
Abstract
Background:
Kick scooters are popular among children in both transportation and recreational activities. The aim of this retrospective study was to assess the incidence of and injury patterns associated with kick scooter accidents in school-aged children and adolescents.
Methods:
All 171 patients at the age of 7–15 years who were treated for kick scooter–related injuries in the metropolitan Helsinki area, Southern Finland from January 2008 to December 2013 were included. Electronic medical records were reviewed and Pediatric Trauma Scores and Injury Severity Scores were utilized to assess the injuries.
Results:
The annual number of patients increased from 7 in 2008 to 55 in 2013. Almost all patients (94%, n = 161) were injured after a fall from their own height. Most patients (n = 118; 69%) were diagnosed with a fracture but only 26 patients (15%) required surgical procedures under general anesthesia. Pediatric Trauma Scores were low and only one patient had an Injury Severity Score > 15 which can be considered major trauma.
Conclusion:
Most injuries acquired from kick scooter injuries were easily treatable fractures and bruises. Considering the background population of 105,000 in the respective age group and the 6-year period of data collection from tertiary care, scooting seems a safe means of increasing the physical activity levels of school-aged children and adolescents.
Introduction
Unintentional injuries are the leading cause of mortality and a significant cause of morbidity in children in the Western world. The most common causes of injuries in children are related to transportation, falling, suffocation, poisoning, and burns (1). Throughout the World Health Organization (WHO) European Region, road traffic accidents are the leading cause of fatal injuries, traumatic brain injuries, and also limb injuries in children (2). The WHO recommends the enhancement of both the quality and quantity of data on morbidity and outcomes of children’s injuries for targeted investments in injury prevention (2).
Non-motorized kick scooters have increased in popularity in Finland during the last two decades. The most common type of kick scooter in Finland comprises a narrow metal board as a standing platform with two small polyurethane wheels, a back-wheel brake, and a 450- to 600-mm-high adjustable metal handlebar. The handlebar can be folded against the board during transport. Older children often use a sturdier, non-adjustable version that can bear the stress of jumping and other tricks.
Research on kick scooter injuries is derived mostly from single-center studies with short data collection periods (3–5). Little attention has been paid to the developmental stage of children and adolescents, although this may impact motor coordination skills as well as risk-taking behavior. A kick scooter that is equipped with a handlebar is easier to control than a skateboard or rollerblades. Consequently, kick scooter injuries often involve younger children than skateboards or rollerblades (3). Younger children with less developed motor coordination skills may acquire injuries that are quite different to those of school-aged children and adolescents, but this difference has been overlooked. Also, none of the studies utilized trauma scores to measure injury severity.
The aim of this study was to describe the epidemiology of injuries from kick scooter accidents and associated injury patterns among 7- to 15-year-old patients who were treated in the hospitals of the metropolitan Helsinki area. We hypothesized that adolescents (age 11–15 years) would have more serious injuries than younger children (age 7–10).
Material and Methods
Study Centers and Background Population
Helsinki Children’s Hospital is the only pediatric hospital in the metropolitan Helsinki area and it has the only children’s Intensive Care Unit in the province of Uusimaa. Töölö Trauma Hospital is the largest trauma center in Finland and provides treatment of severe trauma, and until 2015, also children’s neurosurgical care. Jorvi Hospital in Espoo is the primary provider of specialist care for children from Espoo, Vantaa, and Kirkkonummi. Together, these three hospitals are responsible for the provision of pediatric tertiary care for children from six cities or towns (Helsinki, Espoo, Vantaa, Kirkkonummi, Kerava, and Kauniainen). The size of the background population of children and adolescents aged 7–15 years within these six cities or towns was 105,000 with very little annual variation (6).
