
Abstract
Background and Aims:
To investigate the paraclinical and pathological features of surgically resected intraductal papillary mucinous neoplasms in Sweden.
Materials and Methods:
A review of prospectively collected data on patients undergoing pancreatic resection for a histopathologically verified intraductal papillary mucinous neoplasm between 2010 and 2016 was performed using the Swedish National Registry for Pancreatic and Periampullary Cancer.
Results:
A total of 3038 pancreatic resections were performed during the study period, of which 251 (8.3%) were due to intraductal papillary mucinous neoplasms. The intraductal papillary mucinous neoplasm cases comprised 227 noninvasive and 24 invasive lesions. There was an annual increase in the number of resected intraductal papillary mucinous neoplasms, from 13 in 2010 to 56 in 2016, and an increase in the proportion of intraductal papillary mucinous neoplasm to the total number of pancreatic resections (4.7%–11%). Biliary obstruction was the only independent predictor of invasive disease, with odds ratio 3.106 (p = 0.030). There was no difference in survival between low-, intermediate-, and high-grade dysplastic lesions (p = 0.417). However, once invasive, the prognosis was severely impacted (p < 0.001). Three-year survival was 90% for noninvasive intraductal papillary mucinous neoplasm and 39% for invasive intraductal papillary mucinous neoplasm. Survival was better in lymph node negative invasive intraductal papillary mucinous neoplasm (p = 0.021), but still dismal compared to noninvasive lesions (p < 0.001).
Conclusion:
The number of surgically resected intraductal papillary mucinous neoplasms is increasing in Sweden. Biliary obstruction is associated with invasive disease. Low-to-high-grade dysplastic intraductal papillary mucinous neoplasm has an excellent prognosis, while invasive intraductal papillary mucinous neoplasm has a poor survival rate.
Keywords
Introduction
Intraductal papillary mucinous neoplasm (IPMN) is a cystic tumor arising from the epithelial cells lining the pancreatic ducts (1). IPMN is a heterogeneous disease with a spectrum of clinical and molecular features affecting the likelihood of transformation from low-grade dysplasia (LGD) to invasive carcinoma. On the basis of the ductal involvement, IPMNs are divided into main-duct (MD-IPMN), branch-duct (BD-IPMN), or mixed-type IPMN. There are significant differences in frequencies of malignancy between the morphological types. MD-IPMN has a higher risk for malignancy compared to BD-IPMN (2). IPMN with an invasive carcinoma has been shown to have better survival compared to conventional pancreatic ductal adenocarcinoma (3). According to the latest World Health Organization (WHO) recommendations, the dysplastic grades of IPMN should be designated as low, intermediate, or high grade (4). The term carcinoma in situ is replaced by “high-grade dysplasia” (HGD). When invasive carcinoma occurs, the relationship between the IPMN and the carcinoma should be specified as either “derived from” or “concomitant.” The term “malignancy” has been used frequently, but should only be applied to invasive disease to ease comparison between studies (2).
IPMNs are increasingly being recognized due to advances in cross-sectional imaging and increased usage thereof (5, 6). As a result, the frequency of pancreatic resections, which are performed due to an underlying IPMN, is increasing (7). In the United States, high-volume pancreatic units report an increased frequency of noninvasive and invasive IPMNs, from 1% to 2% in the 1980s and 1990s to 8% in the 2000s (8, 9). However, nationally, a decreasing incidence of invasive IPMN was observed for the period 1990–2010, when the Surveillance, Epidemiology, and End Results (SEER) database was queried (10).
The preoperative assessment of IPMN continues to be a challenge, as the risk of harboring a high-risk lesion must be balanced against the morbidity associated with pancreatic surgery. In this study, we investigate the experience with the surgical management of IPMN in Sweden, with specific emphasis on the following research areas:
What are the trends in the incidence of resected IPMN?
Which preoperative factors can predict invasiveness?
Does the grade of dysplasia affect prognosis?
