
Abstract
Background and Aim:
Endoscopic stents in the common bile duct is the first treatment choice to alleviate symptoms of biliary obstruction due to malignant disease. When endoscopic stenting fails in palliative patients, one option is to use a percutaneous transhepatic biliary drainage, but it is not clear whether and how it can reduce the symptom load. The aim of this study was to evaluate benefits and disadvantages of percutaneous transhepatic biliary drainage in palliative care.
Material and Methods:
Inclusion criteria were malignant disease and bilirubin ≥26 µmol/L in plasma. A structured protocol for obtaining data from the medical records was used. Data were collected from the time of last computed tomography scan before the percutaneous transhepatic biliary drainage was placed and during 14 days afterward.
Results and Conclusion:
Inclusion criteria were fulfilled in 140 patients. Median age was 70 years (33–91 years). Some 126 patients had a remaining external percutaneous transhepatic biliary drainage. Jaundice was the initial symptom in 62 patients (44%). Within the first week after percutaneous transhepatic biliary drainage, the bilirubin decreased from 237 µmol/L (31–634) to 180 µmol/L (17–545). Only 25% reached a level below the double upper reference value. Pruritus occurred in 27% before the percutaneous transhepatic biliary drainage, but the bilirubin value did not differ from patients without pruritus. However, the pruritus was relieved in 56% with percutaneous transhepatic biliary drainage. Antibiotic prophylaxis protected to some extent from infectious complications. Adverse events were common and early mortality was high (16% within 14 days). Jaundice should not by itself be an indication for percutaneous transhepatic biliary drainage for palliation except when the aim is to prepare the patient for chemotherapy. It is mandatory that the patients are informed carefully about what can be expected regarding the positive effects and the risks of adverse events.
Keywords
Introduction
In biliary obstruction due to malignant disease, liver metastases, other distant metastases, or locally advanced tumor growth are common. Various manifestations such as jaundice, pruritus, altered taste of food, anorexia, malnutrition, renal impairment, impaired immune dysfunction (1–3), and impaired quality of life (4, 5) are associated with the obstruction. For a long time, the relief of obstructive jaundice was accomplished with surgical bilioenteric bypass (6, 7). However, percutaneous transhepatic biliary drainage (PTBD) or endoscopic drainage are less invasive alternatives and has been used for several decades. Endoscopic stents in the common bile duct is today the first choice to alleviate symptoms and prolong life by decreasing hyperbilirubinemia before surgery, chemotherapy, or as palliation (8). However, when endoscopic stenting fails in palliative patients, one option is to recommend PTBD and another is to offer best supportive care. The risks for complications should be limited in palliative care as the main purpose is to preserve or improve quality of life and sometimes to prolong life. However, it is not clear whether and how a remaining external drainage can reduce the symptom load in palliative patients. The aim of this study was to evaluate the benefits and the disadvantages of PTBD in palliative care.
Material and Methods
Procedures related to percutaneous transhepatic cholangiography (PTC) were performed in 516 patients during June 2010–June 2013 at Linköping University hospital. All procedures were identified from the hospital registration systems. Inclusion criteria in this study were patients with malignant disease and bilirubin ≥26 µmol/L in plasma. All PTBD procedures were done in general anesthesia, the classification according to American Society of Anesthesiologists (ASA) is shown in Table 1. All included patients had stage IV disease and received palliative treatment without surgery. In 68 patients, an endoscopic retrograde cholangio-pancreaticography (ERCP) with or without successful endoscopic drainage had been performed previously. When possible, the external drainage was converted to an internal drainage. An intention to internal stenting in this patient cohort with advanced diseased was documented in 31 patients and became permanent in 14 patients. The flow chart of patients is shown in Fig. 1. Digital medical records of the patients included were reviewed using a structured protocol from the last computed tomography (CT) scan before the PTBD until 14 days after the PTBD. In addition to age and gender, the protocol included cancer diagnosis, symptoms (lack of appetite, fatigue, pruritus, dark urine, weight loss, abdominal pain, feeling of sickness), performance status, ASA, date of PTBD, antibiotics, kind, time, and duration of complications, effect on symptoms, and various laboratory values.
Characteristics of 140 patients with malignant disease causing biliary obstruction with a value of bilirubin in plasma of ≥26 µmol/L.
