
Abstract
Background and Aims:
Shoulder capsular surgery is nowadays usually performed arthroscopically, and the proportion of arthroscopic method has rapidly increased during the last two decades. We assessed the incidence of shoulder capsular surgery procedures in Finland between 1999 and 2008.
Material and Methods:
We gathered the shoulder capsular surgery procedures for all kinds of shoulder instability in Finland between 1999 and 2008 from National Hospital Discharge Register and limited the patient material to include only certain diagnosis (International Classification of Diseases, 10th Edition) and Nordic Medico-Statistical Committee procedure code combinations. We analyzed the data in the whole country, between different age groups, and in university hospital districts.
Results:
The total incidence of shoulder capsular surgery procedures in Finland increased from 17 to 33 per 100,000 person-years. The incidence of arthroscopic procedures increased from 11 to 30 per 100,000 person-years and the proportion of arthroscopic procedures increased from 63% to 92% between years 1999 and 2007. The incidence of shoulder capsular surgery procedures increased on average around 90% in almost all age groups and particularly in the older age groups. We observed no significant geographical variation between university hospital districts.
Conclusion:
The incidence of shoulder capsular surgery procedures increased on average round 90% in almost all age groups. It seems to be difficult to support the rapidly increased rates of shoulder capsular surgery procedures or the arthroscopic method based on scientific evidence. While also older patients are treated with shoulder capsular surgery, well-defined indications for surgical intervention are needed so that the operations are conducted for the symptomatic patients benefitting most regardless of patients’ age.
Introduction
Shoulder is the most commonly dislocated large joint (1). The incidence of primary shoulder dislocations has varied between 15.3 (1) and 56.3 (2) per 100,000 person-years.
Shoulder instability is most commonly due to a structural damage of the shoulder joint after a traumatic shoulder dislocation or in a case of inherently lax joint, instability may develop either spontaneously or because of microtrauma (3). Dislocation of a non-lax shoulder almost always results in a lesion of capsulolabral complex (4). Atraumatic shoulder laxity without clinical signs or symptoms of instability, that is, subluxations or dislocations, does not require any treatment (5). In addition to a labral lesion, various ligaments around the shoulder joint may be torn and the bone of the humeral head or the glenoid may be damaged in a shoulder dislocation (6).
A typical anteroinferior dislocation of the shoulder is usually treated with reposition and a short immobilization for comfort. In addition, a rehabilitation program to strengthen the stabilizing muscles of the shoulder joint is commonly performed, but the evidence of the effectiveness of supervised physical therapy and training programs after a primary shoulder dislocation is limited and there has been no research on the subject since the advent of arthroscopic shoulder surgery (7, 8). Atraumatic shoulder instability is usually treated initially with exercise therapy as a goal to stabilize the joint by improving the muscle strength, proprioception, and muscle balance around the shoulder girdle. The treatment of atraumatic shoulder instability by supervised physical therapy has recently showed promising results (9).
The goal of shoulder capsular surgery is to stabilize the shoulder joint. There are rarely indications for shoulder capsular surgery due to pain without history or clinical findings of shoulder instability. If shoulder instability with recurrent dislocations and subluxations persists despite appropriate conservative treatment, a surgical treatment is usually offered to the patient (3). The most common surgical method is a Bankart repair, in which the detached labrum and anterior shoulder capsule are refixed to the anteroinferior articular margin of the glenoid (10). In atraumatic shoulder instability, surgery aims to tighten the inferior shoulder capsule (11). The concomitant lesions can be treated in the same operation, according to the surgeon’s discretion and the evaluation of the lesion’s clinical relevance.
Today, shoulder capsular surgery is mainly performed arthroscopically, and especially the proportion of arthroscopic shoulder capsular surgery has rapidly increased during the beginning of 21st century (12–16), even though the increase is not supported by scientific evidence (6, 17–19). Major contributing factors to the increase in arthroscopic procedures in general have been considered altered surgical trends (12), improved imaging technologies (20), financial motivation (12), and patients’ anticipation for superior outcome of arthroscopic procedures (21).
Our aim was to (1) investigate and report the rates of shoulder capsular surgery procedures in Finland between 1999 and 2008, (2) to find out the changes in incidence by age groups, and (3) study the differences of the procedure incidences by geographical location.
Material And Methods
The study was performed on the whole population of Finland excluding the Åland islands. The population of Finland was 5,150,000 at the start of the study in 1999 and increased to 5,300,000 at the end of the study period in 2008. Finland is divided into five university hospital districts, Helsinki, Tampere, Kuopio, Oulu, and Turku listed by population from the largest to the smallest. The population in the university hospital districts in 2008 varied between 1,810,000 and 691,000. The Åland islands were excluded due to healthcare being partly organized in Sweden.
We gathered the shoulder capsular surgery patients, operated for all kinds of shoulder instability or after a shoulder dislocation, in Finland during a 10-year period between 1 January 1999 and 31 December 2008. To gather the most accurate number of shoulder capsular surgery procedures, we included only certain Nordic Medico-Statistical Committee (NOMESCO) procedure code and International Classification of Diseases, Tenth Edition (ICD-10) diagnosis combinations. The translations of the NOMESCO codes vary across countries with respect to which codes are used and what the exact translation is. In Finland, it is not possible to differentiate between the specific part of labrum operated on (anterior inferior glenohumeral ligament (AIGHL) vs superior labrum anterior to posterior (SLAP) lesions), and the exact use of the codes varies among surgeons and institutions.
