
Abstract
Background and Aims:
Even though hydrodilatation has been used for 50 years, the evidence on its effectiveness is not clear. Only one earlier review has strictly focused on this treatment method. The aims of this study are to evaluate the evidence on the effectiveness of hydrodilatation in treatment of adhesive capsulitis and, if appropriate, to assess the correlation between the effects of this procedure and the amount of fluid injected.
Materials and Methods:
A literature search on MEDLINE, Embase, Scopus, Cochrane Central, Web of Science, and CINAHL databases was done; random-effects meta-analysis and meta-regression were employed; and cost-effectiveness and safeness analyses were left outside the scope of the review.
Results:
Of the 270 records identified through search, 12 studies were included in qualitative and quantitative analysis and seven were included in a meta-analysis. The lower 95% confidence interval for the effect of hydrodilatation on pain severity was 0.12 indicating small effect size and mean number needed to treat 12. The pooled effect of hydrodilatation on disability level was insignificant 0.2 (95% confidence interval: −0.04 to 0.44). The lower 95% confidence interval for the effect of hydrodilatation on the range of shoulder motion was close to zero (0.07) indicating small effect size with mean number needed to treat 12. The amount of injected solution did not have a substantial effect on pain severity or range of shoulder motion. The heterogeneity level I2 was acceptable from 0% to 60%.
Conclusion:
According to current evidence, hydrodilatation has only a small, clinically insignificant effect when treating adhesive capsulitis.
Keywords
Introduction
While the arsenal of treatment methods for adhesive capsulitis is broad, there is a well-known lack of evidence on their effectiveness or the superiority of one approach over another. Due to the high probability of spontaneous recovery of adhesive capsulitis, conservative treatment should usually be advised (1). The conservative treatment of adhesive capsulitis may include oral analgesics, oral or intra-articular corticosteroids, physiotherapy, acupuncture, manipulation, and hydrodilatation (distension) (2). Hydrodilatation (distension, hydrodistension) aims at physical distension of the shoulder joint capsule by injecting a substantial amount of fluid into the joint. This quick procedure is technically easy to perform and it is less invasive than actual surgery. While adhesive capsulitis resolves usually spontaneously, the symptoms may persist for many months inflicting significant disability (3). This fact may often force a patient to seek for an invasive procedure rather than for a slower conservative treatment. Even though hydrodilatation has been used for 50 years, the evidence on its effectiveness is not clear (4, 5). Only one review has strictly focused on this treatment method (5). Other reviews on the treatment of adhesive capsulitis have evaluated hydrodilatation among other treatment options (6–9) or left this method outside the scope of study (10, 11).
A previous review dedicated to this topic has suggested the effectiveness of hydrodilatation as short-term benefits in pain reduction, improvement in range of motion (ROM), and function (5). However, this conclusion was uncertain as it was based on the results of two small-sample studies. Of those two studies, a trial by Corbeil et al. (12) found no difference between corticosteroid injections with and without distension component. Another trial by Buchbinder et al. (13) compared hydrodilatation combined with corticosteroid versus placebo and, therefore, the essential effect of hydrodilatation itself was inaccessible. Also, another Cochrane review presented hydrodilatation as an evidence-based method even if no additional support for the recommendation was provided (7). Guyver et al. (9) suggested that even though the evidence on hydrodistension is insufficient, this procedure could be considered an alternative to more interventional procedures such as manipulation under general anesthesia or capsular release. Recent review by Lewis (6) proposed considerably more research on the topic.
Hydrodilatation is an invasive and relatively expensive procedure that may cause pain and joint capsule rupture. The evidence on its effectiveness should be obtained before allocating health care’s and patients’ own resources on this treatment. The objective of this review was to evaluate the evidence on the effectiveness of hydrodilatation in the treatment of adhesive capsulitis and, if appropriate, to assess the correlation between the effects of this procedure and the amount of fluid injected.
Methods
PICO
The criteria for considering studies for this review were based on the PICO (Population, Intervention, Comparison, and Outcome) framework as follows:
Types of studies: Randomized controlled trials (RCTs).
Participants: Adults with adhesive capsulitis, frozen shoulder, painful stiff shoulder, or osteoarthritis, generally defined as the presence of pain with restriction of active and passive glenohumeral joint movements.
Intervention: Hydrodilatation (distension, hydrodistension) of the glenohumeral joint.
Comparison: Placebo, sham, other interventions, or no treatment.
Outcome: All clinically relevant outcome.
○ Primary: Pain and function or disability assessment. ○ Secondary: ROM, severity of the disorder, analgesic use, adverse events, time to recovery or recurrence, and any others.
Data Sources and Searches
The MEDLINE, Embase, Scopus, Cochrane Central, Web of Science, and CINAHL databases were searched in September 2017. The search clause for the Medline search was “(shoulder OR rotator)[TI] AND (hydrodilatat*[TI] OR distension[TI]) AND (Randomized Controlled Trial[ptyp] OR Controlled Clinical Trial[ptyp]).” In order to avoid missing potentially relevant studies, the use of other limiters and filters was restricted relying rather on manual selection. The similar clauses were used when searching on the other databases. The references of identified articles and reviews were also checked for relevancy.