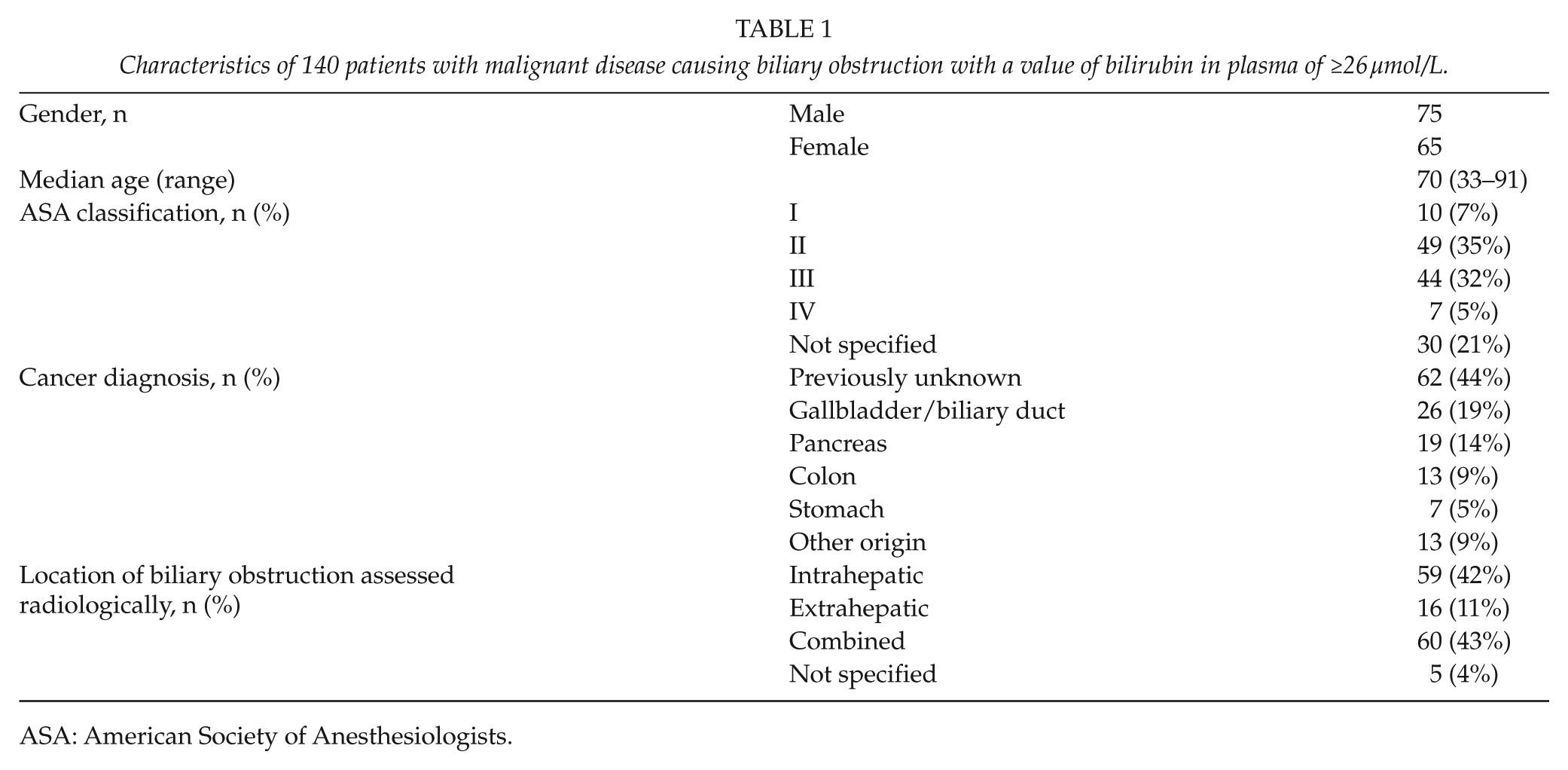
ASA: American Society of Anesthesiologists.