Materials and Methods
Study Population
For this study, we utilized the Swedish National Registry for Pancreatic and Periampullary Cancer. The registry data are stored on a web-based platform (INteractive Content Architecture (INCA)) and contains information on pancreatic resections performed in Sweden from December 2009. In this study, we analyzed data from January 2010 until the end of 2016. The coverage of the registry, which is controlled against the Cancer Registry Statistics by the National Board of Health and Welfare in Sweden, for the included years from 2010 to 2016 are 74%, 77%, 89%, 90%, 95%, 94%, and 88%.
The study conformed to the Strengthening The Reporting of OBservational Studies in Epidemiology (STROBE) guidelines (11).
Selection Criteria and Data Extraction
Only patients with a histopathologically verified resected IPMN were included. Data were extracted from the registry using a predesigned collection form. The following information was extracted: preoperatively assumed diagnosis (IPMN, cystic or solid tumor), age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) score, smoking status, diabetes mellitus, biliary obstruction (bilirubin >50 µmol/L or requirement of biliary drainage preoperatively) (12, 13), carbohydrate antigen (CA) 19-9, type of surgery, postoperative complications (in-hospital or within 30 days), and histopathology (tumor size, lymph node status, radicality of resection (R-status, defined as R1 < 1 mm from margin), and grade of dysplasia). Invasive lesions were classified according to the American Joint Committee on Cancer TNM staging system, 7th edition (14). Mortality (overall survival) was checked against the national death registry through 10 June 2017.
Statistical Analysis
Continuous data are presented as median with interquartile range and categorical data as frequencies with percentage. Baseline characteristics between groups were compared using Mann–Whitney U tests for continuous variables and the chi-square or Fisher’s exact tests for categorical variables. Kaplan–Meier analysis was performed to estimate survival with statistical differences between the survival curves assessed using the log-rank test. Potential risk factors of malignancy were identified with multiple logistic regression analyses. Predictors included age, gender, BMI, ASA score, diabetes mellitus, smoking, biliary obstruction, CA19-9, and tumor size. A p value < 0.25 in univariable analysis was a criterion for inclusion in the multivariable analysis. In the iterative process of variable selection using forward and backward stepwise selection, covariates were removed from (p > 0.1) and added to (p < 0.1) the model, respectively, as described by Hosmer–Lemeshow (15), resulting in the primary main effect model. To handle missing values, which were considered to be missing completely at random (MCAR), the chained equations multiple imputation technique, as described by White et al. (16), was used. The imputation method was predictive mean matching (PMM). In all, 10 imputations with 10 iterations were performed. The factors included in the imputation model (imputed and used as predictor) included age, gender, BMI, ASA score, diabetes mellitus, smoking, biliary obstruction, CA19-9, tumor size, and invasiveness. Of those with missing values (invasiveness, age, and gender had no missing values) the range spanned from 0.8% (diabetes and ASA score) to 28.3% (tumor size). A p value < 0.05 was considered statistically significant. STATA MP Version 14.1 was used for all statistical analyses.
Results
The Cohort
A total of 3038 pancreatic resections were recorded during the study period. We identified 251 patients with histopathologically verified IPMN (Table 1). The median age was 69 years, 54% were female, 20% had diabetes mellitus, and 17% were smokers. The most commonly performed surgical procedure was a pancreaticoduodenectomy (53%), followed by distal pancreatectomy (27%) and total pancreatectomy (16%). A total of 36% had a major postoperative complication, classified as a Clavien-Dindo score ≥ 3, and the 30-day mortality was 2%. The median tumor size was 3 cm.
Patient characteristics.
