
Abstract
Objective:
To compare early and late results of open and endovascular management of popliteal artery aneurysm in a retrospective single-center matched case-control study
Methods:
From 1981 to 2015, 309 consecutive interventions for popliteal artery aneurysm were performed in our institution, in 59 cases with endovascular repair and in 250 cases with open repair. Endovascular repair was preferred in older asymptomatic patients, while open repair was offered more frequently to patients with a thrombosed popliteal artery aneurysm and a poor run-off status. A one-to-one coarsened exact matching on the basis of the baseline demographic, clinical, and anatomical covariates significantly different between the two treatment options was performed and two equivalent groups of 56 endovascular repairs and open repairs were generated. The two groups were compared in terms of perioperative results with χ2 test and of follow-up outcomes with the Kaplan–Meier curves and log-rank test.
Results:
There were no differences between the two groups in terms of perioperative outcomes. Median duration of follow-up was 38 months. Five-year survival rates were 94% in endovascular repair group and 89.5% in open repair group (p = 0.4, log-rank 0.6). Primary patency rates at 1, 3, and 5 years were 81%, 78%, and 72% in endovascular repair group and 82.5%, 80%, and 64% in open repair group (p = 0.8, log-rank 0.01). Freedom from reintervention at 5 years was 65.5% in endovascular repair group and 76% in open repair group (p = 0.2, log-rank 1.2). Secondary patency at 1, 3, and 5 years was 94%, 86%, and 74% in endovascular repair group, and 94%, 89%, and 71% in open repair group, respectively (p = 0.9, log-rank 0.01). The rates of limb preservation at 5 years were 94% in endovascular repair group and 86.4% in open repair group (p = 0.3, log-rank 0.8).
Conclusion:
Open repair and endovascular repair of popliteal artery aneurysms provided in this retrospective single-center experience similar perioperative and follow-up results in equivalent groups of patients.
Introduction
Endovascular treatment represents a promising and fascinating alternative to open surgery in the management of popliteal artery aneurysms (PAAs), providing, with a mini-invasive approach, excellent perioperative results, and satisfactory mid-term outcomes in selected patients (1–4). There are however few prospective studies in the literature directly comparing traditional open repair (OR) to the endovascular approach (5, 6), and in the most recent meta-analysis, the advantage of endovascular repair (ER) was limited to less wound complications and a shorter hospital stay in comparison with open surgery, which however had better primary patency rates in the mid-term period (7). Moreover, the majority of retrospective multi-center and single-center experiences are flawed by selection bias, due to different clinical and anatomical indications for each technique (2, 8, 9). Having in mind such issues and questions, with the present study, we aimed at retrospectively comparing perioperative and follow-up results of open and endovascular treatment of PAAs in equivalent populations.
Materials and Methods
Patient Population, Preoperative Workup, and Indications for Surgery
From January 1981 to December 2015, 309 consecutive interventions for PAA were performed at our Institution. Data concerning such interventions were prospectively collected in a dedicated database, whose characteristics have already been reported (8), including anatomical, clinical, diagnostic, and technical variables, perioperative (<30 days) results in terms of mortality and morbidity, and all relevant clinical and diagnostic data collected during follow-up.
A retrospective analysis of such database was performed and 59 interventions carried on with ER were found, while the remaining 250 interventions were OR. Informed consent for the treatment of personal data was acquired for each patient for insertion into the registry, but the retrospective analysis of the data did not require approval by the Institutional Review Board.
All patients underwent duplex examination and angio computed tomography (CT) scan or digital subtraction angiography (DSA) before surgery. Our indication for treating asymptomatic aneurysm was a diameter greater than 20 mm. In symptomatic patients, indication for surgery was unrelated to aneurysms’ diameter.
At the beginning of our experience, our indications for ER were the presence of a focal PAA, limited to popliteal fossa, with diameters of vessels compatible with commercially available stent grafts, and at least two patent tibial vessels.
In the following years, we adopted more liberal indications, and nowadays, we evaluate for endovascular feasibility also longer lesions, involving the entire popliteal artery from the adductor tendon to the popliteal bifurcation, provided that a proximal and distal landing zone of at least 2 cm length is present, with the patency of at least one tibial vessel.
Intraoperative Strategy
Open surgical technique was chosen on a single-patient basis; a posterior approach was preferred in short aneurysms, limited to the popliteal space, whereas we used a medial approach in patients with lesions extending above and below the knee. Several types of arterial reconstruction were used, on the basis of the characteristics of the aneurysm and of the status of inflow and outflow vessels; also the details of such reconstructions have been already described in our previous papers (10).
The choice of the graft was made on the basis of the anatomic status, too; usually, we used a prosthetic graft in patients with aneurysms not involving the distal vessels and with a good run-off status or when a good quality ipsilateral saphenous vein was lacking. A vein bypass was preferred in patients with long lesions, extending well below the knee, or with a concomitant distal occlusive disease.
