
Abstract
Background and Aims:
Reduction mammoplasty alleviates macromastia symptoms and improves quality of life. We investigated a large series of consecutive reduction mammoplasties to assess various risk factors for both minor and major complications after the procedure.
Materials and Methods:
A retrospective analysis of 453 consecutive reduction mammoplasties was performed between 2007 and 2010 at an academic tertiary referral center to evaluate risk factors and complications.
Results:
The incidence of minor and major complications was 40.5% and 8.8%, respectively. Patients with minor complications had both a significantly higher mean body mass index (30.2 vs 28.0) and sternal notch to nipple distance (33.9 vs 32.4 cm) than patients who recovered without complications (p < 0.001 for both comparisons), as well as more visits to the outpatient clinic (p < 0.001). In the multivariate analysis, body mass index was found to be the only significant risk factor for minor complications (p < 0.001). Furthermore, patients with body mass index higher than 27 had a 2.6-fold greater risk of minor complications (p < 0.001). An increase of one unit in body mass index increased the probability of minor complications by 14.1% (p < 0.001). 22 (4.9%) patients developed a hematoma requiring evacuation in the operating room. The mean body mass index of patients who developed a hematoma was 26.4, a value lower than that of patients without this complication (mean 29.0; p = 0.003). This finding was significant also in the multivariate analysis (p = 0.002).
Conclusion:
A higher body mass index was strongly associated with an increased risk of minor complications after reduction mammoplasty. It is important to inform obese patients about the increased risk of complications and to encourage them to lose weight before surgery.
Introduction
The loss of health-related quality of life (HRQoL) associated with symptomatic breast hypertrophy is well documented (1–3). Reduction mammoplasty (RM) is commonly performed to both reduce breast weight and volume and reposition the breasts, which improves the HRQoL of the patient. Several randomized studies have demonstrated the effectiveness and cost-effectiveness of RM (1, 4, 5). The procedure is also reported to increase HRQoL regardless of the patient’s body mass index (BMI) (6).
Complications of RM vary from minor wound complications to more severe complications, such as systemic infections, hematomas, and other wound complications that require reoperation. Potential factors exposing patients to these complications have been studied, but the results are still somewhat incoherent (6–16). In particular, the association between increased BMI and postoperative complications is unclear. Several studies report an increased risk of complications in patients with a high BMI (6–14), whereas other studies report no such effect or only a weak association (15–19). Gust et al. (13) found that increased BMI increases the risk of surgical site complications, but the risk of major complications is unaffected. The benefits of the procedure in obese patients are proposed to far outweigh the added cost and suffering associated with surgical complications, and thus, many authors recommend that RM should also be offered to this patient group (6, 10, 11, 13).
National guidelines of the indications for RM are published in several health care systems (17, 20, 21). In the Finnish health care system, obesity is not a contraindication for RM, but the Finnish guidelines suggest that a proper risk adjustment should be performed preoperatively. A BMI limit of 30–32 is widely used in the Finnish public health care system. Because of conflicting evidence, however, the association between BMI and surgical complications should be further investigated. Here, we aimed (1) to assess the incidence of minor and major complications after RM and (2) to identify risk factors, especially the role of increased BMI, contributing to such complications.
Materials and Methods
A total of 481 patients underwent RM (ICD codes HAD30 and HAD35) at Tampere University Hospital, an academic tertiary referral center, from 2007 to 2010. The clinical data were collected from medical records and analyzed retrospectively. Of 481 patients, 27 were excluded from the study because of breast cancer prior to surgery (n = 21), male sex (n = 4), and mastopexy instead of a reduction (n = 2). Data concerning one patient were lost during analysis. The remaining 453 patients were included in this study. Data on patient demographics; preoperative sternal notch to nipple distance; comorbid conditions including diabetes, hypertension, and coronary heart disease; and postoperative complications were gathered from medical records. The Institutional Review Board of Tampere University Hospital approved the study.