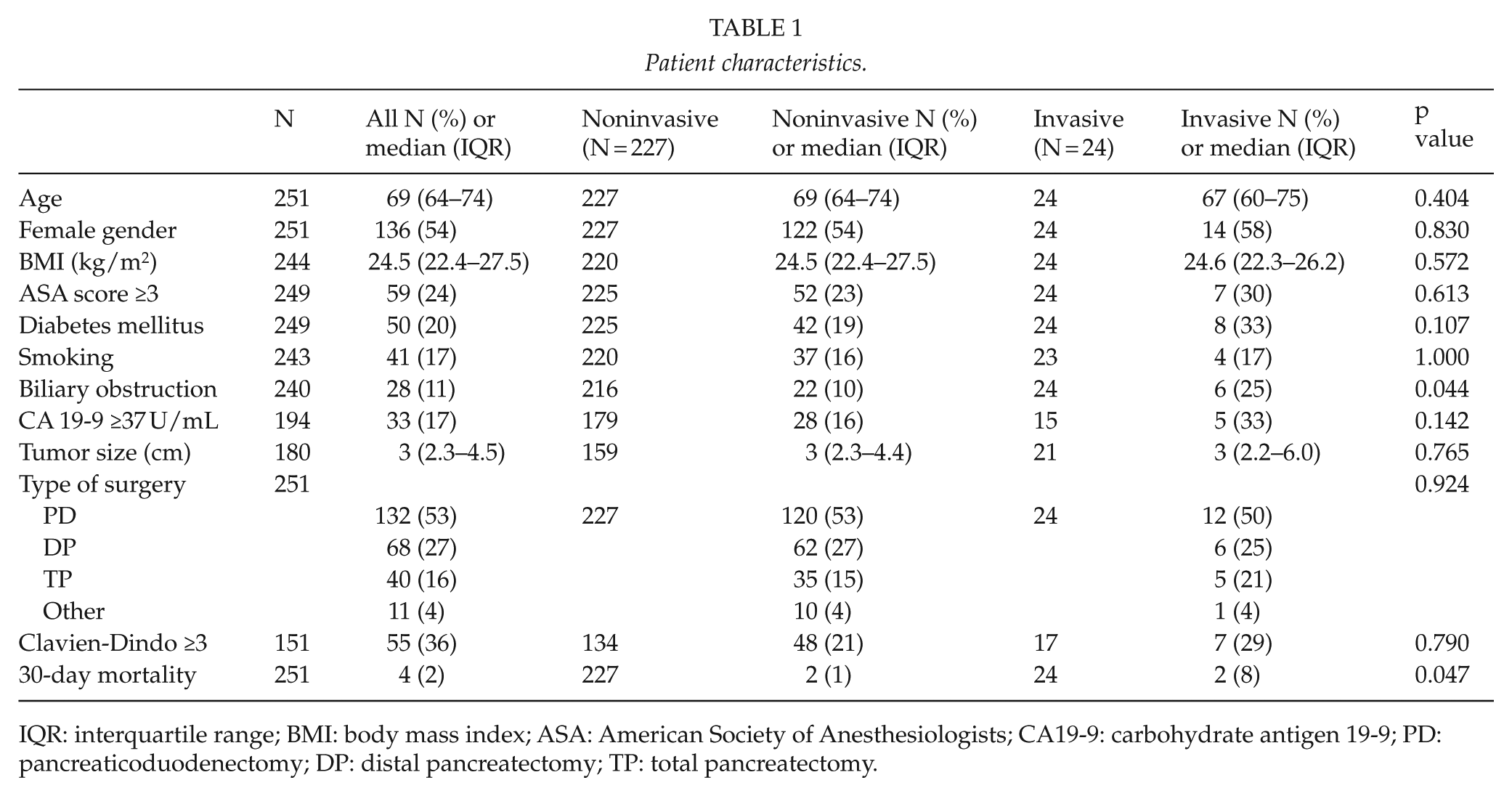
IQR: interquartile range; BMI: body mass index; ASA: American Society of Anesthesiologists; CA19-9: carbohydrate antigen 19-9; PD: pancreaticoduodenectomy; DP: distal pancreatectomy; TP: total pancreatectomy.
Trends in the Incidence of Resected IPMNs
The total annual number of resected IPMNs recorded in the registry increased during the study period from 13 cases in 2010 to 56 cases in 2016 (see Fig. 1). There was a decrease in the number of invasive IPMNs resected during the study period as 4 out of 13 patients (31%) in 2010 were found to have invasive IPMNs compared to only 1 out of 56 patients (2%) in 2016.