All the patients had intraoperative administration of intravenous sodium heparin (30 IU/kg) at arterial clamping; completion control was routinely performed, in most cases with angiography, while in patients with contraindication to contrast medium administration, a completion duplex ultrasound scanning was performed. Postoperative medical treatment consisted mainly in single or double antiplatelet treatment; in selected patients, oral anticoagulants were used.
Endovascular intervention was performed in the operating room in the first years of experience and then in the angiographic suite, under local anesthesia; an ipsilateral open surgical approach with a mini-incision on the groin or a percutaneous puncture was used to gain access to the superficial femoral artery. All the patients had intravenous administration of 5000 IU of sodium heparin at the beginning of the procedure. Covered stents to exclude aneurysmal sac from blood flow and to maintain a direct flow to the foot were placed in all the cases. Endografts were oversized 10%–15% relative to the landing zones. When more than one endograft was required for exclusion, overlap of at least 2 cm to prevent a type III endoleak from component separation was used. Overlapping endografts differed by not more than 2 mm in diameter. In the presence of incomplete proximal sealing of endograft at completion angiography, adjunctive ballooning and, when necessary, stenting were performed. Postoperative and long-term medical treatment consisted of double antiplatelet therapy in all the cases.
Management in Patients with Acute Ischemia
In selected patients with mild-to-moderate ischemia (grade I or IIa according to Rutherford’s classification of acute ischemia) due to acute aneurysms’ thrombosis, preoperative catheter-directed thrombolysis with urokinase (Urochinasi Crinos; Crinos SPA, Milan, Italy) was performed.
Thrombolytic treatment was administered in a bolus of 100.000 IU, followed by continuous infusion with a delivery rate of 70.000 IU/h. In all the patients, 1.000–1.500 IU/h of sodium heparin were administered via the same catheter to maintain values of activated partial thromboplastin time (aPTT) two times higher than normal value.
Angiographic controls were performed daily or more, when necessary, and lytic infusion lasted until patency of popliteal and tibial vessels was achieved or for a maximum of 3 days when unsuccessful. Thrombolysis was defined successful in the presence of restored patency of popliteal artery and at least one tibial vessel. Surgical or endovascular intervention was performed within 24 h from the cessation of administration of thrombolytic treatment. In the case of unsuccessful thrombolysis, a prompt open surgical attempt was performed.
Follow-Up
Follow-up was performed at 1, 6, and 12 months and yearly thereafter with a clinical examination and a duplex ultrasound scan (DUS). All the follow-up visits were performed by a vascular surgeon; the patients were asked to report their clinical history during the indexed period, with particular interest paid to the occurrence of significant clinical events at the indexed limb and their time of appearance, and of major cardiovascular events. DUS studies were performed by the same surgeon, using an Acuson Sequoia 512 Ultrasound System (Acuson Corporation, Mountain View, CA, USA). The patency of the graft, the status of anastomoses, of the inflow and outflow vessels and of the contralateral femoro-popliteal axis were assessed. In patients undergone endovascular treatment, also the exclusion of aneurysmal sac from the blood flow was examined. The analysis of follow-up results was stopped at December 2016.
Definition of the Outcomes
Primary patency was defined as uninterrupted patency without procedures performed on or at the margin of the treated segment, whereas secondary patency was defined as restored patency through the original treated segment. Freedom from amputation was defined as the avoidance of above or below-knee amputation, while freedom from reinterventions was defined as the avoidance of any open or endovascular new procedure on the treated artery.
Statistics
Interventions performed with ER were matched to those performed with OR on the basis of a one-to-one coarsened exact matching (CEM); for its calculation, all the significantly different baseline pretreatment demographic, clinical, and anatomical covariates in the two groups were used. A CEM-based matched control group was then generated. The two groups (ER group, 56 interventions; OR group, 56 interventions) were compared in terms of perioperative (<30 days) results of interventions (mortality, thrombosis, and amputation) with χ2 test and Fisher’s exact test, when necessary.
Follow-up data were analyzed with the Kaplan–Meier curves in terms of primary and secondary patency, freedom from reintervention, and limb preservations, and the results in the two groups were compared by means of log-rank test. The follow-up index (FUI) for late survival in the study group was assessed: it was defined as the ratio between the investigated follow-up period and the theoretically possible follow-up period up to December 2016. A univariate analysis to identify potential significant predictors of graft occlusion in the whole study group was performed with the Kaplan–Meier survival estimates and log-rank test for each covariate. Associations that yielded a p-value ≤0.2 on univariate screen were then included in a forward Cox regression analysis with measurement of hazard ratio (HR) and confidence interval (CI; significance criteria 0.25 for entry, 0.05 for removal).
Results
Demographic Data, Risk Factors, Comorbidities, Clinical, and Anatomical Status
Baseline characteristics of ER and OR patients in the original data set are reported in Table 1. In the same table, the characteristics of the two groups generated after CEM for the significantly differing baseline covariates between OR and ER patients are reported.
Baseline characteristics of ER and OR patients in the whole study group and in the two matched groups.
