
Abstract
Background and Aims:
Hypothermic circulatory arrest carries a high risk of mortality and neurological complications. An important part of assessing surgical treatment is the evaluation of long-term survival and postoperative health-related quality of life.
Material and Methods:
In this prospective study, 30 patients undergoing hypothermic circulatory arrest during surgery of the thoracic aorta, and 31 comparison patients undergoing elective coronary artery surgery without hypothermic circulatory arrest were evaluated for long-term survival and health-related quality of life, using the RAND 36-Item Health Survey questionnaire. The results were compared to national age- and sex-matched reference populations of the chronically ill and healthy adults.
Results:
After 4.6–8.0 years, available study (88%) and comparison (59%) patients were interviewed. The life expectancy was similar with 4- and 8-year survival of 90%, and 87% for the study group, and 94%, and 94% for the comparison group, respectively (log rank test, p = 0.62). The RAND-36 scores for study and comparison groups were congruent in all dimensions, describing physical, mental, and social domains. The study patients’ health-related quality of life results were similar to the national reference population with chronic illnesses.
Conclusion:
After hypothermic circulatory arrest, patients undergoing surgery of the thoracic aorta achieve a similar long-term life expectancy and health-related quality of life as do patients undergoing coronary surgery without hypothermic circulatory arrest, and a health-related quality of life similar to the national reference population with chronic illnesses. These results justify operative treatment in this high-risk patient population.
Keywords
Introduction
The last few decades have born witness to significant advancements in surgical technologies and treatments. Many previously fatal conditions can be treated effectively and thus have become rather long-term chronic diseases. This progression has raised questions of an individual’s perception of well-being, such as what the long-term effects of a medically relevant treatment are from a humane point of view. This determining of the health-related quality of life (HRQoL) is also highly useful in evaluating cost-effectiveness of healthcare. Several tools measuring the ability to function in everyday life have been developed, such as HRQoL questionnaires. These are either generic or disease-specific, addressing a particular condition (1).
Circulatory arrest, which is needed for surgical treatment of thoracic aorta diseases, carries a high risk (2%–14%) for permanent neurological injury, despite protective hypothermia (2). Early mortality after surgery is estimated at 4%–5% (3, 4), and of the surviving patients up to 7% never return to an independent lifestyle (3). In coronary artery bypass surgery (no circulatory arrest), the risk of perioperative stroke is 2.6%, which increases morbidity and mortality (5).
Various studies examine HRQoL after hypothermic circulatory arrest (HCA) and interventions on the thoracic aorta. However, most of these studies are retrospective cohorts, with greatly varying follow-up periods ranging from 6 months to 10.2 years, with shorter follow-up times being more frequent (6). Lohse et al. (4) used the 36-Item Short Form Health Survey (SF-36) to assess the HRQoL in patients with true aneurysms after surgical replacement of the ascending aorta. Khaladj et al. (7) focused on neurological outcome and HRQoL (SF-36) after aortic root surgery with HCA. The RAND 36-Item Health Survey (8), which is almost identical with the SF-36 questionnaire (9), has also been used (10, 11) in elderly patients with acute type A aortic dissection, as well as in patients after cardiac resuscitation following coronary artery bypass grafting (12). Generally, the HRQoL after thoracic aortic and cardiac surgery has been acceptable and often even comparable to an age- and sex-matched general population (4). Few studies with a baseline HRQoL assessment exist, which complicates the evaluation and comparison of the HRQoL outcomes.
The aim of this prospective study was to investigate the long-term HRQoL of patients undergoing HCA during surgery of the thoracic aorta and to compare the results with patients undergoing elective cardiac surgery without HCA, and with national reference populations of the chronically ill and healthy individuals.
Material and Methods
The planned recruitment of 30 study patients (elective or emergency aortic surgery with HCA) and two comparison groups of 15 patients each (elective coronary artery bypass grafting, with cardiopulmonary bypass or off-pump) was initiated in November 2007. All patients were recruited by November 2011. Inclusion criteria for the study group were the use of HCA during elective or emergency surgery of the thoracic aorta. Perioperative temperature measurements were obtained via nasopharyngeal and central venous catheters.
