
Abstract
Background and Aims:
The course of isolated serratus palsy is difficult to predict, especially if, in initial electromyographic examination, long thoracic nerve function is totally absent. How initial electromyography correlates with long-term outcome of isolated serratus palsy is unknown. We evaluated initial electromyographic examinations of isolated serratus palsy patients and compared these to their long-term outcome. We hypothesized that long-term outcome after electromyographic examination–verified partial nerve injuries is better than that seen in cases of total nerve injuries.
Patients and Methods:
We retrospectively reviewed 90 patients with isolated serratus palsy and with initial electromyographic examination treated by brace or observation only, by determining pain, range of motion, and degree of scapular winging after a mean follow-up of 17.8 years.
Results:
Initial electromyographic examination showed total denervation in 21 cases (22%), partial severe denervation in 30 (33%), and partial moderate or slight denervation in 39 (44%). Recovery of serratus muscle function occurred in 17/21 cases (81%) of total denervation and in 47/69 cases (68%) of partial denervation, p = 0.247. Mean flexion in total denervation recovered to 152° and in partial to 157°, p = 0.301, and abduction to 173° and 174°, p = 0.970. In total denervation, 60% of patients were pain-free, in partial, 48%, p = 0.338. The duration of scapular winging among those 42 who subjectively recovered averaged 15.1 months, in 13 patients with total denervation 15.9 months, and in 29 patients with partial denervation 14.7 months (p = 0.599).
Conclusion:
Initial electromyographic examination does not predict clinical outcomes: ROM, pain, scapular winging and strength, but partial denervation may negatively predict subjective outcome.
Introduction
Serratus palsy, causing scapular winging and disruption of scapulohumeral rhythm, contributes to loss of power and to limited flexion and abduction of the upper extremity; it can be a source of considerable pain (1–12). One important diagnostic tool involves electrodiagnostic studies (13–17).
Fardin et al. (13) reported that electromyographic examination is an important prognostic aid in isolated serratus palsy. In contrast, Klebe at al. (16) found no prognostic benefit from electromyographic examination (EMG), and Friedenberg et al. (14) stated that electrodiagnostic studies, particularly EMG, do not predict its functional outcome. Thus, the role of initial EMG as a prognostic tool in isolated serratus palsy is controversial.
We consider that EMG may play some role in prognosis as well as when considering optimal treatment for isolated serratus palsy. We therefore studied initial electrodiagnostic findings and long-term outcome, determining (1) pain, (2) range of motion (ROM) and strength in flexion, and (3) the presence of long-term scapular winging in serratus palsy patients.
Patients and Methods
We retrospectively reviewed 90 patients with isolated serratus palsy, who had visited the senior author’s office at a tertiary referral center between 1980 and 2008. Criteria for study inclusion were (1) scapular winging caused by serratus palsy, (2) initially EMG-verified isolated long thoracic nerve palsy with total or partial denervation, and (3) adequate recording of history and clinical findings at the start of symptoms. Of these patients, 58 underwent treatment with a scapular brace and 32 underwent no special treatment. We obtained permission to perform this study from the ethics committee of the hospital district where the study was conducted.
Initial evaluation by the senior author (M.V.) included a detailed medical history and physical examination, plus an EMG examination. Many patients had already undergone an EMG examination before that first consultation. During the last 20 years of material collection, the same experienced EMG specialist performed all these examinations, and in many cases, EMG was repeated to control possible healing. Active shoulder motion was measured with a handheld goniometer at 5° intervals assessing bilateral active motion simultaneously, with the patient in a standing position. Active forward flexion and abduction measurement was of the angle formed by the arm and thorax. Scapular-winging recording was with a handheld measure in centimeters as the posterior displacement of the medial border of the scapula from the posterior thorax, that is, from the level of the healthy scapula, at the level of maximal winging; this occurred mostly near the inferior medial border of the scapula, arms at 90 degrees unresisted flexion. The strength of shoulder flexion was not measured.