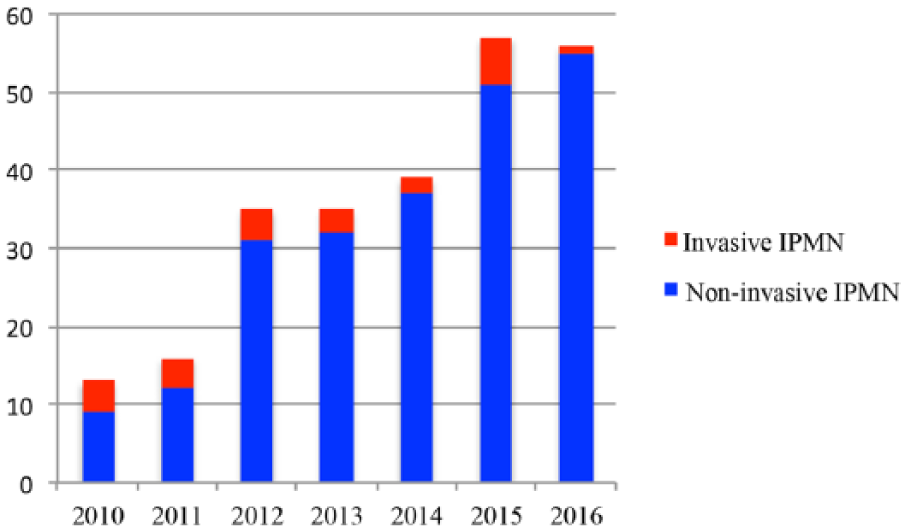
Annual number of surgically resected IPMNs according to the Swedish National Registry for Pancreatic and Periampullary Cancer (2010–2016).
The total number of recorded pancreatic resections was 278 in 2010, which steadily increased to 528 in 2016. Comparison of the number of histopathologically verified IPMN with the total number of recorded resections during the study period (2010–2016), the percentage of surgically resected IPMN was 8.3% (251/3038). IPMN represented 4.7% of pancreatic resections in 2010, which increased to 9.5% in 2016.
Predictors of Invasive Disease
Biliary obstruction was the only independent predictor of invasive disease, with odds ratio (OR) 3.106 (p = 0.030), as shown in Table 2.
Logistic regression for predicting invasive disease.
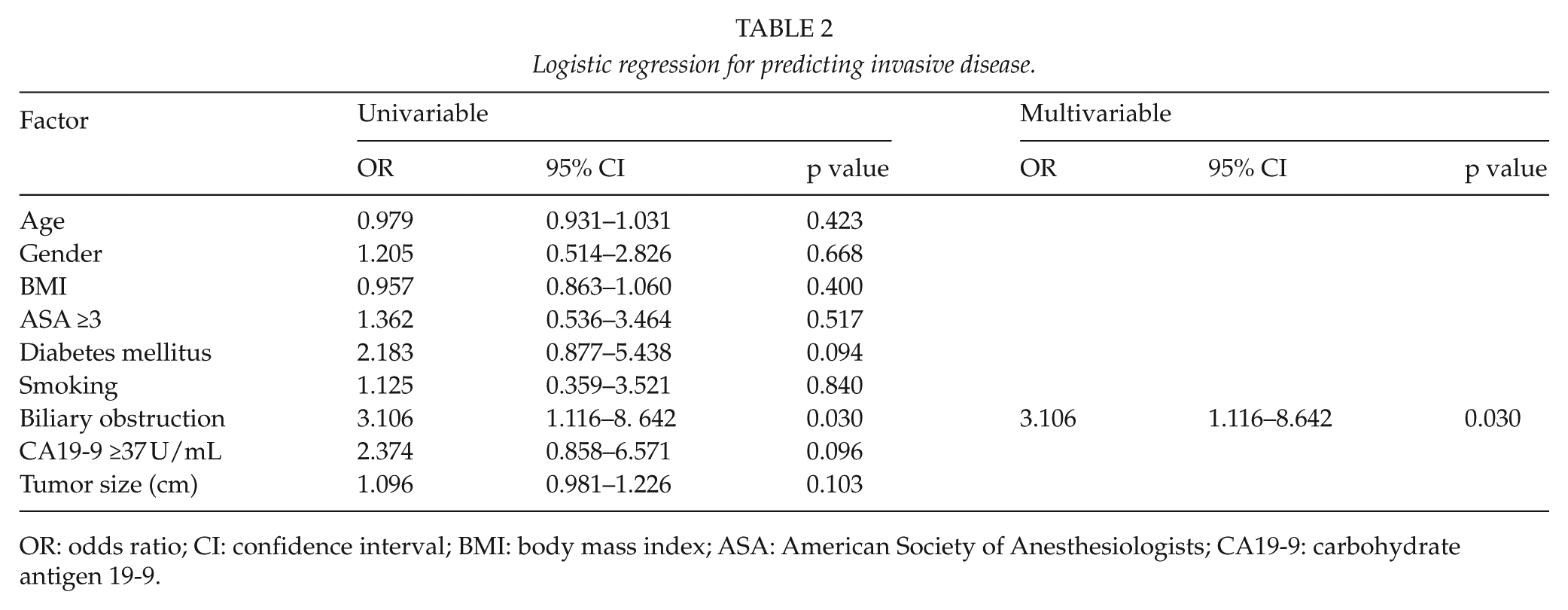
OR: odds ratio; CI: confidence interval; BMI: body mass index; ASA: American Society of Anesthesiologists; CA19-9: carbohydrate antigen 19-9.