We first identified the patients from the Finnish National Hospital Discharge Register (NHDR) maintained at the National Institute for Health and Welfare and from the reimbursement register of Social Insurance Institution to capture all public and private hospital procedures using primary NOMESCO procedure codes NBE20, NBE25, NBE30, NBE35, NBE40, and NBE45. Of these patients, we identified and included only patients with the following primary ICD-10 codes of shoulder injuries or complaints: S42.1, S43.0, M24.2, or M24.4. ICD-10 codes S43.4 and S43.7 were accepted only as secondary ICD-10 codes. We excluded patients with the following primary ICD-10 codes: M05.3, M05.8, M05.9, M06.0, M07.1, M07.3, M08.0, M08.2, M08.3, M08.4, M08.8, M08.9, M35.1, M45, M75.0, S42.0, S42.2, S42.7, S42.8, or S42.9. In addition, to exclude multiple admissions for the same shoulder procedure episode, we assumed that a patient with two different register hits indicating shoulder capsular surgery procedure within 2 months could be considered the same procedure and treatment episode. For details of the content of the included and excluded ICD-10 codes and NOMESCO procedure codes in Finland, see Tables 1 to 3, respectively.
Included ICD-10 codes and explanations according to the Finnish translation.
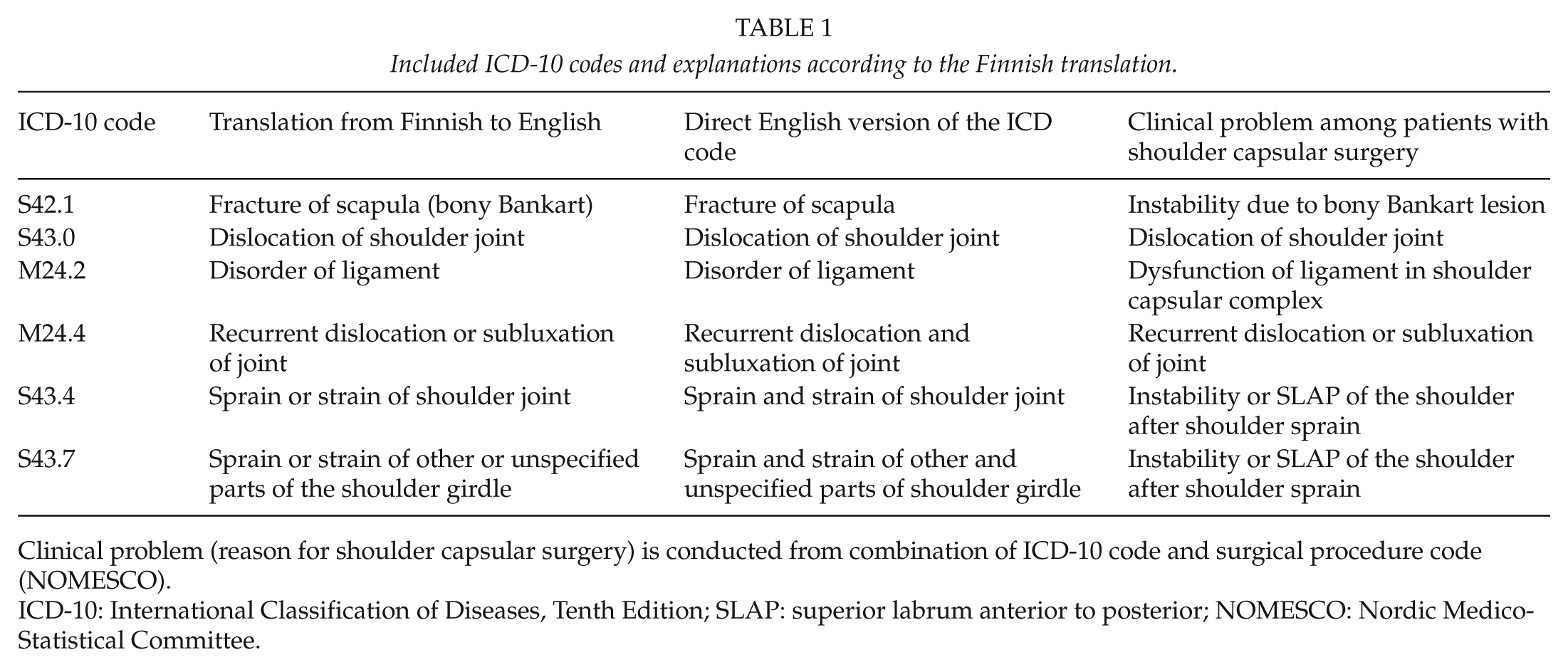
Clinical problem (reason for shoulder capsular surgery) is conducted from combination of ICD-10 code and surgical procedure code (NOMESCO).
ICD-10: International Classification of Diseases, Tenth Edition; SLAP: superior labrum anterior to posterior; NOMESCO: Nordic Medico-Statistical Committee.
Excluded ICD-10 codes and explanations according to the Finnish translation.