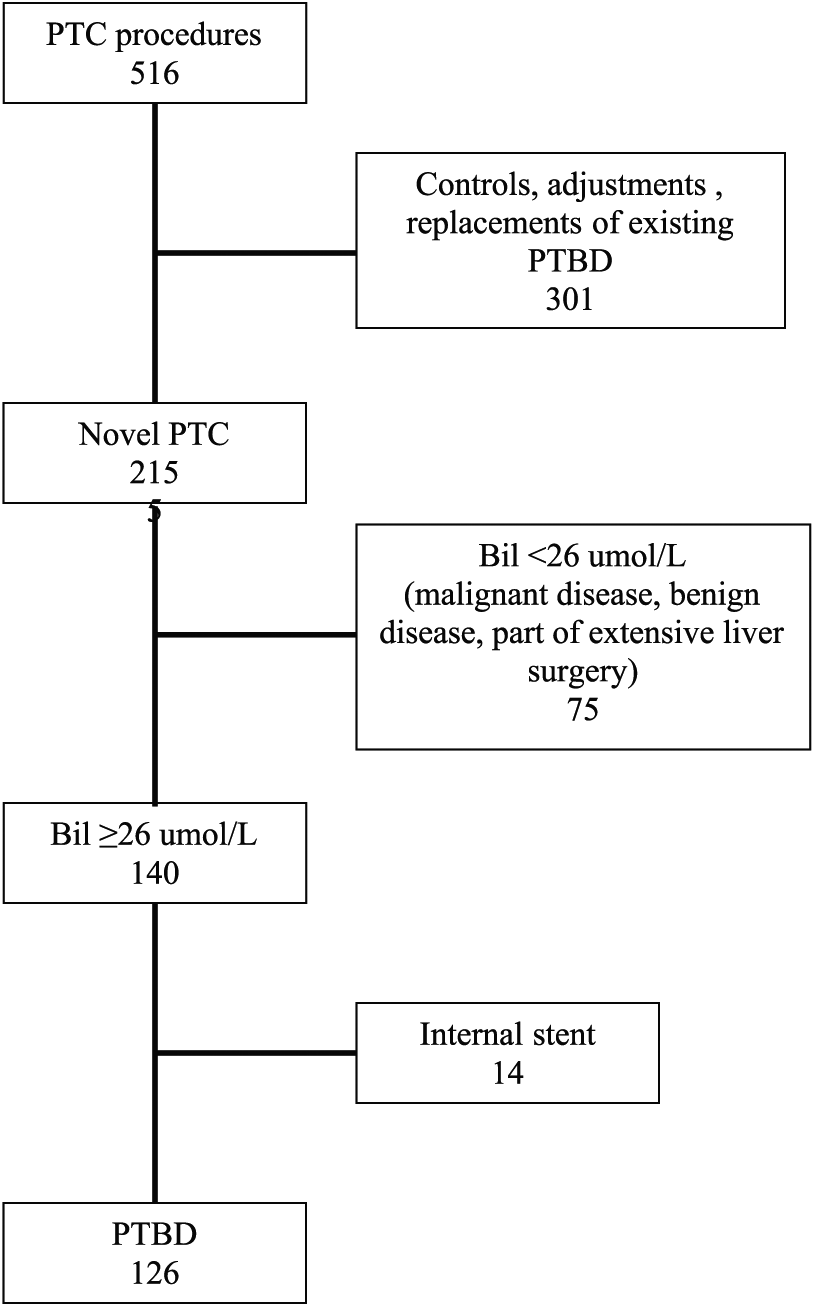
Flow chart showing the number of patients undergoing percutaneous transhepatic cholangiography (PTC) from June 2010 to June 2013, and how 126 patients with permanent external drainage (PTBD) and 14 patients with temporary external drainage and later internal drainage became included in the study.
Magnetic resonance imaging (MRI) was used to determine the level of biliary obstruction and to assess the amount of functional liver parenchyma that could be drained. Puncture of the bile ducts close to the liver hilus was guided by ultrasound. Radiological classification of the biliary obstruction was discussed in separate sessions until consensus was obtained. It comprised intrahepatic, extrahepatic, and combined intra- and extrahepatic obstruction.
Ethics
This report was part of a quality control and written permission to the study design was given by the chairman at the Department of Surgery, Linköping University hospital (dnr CKOC-2014-00172).
Statistical Analysis
Differences between patient groups were tested with a Z-test and comparisons of the distribution between the different groups with a two-sided chi-square test both taking a p-value of 5% as significant.