Study Selection
Due to a small amount of records identified as potentially relevant, full texts of records without a preliminary screening based on titles and abstracts are assessed (Fig. 1). Disagreements between reviewers were resolved by consensus or by a third reviewer. The methodological quality of the included trials was not rated.
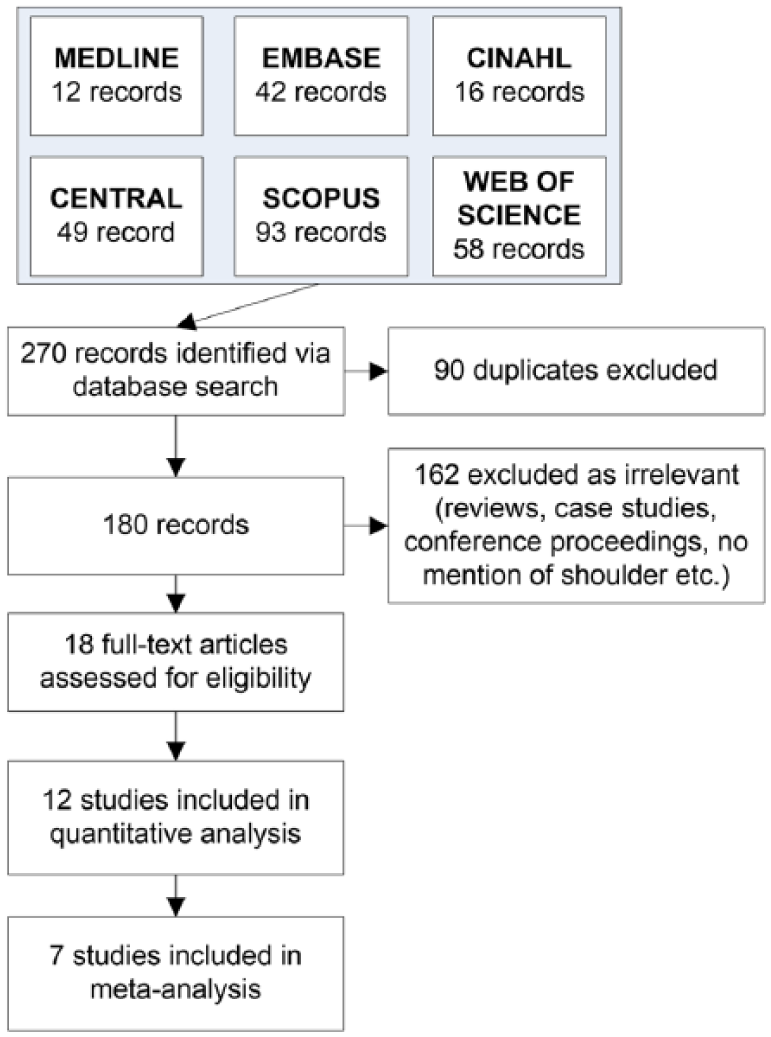
Search flow.
Data Extraction and Quality Assessment
Data needed for meta-analysis were extracted from the included trials using a standardized form based on recommendations by the Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0, part 7.6 (14).
The methodological quality was assessed according to the Cochrane Collaboration’s domain-based evaluation framework. Main domains were assessed in the following sequence: (a) selection bias (randomized sequence generation and allocation concealment); (b) performance bias (blinding of participants and personnel); (c) detection bias (blinding of outcome assessment); (d) attrition bias (incomplete outcome data, for example, due to dropouts); (e) reporting bias (selective reporting); and (f) other sources of bias. The scores for each bias domain and the final score of risk of systematic bias were graded as low, high, or unclear risk.
The protocol of review was registered on Prospero database: CRD42017075985.
Statistical Analysis
When only interquartile range (IQR) was reported, the standard deviation (SD) was calculated as IQR/1.35. When only median was reported, mean was assumed the same as median as suggested by the Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0, Chapter 7.7.3.5 (14). When only range was reported, SD was calculated as (max − min)/4. The effect sizes of the included trials were calculated as Cohen’s d—a standardized mean difference in variable change between groups. As the SD of difference in means was reported by only a few studies, when pooling, the pre–post correlation coefficient was set at 0.6 and the sensitivity test was ran with the coefficient set at 0.8. The effect sizes were accompanied by their 95% confidence intervals (95% CI). For each included paper, the synthesis was started from pooling together all the reported outcomes (grouping them as pain, disability, and motion related) gathered at all the reported time points. Subgroup and sensitivity analyses included syntheses excluding one study at the time and excluding studies with high risk of systematic bias.