Follow-Up and HRQOL
Interviews for HRQoL were performed during November 2015, at which point survival was also confirmed from the National cause of death registry. Interviews for HRQoL were conducted using the age- and sex-matched Finnish version of RAND 36-Item Health Survey, which was posted to all study participants. If no answer was received, patients were contacted by phone. The RAND 36-Item Health Survey instrument (8) was selected because it is one of the most widely used HRQoL survey instruments, and because it has been validated for the Finnish adult population (n = 2175; year 1995) (9). The RAND-36 consists of an eight-dimensional questionnaire, with scores transformed to a 0- to 100-point scale (with low scores denoting greater limitations and problems in performance), measuring (I) physical functioning, (II) role—physical (role limitation due to physical impairment), (III) bodily pain, (IV) general health, (V) vitality, (VI) social functioning, (VII) role—emotional (role limitation due to emotional impairment), and (VIII) mental health. The determining of the chronically ill reference population is based on self-reported chronic illnesses at the time of the questionnaire.
Aortic aneurysms and coronary artery disease are chronic illnesses, as are most of the risk factors of both conditions. These risk factors, such as hypertension, diabetes, and active smoking, are common in patients requiring aortic or coronary surgery (13, 14). In addition, after aortic surgery, most patients receive antihypertensive medication, and patients with concomitant cardiac procedures (e.g. coronary artery bypass grafting) receive beta blockers. Therefore, comparing the HRQoL results to a reference population with chronic illnesses was the primary aim of this study, and comparison between the two groups and with a healthy reference population were secondary aims.
Statistics
With a non-Gaussian distribution of data and an inherent skewness of HRQoL questionnaire results, the results are reported as median values with range, or 95% confidence interval (95% CI) for HRQoL data. The demographic and clinical data of the study and comparison groups were analyzed by the Mann–Whitney U test, or Pearson χ2 test for categorical variables. Overall survival was obtained by the Kaplan–Meier analysis and the log rank test was used to compare survival times between groups. Quality of life analyses were performed with the Mann–Whitney U test for the study group to comparison group comparison, and with the Wilcoxon one-sample signed rank test for reference population comparison. Missing data lead to post hoc sensitivity analysis with the multiple imputation method to assess the robustness of the results and conclusions. Little’s MCAR (missing completely at random) test was used to determine the pattern of missing data.
The type I error was set at 5% (two-sided) for all statistical tests. The statistical analyses were carried out using IBM SPSS Statistics 21 (IBM Corporation, NY, USA). The study was approved by the Helsinki University Hospital Ethics Committee.
Results
The HRQoL interview was answered by 88% (23 of 26 survived) of the study patients and 59% (17 of 29 survived) of the comparison group patients, with 10 (67%) patients from the on-pump and 10 (50%) from the off-pump group. With a lower than anticipated response rate in the two comparison groups, the two groups were merged for further analysis. The median (range) follow-up time at interview for the study group was 6.8 (5.0–8.0) years and 6.3 (4.6–7.8) years for the comparison group.
The demographic and clinical data are presented in Table 1. The results show some significant differences, with higher risk scores and neurological complications (defined as ischemic lesions on postoperative CT scan) in the study group, while in the comparison group there was a higher percentage of a history of smoking and diabetes.
Demographics, and postoperative clinical data of all patients (N = 61).