All patients underwent mammography and an ultrasound examination before surgery. Criteria set by the Finnish Ministry of Social Affairs and Health for indications for RM performed in public hospitals for health reasons were followed (21). These criteria indicate no exact BMI limit. While our institution mainly sets a BMI limit of 32, patients with higher BMI may also be operated on after risk adjustment following national guidelines (21). Smoking was considered a contraindication and all patients were expected to quit before the operation. The reduction technique was selected by the operative surgeon based on patient characteristics. Tampere University Hospital is a teaching hospital. Thus, most operations were performed by plastic surgery residents under supervision. Complications after RM were assessed from the medical records. Emergency plastic surgery in the whole Pirkanmaa Hospital District is organized at our institution, and thus, it is highly likely that the vast majority of patients with complications were treated at our unit and thus documented in the medical records. During the study period, all patients were kept overnight after RM in our hospital. The number of readmissions to either the plastic surgery ward or the emergency ward and additional visits at the outpatient clinic as well as the length of readmissions to the ward were recorded. Of the 453 patients, only 6 (1.3%) did not attend any follow-up visits at the outpatient clinic.
Complications were classified into two different categories: major and minor complications. Complications were classified major if the patient needed a reoperation or was readmitted to hospital for further treatment. Other complications treated on an outpatient basis were classified as minor. Major complications included hematoma; seroma; wound dehiscence; deep infection and necrosis of the nipple, areola, or wound requiring reoperation; and severe systemic or wound infection leading to hospitalization. Minor complications included delayed conservatively treated wound healing, superficial wound infections, and lymphadenitis, as well as conservatively treated hematomas, seromas, fat necrosis, necrosis of the nipple, areola, or wound.
Statistical analysis of the collected data was performed using IBM SPSS Statistics Version 20. An unpaired t-test for Gaussian populations was used to investigate whether hematomas requiring surgery, major complications, and minor complications were associated with age, BMI, or sternal notch to nipple distance. A chi-squared test for binominal variables was used to investigate whether hematomas requiring surgery, major complications, and minor complications were associated with hypertension, diabetes, and coronary heart disease. Analysis of variance (ANOVA) and post hoc tests were used to assess the effect of an increased BMI on the number of minor complications (0, 1, or ≥2 complications). Receiver operating curve analysis and logistic regression analysis were used to study the association of BMI with minor complications and hematoma evacuations.
Results
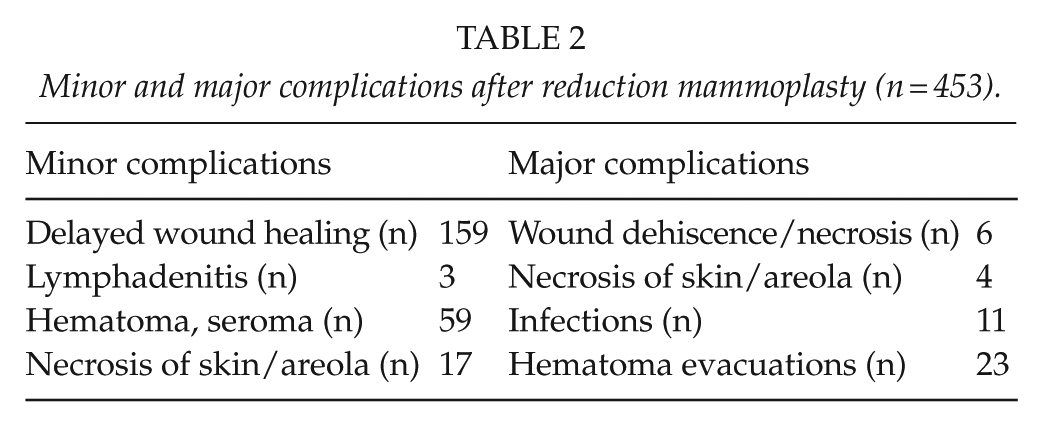
Patient characteristics are presented in Table 1. Hypertension was the most common comorbidity. The patients were, on average, overweight (mean BMI value 28.9, range 18.6-47.2); 80.2% (n = 364) of the patients had a BMI lower than 32.0, 12.8% (n = 58) had BMI a value of 32.0–34.9, and 6.8% (n = 31) of the patients had BMI of 35 or higher. Almost half of the patients (44.3%, n = 201) had at least one minor or major complication (Table 2).