Results
Manifest or suspected malignant disease and bilirubin ≥26 µmol/L in plasma were identified in 140 patients (75 males, 65 females). The median age was 70 years (range, 33–91 years) (Table 1). In all, 67% had ASA classification II–III. Some 126 patients continued with a remaining external PTBD while 14 patients received an internal drainage, but these had a temporary external drainage either at the stenting procedure or later (Fig. 1). According to the X-ray findings, the biliary obstruction was extrahepatic in 16 patients (12.7%), intrahepatic in 59 patients (46.8%), and combined extra- and intrahepatic in 60 patients (47.6%). In five patients (4.0%), it could not be classified (Table 1).
Jaundice was the initial symptom of the malignant disease in 62 patients (44%). The median value of bilirubin in plasma before PTBD was 237 µmol/L (range, 31–634). Within the first week after PTBD, the bilirubin level decreased to 180 µmol/L (range, 17–545) and 14 days after PTBD it was further decreased to 112 µmol/L (range, 16–443). After that there was only a small decrease with a median value of 103 µmol/L. The majority of the patients decreased their bilirubin value in plasma but only 35 patients (25%) reached a level below 52 mmol/L (double upper reference value) (Fig. 2). In total, 12 of these patients received neoadjuvant chemotherapy and 4 patients also received postoperative chemotherapy. Two patients went into remission and the others had a median survival of 9 months, which was 3 months more than the total patient material (n = 126). Some 100 patients had a bilirubin value higher than 52 mmol/L after PTBD (Fig. 2).
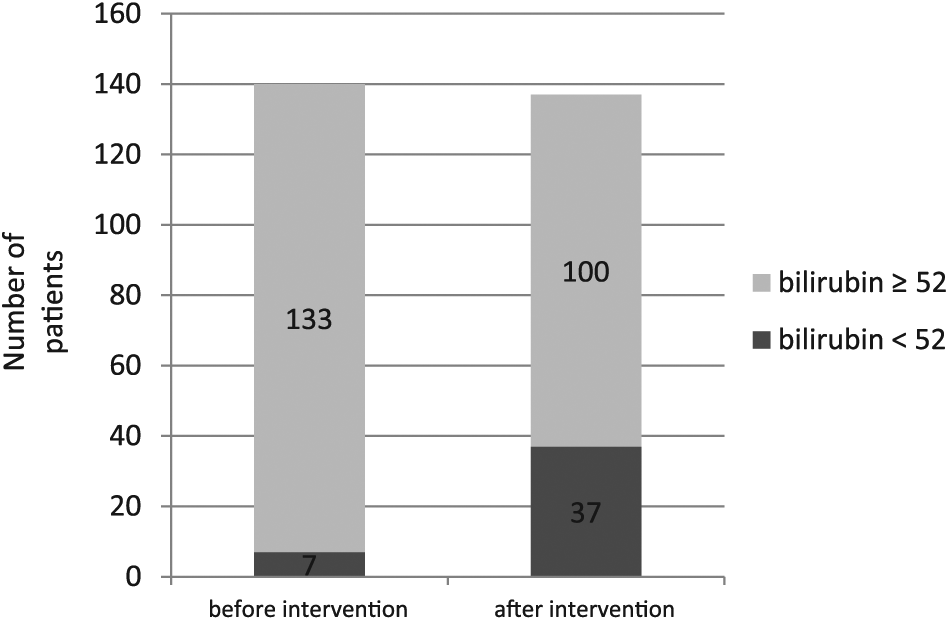
Bilirubin in plasma before PTBD (left column) and after PTBD (right column). Gray color depicts number of patients with a bilirubin value of ≥52 µmol/L and black color a value of <52 µmol/L. Three patients are missing in the bar showing bilirubin after PTBD.
In patients with permanent PTBD, the median bilirubin value did not differ between the 34 patients (27%) with pruritus (279 µmol/L) and the 92 patients without pruritus (236 mmol/L). After PTBD, pruritus was relieved in 19 patients (56%). The bilirubin value was not correlated to pruritus or to survival.
Some 269 adverse events (AE/complications) were documented. Most common were pain demanding increased dose of opioids, local discomfort, and cholangitis/septicemia (Table 2).
Distribution of 269 adverse events/complications within 14 days after external PTBD.