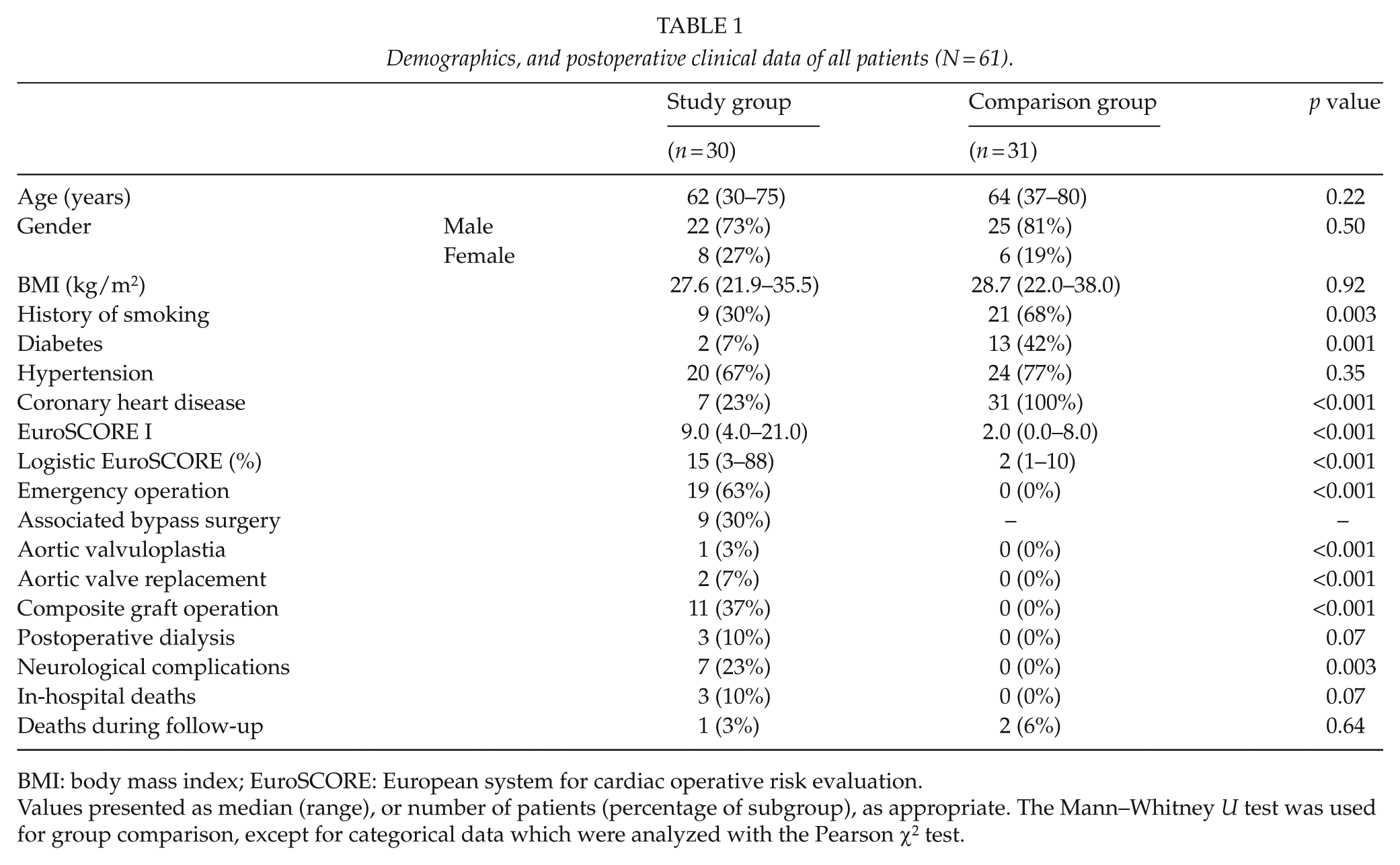
BMI: body mass index; EuroSCORE: European system for cardiac operative risk evaluation.
Values presented as median (range), or number of patients (percentage of subgroup), as appropriate. The Mann–Whitney U test was used for group comparison, except for categorical data which were analyzed with the Pearson χ2 test.
In the study group, two (7%) had suffered a previous stroke prior to surgery, but made a full recovery with no remaining neurological symptoms. In the comparison group, one (3%) patient had suffered a previous transient ischemic attack and undergone carotid endarterectomy without neurological complications. None of the patients had permanent neurological symptoms at the time of recruitment.
All patients were operated via a median sternotomy, except for one (2%) study group patient (left thoracotomy, dissection tear in ascending aorta but extending retrogradely to the ascending aorta). Antegrade selective cerebral perfusion was initiated for 16 (53%) study patients, with 11 (69%) patients perfused from the right side, and 5 (31%) patients bilaterally. The perfused artery was the carotid in 11 (69%) patients, and the axillary artery in 5 (31%) patients, with a median (range) cerebral perfusion time of 23.5 (11–80) min. One of the recruited off-pump patient’s operation was converted into an on-pump operation during surgery, resulting in 16 on-pump comparison patients.