The test for heterogeneity was conducted using the I2 statistic describing the percentage of variation across studies originating more from heterogeneity than from chance. The potential publication bias was evaluated by Egger’s test for asymmetry of the funnel plot (test for the Y intercept = 0 from the linear regression of normalized effect estimate against precision), where the trim-and-fill method was used to impute studies into funnel plot to correct asymmetry. Expecting wide-range variability in studies’ settings, a random-effects meta-synthesis was employed despite particular percentages of heterogeneity.
To explain the obtained Cohen’s d figures in a common language, four additional statistics were estimated for statistically significant effects:
Cohen’s U3. The percentage of a treatment group that is above the mean of a control group. U3 = Φ (Cohen’s d), where Φ is cumulative distribution function of the standard normal distribution.
Percent of overlap (OVL). The OVL of results observed in treatment and control groups (percent)
Probability of superiority (CL). The chance that a person picked at random from the treatment group will have a higher score than a person picked at random from the control group (percent)
Number needed to treat (NNT). The number of people needed to treat to obtain one more favorable outcome in the treatment group compared to the control group. NNT = 1/(Φ (Cohen’s d + Ψ (CER)) − CER), where Ψ is inverse of Φ and CER is control group’s event rate.
Due to missing data, the control group’s event rate was set at the level 0.1%–10% of controls having “favorable outcomes.” That way, we ensured that the reported NNT would be at its smallest possible level.
Cohen’s d of 0.2 was considered a “small” effect size, 0.5 a “medium” effect size, and 0.8 a “large” effect size. The cut-off for acceptable NNT was set at 4 (15)—meaning that four patients have to be treated in order to observe one positive response.