Patient Population and Clinical Data
We conducted a retrospective review of patient records of all children and adolescents aged 7–15 years who were treated for trauma at the Helsinki Children’s Hospital, Töölö Trauma Hospital, and Jorvi Hospital between January 2008 and December 2013. Since no International Statistical Classification of Diseases (ICD)-10 code exists for kick scooter injuries, emergency department registration lists of trauma patients within the desired age range (7–15 years) were manually screened to include only those injured in kick scooter accidents. To enable the calculation of incidence rates, patients who lived outside the six cities and towns of the primary catchment area were excluded. The final study population comprised 171 patients who presented with kick scooter–related injuries.
We collected the following data (when available): age, gender, possible use of drugs and alcohol, and the use of protective gear. Accident data collected included the mechanism of injury, place of accident, possible counterpart data, diagnoses, the Pediatric Trauma Score (PTS), and the Injury Severity Score (ISS). We also gathered clinical data on the duration of in-patient care, operations, and the number of out-patient clinic visits.
Trauma Scores
The PTS predicts morbidity, mortality, and the length of the hospital stay (7). The PTS can be used either by paramedics at the scene of the accident or the trauma team in the hospital. The PTS takes into account the child’s weight, airway status, systolic blood pressure, Glasgow Coma Scale (GCS), and obvious fractures and wounds. The PTS ranges from −6 to +12, and PTS < 8 predicts a mortality rate of 9% and PTS ⩽ 0 is associated with a mortality rate of 100%.