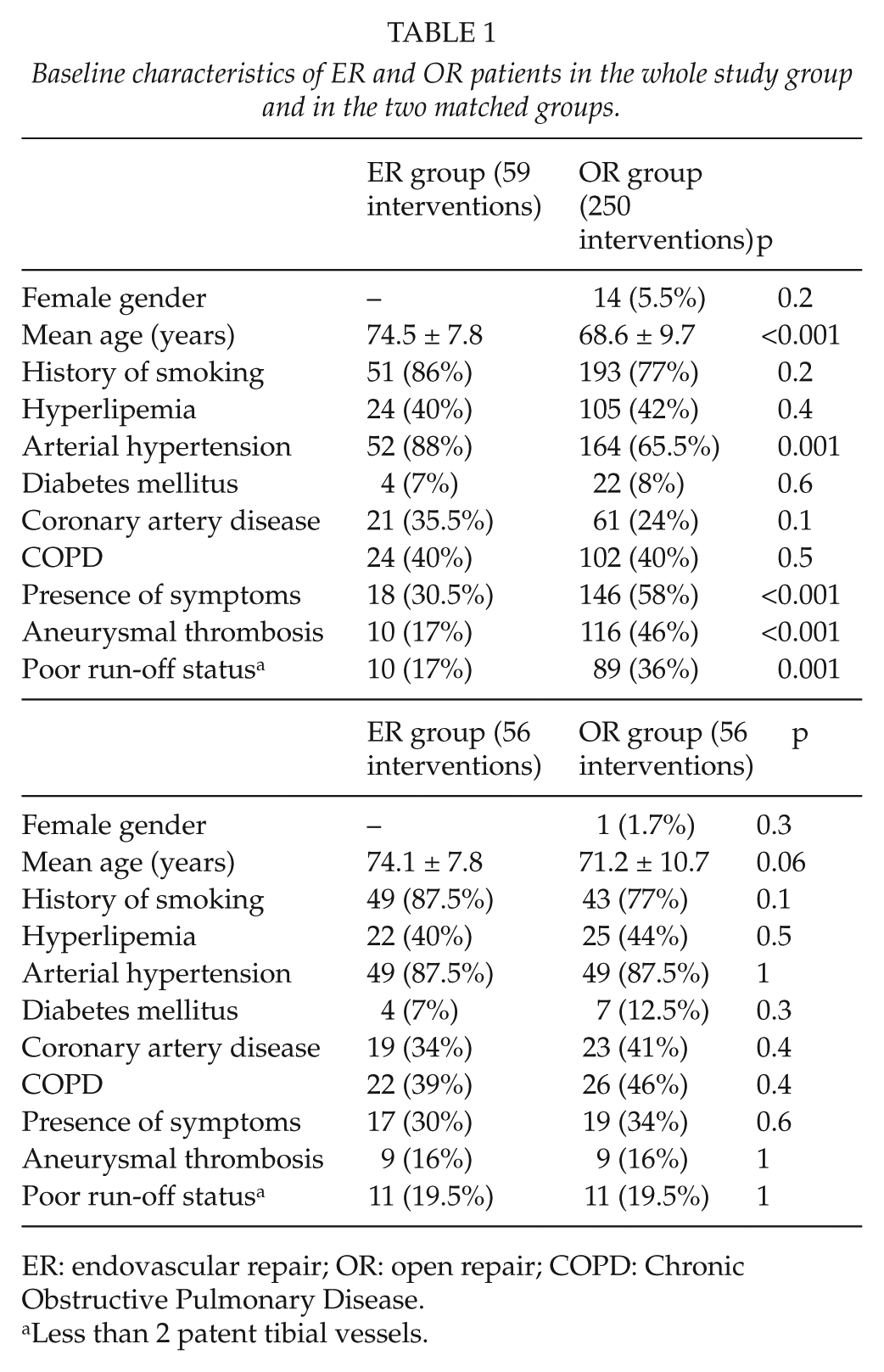
ER: endovascular repair; OR: open repair; COPD: Chronic Obstructive Pulmonary Disease.
Less than 2 patent tibial vessels.
Most patients were asymptomatic at the time of the intervention, with no differences between the two groups. In ER group, 17 patients (30%) were symptomatic, in three cases each for intermittent claudication, critical limb ischemia, and rupture and in eight cases for acute limb ischemia; in OR group 19 patients were symptomatic, in nine cases for intermittent claudication, in five cases for acute limb ischemia, in two cases for rupture, and in one case each for critical limb ischemia, compression, and distal embolization. The mean diameter of the treated aneurysm was 32.9 ± 12.7 mm in ER group and 32.5 ± 11.2 mm in OR group (p = 0.8).
Technical Details
In ER group, 55 patients had endoprosthesis placement (Hemobahn or Viabahn®; W.L. Gore & Associates Inc, Flagstaff, AZ, USA); in the remaining patient, a multilayer nitinol stent was used (Cardiatis Multilayer 3D Stent®; Cardiatis SA, Isnes, Belgium).
In 34 cases, ipsilateral surgical femoral approach was used, while 22 patients had ipsilateral percutaneous access. Inflow vessels were superficial femoral artery in 42 cases and proximal popliteal artery in 14 cases; the outflow vessel was in all but one case the below-knee popliteal artery, while in the remaining patient it was the tibioperoneal trunk.