Dysplastic Grades of IPMN
Of the 251 patients, 227 were classified as noninvasive IPMN and 24 as invasive IPMN. Of the noninvasive IPMN cases, the dysplastic grade was recorded in 213 patients, including LGD in 65 patients, intermediate grade dysplasia (IGD) in 88 patients, and HGD in 60 patients. No concomitant synchronous malignancy was recorded in the noninvasive IPMNs.
Comparing HGD versus LGD and IGD showed that the type of surgery differed between groups (p = 0.001). Total pancreatectomy was performed in 30% (n = 18) of HGD compared to 10% (n = 16) of LGD and IGD and distal pancreatectomy in 20% (n = 12) of HGD compared to 31% (n = 47) of LGD and IGD. The different dysplastic grades of IPMN did not impact survival following surgery (p = 0.417). Similar 1- and 3-year survival rates were observed (Table 3).
Survival rates in IPMN with different grades of dysplasia.
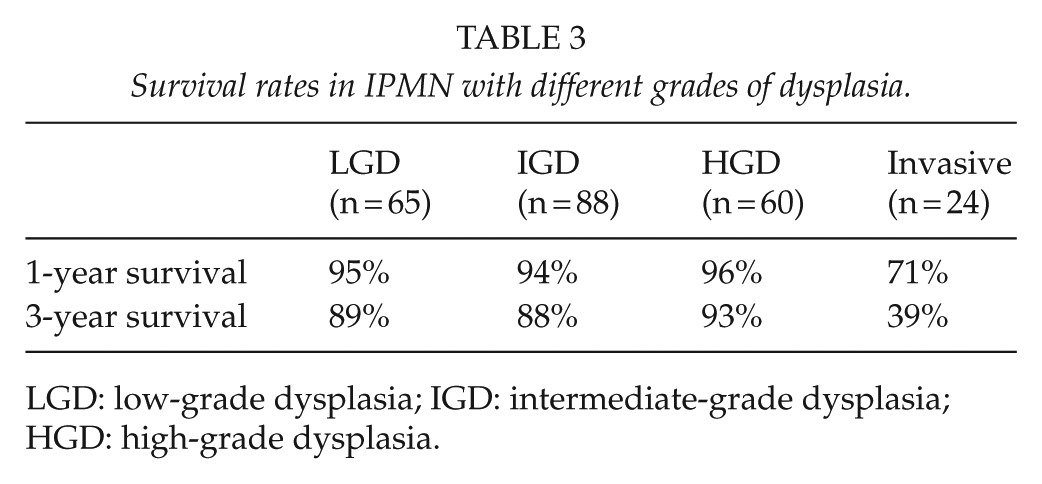
LGD: low-grade dysplasia; IGD: intermediate-grade dysplasia; HGD: high-grade dysplasia.