The ISS is currently the most commonly used trauma score which correlates with mortality, morbidity, and length of stay in the hospital. The ISS takes into consideration the precise definitive injuries found upon clinical evaluation, CT or magnetic resonance imaging (MRI) imaging, or during operations (8). The ISS ranges from 0 to 75 and ISS > 15 is considered major trauma. Since the ISS overlooks hemodynamics, GCS, and airway problems, we used both the PTS and ISS in this study.
Statistics
We used percentages and means (with standard deviations) and, if the data were skewed, medians (with ranges) to describe the findings. Dichotomous variables were compared between age groups using Fischer’s exact test and the Mann–Whitney U test was used for continuous variables. For calculation of annual incidence rates, population data from Statistics Finland (6) were used to determine the population at risk. Annual incidence rates were then derived as the annual number of patients per the respective year’s population size.
Results
Altogether, 171 children and adolescents were treated at the study centers due to injuries acquired from kick scooter accidents during the 6-year study period. The annual number of patients increased from 7 in 2009 to 55 in 2013 (Fig. 1). Annual incidence of kick scooter injuries increased from 0.07 per 1000 to 0.52 per 1000 7- to 15-year-olds in the study area during the study period (p < 0.001; Fig. 2). Most patients (n = 134; 78%) were boys, and 48% (n = 82) of patients were between 9 and 12 years old (Fig. 3).
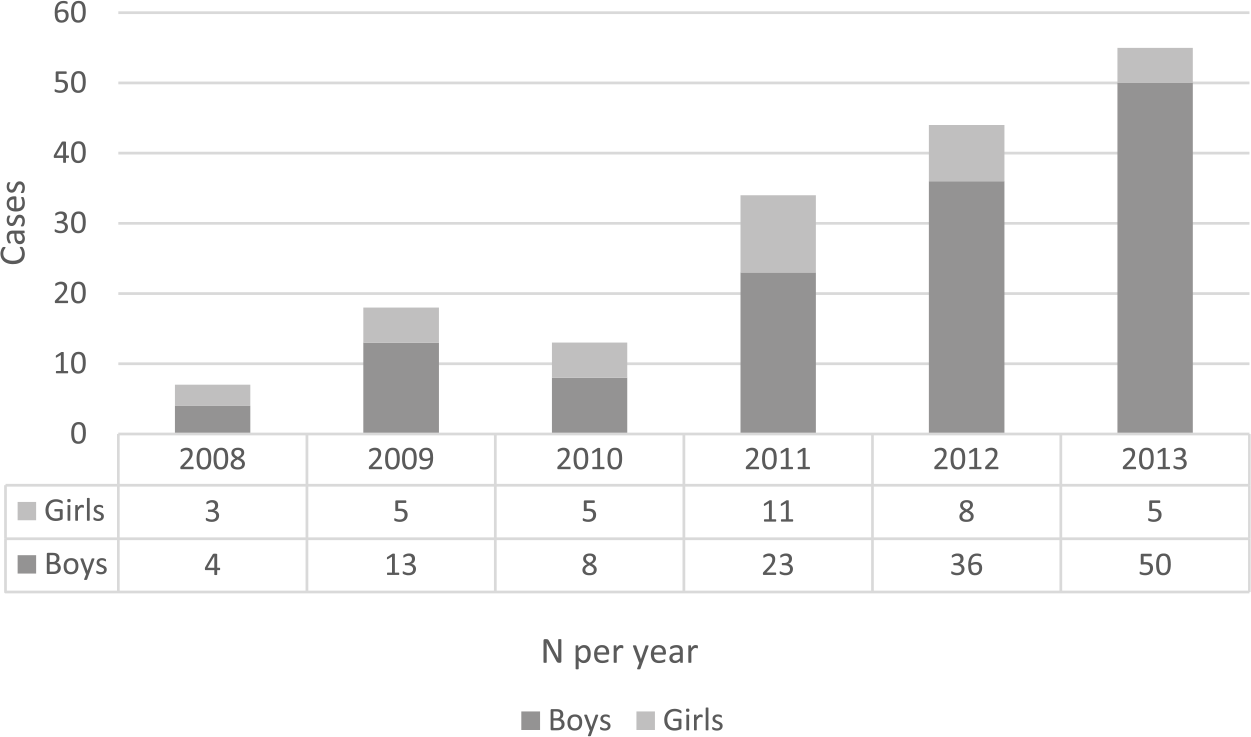
Annual number of patients admitted for injuries from kick scooter accidents.
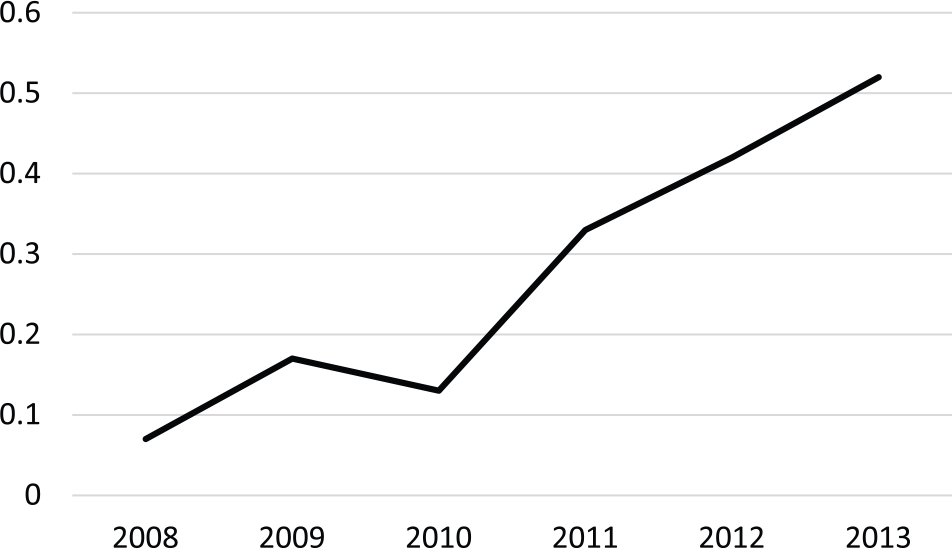
Annual incidence of kick scooter injuries per 1000 7- to 15-year-olds in the study area.