The surgical perfusion was performed via the ascending aorta in 5 (17%) patients, via the axillar artery in 6 (20%) patients, and via the femoral artery in 19 (63%) patients. For the study patients, the median (range) cardiopulmonary bypass time was 208 (121–372) min, aortic clamping time 113 (28–215) min, and circulatory arrest time 25 (9–110) min. For the on-pump comparison patients, the median (range) cardiopulmonary bypass time was 88.5 (51–117) min and aortic clamping time 65 (34–78) min. The median (range) lowest temperature was 18.2 (15.1–27.6) °C for the study group and 34.2 (28.7–36.2) °C for the comparison group. Of the study group, 23 (77%) were operated under deep hypothermia (≤20 °C), and 7 (23%) under moderate hypothermia (20.1 °C–28.0 °C).
The depth of hypothermia (deep or moderate), the length of arrest, the use of selective cerebral perfusion, and the results of a postoperative brain CT scan were tested against mortality, surgical and neurological outcomes, and later HRQoL. The other variables did not have a significant correlation with any of the tested outcomes, but an abnormal postoperative brain CT scan correlated with a poorer primary neurological outcome (8 of 8 vs 2 of 22; p < 0.001), a higher incidence of neurological complications (8 of 8 vs 0 of 21; p < 0.001), a longer intensive care unit stay (median (range) 7 (1–21) vs 3 (0–18) days; p = 0.02), and an increased need for secondary care hospitalization (6 of 7 vs 6 of 21; p = 0.008).
The reason for surgery in the study group was aortic dissection in 20 (67%) patients, and aortic aneurysm in 10 (33%) patients. Of the dissection operations, 17 (90%) were emergency operations, with the single exception treated conservatively as a type B dissection at admission. A follow-up CT scan showed the dissection continuing retrogradely to the ascending aorta, leading to an immediate operation for type A dissection. Of the aneurysm operations, 2 (20%) were emergency operations, with the remaining 8 (80%) elective operations for chronic conditions. The distal seam was the ascending aorta for 8 (27%) patients, hemiarcus for 15 (50%) patients, aortic arch 3 (10%) patients, and the descending aorta for 4 (13%) patients.
Early Mortality
Overall 30-day mortality was 3% (2 of 61), and 90-day mortality 5% (3 of 61). All deaths occurred in the study group and were categorized as ischemic cardiac-related deaths.
Overall Mortality
During the long-term follow-up, the late mortality was 5% (3 of 58 survived patients). One patient from the study group on anticoagulation and with chronic kidney failure developed a fatal retroperitoneal hematoma after falling down. A patient from the on-pump group developed refractory ischemic heart failure, and another one from the on-pump group died of lymphoma. Of the later deaths, 33% (1 of 3) were cardiovascular deaths. The 1-, 4-, and 8-year survival rate was 90%, 90%, and 87% for the study group, and 100%, 94%, and 94% for the comparison group, respectively (log rank test, p = 0.62). The Kaplan–Meier analysis is presented in Fig. 1, including all incidents after surgery (early and late mortality).