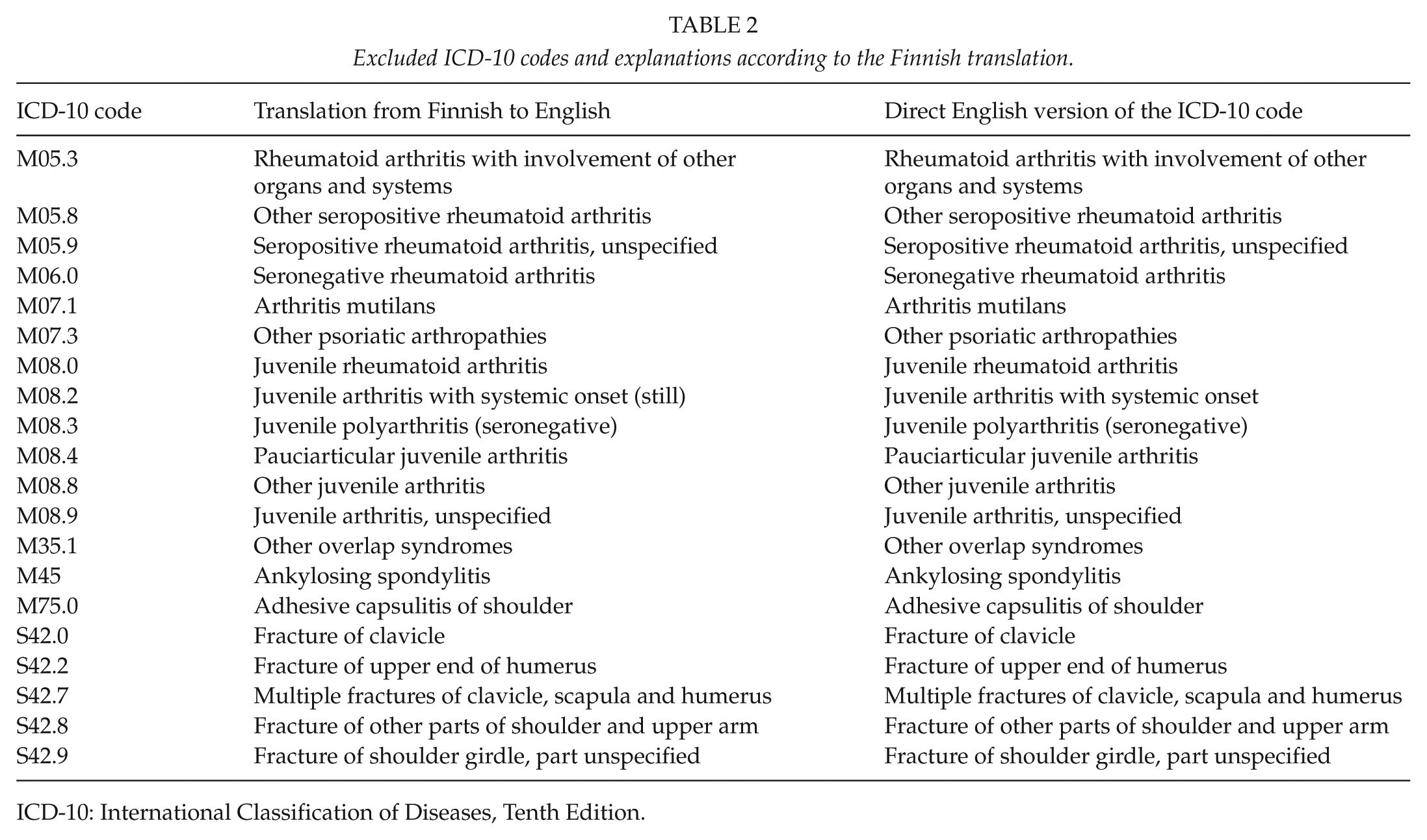
ICD-10: International Classification of Diseases, Tenth Edition.
Included surgical procedure codes (NOMESCO) and explanations according to the Finnish translation.
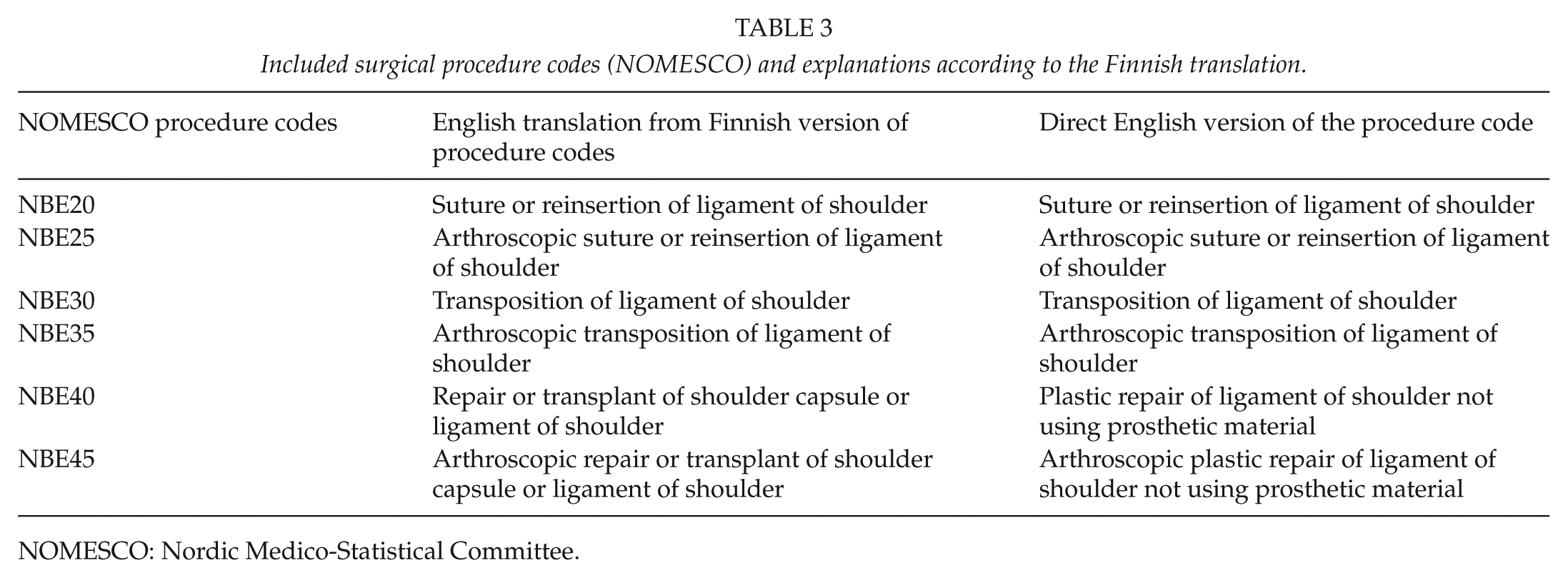
NOMESCO: Nordic Medico-Statistical Committee.