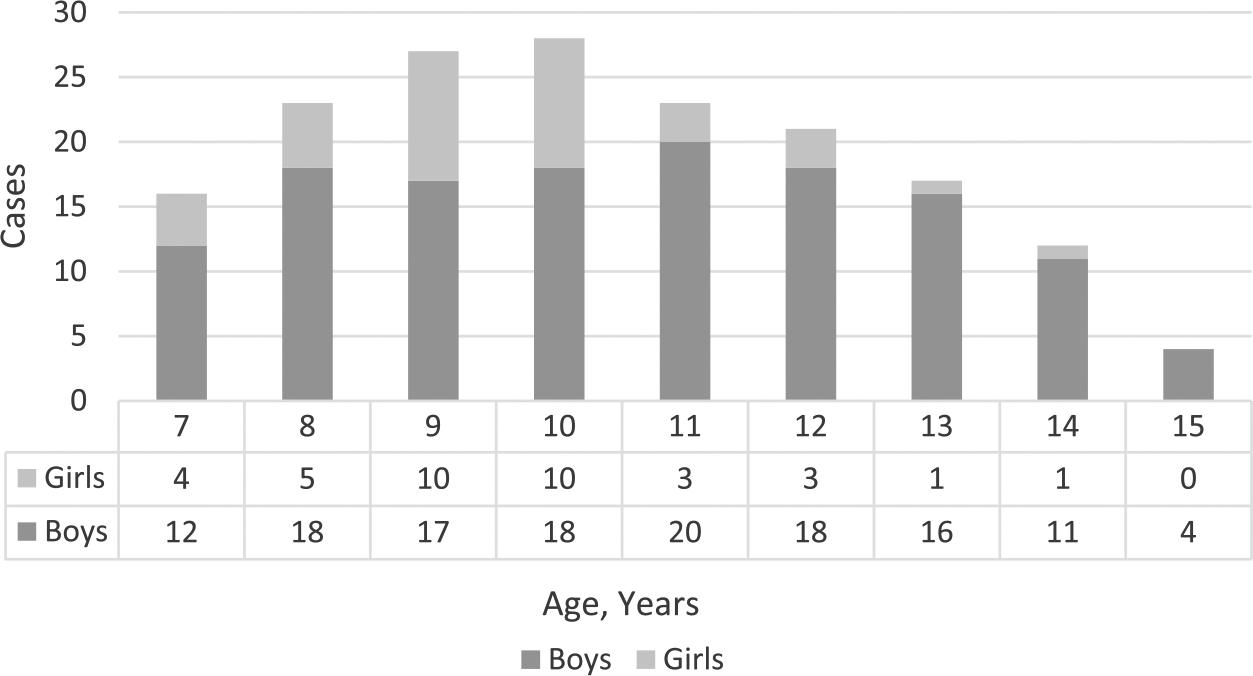
Age distribution of 171 patients injured in kick scooter accidents.
The most common mechanism of injury was falling down (n = 161; 94%). Nine patients were injured in collisions (counterparts: car (n = 3), solid object (n = 3), another scooter (n = 2), bicycle (n = 1)) and one after falling from a height of 1.5 m. The site of the accident was reported in only 13% of cases (n = 23) and the most common site was on the road going downhill.
Injury Types
The most common injury was a fracture or dislocation of the upper extremity (53%; Table 1).
Trauma of 171 patients injured in kick scooter accidents.