Customized, in part literature-based questionnaires (18) went by post to the patients along with the invitation to participate in the study. The questionnaire included questions regarding demographics, work history, onset of symptoms and preceding factors, treatment, healing, and current condition. One dichotomous question was whether the patients considered themselves healed or not healed of the condition. The patients completed these questionnaires at home.
At follow-up, all 90 patients each underwent a physical examination by an independent observer (V.P.), who again recorded the patients’ medical history, also checking previous treatment records from other hospitals, which were received by fax or mail. She performed the clinical examination in exactly the same way as with the first consultation. In addition, shoulder flexion strength was measured with a Salter spring balance. We determined whether the palsy was totally, partially, or not at all healed, as indicated by scapular winging, flexion strength, and ROM (totally healed = no scapular winging, normal flexion strength, and ROM; no recovery = situation similar as or worse than at the first consultation; partially healed = all other situations = any condition between totally healed and no recovery).
Descriptive data are presented as proportions or as means. Categorical data were compared with Pearson’s chi-square test and continuous data by Student’s t-test. Statistical analysis was performed with SPSS1 23.0 for Windows (SPSS Inc, Chicago, IL, USA).
Results
The mean age of 90 patients at symptom onset was 31.8 (range 12–54, standard deviation (SD) 11) years. Mean follow-up was 17.8 (range 2–26, SD 7.4) years. Palsy occurred on the right side in 79 patients (88%). Trauma preceded 27 (30%) of the cases, exertion 37 (41%), infection 14 (15%), and surgery/anesthesia 7 (8%); in 5 (6%) cases, no etiologic factor was evident. The first consultation took place a mean 8.7 (range 0.1–33.4) months after symptom onset. The first EMG was carried out a mean 5.1 (range 1–17) months after symptom onset. Initially, the groups sorted by EMG findings did not differ significantly: flexion for the total denervation group versus partial denervation, p = 0.481, and winging, p = 0.318 (Table 1). We further divided the partial denervation into two subgroups (severe and slight) but there was no significant difference between these subgroups in subjective or objective recovery.
Clinical data of patients with isolated serratus palsy and initial EMG examination.

EMG: electromyographic examination; SD: standard deviation.
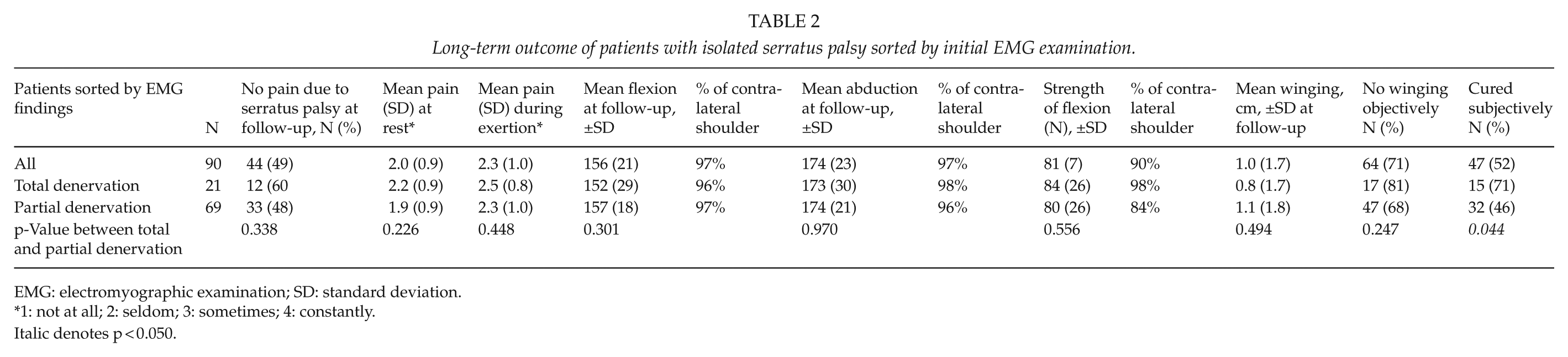
Mean duration of palsy as reported by 42 patients who considered themselves cured was 15.1 (range 3–30, SD 7.1) months, for the total denervation group 15.9 (range 3–20, SD 7.0) months, and for partial denervation 14.7 (range 3–30, SD 7.0) months, p = 0.599 between the groups. Winging measured in 90° flexion after mean follow-up of 17.8 years averaged in total denervation 0.8 cm and in partial 1.1 cm, p = 0.494. Winging resolved in 17 patients (81%) in total denervation and in 47 (68%) in partial denervation (Table 2). In total denervation, flexion improved from 133° to 152° and abduction from 149° to 173°, and in partial from 138° to 157°, p = 0.301, and abduction from 153° to 174°, p = 0.970 (Table 2). Strength in flexion averaged 84 N in total denervation and 80 N in partial, p = 0.556. The only significant difference between the total and partial denervation groups appeared in subjective assessment; 71% of patients reported being cured subjectively in the total denervation group, but only 46% in those with partial denervation, p = 0.044.
