
Abstract
Background and Aims:
Intra-abdominal local recurrences of colorectal cancer can be difficult to localize and excise because they are not easily visible or palpable.
Materials and Methods:
We report on our experience using the computed tomography–guided harpoon technique to locate and resect these nodules in seven patients.
Results:
No complications were recorded during the procedures. Six nodes were malignant and all margins were tumor free.
Conclusions:
Harpoon placement for intra-abdominal local recurrences of colorectal cancer is a feasible and useful technique that provides direct localization and complete excision of lesions.
Keywords
Introduction
Intra-abdominal local recurrence of colorectal cancer is a major issue after surgery in colorectal cancer. Surgical localization and removal can be technically difficult as recurrent lesions may be small and located in relatively inaccessible areas of the abdomen, such as the pelvis or the perineum, or surrounded by necrotic or fat tissue (1, 2). As a result, they are not easily visible or palpable. Precise localization of a small nodule is paramount, however, as resection of recurrences can improve survival. Localization and surgical management in non-palpable breast lesions, pulmonary nodules, and other small masses in other parts of the body is often performed by means of preoperative hookwire placement using the harpoon technique (3). The use of this technique in the case of intra-abdominal local recurrences of colorectal cancer, however, is not well defined, but it has shown to be feasible and useful in this setting, especially when the anatomic landmarks are not clear or when exposure of surgical field is altered (1). We report our experience in seven patients with intra-abdominal local recurrences localized with harpoon technique and surgically resected. To our knowledge, this is the first series in the literature to describe this technique for intra-abdominal local recurrences of colorectal cancer.
Materials and Methods
We retrospectively analyzed data from seven patients who underwent surgery for intra-abdominal local recurrences of colorectal cancer at our hospital from April 2012 to January 2016. For the purpose of this study, no institutional review board approval was required, according to Spanish Law 14/2007 for Biomedical Research. The patients (one male and six females) were aged between 41 and 81 years. All had previously undergone surgery for colorectal cancer and presented recurrences during the follow-up (Table 1). All the primary tumors were colorectal adenocarcinomas and none were of mucinous origin. Thoraco-abdominal computed tomography (CT) scan and/or positron emission tomography (PET) scan was performed in all patients to exclude disseminated disease or the presence of multiple nodules (Fig. 1A). Due to the potential difficulty for surgeons to locate small abdominal lesions in obese subjects or patients with multiple previous abdominal operations, placement of a CT-guided harpoon was undertaken after the patients’ written consent was obtained. Patients were admitted on the day of surgery. The radiological procedure was performed under local anesthesia with 10 mL of 2% lidocaine. Under CT guidance, the radiologist planned the site, depth, and angulation of harpoon entry. The lesions were localized by CT scan (2.5 mm section thickness). The puncture route was anterior or lateral transperitoneal in all but one patient, in whom trans-gluteal access was preferred due to a deep pelvic lesion. A radio-opaque skin marker was placed and the depth of the lesion was calculated. A harpoon, Hawkins 20 gauge × 10 cm type, was placed under sterile conditions near the lesion through a rigid introducer, positioning it less than a 1 cm away from the recurrence. Correct placement of the device was checked by CT scan (Figs 1A and 2). The extra-abdominal wire was fixed to the skin to prevent tampering or mobilization. Utmost care was taken during any moving of the patient. The patients were transferred to the operating room after the radiological procedure was completed. Depending on the location of the nodules, the open surgical approach through median laparotomy (three patients) or a lateral incision was performed (four patients). The recurrences were easily located using harpoon-guided CT and lesions were resected. A safety margin of healthy tissue of at least 1 cm was excised together with the lesion. En-bloc excision of the nodules was achieved without manipulation or removal of the harpoon (Fig. 3). A colonic resection was necessary in one patient due to neoplastic infiltration.
Patients’ clinical and pathological characteristics.