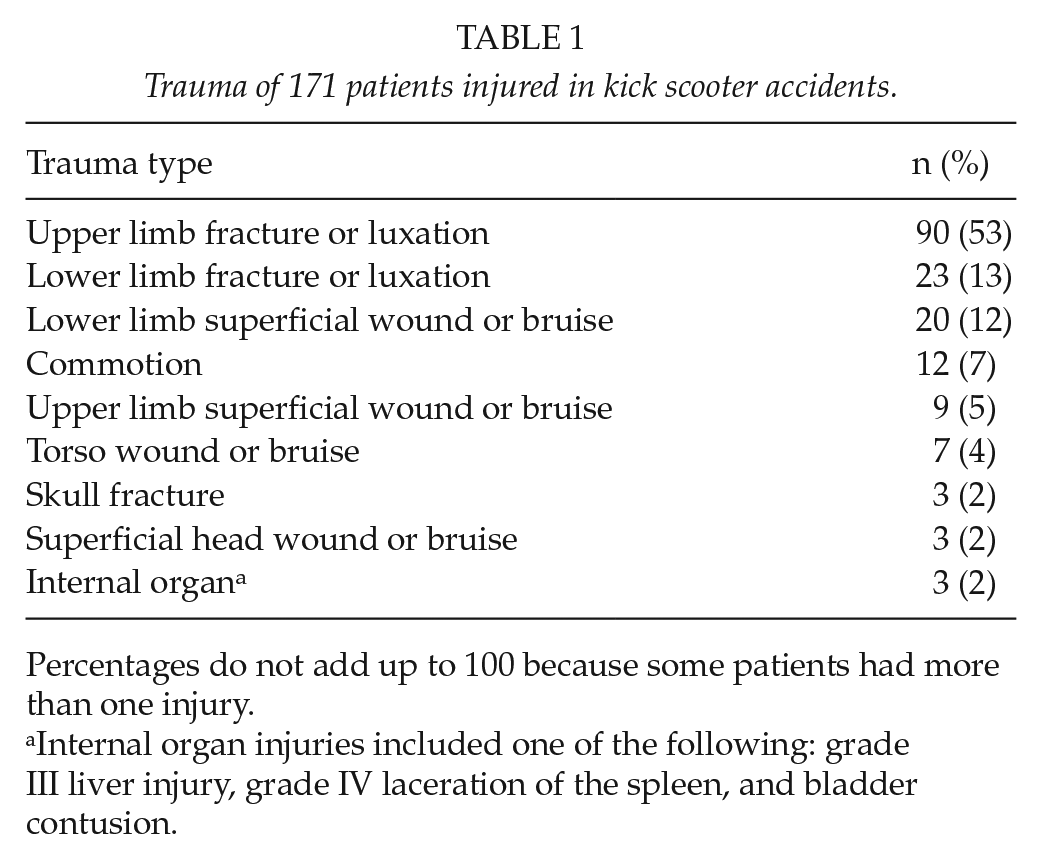
Percentages do not add up to 100 because some patients had more than one injury.
Internal organ injuries included one of the following: grade III liver injury, grade IV laceration of the spleen, and bladder contusion.
The second most common injury was a fracture of the lower extremity (13%). Internal injuries were found in three patients (one each: grade III liver injury, grade IV laceration of the spleen, and bladder contusion) and severe head injuries in three patients, two of which were fractures of the skull and one open mandibular fracture. In total, 12 patients were treated for a concussion. None of the patients had spinal injuries or intracranial bleeding.
The most common upper limb injury was a distal (metaphysis or more distal) fracture of the radius, ulna, or both (n = 52), followed by fractures of the carpal bones (n = 22). The most common lower limb injury was an ankle fracture (tibial, fibular metaphyseal, or more distal; n = 12), followed by fractures of the metaphysis of the tibia (n = 5) and tarsal bones (n = 5).
Helmet use was reported in 13% (n = 23) of patient records; six patients had been wearing a helmet, while 17 had been scooting without one. Of the 15 patients who sustained head injuries, one commotion patient had been wearing a helmet, while 11 patients had no helmet and information on helmet use was missing in three cases. The use of other protective gear was not mentioned in any patient files.
Trauma Scores
In total, 22 patients (13%) received a PTS < 11 but none had a PTS < 8 points. The most common ISS was 4 (in 85 patients, 50%; Fig. 4). Five patients (ages 9–11 years) had an ISS of 9. Their most prominent trauma included a base of the skull fracture, an orbital fracture, a mandibular fracture, a grade III liver injury, and an open wrist fracture. The ISS was >15 in one patient (ISS 16; age 12) who fell down, got hit in the stomach by the handlebar, and was diagnosed with a grade IV laceration of the spleen.