However, once invasive, the survival was significantly impaired (p < 0.001; Fig. 2). This observation persisted even when excluding lymph node positive invasive IPMN, p < 0.001 (data not shown). Three-year survival was 90% for noninvasive IPMN and 39% for invasive IPMN.
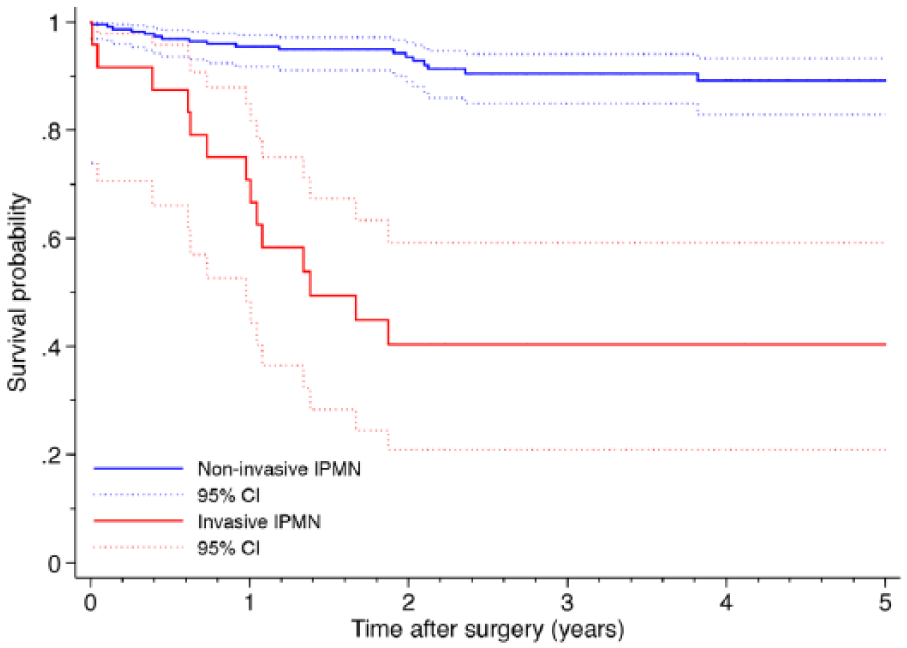
Kaplan–Meier survival curves according to noninvasive and invasive IPMN. The solid lines show the observed cumulative survival and the dotted lines show the 95% confidence interval (estimated with Kaplan–Meier survival function).
Of the invasive lesions, five patients were staged as IA, five patients as IB, eight patients as IIB, two patients as IV, and four patients had unknown stage. Ten (10/23; 42%) of the invasive IPMNs had lymph node metastasis, with two cases showing distant metastasis. Eight patients (8/22; 33%) had R1 disease. Lymph node metastasis (p = 0.021) and R1 resection (p = 0.009) were significant prognostic factors in patients with invasive IPMN. The extent of surgery (total vs partial pancreatectomy) did not impact survival (p = 0.273).
Discussion
In this study, the national trends in IPMNs were investigated in Sweden using registry data. There was an increase in the annual number of resected IPMNs during the study period. This may in part be explained by the increased coverage of the registry. However, increased annual numbers of resected IPMNs are seen in our local database from Lund, where we have 100% coverage since 2000. Lund is part of the National Registry. The frequency of IPMNs among resected tumor specimens was stable at around 8% when accounting for the total number of resections performed. Other centers have reported similar percentages (17). However, there was a decrease in the percentage of invasive IPMNs. A decrease in the number of resected invasive IPMNs has been demonstrated by other studies (10). The reason for this decrease may be explained by the increased awareness and detection at a noninvasive stage, with a more aggressive approach in the selection of surgical candidates. Unfortunately, assessment of surgical indication could not be performed in this study.