Patient characteristics (n = 453).
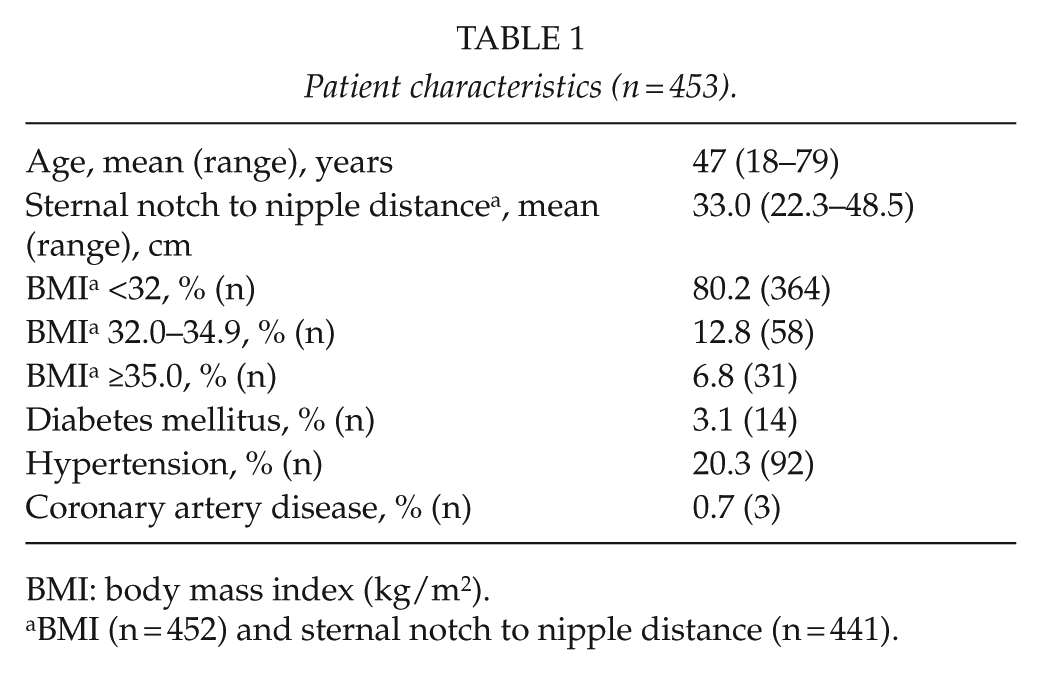
BMI: body mass index (kg/m2).
BMI (n = 452) and sternal notch to nipple distance (n = 441).
Minor and major complications after reduction mammoplasty (n = 453).
Major Complications
In all, 40 (8.8%) patients had at least one major complication and four (0.9%) patients had more than one major complication (Table 2). None of the patients were diagnosed with a deep venous thrombosis or pulmonary embolism. A total of 22 (4.9%) patients developed a hematoma requiring evacuation in the operating room. One of these patients had bilateral hematomas that both required evacuation. Evacuation of the hematoma was performed on the same day as the primary operation in 8 (36.4%) patients, the next day in 12 (54.5%) patients, and 2 days postoperatively in 2 (9.1%) patients.
In all, 16 (3.5%) patients were readmitted to the ward due to complications and 2 of these patients were readmitted twice. The mean length of the stay was 2.7 (standard deviation (SD) = 1.6) nights. There was no association between any of the major complications and sternal notch to nipple distance, age, diabetes, or hypertension. One of the three patients with coronary heart disease had a major complication. Mean preoperative BMI of the patients who developed a hematoma requiring surgery was 26.4 (SD = 3.0), a significantly lower value than that of patients without this complication (29.0, SD = 4.2; p = 0.003). Logistic regression analysis showed that an increase of one unit in BMI decreased the risk of a hematoma requiring surgery by 16.9% (odds ratio (OR) = 0.83, 95% confidence interval (CI) = 0.73–0.94; p = 0.004). This finding was also significant in the multivariate analysis (p = 0.002; Table 3). No other factors analyzed were associated with a hematoma requiring evacuation.