We analyzed the register data according to year, age group, and university hospital district. We obtained the surgery procedure incidences by dividing the number of procedures by the respective number of people at that year in the population. We calculated the incidence of shoulder capsular surgery procedures (per 100,000 person-years) in predetermined age groups (<20, 21–30, 31–40, 41–50, 51–60, and >61 years) and in different university hospital districts, and the procedures were performed in the (publicly funded) university hospitals. We gathered the annual populations in our age groups and in university hospital districts from the Finnish Official Statistics (22). The surgery rates were based on the entire population of Finland rather than on sample-based estimates, and thus, we did not calculate 95% confidence intervals. We performed the statistical analysis using Microsoft Excel (2013) computer software (Microsoft, Seattle, WA, USA).
Results
In Finland, a total of 13,673 shoulder capsular surgery procedures were performed between 1999 and 2008, and the average annual incidence of all shoulder capsular surgery procedures was 26 (range: 17–33) per 100,000 person-years. Increase in the incidence of procedures was 88% between years 1999 and 2007, when the peak in annual procedures was reached. The annual growth in the incidence of procedures was on average 7% (range: −3% to 18%). The annual incidences of shoulder capsular surgery procedures and the geographic variation between incidences of shoulder capsular surgery procedures in university hospital districts per 100,000 person-years between 1999 and 2008 are presented in Figs 1 and 2, respectively. The key descriptors of the data are presented in Table 4.
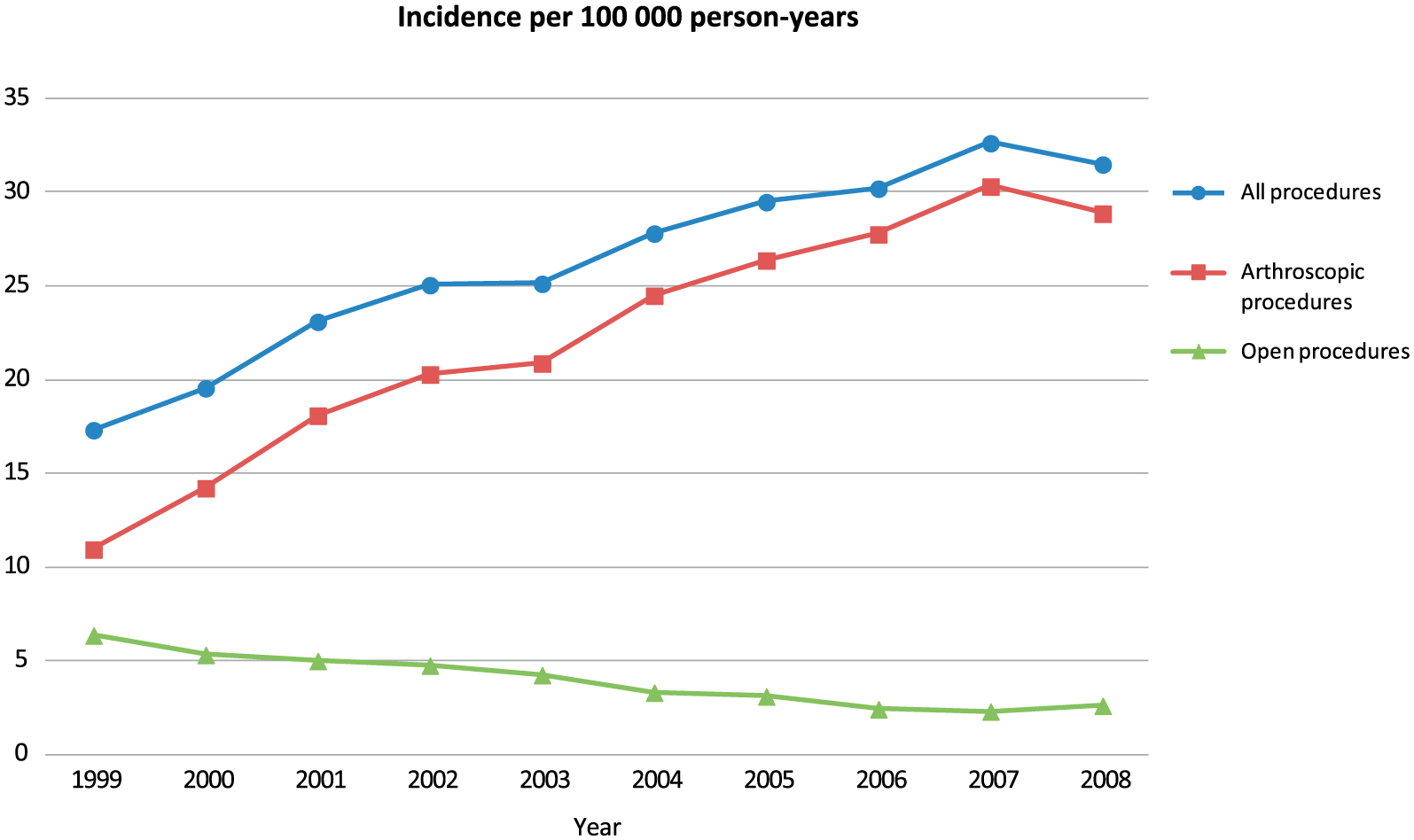
Incidence of shoulder capsular surgery procedures in Finland between 1999 and 2008. The amount of procedures has risen significantly, and the rise is due to the increase in the incidence of arthroscopic procedures.