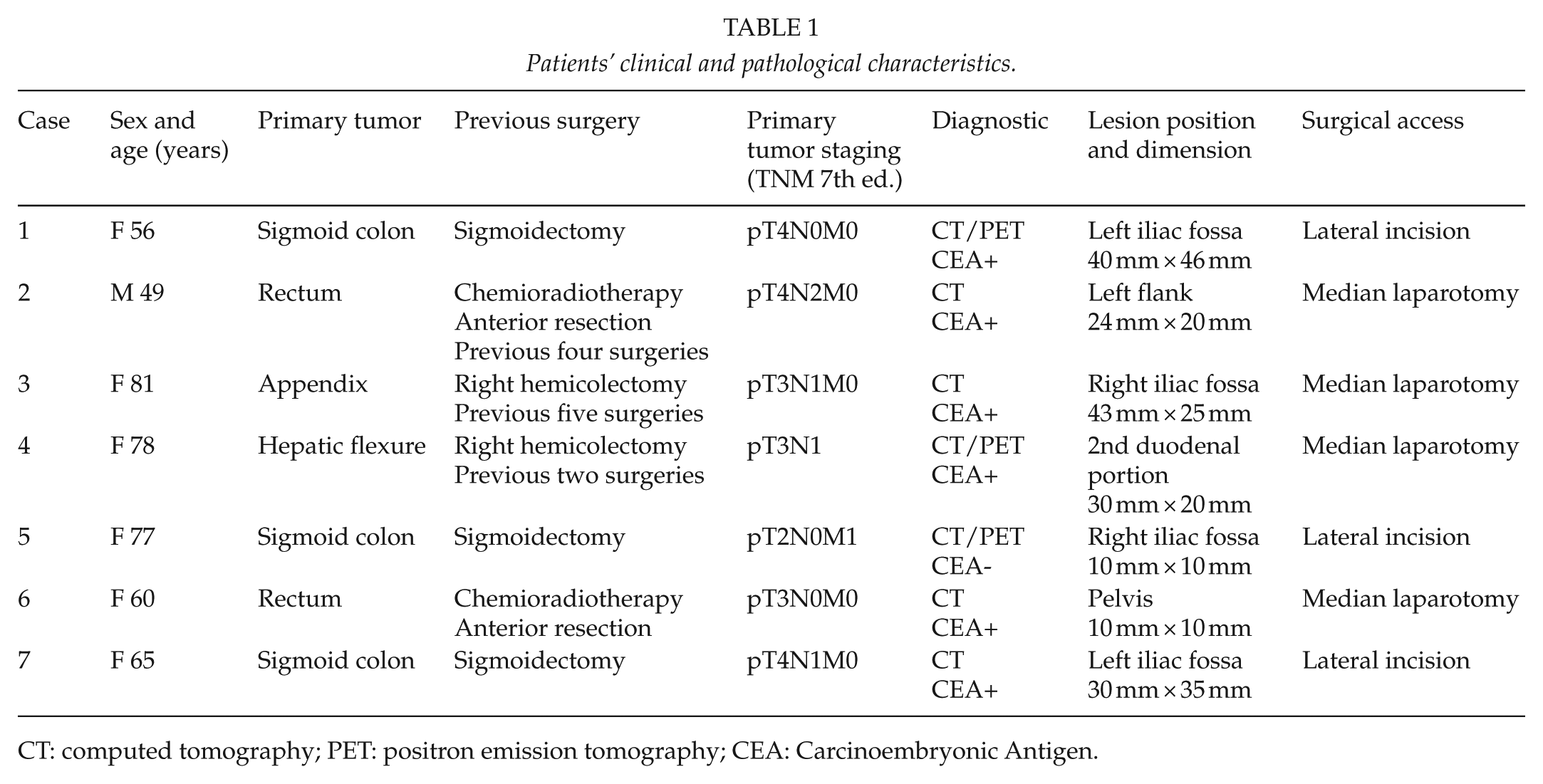
CT: computed tomography; PET: positron emission tomography; CEA: Carcinoembryonic Antigen.