Random-effects meta-regression was conducted on Cohen’s d on injected volume. The regression coefficient was reported along with 95% CIs and two-sided p values.
The analysis was made using Comprehensive Meta Analysis CMA, Version 3.3, available from www.meta-analysis.com and Microsoft Excel 2013.
Results
Of the 270 records identified through search, 152 duplicates and irrelevant (reviews, case studies, proceedings, theses, etc.) records were excluded resulting in 18 records for a full-text assessment. At the first round of selection, the percentage of agreement between raters was 65%. Of them, 12 studies were included in qualitative and quantitative analyses (13, 16–26). Of the assessed studies, eight were considered to have low risk and four were considered to have high risk of systematic bias (Table 1). The sizes of intervention groups varied from 8 to 60 patients with predominance of people of middle age (mostly women). In four studies, the procedure was performed with the assistance of sonography and one study used only visual guidance. Otherwise, X-ray guidance was used. The inclusion and exclusion criteria varied mildly being quite similar in the majority of the studies. During the distension procedure, the volume of injected mixture varied widely from 20 up to 90 mL. The mixture usually contained triamcinolone or methylprednisolone, contrast, local anesthetic, and normal saline solution. Park et al. (21) used hyaluronate instead of corticosteroid. The included studies reported some side effects such as flushing or disturbances in heat regulation, loss of sensation and motor control in the affected arm, loss of sleep, nausea, dizziness (20, 25, 26), after-pain (25), hypotensive syncope (26). In one case, a patient developed a glenohumeral joint infection (20) (Table 2).
Risk of systematic bias of the included studies.
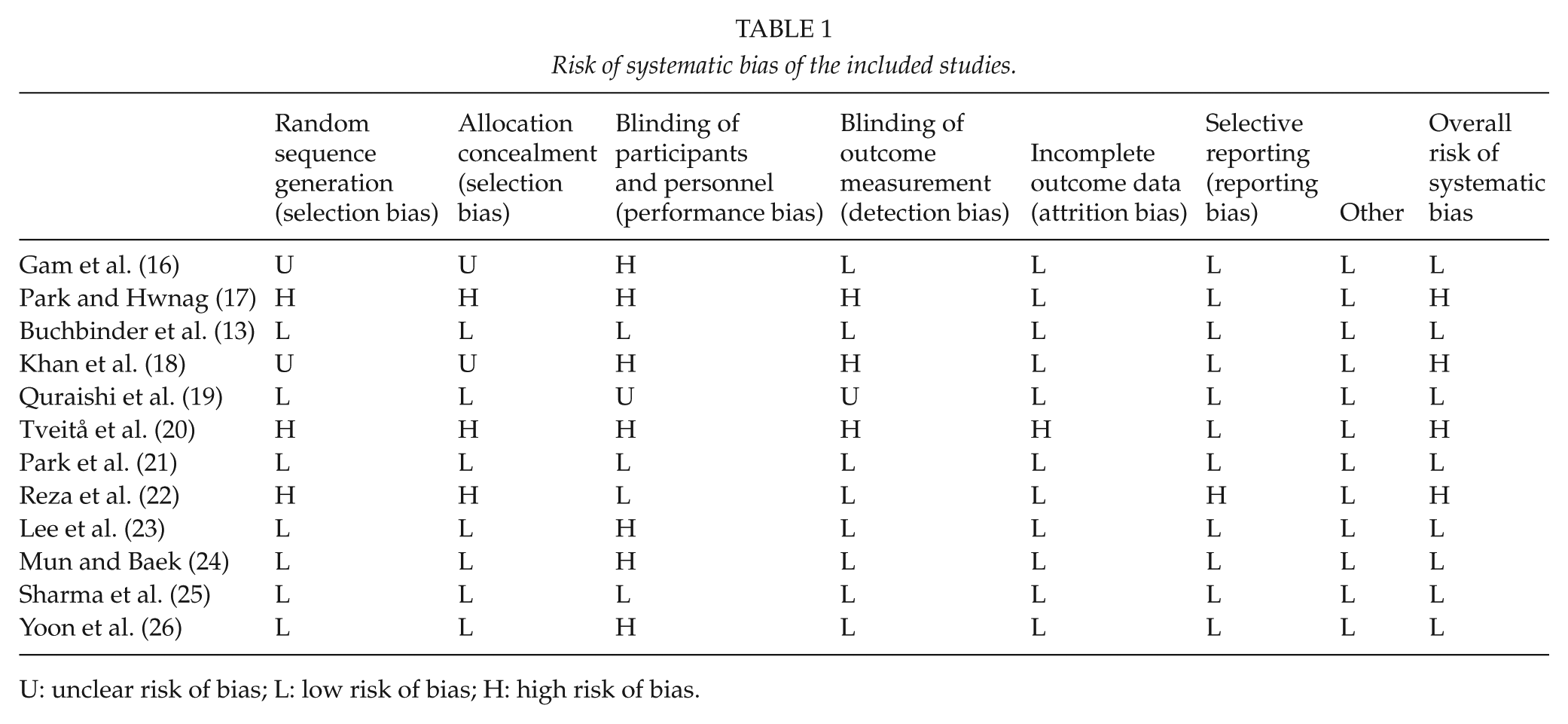
U: unclear risk of bias; L: low risk of bias; H: high risk of bias.
Basic characteristics of the included studies.
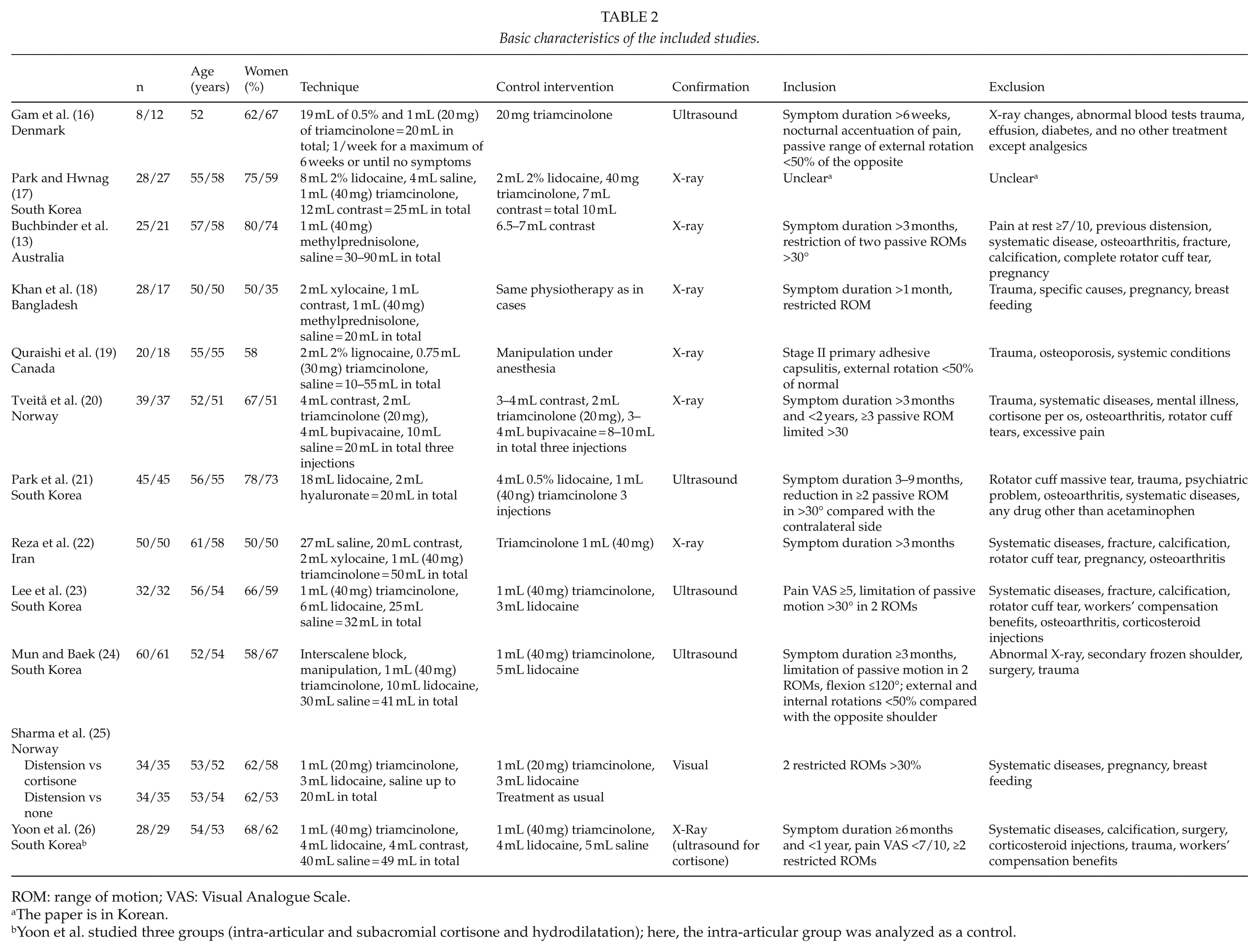
ROM: range of motion; VAS: Visual Analogue Scale.
