger volume of free fluid and a worse postoperative outcome, but were excluded from the study due to missing preoperative CT scans. The results may propose an increase in the mortality rate in patients with free fluid density above 20 HU. Table 2 shows that patients with HU above 20 had a mortality rate of 16.7% versus 12.7% in the group with HU under 20. The results may indicate an increase in mortality rate with increasing density of the fluid. However, the sample size is relatively small with only 18 patients in the study having HU above 20. Another important limitation is that we have not validated that an increased density represented by HU > 20 actually represents higher density confirmed by biochemical analysis.
In conclusion, this study did not demonstrate any association between the presence of free fluid nor its density and postoperative complications and mortality in patients with SBO. If the correlation between the free fluid and postoperative outcomes should be explored further, it might be interesting to examine a much larger group of the population with prospective biochemical and microbiological analysis of the peritoneal fluid.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This article does not contain any studies with human participants performed by any of the authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.