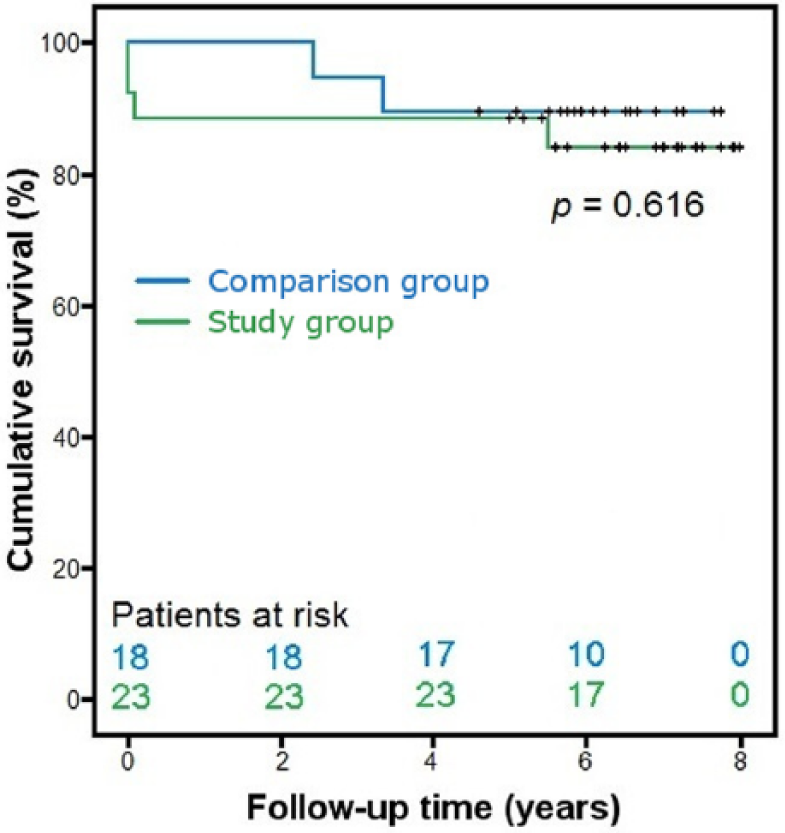
Overall survival of study and comparison groups with the Kaplan–Meier plots and group comparison of survival times. Censor times are marked with “+” on the survival line; log rank test was used for group comparison.
HRQOL
The RAND-36 HRQoL data are presented in Table 2, with comparison to the age- and sex-matched Finnish adult reference populations presented in Fig. 2. The study group did not differ from the reference population with chronic illnesses. When compared to the healthy reference population, the study group had lower median (95% CI) scores in the physical functioning (80.0 (57.5–95.0) vs 91.7 (90.8–92.6); p = 0.001), the role—physical (62.5 (0.0–100.0) vs 87.3 (85.7–88.9); p = 0.02), and the general health categories (55.0 (40.0–70.0) vs 72.9 (71.8–74.0); p = 0.003). The comparison group differed from the reference population with chronic illnesses only in the mental health category, with a surprising result of a higher median (95% CI) score (80.0 (70.0–92.0) vs 70.0 (68.7–71.3); p = 0.009). When compared to the healthy reference population, the comparison group had lower median (95% CI) scores in the physical functioning (75.0 (50.0–85.0) vs 91.7 (90.8–92.6); p = 0.001), role—physical (62.5 (6.3–100.0) vs 87.3 (85.7–88.9); p = 0.05), bodily pain (67.5 (61.3–90.0) vs 85.8 (84.7–86.9); p = 0.02), and general health categories (50.0 (45.0–70.0) vs 72.9 (71.8–74.0); p = 0.004). A post hoc analysis showed no significant difference in HRQoL between patients operated under deep (23/30, 77%) or moderate (7/30, 23%) hypothermia (the Mann–Whitney U test, for all HRQoL categories, p > 0.20).
Quality of life results for study and comparison groups, with comparison of the results of the health-related quality of life RAND 36-Item Health Survey.

Values are given as median (95% confidence interval) and p values were obtained with the Mann–Whitney U test.