The paper is in Korean.
Yoon et al. studied three groups (intra-articular and subacromial cortisone and hydrodilatation); here, the intra-articular group was analyzed as a control.
Of the 12 RCTs, only 7 assessed the essential effect of hydrodilatation by comparing hydrodilatation combined with corticosteroid versus corticosteroid alone (16, 17, 20, 22, 23, 25, 26). Those seven studies were included in a meta-analysis. Two other studies compared hydrodilatation combined with corticosteroid versus treatment as usual or contrast alone (13, 18); Quraishi et al. (19) compared hydrodilatation combined with corticosteroid versus manipulation; Park et al. (21) studied the effect of hydrodilatation combined with hyaluronate versus corticosteroid; and Mun and Baek (24) investigated the effect of hydrodilatation combined with interscalene block, manipulation with corticosteroid versus corticosteroid alone. Separating the effect of hydrodilatation itself was impossible in these five studies and they were excluded from a meta-analysis.
Quantitative Analysis of the Five Studies not Included in Meta-Analysis
The effect sizes for each outcome combining repeated measures at all time points are shown in Fig. 2A. When combining all the reported outcomes at all time points, the effect sizes of three studies were either very small (considering their lower 95% CIs) or insignificant (13, 19, 21) (Fig. 2B). Two studies showed large effects when evaluating (a) combination of interscalene block, manipulation, and hydrodilatation versus corticosteroid alone (study with a high risk of systematic bias) and (b) hydrodilatation and corticosteroid versus treatment as usual (small study with 18 participants in the intervention group) (18, 24).
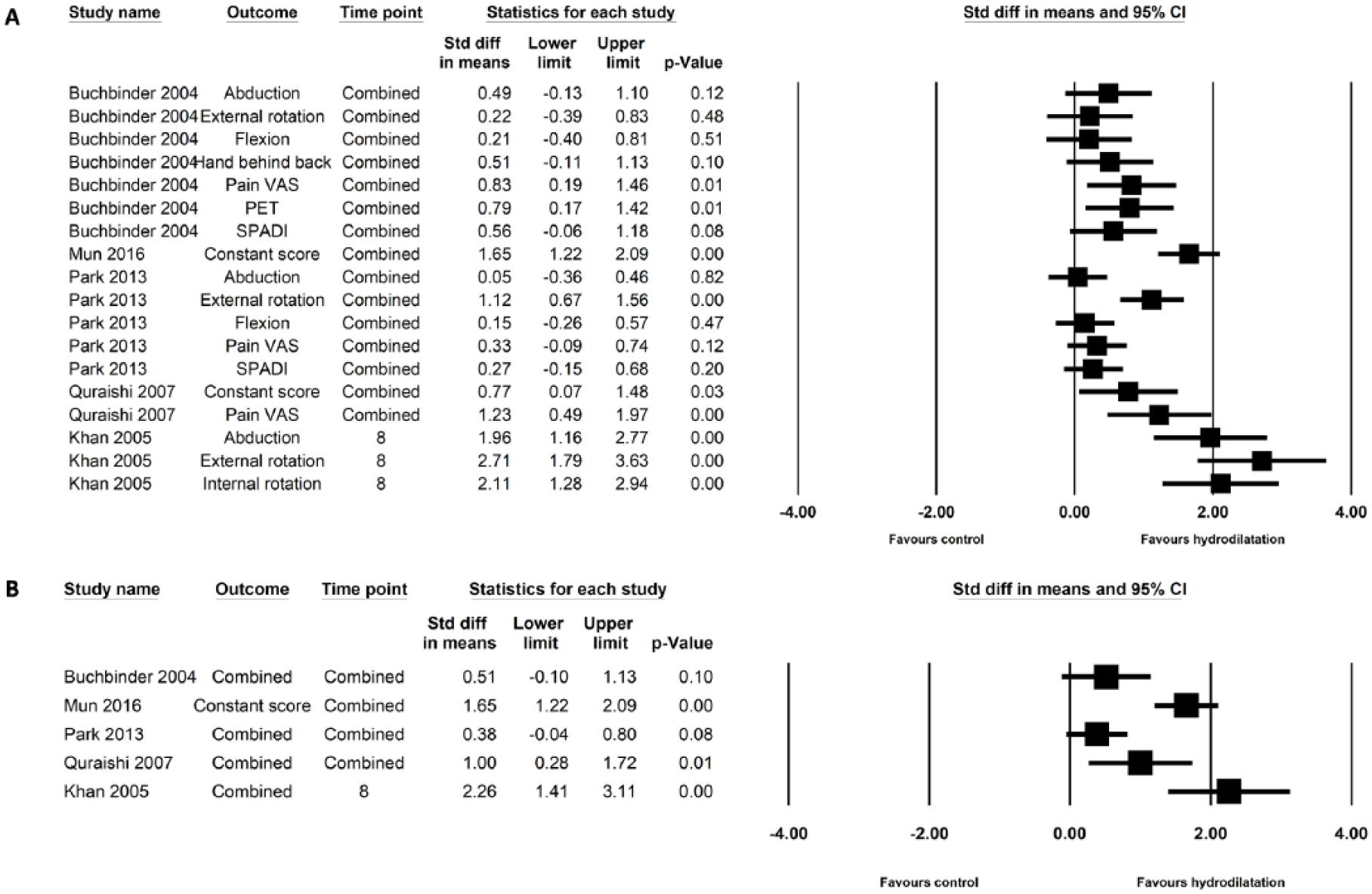
Effect sizes of the studies not included into meta-synthesis. (A) Effect sizes for each outcome combining repeated measures at all time points. (B) Effect sizes for each study combining both outcomes and time points.