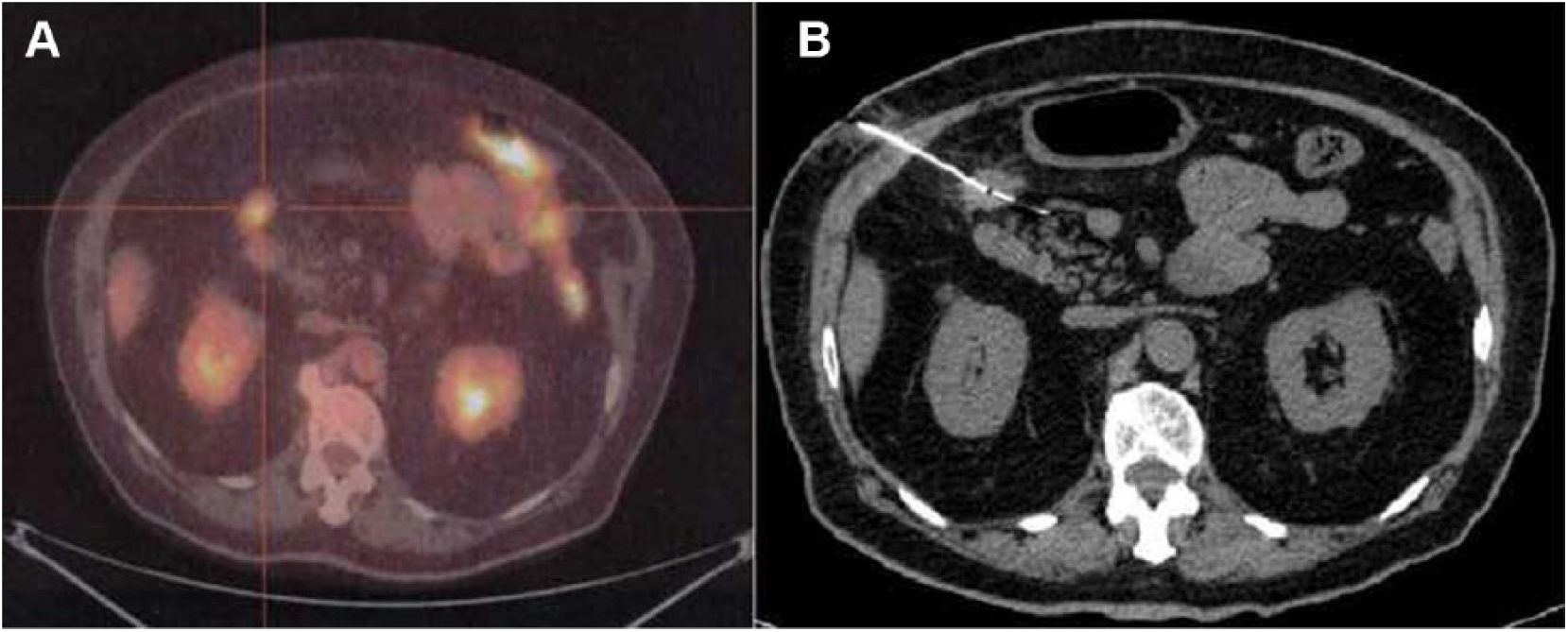
A) Diagnostic PET of a small periduodenal recurrence and B) CT scan checking correct harpoon positioning near the duodenum.
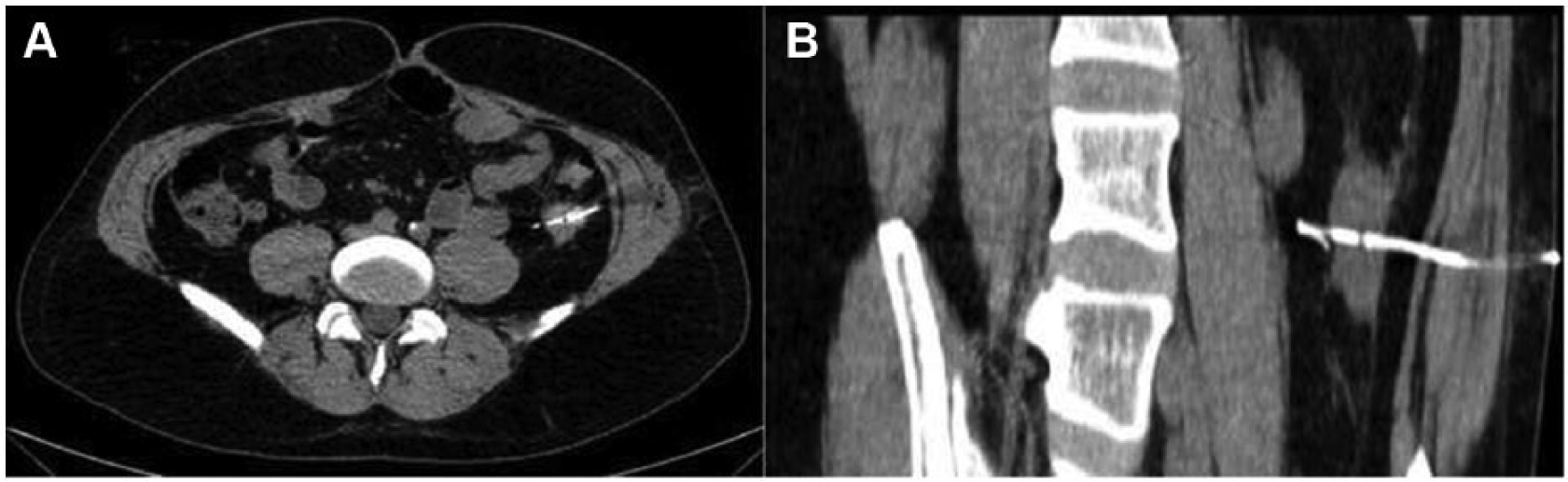
A) Axial and B) sagittal CT scan of harpoon positioning in a case of left flank nodule.