The mean number of placed stents was 2 (range 1–5), with a mean length of 220 mm (range 100–350). One patient had concomitant aneurysmectomy and graft interposition of an ipsilateral common femoral artery aneurysm, while in one case percutaneous transluminal angioplasty (PTA) of the posterior and anterior tibial arteries was performed.
In OR group, 19 aneurysms were treated with aneurysmectomy and graft interposition, while in 9 cases the aneurysm was opened and a graft was placed inside the aneurysm in fashion similar to that used to repair aortic aneurysms; one patient had aneurysmectomy with end-to-end anastomosis of popliteal artery. In 27 cases, proximal and distal ligation of the aneurysm with bypass grafting was carried out.
A medial approach was used in 35 cases (62.5%) and a posterior approach was used in 21 patients (27.5%). A prosthetic graft was used in 49 cases, while in 6 limbs ipsilateral autologous saphenous vein was the material for revascularization. Saphenous vein was used in two patients who had proximal and distal ligation of the aneurysm with bypass grafting and in four patients who had aneurysmectomy or endoaneurysmectomy and graft interposition. In patients who had a prosthetic graft, expanded polytetrafluoroethylene (ePTFE) was used in all the cases and it was placed in 24 patients who undergone proximal and distal ligation of the aneurysm with bypass grafting and in 24 patients who had graft interposition. As already mentioned, one patient had no graft insertion. In 34 interventions, the inflow vessels were the common or superficial femoral artery and in the remaining 22, it was the above-knee popliteal artery. The outflow vessel was in most cases the below-knee popliteal artery (48 cases, 86%), as in six cases it was the tibioperoneal trunk and in two cases a tibial vessel. Adjunctive procedures were performed in 15 cases: in 2 cases, they involved the run-in vessel (patching of the femoral bifurcation in one limb and ipsilateral iliac stenting in the remaining case), while in 13 cases they were at the distal anastomotic sites (patching of the anastomosis in 11 cases, tibial angioplasty in 2 cases). Two patients had a concomitant major vascular intervention: in one case, an OR of an abdominal aortic aneurysm (AAA) was performed, while one patient had an AAA endovascular exclusion.
Acute Ischemia
Eight patients with mild-to-moderate acute ischemia due to PAA thrombosis underwent preoperative intra-arterial thrombolysis, 5 in ER group 1 and 3 in OR group. The mean duration of thrombolytic treatment was similar in the two groups (36 and 42 h, respectively, p = 0.9). Thrombolysis was successful in all the patients of ER group and in one patient of OR group (p = 0.1). The remaining patients of OR group had complete recanalization of PAA but only partial recanalization of tibial vessels. No major complications occurred during thrombolysis in both groups.
The remaining three patients with acute ischemia in ER group underwent primary stenting of the thrombosed PAA (11), while in the two patients of OR group with acute ischemia proximal and distal ligature with bypass grafting and concomitant intraoperative thrombolytic distal perfusion was performed.
Perioperative Results
Technical success occurred in all the patients of ER group. There was one perioperative death in a patient of ER group, who had undergone PAA endografting for an asymptomatic 30 mm aneurysm and developed in the second postoperative day a fatal cerebral hemorrhage. Six perioperative thromboses occurred, two in ER group (3.5%) and four in OR group (7%; p = 0.4). In ER group, the two thromboses were successfully treated with thrombolysis, in one case with adjunctive distal stenting. In OR group, successful treatment with surgical thrombectomy (one case) and thrombolysis (one case) was achieved; in one patient, operated on for limb threatening ischemia due to PAA thrombosis, surgical reintervention was ineffective and above-the-knee amputation was unavoidable. In the remaining patient, thrombosis was asymptomatic and the patient refused any further reintervention. One patient in ER group required an adjunctive reintervention due to postoperative bleeding at the site of arterial catheterization and underwent surgical repair of common femoral artery lesion. Mean hospital stay was 3.2 ± 1.1 days in ER group and 5.7 ± 3.3 days in OR group (p < 0.001). Cumulative 30-day death and amputation rate was 1.7% in OR group (p = 0.3 in comparison with ER group), while the corresponding figures in terms of 30-day reintervention rate were 5.3% in both groups (three cases each, p = 0.6).
Follow-Up Results
Median duration of follow-up was 38 months (range 1–312); 108 patients (96.5%) had an available follow-up, while the remaining four patients did not complete the follow-up and were not reachable via telephone. The duration of follow-up was significantly longer in OR group (71.5 ± 10.4 months) than in ER group (36.4 ± 3.4 months; p < 0.001). The mean FUI in the whole study group was 0.63 ± 0.34, and it was similar between the two groups (0.61 ± 0.3 in OR group and 0.65 ± 0.29 in ER group, p = 0.08).
During follow-up, 11 deaths were recorded, 1 in ER group, due to acute myocardial infarction, and 10 in OR group. The cause of death among OR patients was cancer in three cases, stroke in one case, end-stage renal disease in one case, and car accident in one case; in the remaining four cases, the cause of death was unknown. Estimated 5-year survival rates were 94% (standard error, SE, 0.04) in ER group and 89.5% (SE 0.05) in OR group (p = 0.4, log-rank 0.6).