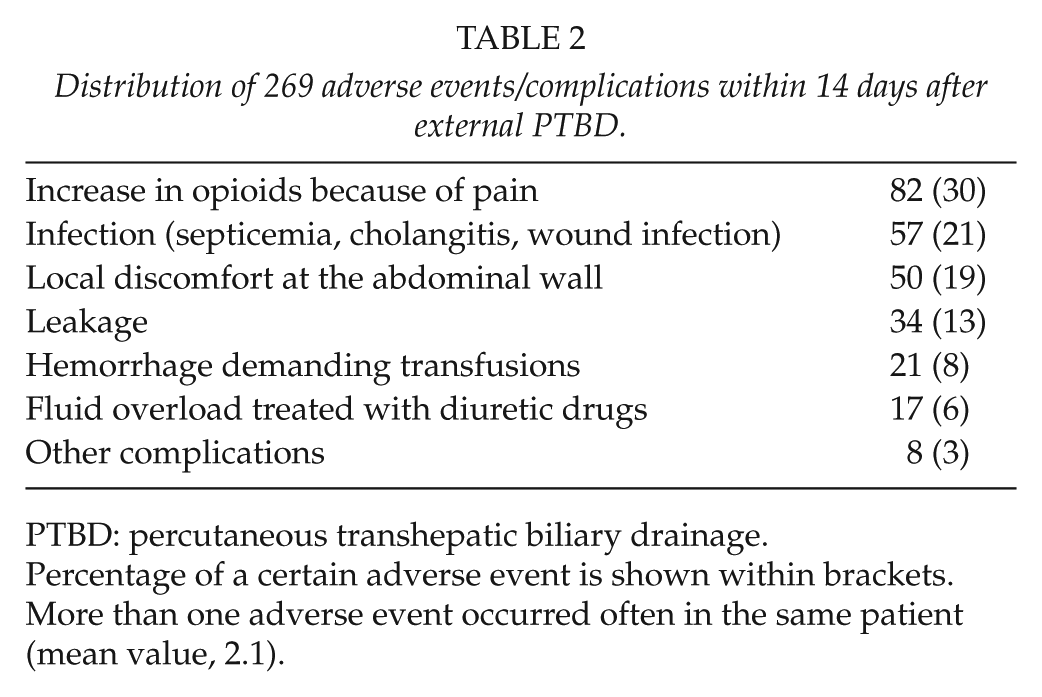
PTBD: percutaneous transhepatic biliary drainage.
Percentage of a certain adverse event is shown within brackets. More than one adverse event occurred often in the same patient (mean value, 2.1).
AE/complications associated with increased demand of opioid treatment were documented in 67 of 126 patients (53.2%) and 12 patients (9.5%) were treated with increased dose of opioids without any documented AE (Table 3). Local discomfort was documented in 21 patients (19%). If patients with local discomfort or increased doses of opioids were excluded, 36.5% of the patients developed an AE/complication. No AE was documented in 44 patients (34.9%). Each of these patients had 2.1 AE/complications in mean. Early mortality after PTBD was high in this palliative cohort. Within 14 days, 20 patients (16%) had died, and after 3 months 50% (n = 70) had died due to the malignant disease. The survival is shown in Fig. 3.
Number of patients (n = 67) with some adverse events/complications and increased demand of opioids after PTBD.