Results of multivariate analysis: hematoma evacuations and risk factors.
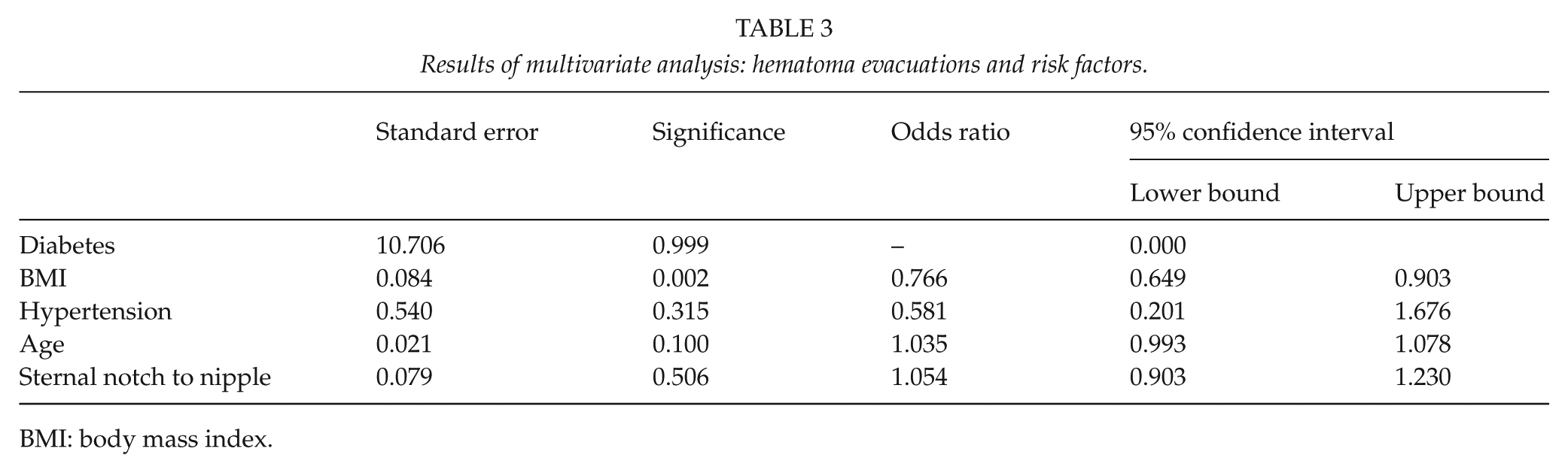
BMI: body mass index.
Minor Complications
A total of 184 (40.6%) patients had a minor complication and 39 of them (8.6% of all patients) had more than one minor complication (Table 2). Patients who suffered a minor complication had both a higher mean BMI (30.2 vs 28.0) and a longer mean sternal notch to nipple distance (33.9 cm vs 32.4 cm) than patients without any minor complications (p < 0.001 for both comparisons). In the multivariate analysis, however, BMI was found to be the only significant risk factor for minor complications (p < 0.001; Table 4). Patients who had at least one minor complication also made more visits to the outpatient clinic (p < 0.001). The mean number of visits was 1.23 (SD = 1.74) for patients with a minor complication compared to a mean of 0.23 (SD = 0.53) for those who experienced no complications.
Results of multivariate analysis: minor complications and risk factors.