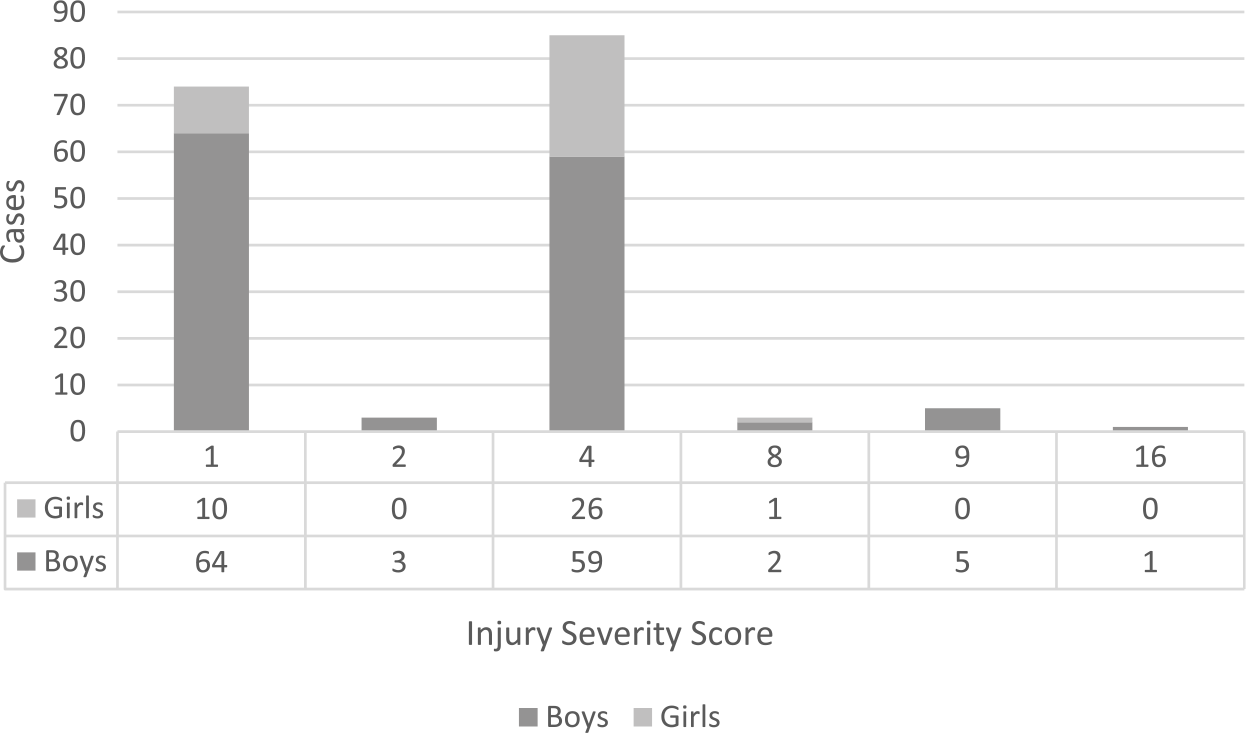
Injury severity scores of 171 patients injured in kick scooter accidents.
Treatment of Injuries
The majority of the patients (n = 138; 81%) spent less than 24 h in the hospital. Most of the injuries were treated at the emergency department with the help of local anesthesia and oral pain medication (paracetamol, ibuprofen, tramadol). A total of 26 patients (15.2 %) required procedures under general anesthesia (Table 2). Most of these injuries were fractures although one patient had a wound that required debridement and closure in the operation theater. More than half of the patients (n = 103; 60%) had at least one visit (median 1, range 0–6) to the out-patient clinic. Most of these out-patient clinic visits were fracture related.
Procedures conducted under general anesthesia (N = 26).