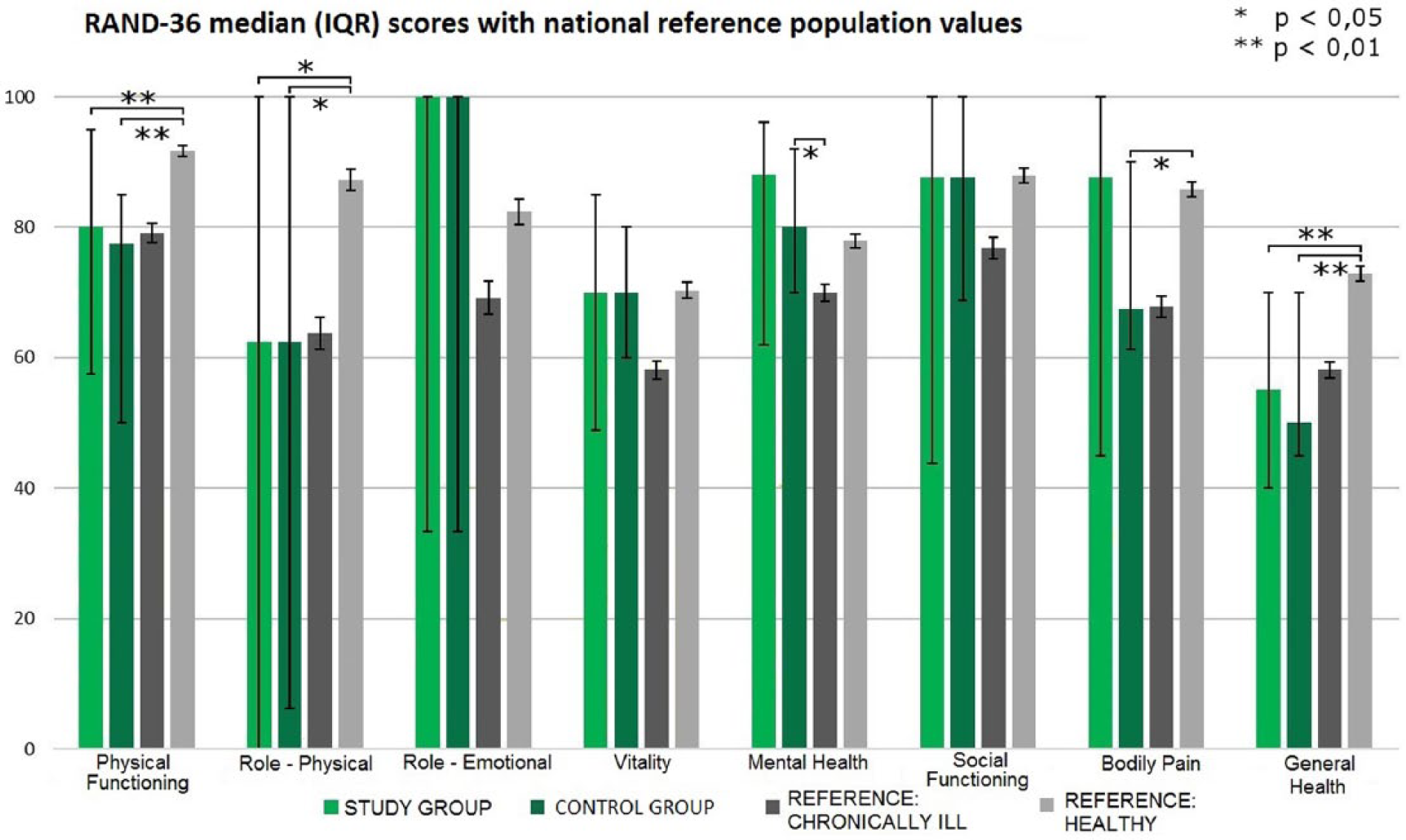
Health-related quality of life questionnaire results of the RAND 36-Item Health Survey for study and comparison groups, with healthy and chronically ill reference populations of the age- and sex-matched Finnish general population for comparison. Statistically significant differences between groups are marked by a staple figure and asterisks denoting the level of statistical significance (above for study group, below for comparison group).
Missing Data
Of the non-responders, one declined answering, one did not feel able to answer, and one never returned the questionnaire. The rest (12 of 15) were lost to follow-up, except for survival data which was available for all patients. Based on a Little’s MCAR test, missing data were deemed to be missing randomly (χ2 = 35.7, Df = 28, p = 0.15).
The results of post hoc multiple imputation testing (20 imputations) confirmed statistical robustness of presented results for the study and comparison group HRQoL correlation, despite missing values. The results of the study group versus national reference populations differed from original results in a few categories, while the results of the comparison group versus reference populations differed in several categories. For study patients compared to the chronically ill, median vitality (p = 0.045) and mental health (p = 0.021) were higher. For study patients compared to the healthy reference population, the median of social functioning (p = 0.028) was higher. For comparison patients compared to the chronically ill reference population, the median physical functioning (p = 0.001), vitality (p = 0.002), and social functioning (p = 0.047) differed significantly. For comparison patients compared to the healthy reference population, the median role—emotional (p = 0.041), social functioning (p = 0.012), and bodily pain (p < 0.001) differed significantly.