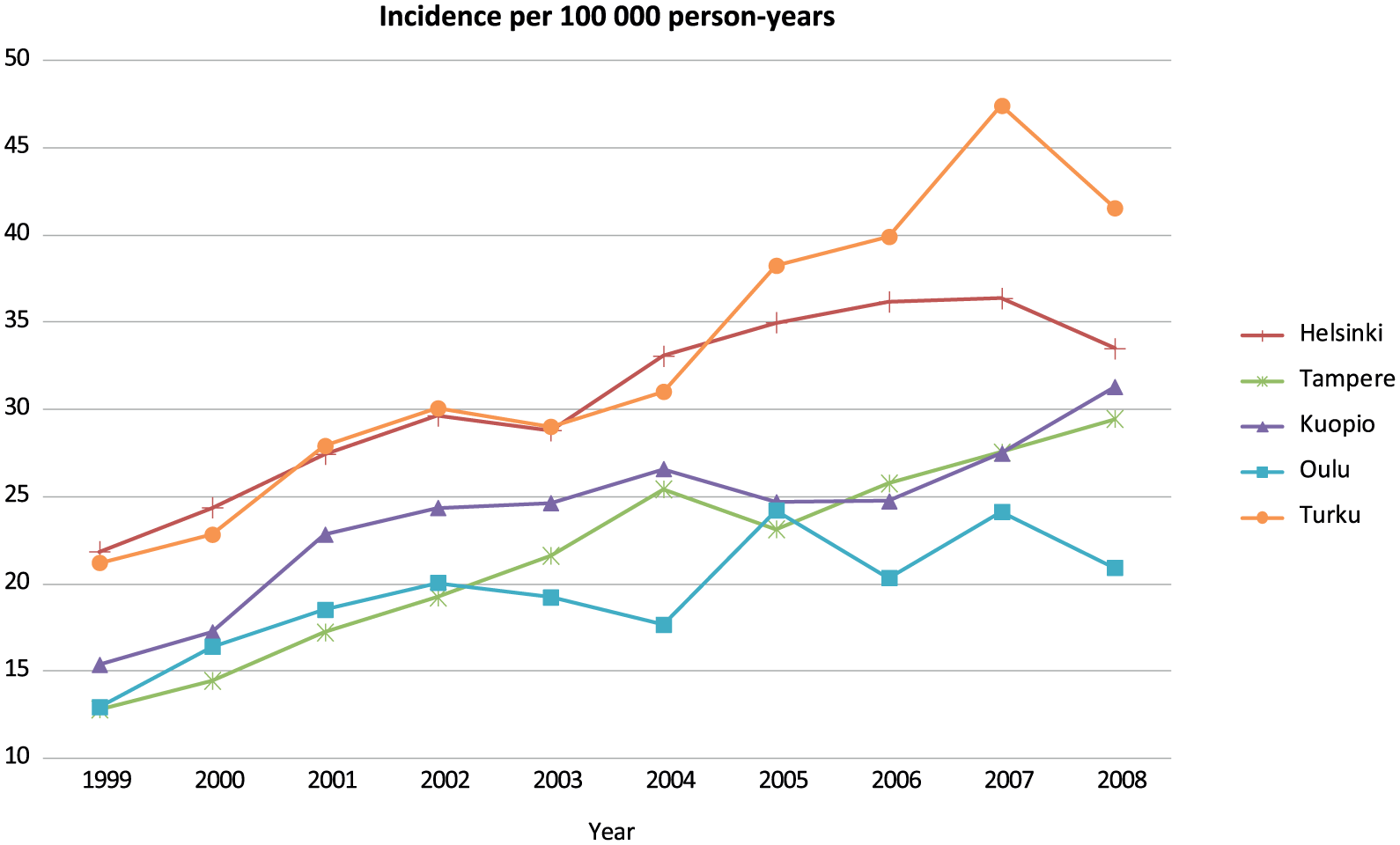
Geographic variation in incidence of shoulder capsular surgery procedures in university hospital districts in Finland between 1999 and 2008 per 100,000 person-years. The incidence has risen in all university hospital districts. University hospital districts are listed according to their size from largest to smallest.