Twenty-two late thromboses occurred: 10 in ER group and 12 in OR group. Primary patency rates at 1, 3, and 5 years were 81% (SE 0.04), 78% (SE 0.06), and 72% (SE 0.08) in ER group and 82.5% (SE 0.04), 80% (SE 0.05), and 64% (SE 0.07) in OR group, respectively (p = 0.8, log-rank 0.01). In ER group, all the late thromboses were treated with a reintervention, in seven cases with a new endovascular approach and in three cases with open surgery; in OR group, six patients had a redo open surgical repair, three patients were endovascularly treated whereas in the remaining patients the thrombosis led to mild-to-moderate intermittent claudication and the patients refused any other intervention. One patient in OR group underwent reintervention despite a patent bypass graft due to the occurrence of a distal anastomotic pseudoaneurysm, requiring surgical resection with graft interposition; one patient in ER group required an endovascular reintervention for a type II endoleak leading to sac enlargement. The details of late reinterventions are reported in Table 2. Freedom from reintervention at 5 years was 65.5% (SE 0.08) in ER group and 76% in OR group (SE 0.07, p = 0.2, log-rank 1.2; Fig. 1); the corresponding figures in terms of secondary patency at 1, 3, and 5 years were 94% (SE = 0.03), 86% (SE 0.05), and 74% (SE 0.08) in ER group, and 94% (SE 0.03), 89% (SE 0.05), and 71% (SE 0.08) in OR group, respectively (p = 0.9, log-rank 0.01). Four amputations were recorded, three in OR group and one in ER group, in all the cases following unsuccessful reintervention for graft thrombosis. The rates of limb preservation at 5 years were 94% (SE 0.07) in ER group and 86.4% (SE 0.08) in OR group (p = 0.3, log-rank 0.8).
Late reinterventions in the two groups.
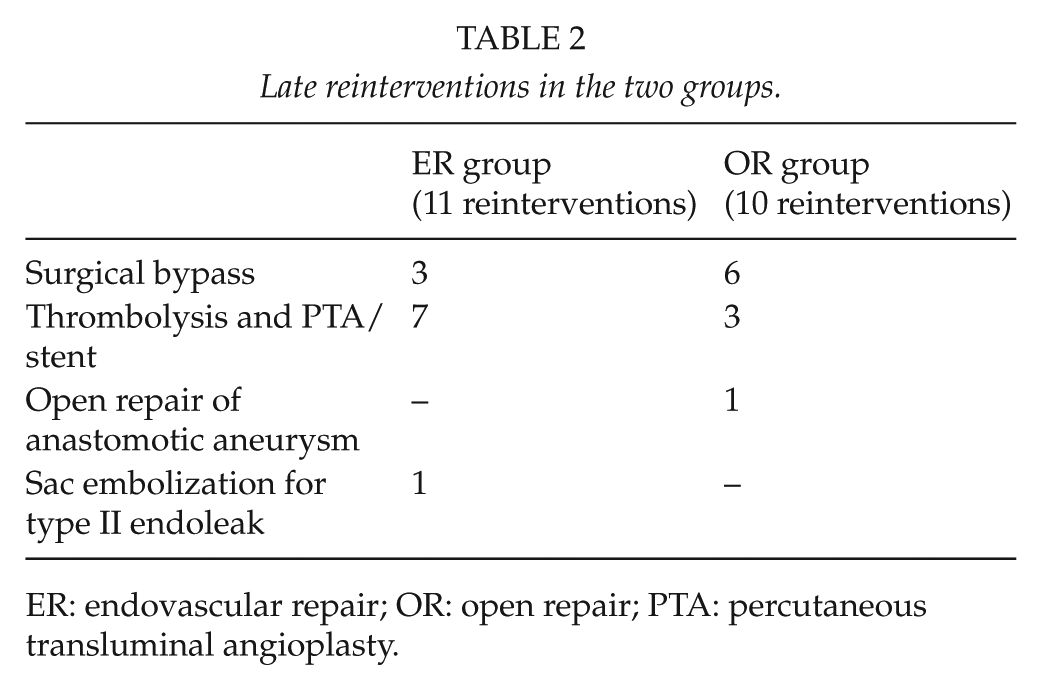
ER: endovascular repair; OR: open repair; PTA: percutaneous transluminal angioplasty.