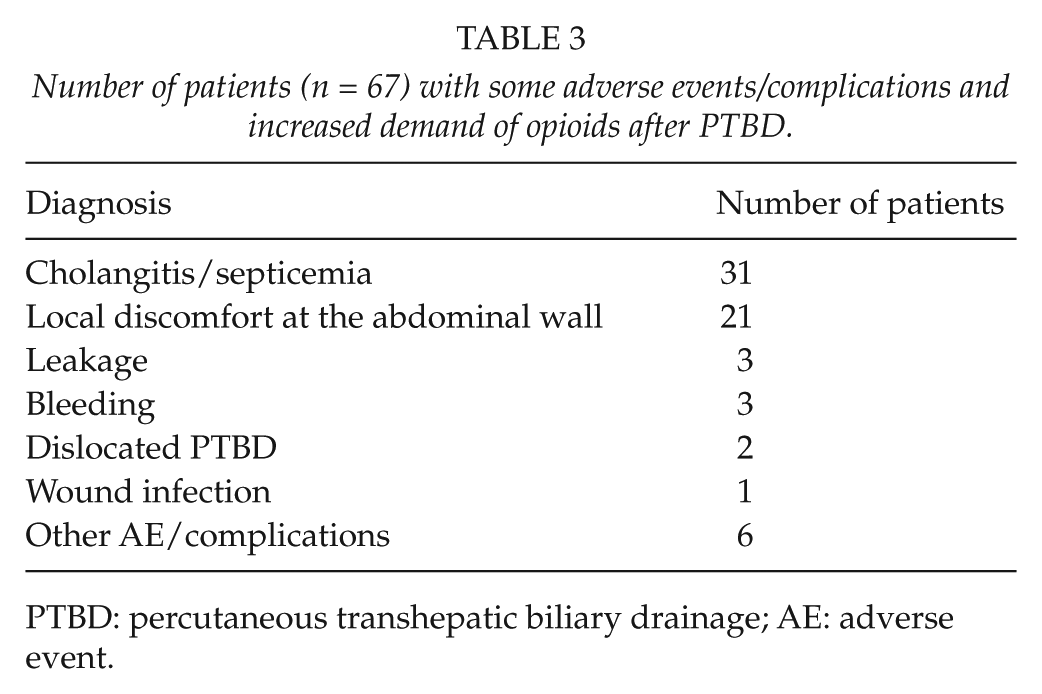
PTBD: percutaneous transhepatic biliary drainage; AE: adverse event.
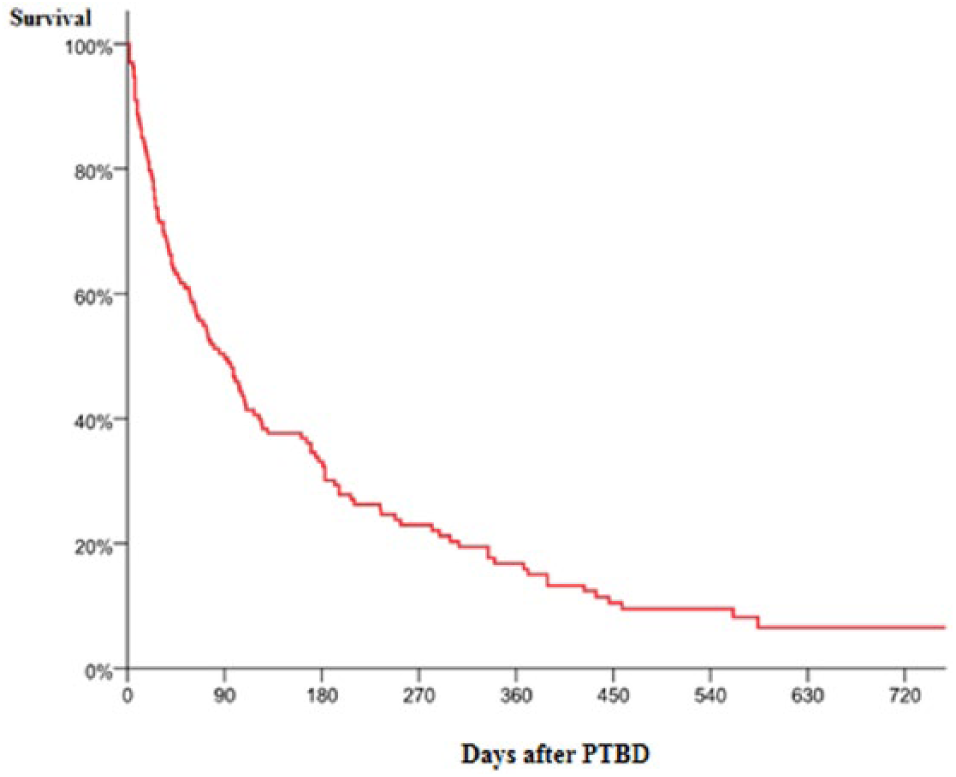
Survival in 140 patients (100%) who were followed up after receiving a biliary drainage due to advanced malignant disease and hyperbilirubinemia. Half of them (n = 70) were alive after 90 days, 30% (n = 42) after 180 days, and 20% (n = 28) after 270 days.
Antibiotic prophylaxis was given to 69 patients of whom 32% (n = 22) developed some infectious complication (cholangitis, septicemia, wound infection), which is significantly lower than in patients without prophylaxis (n = 71) where the corresponding figure was 51% (p = 0.02). The 2-week mortality did not differ (16% vs 15%).