Key descriptors among 13,673 patients operated for shoulder capsular lesions in Finland between 1999 and 2008.
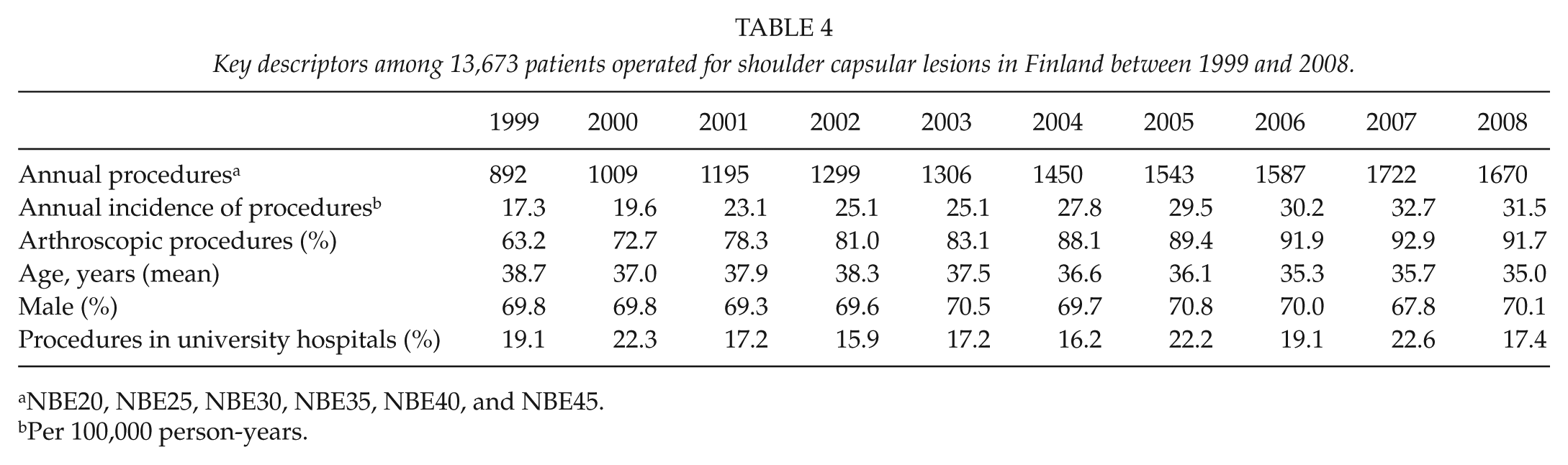
NBE20, NBE25, NBE30, NBE35, NBE40, and NBE45.
Per 100,000 person-years.
Of the average annual incidence of 26 procedures per 100,000 person-years, 22 (85%) (range: 11–30) were arthroscopic. The total incidence of procedures increased annually on average 7% (range: −4% to 18%), whereas the annual rate of arthroscopic procedures increased on average 12% (range: −5% to 30%). Between years 1999 and 2007, the increase in the incidence of arthroscopic procedures was 89% and the proportion of arthroscopic procedures increased from 63% to 93% (Table 4). Only from 2007 to 2008 the incidence of arthroscopic procedures decreased slightly and was 30 and 29 per 100,000 person-years, respectively.
The annual incidence of open shoulder capsular surgery procedures was on average 4 (range: 2–6) per 100,000 person-years. The annual decrease in the incidence of open procedures was on average 9% (range: −22% to 13%), and the incidence decreased 64% between years 1999 and 2007.
The total shoulder capsular surgery incidences in age groups are presented in Fig. 3. In the age group of >61 years, the average annual incidence of shoulder capsular surgery procedures was the lowest 11 (range: 6–15), whereas in the age group of 21–30 years the incidence was the highest 66 (range: 37–86) per 100,000 person-years. The incidence of all shoulder capsular surgery procedures increased between 1999 and 2007 on average 89% (range: −37% to 200%) in all age groups, but particularly in the age group of 41–50 years. The incidence decreased only in the age group of >61 years.