The revised International Consensus Guidelines (2) recommend that all IPMNs with suspected main pancreatic duct involvement should undergo surgery due to the higher frequency of HGD and invasive disease. In branch-duct IPMN, different radiological features classified as “high risk stigmata” and “worrisome features” are used to assess the need for surgical intervention. In this study, biliary obstruction remained significant in multivariable analysis. This feature is also stated in the international consensus guidelines (2). Serum CA19-9 was a relatively poor predictor of malignancy in our study. However, a recent meta-analysis found that an elevated serum CA19-9 was the most specific factor for predicting HGD or invasive cancer with a pooled specificity of 90.3%. However, the pooled sensitivity was only 38.0% (18). In another meta-analysis focusing on CEA and CA19-9, the pooled specificity and sensitivity of serum CA19-9 in predicting invasive IPMN were 88% and 52%, respectively.
Low-grade and intermediate-grade dysplastic IPMN have previously been demonstrated to have excellent prognosis (19–22). We found no difference in survival for noninvasive lesions when stratified by dysplastic grades. These results are in line with several other studies. Chari et al. (20) found a 5-year survival of 88% for noninvasive IPMN (classified as adenoma, borderline, and carcinoma in situ). In a study by Rezaee et al. (22), the median overall survival was similar between LGD/IGD and HGD at 118 and 92 months, respectively. Kang et al. (21) found a significantly worse 5-year survival in HGD compared to LGD/IGD at 83% and 90%, respectively.
Once IPMN becomes invasive, the prognosis is poor. In the US National Cancer Database, the median overall survival for invasive IPMN was 28.9 months with a 1- and 5-year survival of 76% and 17%, respectively (23). Our findings are in concordance, with a 1- and 3-year survival of 71% and 39%, respectively. These numbers indicate a slightly better prognosis for invasive IPMN as a group compared to conventional pancreatic ductal adenocarcinoma, which may partly be explained by differences in tumor biology (3, 24). In this study, 43% was found to have lymph node metastasis on histopathology.
The choice of surgical procedure should be based on oncological safety, which means that intended partial resections may be extended to frank total pancreatectomy. Frozen sections of the cut surface can guide surgeons during the operation (2). The extent of the surgery and the acceptable grade of margin dysplasia are controversial topics. A meta-analysis from 2016 concluded that noninvasive IPMN at the resection margin may not warrant further resection (25). A more aggressive approach has been proposed by the European Study Group on Cystic Tumours of the Pancreas when suspecting invasive IPMN (26). In this study, frozen sectioning was performed in about one-third of the operations and the R-status was prognostic in patients with invasive IPMN.
The multifocal nature of IPMN is an important topic, and may be partly responsible for disease recurrence even in the setting of R0 disease (27). The overall recurrence rate has been found to be 10%–17% (21, 28, 29) and invasive IPMN may recur at a much higher rate (22, 28, 29). Even noninvasive IPMN has been found to recur with distant metastasis (21). Some studies have found that a lesion with HGD on initial resection is a risk factor of recurrent disease compared to lower grades of dysplasia (21, 27), while the rate of recurrence seems to be similar in other studies (28, 29). In a recently published multicenter study, HGD and invasive carcinoma in BD-IPMN were found to be risk factors for recurrent disease. However, only patients with initial invasive IPMN recurred with a new invasive lesion (30).
The results of this study carry limitations associated with the retrospective analysis of a registry database, the quality of the source data, the number of missing data, and the lack of standardization associated with multicenter studies. The preoperative imaging findings were not available and the morphological types of IPMN were only stated in a minority of the cases in the registry. The relatively short follow-up time is another limitation. These limitations should be considered when interpreting our findings. However, this is the first national study evaluating IPMNs in Sweden, and as such provides important information regarding current management of the disease from a national perspective.
Conclusion
The number of resected IPMNs is increasing in Sweden. Biliary obstruction was associated with invasive disease. IPMN has an excellent survival rate if resected at a noninvasive stage, even in high-grade dysplasia. However, once invasive, the prognosis is severely impacted.
Footnotes
Acknowledgements
Thanks are due to the HPB surgeons of Sweden for reporting data to the Swedish National Registry for Pancreatic and Periampullary Cancer and to all persons involved in maintaining the registry.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Regional Human Ethics Committee in Lund Sweden (dnr 2015/393).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by funding from SWElife/Vinnova, the Royal Physiographic Society of Lund, the Magnus Bergvall Foundation, the Tore Nilsson Foundation, and the Inga and John Hain Foundation for Medical Research.