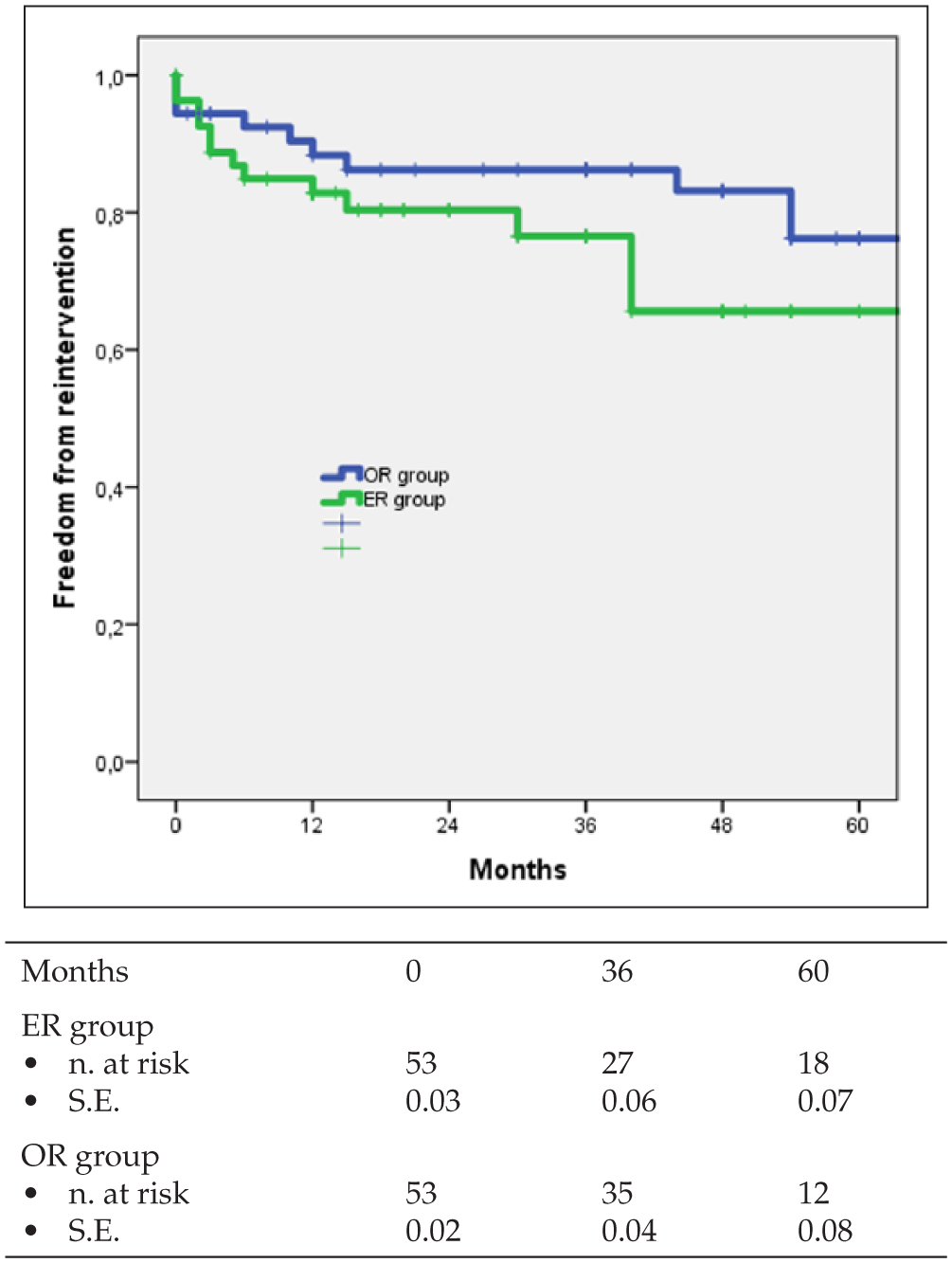
Kaplan–Meier curves for freedom from reintervention with number of patients at risk in both groups.
Univariate analysis for the risk of graft occlusion at 5 years in the whole study group is reported in Table 3. The presence of thrombosed PAA and of acute limb ischemia, diabetes, and the poor run-off status entered the multivariable analysis; only the latter factor was independently associated with that outcome (HR-3.9, 95% CI 1.3–11.3, p = 0.01).
Univariate analysis for factors affecting primary patency at 5 years in the whole study group.