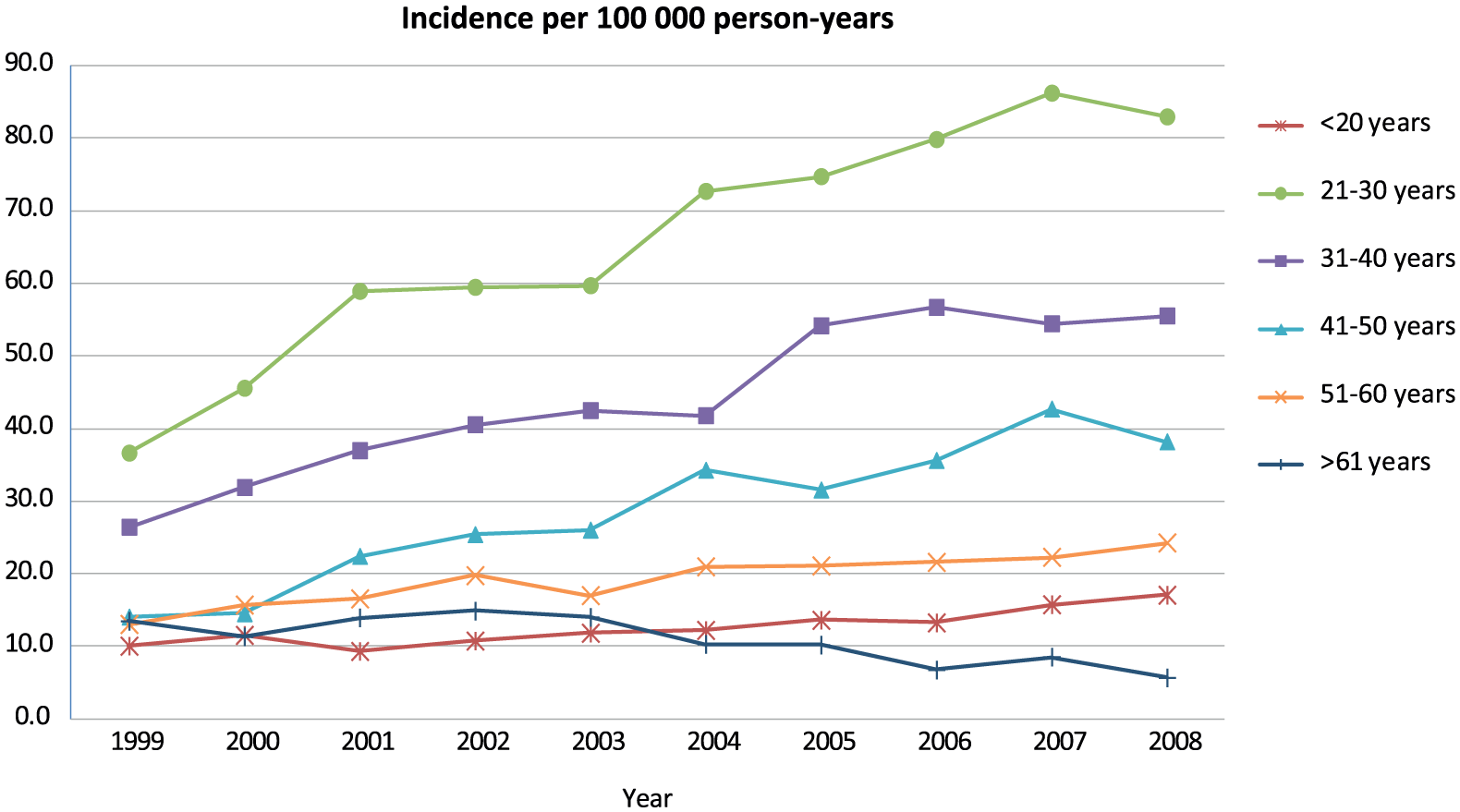
Incidence of shoulder capsular surgery procedures in age groups in Finland between 1999 and 2008 per 100,000 person-years. The incidence has risen in all but the oldest age group of >61 years.
In the age group of >61 years, the average annual incidence of arthroscopic procedures was the lowest 6 (range: 4–8), whereas in the age group of 21–30 years the average annual incidence was the highest 59 (range: 25–82) per 100,000 person-years. The incidence of arthroscopic shoulder capsular surgery procedures increased in all but the oldest age group on average 160% (range: −12% to 280%) between years 1999 and 2008; most increase was in the age group of 41–50 years, and in addition, the increase was 150% in the age group of 51–60 years.
The smallest incidence of open shoulder capsular surgery procedures was in the age group of <20 years, in which the annual incidence was on average 1 (range: 0.5–3) per 100,000 person-years. The highest incidence of open shoulder capsular surgery procedures was in the age group of 21–30 years being 7 (range: 4–12) per 100,000 person-years. The annual incidence of open procedures decreased on average 55% (range: 24%–80%) in all age groups, but particularly in the age group of >61 years between 1999 and 2008.
Discussion
The increase in shoulder capsular surgery procedures in Finland almost doubled between years 1999 and 2007, and thereafter slightly decreased in 2008. The incidence of arthroscopic procedures almost tripled and the proportion of arthroscopic procedures increased from 63% to 92%. The incidence of all shoulder capsular surgery procedures increased on average around 90% in all age groups (except those >61 years), but particularly in the age group of 41–50 years. We did not find any significant geographical variation between university hospital districts.
The most important limitation in our study is that the Finnish translation of NOMESCO procedure codes concerning shoulder capsular surgery operations (NBE2x, NBE3x, NBE4x) does not characterize the specific subtypes of procedures (e.g. Bankart repair, capsular shift, SLAP repair), but only indicate that a shoulder capsular surgery procedure has been performed. The inaccuracy of the terms has led to inconsistent use of the procedure codes in Finland. For example, for the arthroscopic Bankart repair, any of the codes NBE25, NBE35, and NBE45 has been used. The inaccuracy of the procedure codes could have been leading to overuse of the codes NBE35 and NBE45 instead of NBE25 because billing of the treatment episode is based on the procedure codes. Thus, we had to analyze these procedures without meticulous categorization, and so also SLAP injuries may be included in the patient material. This misuse of the procedure codes leads to an additional limitation of the study, while clinicians may use less suitable or even wrong procedure codes to indicate these performed procedures. In our opinion, however, combination of these diagnosis–procedure pairs makes our material to represent shoulder capsular surgery in Finland to clinically relevant extent.
A major strength of the study is that we have a nationally comprehensive patient data covering 10-year cohorts. In addition, taking these limitations into account, the accuracy of data in Finnish NHDR can be considered good (23).
According to our knowledge, comprehensive national long-term population-based studies of shoulder capsular surgery incidence rate have not been reported. Six previous studies have reported only short-term or nationally uncomprehensive register data of shoulder capsular surgery procedures (12–16, 24).