Meta-Analysis of Seven Studies Evaluating the Effect of Hydrodilatation Combined with Corticosteroid Versus Corticosteroid Alone
Following outcome variables had to be left out of final meta-analysis because of insufficient data in the original studies: shoulder ROM, use of analgesics, and symptom severity in study by Gam et al.; use of analgesics in report by Buchbinder et al.; ROM change in study by Quraishi et al.; and pain severity in studies by Reza et al., Mun et al., and Khan et al.
During the synthesis, repeated measures at all available time points were combined (Fig. 3). The lower 95% CI for the effect of hydrodilatation on pain severity was 0.12 indicating small effect size with Cohen’s U3 64% (95% CI: 55%–73%), overlapping coefficient 85% (95% CI: 76%–95%), probability of superiority 60% (95% CI: 53%–67%), and mean NNT 12. The pooled effect of hydrodilatation on disability level was insignificant 0.2 (95% CI: −0.04 to 0.44). The lower 95% CI for the effect of hydrodilatation on the range of shoulder motion was close to zero (0.07) indicating very small effect size with Cohen’s U3 65% (95% CI: 54%–75%), overlapping coefficient 85% (95% CI: 73%–97%), probability of superiority 61% (95% CI: 52%–69%), and mean NNT 12.
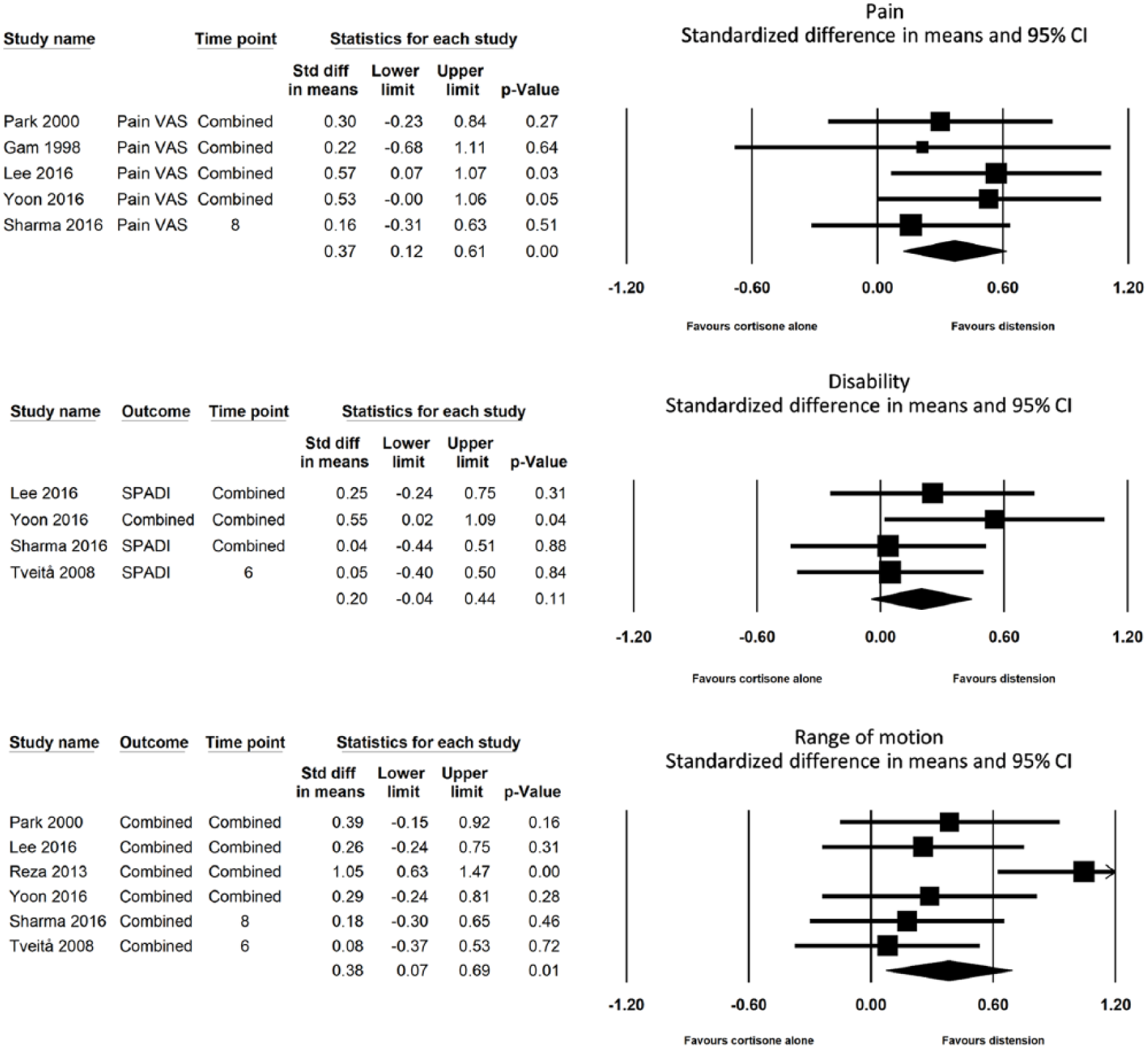
Forest plots of pooled effect sizes.
Meta-regression analysis was conducted for statistically significant pooled effects (pain severity and change in the range of shoulder motion) (Fig. 4). The regression coefficient for the correlation between injected volume and the magnitude of effect size (measured by pain severity) was 0.01 (95% CI: −0.01 to 0.04; p = 0.27). The amount of injected solution did not have a substantial effect on the reduction in pain severity. When adding that amount of injected solution >30 mL, the effect on ROM increased, although still only around 0.3. The regression coefficient for the correlation between injected volume and the magnitude of effect size (measured by ROM) was 0.02 (95% CI: 0.0–0.037; p = 0.028).
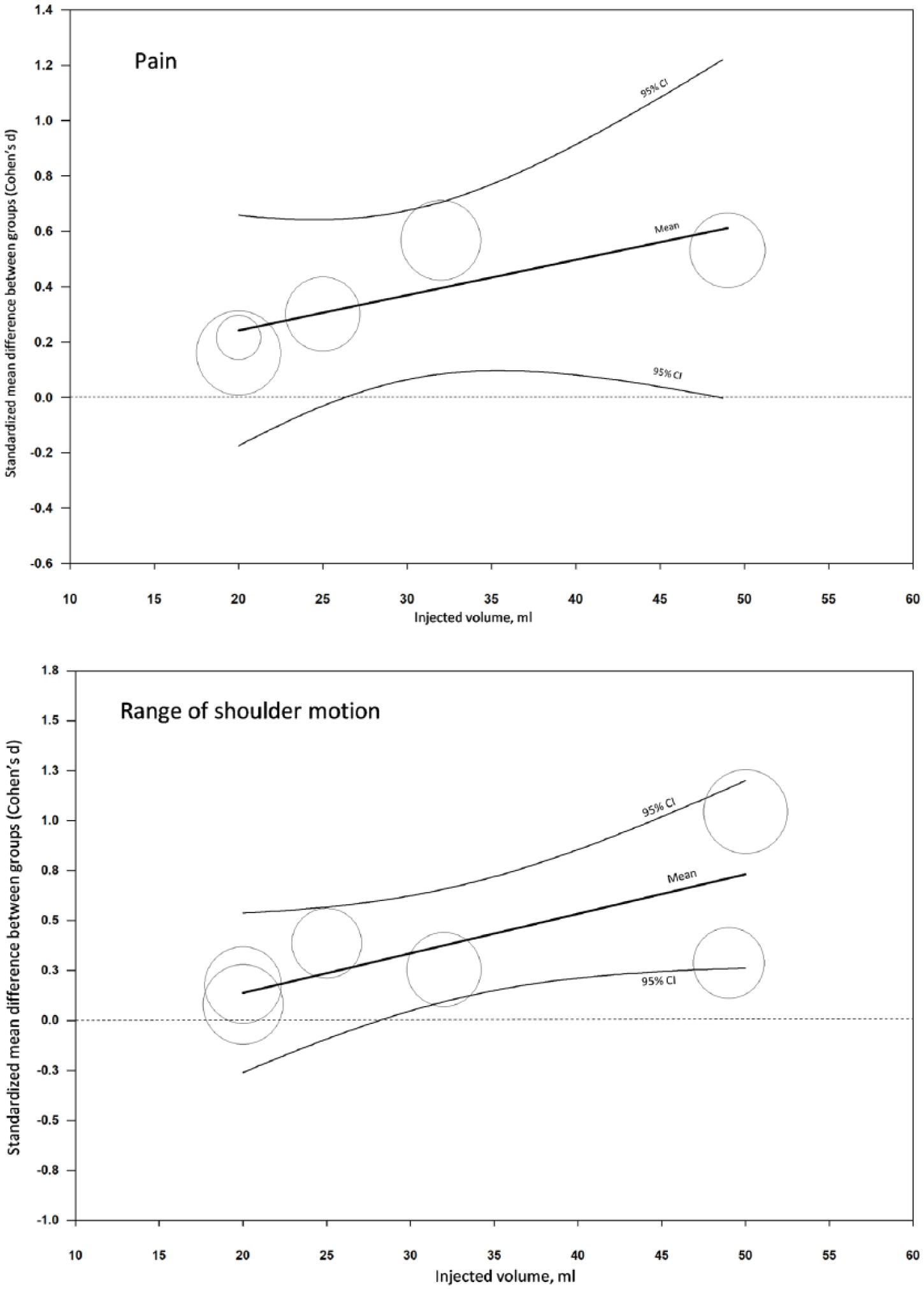