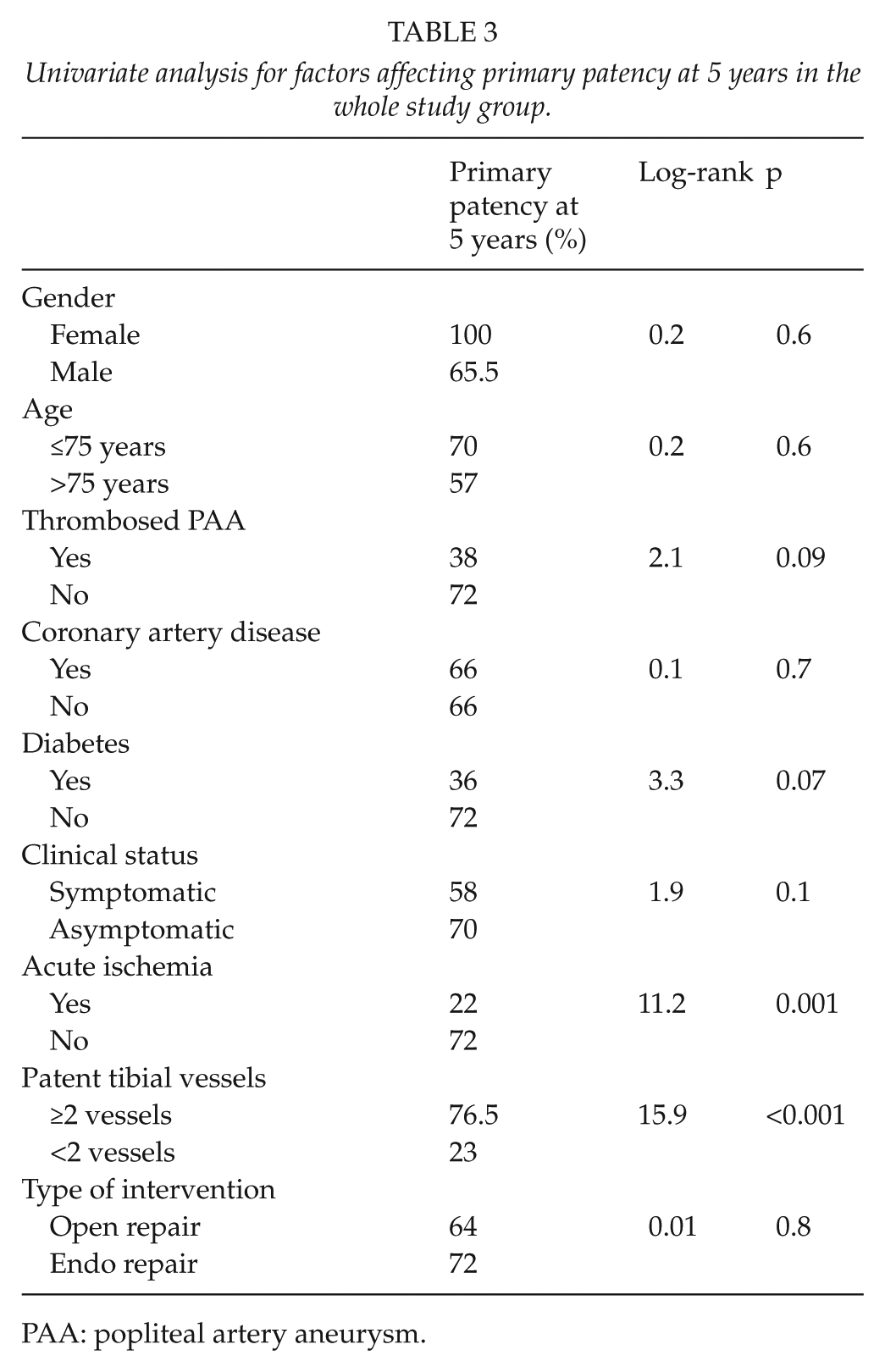
PAA: popliteal artery aneurysm.
Discussion
The efficacy of the surgical repair of PAA has been widely demonstrated in several reports (12, 13). Surgical intervention provides excellent results both in asymptomatic and in chronic symptomatic aneurysms, while also in acutely complicated lesions the possibility of preoperative thrombolysis allows in many cases to perform a successful elective intervention after the restoration of the patency of popliteal artery and tibial vessels, without compromising the results of surgery if unsuccessful (14, 15).
In spite of such excellent results, which are achieved in the everyday practice in the most experienced vascular centers, nowadays, with the worldwide diffusion of endovascular procedures, the endovascular approach to PAA has been gaining popularity and interest, due to the easy deployment of stent grafts and to the low invasiveness of the procedure. Many authors in recent years reported satisfactory early and mid-term results with the use of endografts in the exclusion of a PAA, even if few randomized studies comparing the two treatment options do exist and most single-center series include substantially different patients under clinical and anatomical point of view (1, 5, 6, 16). In the present study, we updated the results of our previous comparative series (8) by adding the data regarding the interventions performed in the years following its publication and we tried to make the comparison more reliable by adjusting for baseline confounding factors. In our practice, we were used to treating with endovascular means elderly patients with more severe cardiovascular comorbidities, but with less complex lesions under a clinical and anatomical point of view. This is a common finding in the literature; in the most recent meta-analysis (7), OR patients were younger and had a worse anatomical condition than their ER counterparts. Moreover, in the largest nonrandomized comparative series (2, 9), OR was preferred in symptomatic patients, with thrombosed PAAs and ischemic rest pain, while ER was usually performed in asymptomatic, uncomplicated lesions, with a good run-off status. Taking into account these differences on baseline characteristics, we performed a CEM so to have equivalent populations and to reduce the methodological flaws of the study. CEM methods specify how covariates differ across groups before matching, instead of merely taking those differences as a post-matching result as in a propensity score (17). After CEM, we were able to compare early and late outcomes of ER and OR of PAA in equivalent populations under clinical and anatomical point of view. One-third of the patients in both groups were symptomatic, and a large proportion of acute limb ischemia due to aneurysmal thrombosis or embolization was present in the two groups.