Even though the analyzed data in previous register studies (12–16, 24) are not generalizable to national level nor are the incidences or the amounts directly comparable with our surgery procedure rates, the evolution of shoulder capsular surgery procedure rates corresponds with our study. In our material, the proportion of arthroscopic procedures in 2008 (92%) was even higher compared to the previously published rates of 80%–90% (13, 15, 16).
In our material, the incidence of annual procedures in age group of 21–30 years was clearly bigger than in all other age groups. However, increase in the incidence of shoulder capsular surgery procedures was rapid and surprisingly high in patients of 41–60 years comprising 27% of the arthroscopic procedures. Our proportion of older patients agrees with a previous study (13).
In Norway, the incidence of shoulder capsular surgery procedures in 2009 was 12 per 100,000 person-years and the annual shoulder capsular surgery procedure rate increased 20.8% between years 2007 and 2009. Norwegian material shares the same problem including also SLAP repairs (24). In our material, the amount of arthroscopic shoulder capsular surgery procedures increased 5% between the years 2006 and 2008, whereas between years 2003 and 2005 the increase was 27%. The incidence of shoulder capsular surgery procedures in Finland was significantly higher than in Norway, an observation difficult to explain by differences in underlying prevalence of instability.
In the United States, a significant geographical variation in shoulder capsular surgery procedures has been previously reported and the variation might represent effects of variability in orthopedic training programs and the number of orthopedic fellowship trainees (16). In our study, the incidence of shoulder capsular surgery procedures increased in every university hospital district (Fig. 2). In Finland, the public hospitals bear a century-old constitutional responsibility to provide necessary healthcare to all citizens, and thus the structure of national healthcare system, treatment practices, and training programs may be more uniform than in the United States.
Probably to a smaller degree, the variation in regional surgery procedure rates is due to differences in illness burden, diagnostic practices, and patient attitudes. It is plausible that surgeons’ attitude, beliefs, and decision-making about the indication for surgical intervention may also affect the amount of executed surgical procedures (25). In addition, financial incentives (12) or insurance policies (26) have been introduced as possible determinants. Treatment habits may also change even though surgeon-perceived outcomes with newer techniques are similar rather than better than with older techniques (27). It is notable, though, that the proportion of the procedures performed in (publicly funded, staffed by not-per-procedure paid surgeons) university hospitals stayed almost constant during the study period, indicating more likely a change in either background incidence or treatment practices rather than change driven by secondary, provider or insurer-related, incentives.
Patients’ anticipations may influence increasing shift of surgery from open to arthroscopic and on increasing the incidence of surgery in general. According to a survey of how people perceived open versus arthroscopic shoulder surgery, 92% of patients perceived a strong preference for arthroscopic surgery compared with open surgery. It was more likely that a patient wished to avoid surgery if only open surgery was suggested, and 92% of patients with previous shoulder surgery would prefer arthroscopy. Patients also believed that functional outcomes would be superior; even in long-term, they would have less pain, faster recovery, and less time away from activities with arthroscopic approach (21). In addition, improved cosmetic appearance could make arthroscopic procedures more favorable option from patients’ perspective.
Recent meta-analyses (6, 17) and a systematic review (18) have concluded that there are no relevant clinical differences between open and arthroscopic Bankart operations in terms of shoulder instability or as in a recent meta-analysis (19) that the recurrent instability rate might even be higher after an arthroscopic Bankart operation. Therefore, from surgeons’ perspective, indications to favor arthroscopic procedure are relative.
In the United States, arthroscopic shoulder instability surgery is nowadays primarily an ambulatory procedure, which makes the overall expenses for this procedure lower (28). Arthroscopic shoulder capsular surgery has advanced considerably over the past 10 years, with improved instrumentation, implants, fluid delivery systems, surgical techniques, and aftercare (4). Improved imaging technology has enhanced the preoperative diagnostics of shoulder capsular abnormalities (20), while clinical relevance and, specifically relation to a clinical complaint, has remained somewhat unclear (29).
In Finland, the number of shoulder capsular surgeries increased between years 1999 and 2008 in (almost) all age groups, and it is particularly difficult to rationalize the increase in the older population, as shoulder capsular lesions and complaints—especially recurrent instability—are more clinically relevant in the younger population (30). According to our results, the need to carefully consider other treatment options—that is, conservative management—cannot be overstated, as the scientific evidence does not support the rising incidence of procedures (6, 17–19).
The rising incidence of shoulder arthroscopy is clear, but similar studies are needed to evaluate the trends more globally. We also need more up-to-date estimates of the incidence rates in general, in specific procedure types, and in different age groups. It would be important to gain data on whether the procedure is performed due to shoulder instability or ligamentous or labral pathology. This underlines the need for disease-specific national shoulder registers.
In conclusion, the incidence of shoulder capsular surgery procedures increased on average around 90% in almost all age groups. It seems to be difficult to support the rapidly increased rates of shoulder capsular surgery procedures or the arthroscopic method based on scientific evidence. While also older patients are treated with shoulder capsular surgery, well-defined indications for surgical intervention are needed so that the operations are performed for the symptomatic patients benefitting most regardless of patients’ age.
Footnotes
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
L.K. has received a research grant from Finnish Research Foundation for Orthopaedics and Traumatology and Helsinki Academic Medical Center.