In 90% of the patients, there was no documented information in the case records about expected possible positive and negative effects of PTBD.
Discussion
It has previously been reported that biliary drainage may improve immune function, improve nutritional status, and reduce the risk of infection in patients with biliary obstruction (9, 10). However, it has been shown in animal experiments that endotoxemia often persists after external biliary drainage (2). In a recent systematic review on palliation of advanced malignant hilar obstruction, endoscopic drainage was compared with PTBD. It was concluded that PTBD was associated with higher rates of successful biliary drainage and lower rates of cholangitis. Endoscopic drainage had lower rates of bleeding complications, but overall there was no difference in AEs (11). However, there are several publications reporting that endoscopic approach is the optimal method, particularly in distal obstruction (8, 11–13).
Our and other studies report a significant decrease in plasma bilirubin during the first week after PTBD (5, 14, 15). Pruritus is often out of proportion to the serum bilirubin level and its pathogenesis is poorly understood (13). The intensity of pruritus was decreased in half of our patients after PTBD, but the correlation between pruritus and the bilirubin level in plasma seems to be weak. We agree with other authors that jaundice should not by itself be an indication for palliative PTBD except when the aim is to prepare the patient for chemotherapy as the catheters not seldom require maintenance and adjustments to lifestyle (3, 11). On the other hand, when the indication for drainage is relief of pruritus, drainage of even one segment of the liver may reduce the symptoms (3).
Some kind of AE after external PTBD was common and early mortality was high in our patient group with advanced malignant disease, which has also been reported by others (10, 14–16). In most other reports, pain associated with local discomfort or increased demand of opioid treatment has not been included among complications or AEs (16–20). However, a biliary drainage can cause significant pain (5, 11, 21). When this group was excluded in our study, the complication rate was 34%, which is in agreement with other reports (16–17). In a large study comprising both patients with benign disease and patients with malignant disease receiving external drainage or stent, there were complications associated with the PTBD in 10%. However, only bleeding, infection, and bile leak were included. A score based on a multivariate analysis of independent predictors for those complications was suggested (low albumin level, bilirubin higher than 300 mmol/L, high WBC, low hemoglobin, high C-reactive protein, and proceeding to stent) (20).
Cholestasis is associated with decreased effectiveness of clearance of bacteria and increased susceptibility to systemic infection (22). Cholangitis usually occurs after manipulation of the biliary tree with concomitant direct or enteric contamination (3). It has been reported that about half of the patients with biliary obstruction have positive bile cultures and biliary infection is a major risk factor after PTBD (23, 24). Broad-spectrum antibiotic prophylaxis should therefore be recommended to all patients undergoing PTBD (13, 21, 23, 25). In our study, unfortunately only half of the patients received antibiotic prophylaxis and once more it was shown that patients with antibiotic prophylaxis had a significantly lower risk of getting infectious complications compared with those without antibiotic prophylaxis.
PTBD is most successful in patients with obstruction of the bile duct below the insertion of the cystic duct. On the other hand, endoscopic treatment with metallic stents is favored in these cases because they offer complete drainage without the inconvenience of an external catheter. Previous attempts with endoscopic drainage of the biliary ducts had been done in some of our patients with varying location of the obstruction before the PTBD was performed. According to the high risk of AEs, PTBD should not automatically be a second-line treatment until endoscopic treatment with rendezvous technique has been attempted (26–29). Today, PTBD still has a role in high duct obstruction (Bismuth type III–IV) (6, 9, 11, 16). A recent study compared percutaneous transhepatic biliary stenting (PTBS) with endoscopic stenting in advanced malignancy (30). There was no significant difference in effectiveness of biliary drainage or survival time, and the PTBS group had lower costs. The early complication rate was lower in the PTBS group and the rate of late complications did not differ.
Hopefully, more than the documented 10% of the patients in our study received information of what could be expected after PTBD. Such documentation should include a careful description of the indication for PTBD and which palliation can be expected. Risks for inadequate effect of PTBD on jaundice, pruritus, various AEs—such as pain, bleeding, infectious complications, and leakage—and also death should be discussed with the palliative patient.
Footnotes
Acknowledgements
We want to thank Victoria Fomichov, Regional Cancer Center southeast region, Sweden, for statistical advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.