Perioperative results were excellent, with low rates of thrombosis and only one amputation; also the need for early reinterventions was limited to three patients for each group, perioperative thrombosis being the most common cause of early redo surgery. We did not find significant differences between the two groups in terms of perioperative complications, and this is an interesting finding, considering that main published series report a trend toward more frequent and severe local and systemic complications among patients operated on with OR (9). The only significant advantage for ER in perioperative outcomes was the halved length of stay in comparison with OR patients, as already reported by other studies (7). In acutely thrombosed PAAs, our aggressive policy of tibial salvage, with the use of intra-arterial thrombolysis in selected patients with moderate ischemia, maintained its effectiveness in approaching this potentially catastrophic complication; once the patency of popliteal artery and tibial vessels is restored, it is now possible to choose between open and ER on the basis of clinical and anatomical consideration; this was also our strategy, providing satisfactory perioperative outcomes. In three cases, we were able to treat acute PAA thrombosis with a primary stenting without a preliminary preoperative thrombolysis; this strategy can represent an effective option in favorable anatomical conditions (a suitable landing zone in the distal popliteal artery of ≥2 cm of length, and a diameter of ≥4 and ≤8 mm, with at least one vessel patent to the foot) after a successful attempt to cross the occlusion with a hydrophilic guidewire supported by an angiographic catheter. We recently reported (11) encouraging results with such a technique, which can represent an alternative solution to classical surgical approaches in selected patients with specific anatomical requirements.
Follow-up program was achieved in more than 95% of the patients, with a satisfactory FUI, approaching 65% in both groups. As expected, the follow-up duration was longer among OR patients, and this is a common finding in the literature (9), considering the relatively recent diffusion of endovascular techniques in comparison with open surgery; however, we were able to obtain reliable follow-up data up to five postoperative years. Long-term results were equally satisfactory in both groups, without significant differences between ER and OR. Primary patency rates well compared with the main published studies, both for open surgery and for endovascular techniques (2, 4). Interestingly, we did not find any significant advantage in favor of OR in terms of follow-up patency rates; even if this result is supported by other single-and multi-center studies and meta-analysis (2, 16, 18), a more recent systematic review (7) showed better primary patency rates at 1 and 3 years for OR in comparison with ER. Moreover, a large study from the Swedvasc Registry (19) recently reported 1-year better results for OR in comparison with ER, particularly in acute ischemia; however, the number of endovascular interventions in those studies was limited in comparison with open interventions, and the characteristics of the follow-up programs, along with its completeness, were not described in details, thus raising several doubts concerning the reliability of follow-up outcomes.
We found a trend toward a higher risk of reintervention during follow-up in ER patients, and this is relatively uncommon finding in the literature. Only Leake et al. (7) found in their recent meta-analysis that OR more frequently required reintervention than ER with a high statistical significance (OR 0.27, p < 0.001). This finding should probably be considered when planning an endovascular procedure; in our experience, however, most reintervention in both groups could be performed with endovascular means, and the results in terms of secondary patency were not significantly different at each time interval during follow-up. The need for multiple endovascular revisions is probably the price to be paid for having a mini-invasive approach, which offers undoubted advantages; the future technological developments may possibly allow a further significant improvement also in the long-term outcomes. On the other hand, the risk of developing an endoleak following ER is low in our experience, and probably, it does not represent the main complication of ER of PAAs.
In review of the entire cohort of patients, we attempted to identify predictors of graft failure during follow-up; the only predictor of loss of primary patency was a poor run-off status, similarly to what reported in previous studies (2, 9). This result further underlines the need for having as much patent tibial vessels as possible at the moment of the intervention, with the aggressive use of preoperative and intraoperative thrombolysis, particularly in the acute/urgent setting. We found a trend toward poorer outcomes in patients with acute limb ischemia and graft thrombosis, and one can suppose that with a larger number of patients and a longer follow-up duration, also those factors become significantly associated with loss of primary patency.
Following those results, in our daily practice nowadays, the endovascular approach represents our first line choice in patients at high surgical risk and with suitable anatomy; however, considering the excellent long-term results of open surgery and the large experience with such a technique, we are not pushed to attempt an endovascular approach no matter what, but we are able to choose the right strategy for that particular patient with its unique clinical and anatomical characteristics.
This study has several limits: it is a retrospective, nonrandomized study, with a limited number of patients and events. On the other hand, the exact matching allowed us to reduce the selection bias in the choice of treatment; moreover, the follow-up was accurate and robust, allowing to draw firm conclusions on long-term outcomes. Even if the most recent Cochrane Review (20) concludes that a randomized controlled trial (RCT) is necessary to define the true role of ER and OR in the treatment of PAA, such a study, in this relatively small group of patients with low event rate in the early and long-term period, is probably barely feasible in an achievable period of time; for this reason, a study like the present can contribute to add knowledge with a good level of evidence to the heretofore paucity of data in the contemporary literature.
Conclusion
OR and ER of complicated and uncomplicated PAAs provided in this retrospective single-center experience similar perioperative and follow-up results in equivalent groups of symptomatic and asymptomatic patients. There is a trend toward a higher risk of reintervention in ER patients, requiring further analysis and a longer follow-up time; however, most reinterventions can be successfully carried out with further endovascular procedures.
Footnotes
Declaration Of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.