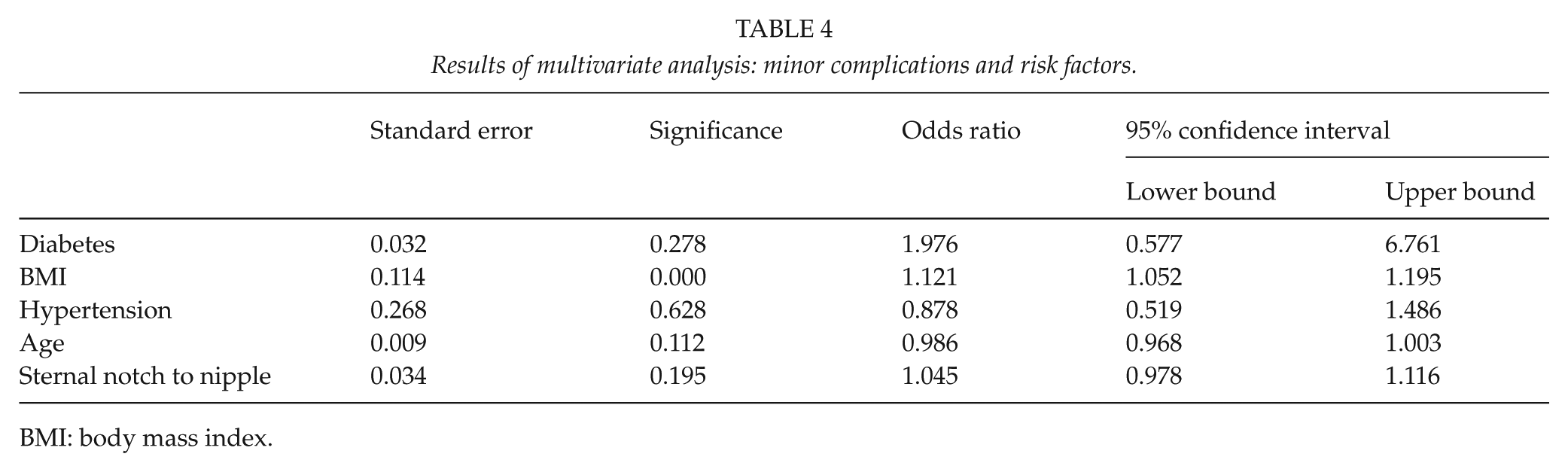
BMI: body mass index.
Further receiver operating curve analysis of the effect of BMI revealed an optimal cut-off point of 27.0. Patients with BMI higher than 27.0 had 2.6-fold higher odds for minor complications (OR = 2.56, 95% CI = 1.68–3.90; p < 0.001). The association between BMI and minor complications was further analyzed using a logistic regression analysis, which showed that an increase of one unit in BMI also increased the probability of minor complications by 14.1% (OR = 1.14, 95% CI = 1.09–1.20; p < 0.001). As patient BMI increased, the number of minor complications per patient increased significantly (p < 0.05 for all comparisons).
Discussion
A variety of guidelines exist regarding the indications for RM (20, 21). The criteria include minimum cup size, resection weight, sternal notch to nipple distance, BMI, psychologic morbidity, and smoking habit. BMI is a good indicator for obesity and also predicts surgical complications (22). A BMI of 25–30 indicates overweight, 30–35 moderate obesity, 35–40 severe obesity, and a BMI over 40 indicates very severe obesity. While we found no correlation between major complications and an increase in the BMI, a definite correlation between minor complications and an increase in BMI was detected.
The association between sternal notch to nipple distance and complication rate is controversial. Some studies have reported a positive association (9, 10). Manahan et al. (9) reported that a sternal notch to nipple distance greater than 37 cm was associated with increased rates of fat necrosis and minor wound complications, and a distance over 41 cm was associated with an increased risk of infections and major wound complications. Setälä et al. (10) found that the distance between the clavicle and areola was greater in patients with areola necrosis. Our results showed that the mean sternal notch to nipple distance was significantly higher among patients developing minor complications. Multivariate analysis, however, did not reveal this to be a significant risk factor. Other studies have reported no connection (7, 8, 14, 16, 19).
One interesting finding of this study was that the mean BMI value among patients requiring evacuation of a hematoma was significantly lower than that in patients without this complication. The reason for this finding is unclear. Previous studies demonstrated an association between hypotension during anesthesia and an increased number of hematomas requiring hematoma evacuation (23, 24). Due to the retrospective nature of this study, these data were not collected. It is possible that breast tissue itself differs between overweight and obese patients, that is, there may be more vascular glandular tissue instead of fat tissue in patients with a lower BMI.