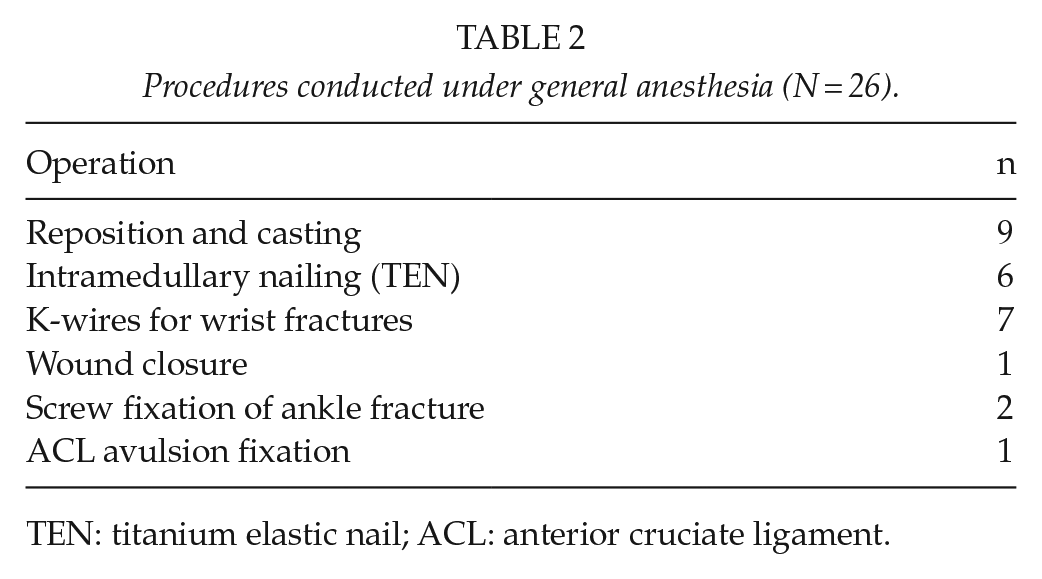
TEN: titanium elastic nail; ACL: anterior cruciate ligament.
Adolescents (age 11–15) were more often diagnosed with fractures in the lower extremity than younger children (age 7–10) but overall severity of injuries was similar in these age groups (Table 3).
Injuries, operations, and Pediatric Trauma Scores according to patient age.
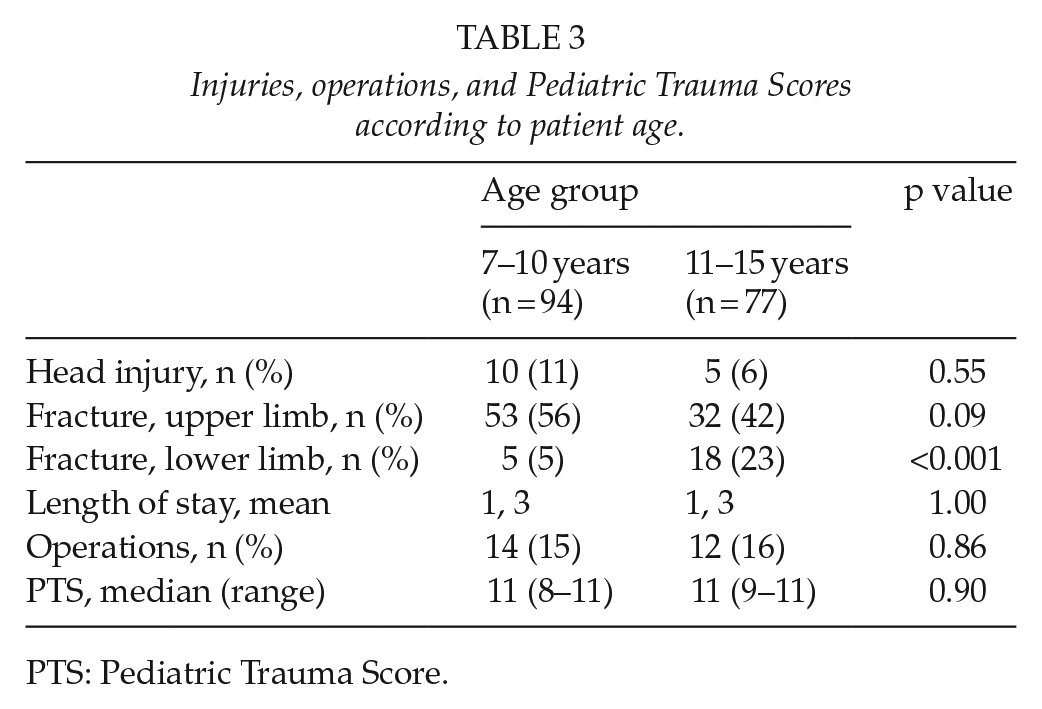
PTS: Pediatric Trauma Score.