Discussion
Patients undergoing HCA during surgery of the thoracic aorta achieve an equal life expectancy and HRQoL as do patients undergoing elective coronary artery surgery without HCA. In addition, they achieve a similar level of HRQoL when compared to the age- and sex-matched general population with chronic illnesses. The study groups’ scores in vitality, mental health, social functioning, and experienced bodily pain were non-significantly higher than the scores of the reference population of the chronically ill, probably reflecting more positive and healthy mental attitudes of survivors of aortic operations. Overall, both study and comparison patients received higher scores in non-physical categories and lowest scores in the role—physical and general health categories. This is probably linked to undergoing and surviving major cardiac surgery; however, such speculation is beyond the scope of this study. Despite a fourth of the study patients suffering neurological complications, the HRQoL for survivors compared favorably with the comparison group and the reference population of the chronically ill, even after accounting for missing data. These results suggest that even though neurological complications are frequent in aortic surgery with HCA (3), patients recover surprisingly well, with only minor adverse consequences on later HRQoL.
With the increasing demands of lowering the cost of healthcare, and the advances in medicine and social care leading to a high life expectancy and reduced general morbidity and mortality (especially in cardiovascular disease), previous quality of life studies is becoming outdated. This prospective study with comparison groups in a Nordic welfare state responds to these challenges, showing that surgery of the thoracic aorta during HCA is feasible in a modern society, and leads to an acceptable HRQoL.
Concerns of the adverse effects of deep hypothermia have shifted clinical care toward moderate hypothermia, with several studies testing the effects on morbidity and mortality (15). Earlier studies have shown that prolonged HCA of up to 40 min does not notably increase the risk for neurological complications (16). In this study, the length of HCA was not associated with adverse outcomes or increased late mortality, even though the longest HCA was an incredible 110 min long. To our knowledge, this is the first study to report that later HRQoL is not affected by the depth of hypothermia (deep or moderate), nor the length of arrest. This is mostly due to the neuroprotection of hypothermia and selective cerebral perfusion, of which the latter was in use in all patients with an arrest time of over 38 min. Ischemic lesions on postoperative brain CT scans correlate with a worse neurological prognosis, but not with a lower HRQoL. While patients with an abnormal postoperative brain CT scan had a worse primary neurological outcome and more neurological complications, there was no significant difference in morbidity, mortality, or late-survival.
Almost half of all the interviewed study patients received aortic valve prosthesis during surgery (10 of 22). Mechanical valves may cause subjective disturbances, which are partly related to the type of valve (17). However, it has also been shown that patients undergoing composite graft aortic root replacement, with a mechanical or tissue valve, achieve an equal HRQoL when compared to those undergoing a David operation (7). How these patients would have scored when compared to a chronically ill population remains unresolved.
The comparison group was composed of patients undergoing elective coronary artery surgery. Their HRQoL was similar to that of the study patients with hypothermic arrest. The original aim was to compare the study patients’ results with a group undergoing cardiac surgery with HCA and a group without HCA. However, due to a low response rate, it was decided post hoc that the comparison would be made with a single group of elective cardiac surgery patients. While the primary analysis showed that the comparison group fared favorably in HRQoL when compared to the national reference populations, the impact of missing data makes it impossible to draw conclusions from these results.
This study has some limitations. With no baseline evaluation and a single time point at which HRQoL was measured, there is no way of controlling confounding factors, or suggesting a direct causal link between surgery and later HRQoL. On the other hand, the study population represents the real-life patient population needing surgical care for diseases of the thoracic aorta. While the study and comparison groups differ notably, and cannot be used as true controls, the similar results of the two groups present a basis for comparing results and show that these groups fare equally in later HRQoL. The patient recruitment was not randomized, nor consecutive. The low response percentage in the comparison group was a major limitation for comparison group analyses; however, based on post hoc testing, the main results of the study remain robust.
The number of prospective, long-term studies (17, 18) on the HRQoL of patients undergoing surgery of the thoracic aorta with HCA remains sparse (6). The follow-up time of the present study was 5–8 years providing a representative period of the postoperative course, being notably longer than in most previous reports (6). Despite the limitations, the results of this study provide valuable insight into the long-term effects on life and HRQoL after HCA during surgery of the thoracic aorta.
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.