En-bloc lesion and harpoon excision.
Results
Harpoon placement was successful in all seven patients. No patients reported pain during the radiological procedure. No harpoon-related complications were noted and no intra-abdominal organ injuries occurred. In all cases, the tumor was undoubtedly located near the harpoon.
Surgical excision of the lesions was performed without complications in any patient. Resection was complete and curative in all cases. Pathological analysis confirmed the neoplastic nature of the nodules in six patients, but the lesion was fibrotic (no malignant) in one patient. A PET scan in this patient showed a false pathological uptake in the right lower quadrant.
Discussion
Excision of intra-abdominal local recurrences improves prognosis and survival in patients who have undergone surgery for colorectal cancer. However, the effects of primary surgery and radiation on tissues make the surgeon’s search for these recurrences and their excision difficult because small lesions may be relatively inaccessible due to their deep location and they are not always palpable and visible (1). Furthermore, the consistency of the lesions may be similar to surrounding tissues with postoperative or radiotherapy-related fibrosis changes, making surgical identification difficult. It can therefore be challenging to locate and excise a small pelvic or abdominal nodule that often has the same characteristics of the surrounding fatty or fibrotic tissue. In such cases, placement of a CT-guided harpoon can be a useful technique to help reduce surgical time and favor accurate tumor resection (1, 4). The viability of the approach can be assessed by radiological examination, but the final access route is based on the images obtained at the time of the procedure. If feasible, the anterior or lateral transperitoneal approach is recommended to insert the harpoon to facilitate surgical access to the peritoneal cavity. The route of the harpoon should then be followed until the exact location of recurrence is reached. Using saline injection or changing the patient’s position during the imaging procedure may help prevent visceral or vascular lesions. A curved needle may also be useful to decrease the risk of puncturing organs. Other approaches may also be undertaken. The trans-gluteal approach, for example, is indicated for recurrences located deep within the pelvis, the pre-sacral area, or the peri-rectal area and for those situated postero-laterally to the bladder. Using this approach, the harpoon is more stable, avoiding peritoneal puncture, but sacral plexus, gluteal sciatic nerve, and vascular structure injuries may occur. When pelvic lesions are inaccessible by the trans-gluteal or anterior or transperitoneal lateral approaches, especially in the posterior area, the approach could be via bone or via trans-sacral or trans-iliac access. For recurrences in the region of the iliac nodes or in the lateral wall of the pelvis, anterolateral extraperitoneal access through the ileo-psoas muscles is indicated. Femoral nerve injury is rare and the approach is painless. During harpoon placement, the radiologist should not manipulate the lesion because it may cause neoplastic dissemination. Harpoon placement should be performed with the patient in the same position as for surgery, in order to prevent harpoon migration. The possible complication of harpoon displacement could be resolved using an internal spring harpoon and external fixation to the skin. In our series, all patients underwent surgery immediately after placement of the harpoon, thus preventing tampering or device migration. The technique of locating intra-abdominal local recurrences or colorectal cancer with the CT-guided harpoon technique is similar to CT-guided fine-needle aspiration (FNA) of intra-abdominal masses. Patient tolerance and duration are also similar. The incidence of possible secondary complications of harpoon placement can thus be extrapolated from the incidence of FNA, which is about 1.3% (5). Mortality performing FNA has been reported as 0.006%, mainly occurring in liver and pancreatic biopsies (6). We consider these data support the safety of the harpoon technique, taking into consideration the tumor location, the intra-abdominal route chosen, and the experience of the radiologist (5). Minor complications include pain, local bleeding at the puncture site, and vasovagal reaction. The most feared complication is intestinal perforation, especially with the transperitoneal approach, but it is generally accepted that fine-needle puncture in immunocompetent patients is safe and does not lead to major complications. The incidence of post-puncture peritonitis may reach 0.3% (5, 6). In our series, we did not encounter any complications during radiology or during surgery.
Conclusion
CT-guided harpoon placement in cases of intra-abdominal local recurrences of colorectal cancer is a feasible and useful technique if patients have undergone several previous interventions, if they have had prior radiotherapy, or if they are obese. It provides direct surgical location and precise and complete excision, avoiding unnecessary manipulation or resection of other organs. We indicate the use of the harpoon technique in cases of single small (<3 cm) abdominal recurrent nodules requiring surgical excision.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.