Meta-regression scatter plots.
The risk of publication bias was overall small without a need for a trim-and-fill correction: for pain severity, Egger’s regression intercept was −0.42 (95% CI: −6.23 to 5.39), for disability level 12.76 (95% CI: 0.60–24.93), and for ROM −8.81 (95% CI: −28.96 to 11.35), respectively. The heterogeneity level was 0% (measured by I2) for pain severity and disability level and 60% for ROM. Excluding papers with high risk of systematic bias from the analysis did not significantly change the magnitude of pooled effects.
Discussion
The main result of this review is that, according to current evidence, hydrodilatation seems to have a small-size effect in patients with adhesive capsulitis measured by pain reduction and ROM improvement. While this effect was statistically significant, it did not achieve the level of clinical significance demonstrating unacceptably high NNT figures. In other words, at least 12 patients should undergo the procedure to achieve any improvement comparing to controls. Hydrodilatation did not improve disability levels in the studied populations. Our results were based on seven RCTs with mostly low risk of systematic bias. Additionally, the results suggested that the amount of injected fluid does not substantially affect the magnitude of the effect when measured by pain reduction and has only a small effect on shoulder ROM.
When generalizing the results, it should be kept in mind that meta-synthesis is always only an approximation, especially in small samples. The reliability of meta-analysis depends greatly on the preciseness of variance figures reported by original research. In this meta-analysis, several approximation and imputations were made when converting medians into means and ranges and confidence limits into variances. In addition, this review measured the effectiveness of hydrodilatation by only a few outcomes—change in pain severity and disability level and improvement in ROM. Thus, many potentially relevant outcomes