Several studies have demonstrated a correlation between a higher BMI and postoperative complications after RM, consistent with our findings (6–14). Other studies, however, have reported an unclear connection (16–18) or no connection between preoperative BMI and post-surgical complications (15, 19). Zubowski et al. (18) reported a significant increase in the complication rates in obese patients. When the population was subdivided into five groups based on the degree of obesity, however, the correlation no longer held. The subgroups may have become too small for reliable analysis. The study by Eggert et al. (17) included no women with a BMI over 30. They observed a tendency toward more complications in the overweight group of patients (BMI = 25–30), but were unable to draw any conclusions due to the small size of the group. Cunningham et al. (15) and Neaman et al. (19) found no connection between BMI and post-surgical complications.
Chun et al. (6) suggested that patients with a BMI of ≥35.6 have significantly more postoperative complications overall. Manahan et al. (9) found that a BMI ≥ 35 increases the risk for infections, seromas, fat necrosis, and minor wound complications. Chen et al. (11) associated obesity (BMI > 30) with a nearly 12-fold increase in the odds for postoperative complications after elective breast procedures. Stevens et al. (14) associated a BMI > 27 with poor wound healing. Two large studies by Nelson et al. (12) and Gust et al. (13) using the National Surgical Quality Improvement database found a significant increase in the complication rates with increasing obesity classes. In our study, a correlation between BMI and complications was detected regarding minor, but not major, complications. This could be explained by the selection of patients. A BMI limit of 32 was used for the surgeries, and only 6.8% of the operated patients were severely or very severely obese (BMI > 35). Moderate BMI value can also explain the low number of patients with diabetes and coronary artery disease. In contrast, the number of patients with hypertension was higher. No connection between hypertension and postoperative complications was detected, consistent with previous studies (6, 9, 11, 13, 17).
The 40.5% rate of minor complications in this study is high, but the 8.8% rate of major complications is fairly low. These results are consistent with previous studies (25–27). The risk for minor complications was found to increase already in patients with a BMI of 27. This cut-off point is quite low compared to that suggested in earlier studies, which reported an increase in the risk with BMI > 26.3–40 (6, 7, 9, 12–14). It seems that most of the complications related to RM are minor, and thus, it is a safe procedure for overweight patients. In addition, esthetic outcome is also good in patients with higher BMI values (27). Only morbidly obese patients are at high risk for complications (10, 12). The benefits of RM in terms of QoL far exceed the risk of prolonged healing due to minor complications. Based on these facts, several studies recommend no restrictions based on patient BMI despite the significant increase in complication rates with increasing obesity (10, 12, 13). Current opinion is that informing patients of the potential risks well in advance of the surgery is sufficient. However, our study showed that patients with minor complications have more additional visits to the hospital, thereby increasing costs. This has implications for both health care staff and health care payers. RM itself can be accepted for obese patients for medical reasons. Public health care resources, however, are limited and there should be guidelines regarding which operations should be performed in a public hospital. In this respect, the current BMI limit of 30–32 is not too strict.
A strength of this study is the fairly large study population representing all women operated on in the public sector during the study period, thereby improving the generalizability of the results. Because of the structure of the Finnish health care system, it is likely that all major complications requiring hospital treatment or reoperation were included. The low number of very obese subjects (n = 89) and major complications (8.8%) in this study may have affected the weak association noted between these parameters. Another limitation to this study is its retrospective nature. The assessment of postoperative complications was based on medical records, and thus, bias of the information cannot be ruled out. It is also likely that some visits, for example, to the private sector due to minor complications, are missing from this study.
The amount of complications affects the cost of care. Data on health-related quality of life (HRQoL) before and after interventions should be collected in a further study. This approach would enable estimation of the number of quality-adjusted life years (QALY). Furthermore, when combined with costs of providing treatment, available from the hospital accounting records, this approach would also enable comparison of the cost utility of services offered for the patients.
In conclusion, a higher BMI is strongly associated with an increased risk of minor complications after RM. It is important to inform obese patients about the increased risk of complications and to encourage them to lose weight before surgery. Future studies are needed to analyze the effect of increasing BMI on the cost-effectiveness of RM.
Footnotes
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.