Discussion
In this retrospective study spanning 6 years, kick scooter injuries in children were mainly minor fractures and bruises but increased significantly during the study period. In total, 15% (n = 26) of the patients required a procedure under general anesthesia to treat their injuries and 59 out-patient visits were undertaken to ascertain proper healing of the injuries. The PTS and ISS confirmed that the patients were in good overall condition upon arrival at the hospital, but six patients (4%) had fairly severe injuries according to an objective rating score (ISS).
The main strength of our study is the inclusion of all kick scooter patients treated in hospital settings during a 6-year period in a population-based sample of children and adolescents of the metropolitan Helsinki area. In Finland, all pediatric patients requiring ambulance transportation are brought to public hospitals. Primary healthcare treats minor injuries but in the study area virtually all children’s fractures are diagnosed and treated at hospitals. The private sector may have treated some children with minor injuries. Our experience has shown, however, that the numbers of children and adolescents treated in the private sector for recreational injuries (except licensed sports, such as football) are relatively low. Thus, the study population can be considered representative of the most serious injuries. Another strength is that all medical records were meticulously reviewed to include also follow-up data on out-patient visits. Our data are limited by their retrospective nature, resulting in missing data, for example, regarding the use of protective gear.
Skateboard parks have become increasingly popular in Finland in recent years and kick scooters are a frequent sight in these parks. Unfortunately, data on the location of the accident leading to injury were only available for 13% (n = 23) of our patients. None of these data specified whether the injury happened in a skate park. Children and adolescents often conduct high-speed, demanding tricks in park settings, but based on our data we are unable to comment on the safety of these parks from the perspective of kick scooter riders.
In line with other studies and reports, most patients in our study were males (3–5, 9). Among our patient population, the most common site of injury was the upper limb which is consistent with the most commonly reported injury mechanism, involving a fall and a protective reaction using the upper extremity (3–5, 10). The handlebar of a kick scooter rarely causes internal injuries similar to cycling injuries and our patient population included only one such case. Possibly due to the longer study period and older age distribution of patients in this study than in previous studies, however, our study population also included six patients with more serious injuries. Even deaths have been reported to the United States Consumer Product Safety Commission (11) but they should be weighed against the length of the data collection period and large background population of the country before restricting the use of kick scooters.
In general, head injuries are the major injury causing long-term morbidity and mortality. Consequently, we also hoped to provide information on the protective effect of helmets. Unfortunately, data on helmet use were only available for 23 patients and data had been recorded more often for patients who sustained head injuries than for others (data missing for only 3/15 patients with head injuries). Only one of the patients diagnosed with a head injury had been wearing a helmet. Still, too much data are missing to draw any robust conclusions.
Although unintentional injuries pose the greatest immediate threat to the health of children and adolescents, these should be weighed against the rising rates of childhood obesity. In time, obesity will cause significant health problems and unsustainable increases to the costs of healthcare (1). In search of effective prevention, the possible risks of new innovative activities should be evaluated against their possible benefits. Riding a kick scooter is one good option for developing children’s motor skills and for increasing their physical activity levels. Based on the findings of this study and the results of previous research, despite the possible injuries associated with riding a kick scooter, we believe that the benefits by far outweigh the risks of this activity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.