Long-term outcome of patients with isolated serratus palsy sorted by initial EMG examination.
EMG: electromyographic examination; SD: standard deviation.
1: not at all; 2: seldom; 3: sometimes; 4: constantly.
Italic denotes p < 0.050.
Discussion
We had hypothesized that long-term outcome after EMG-verified partial thoracic long nerve injury is better than that of total nerve injury. Fardin et al. (13), after evaluation of 10 cases of isolated serratus palsy followed up for a mean 2 years until recovery or stabilization of the motor impairment, stated that EMG is an important prognostic aid in isolated serratus palsy. Our study appears to contradict the view that electrodiagnostic studies can predict functional outcome in long thoracic neuropathy. After interviewing 50 serratus palsy patients by telephone a mean 4 years after onset of symptoms, the Friedenberg group (14) reported in 2002 that analysis of their electrodiagnostic data failed to identify in nerve conduction studies or needle EMG variables that could predict clinical outcome. They found that absent motor unit potentials or dense fibrillation potentials after 3 months did not correlate with clinical outcome. Nor, after evaluating their 64 serratus palsy patients, did Klebe at al. (16) find any prognostic gains. We cannot explain why, in subjective assessment, total denervation patients were healed subjectively better than did those with partial denervation. Subjective recovery may be strongly based on psychological factors. The total denervation patients may have had even worse situation in the beginning and compare to that while partial denervation patients compare recovery to different base line situation. All-over, subjective recovery was reported more seldom than objective, because those patients without objective scapular winging still might experience somewhat pain, discomfort, and weakness around the shoulder area. We acknowledge limitations in our study. Electrodiagnostic techniques for diagnosing serratus palsy were rather limited in the 80s, although clinical neurophysiology, especially including teaching of EMG, was already in 1966 a main specialty in our country.
In four cases, EMG was first carried out between 12 and 17 months after symptom onset (two total and two partial palsy). We, however, believe that this time-lag did not affect results, because recovery from serratus palsy normally takes more than 1 year. Concerning evaluation, we obtained no validated functional scores at the time that most patients initially were seen or at follow-ups, because no suitable valid score for serratus palsy presently exists. We therefore used a self-made scoring system. We consider that in evaluation of serratus palsy, the most important factors are scapular winging, shoulder ROM, strength in flexion, and pain. We found no discussion in the literature concerning these matters applied to serratus palsy.
We conclude that initial EMG does not predict clinical outcomes: ROM, pain, scapular winging and strength, but partial denervation may negatively predict subjective outcome. Thus, initial EMG does not play any role when considering optimal treatment for isolated serratus palsy.
Footnotes
Acknowledgements
The authors thank Carol Norris PhD, University of Helsinki, for language revision.
Ethical Approval
Each author certifies that his or her institution approved the human protocol for his investigation that all investigations were concluded in conformity with ethical principles of research, and that informed consent for participation in the study was obtained. This work was performed at ORTON Research Institute, Invalid Foundation, Helsinki, Finland.
Funding
The institution of the authors has received, during the study period, funding from EVO, HUS (government grant from Helsinki University Hospital District).