were not taken into account—such as incidence of complications, the effect of procedure on recovery speed, or differences in patient satisfaction. On the other hand, this study is the first one that has succeeded to identify seven RCTs on the topic. The meta-analysis included sensitivity and sub-group analyses and meta-regression ensuring the reliability of the findings. Some uncertainty concerning the preciseness of injections is to be taken into account as visual guidance method was also included in the review even if the joint space in frozen shoulder may be very small and difficult to reach without radiological guidance. In the study by Mun and Baek (24), the true effect of hydrodilatation was uncertain as hydrodilatation was combined with interscalene block, manipulation, and corticosteroid.
These results differ from the results of previous reviews on the topic (1, 2, 5, 6, 8–11, 27). While previous reviews did not find evidence on the effectiveness of hydrodilatation, the present review suggests that there is support for the use of hydrodilatation to treat adhesive capsulitis, but with only small or insignificant effect sizes. This leads to a conclusion that no additional research on the subject is needed. Considering the invasive character of the hydrodilatation procedure, its’ further testing could be difficult to justify especially from an ethical point of view.
Conclusion
According to current evidence, hydrodilatation has only a small and insignificant clinical effect when treating adhesive capsulitis of the shoulder.
Supplementary Material
Supplementary Material, Supplementary_material – Effectiveness of Hydrodilatation in Adhesive Capsulitis of Shoulder: A Systematic Review And Meta-Analysis
Supplementary Material, Supplementary_material for Effectiveness of Hydrodilatation in Adhesive Capsulitis of Shoulder: A Systematic Review And Meta-Analysis by M. Saltychev, K. Laimi, P. Virolainen, M. Fredericson in Scandinavian Journal of Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.