
Abstract
Background and Aims:
A right hemicolectomy is a technically demanding procedure and the quality of the operation influences the short- and long-term outcomes. An increasing number of certified centers employ surgeons who are specialized in this procedure. Residency training is obligatory, but trainee surgeons often cannot perform technically demanding procedures because of economical and certification requirements imposed on the center. This study was performed to evaluate the suitability of right hemicolectomy as a training procedure.
Material and Methods:
Between 2009 and 2013, 133 patients received a right hemicolectomy during cancer treatment. Patient data were analyzed in two cohorts: cohort 1 contained 90 patients who were operated by a resident under supervision, and cohort 2 included 43 patients who were operated by a specialized senior surgeon. Outcome and safety were evaluated by mortality rate, anastomotic leakage, complication rate, and operation time. The resection status and the number of resected lymph nodes were surrogate parameters for oncological quality. Gender, age, American Society of Anesthesiologists classification, body mass index, and general risk factors were compared in both cohorts.
Results:
There was no significant difference in the rate of anastomotic leakage between the two groups (p = 0.799). Oncological criteria were met in both cohorts and the oncological quality was similar between groups. Furthermore, there were no significant differences in risk factors, operating time, postoperative complications, and mortality between the groups.
Conclusion:
Oncological open right hemicolectomy is a safe and suitable training procedure for residency training under standardized conditions.
Keywords
Introduction
Colorectal tumors are very malignant and have to be treated surgically by radical resection, including the lymph nodes (1). The skill of the surgeon is a key prognostic factor because the quality of the operation affects both short- and long-term surgical and oncologic outcomes (2). Therefore, surgeons must be well qualified and continuously trained to perform this procedure (2).
In recent years, exact dissection along the embryological layer with radical lymphadenectomy up to the mesenteric vessels (complete mesocolic excision (CME)) has become a focus of attention (3). Analogous to total mesorectal excision (TME) for rectal cancer, this surgical procedure has significantly improved the oncological outcome compared with conventional lymphadenectomy (3–5). However, CME is a technically demanding procedure.
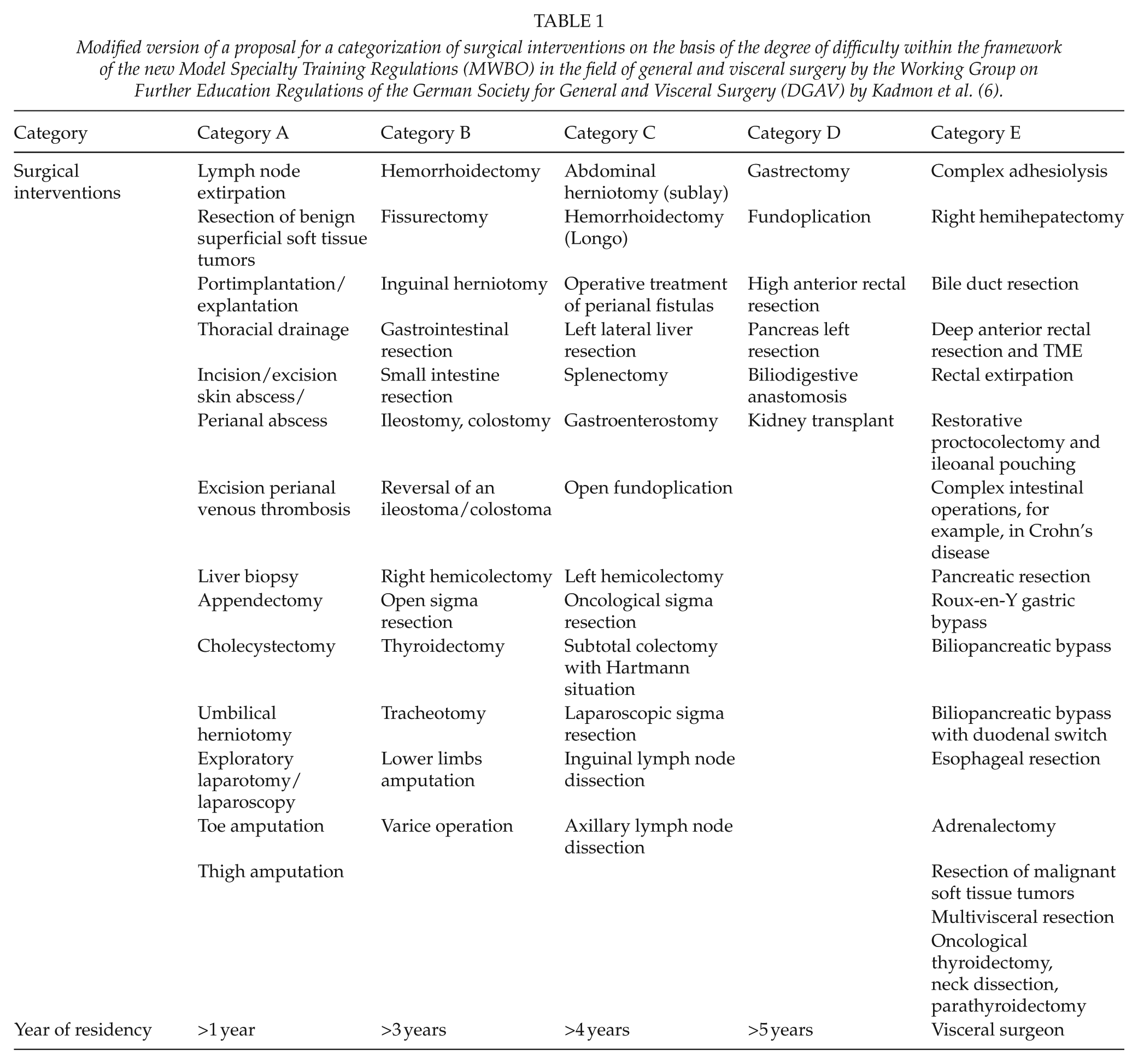
Kadmon et al. (6) have discussed competence-based training concepts and suggested that training procedures be categorized according to their difficulty (Table 1). Open right hemicolectomy is classified as a category B procedure and is performed from the third year of surgical training in our department (6). Nevertheless, the safety and oncological outcomes of this operation as a training procedure have not been validated. To address this, the aim of this study was to retrospectively evaluate whether oncological open right hemicolectomy has been a safe and suitable procedure for residency training in our department.
Modified version of a proposal for a categorization of surgical interventions on the basis of the degree of difficulty within the framework of the new Model Specialty Training Regulations (MWBO) in the field of general and visceral surgery by the Working Group on Further Education Regulations of the German Society for General and Visceral Surgery (DGAV) by Kadmon et al. (6).
Materials and Methods
Patients
We evaluated the data of 133 patients with ascending colon carcinoma who received an open right hemicolectomy at our department between 2009 and 2013. Data were acquired in a specific database and evaluated retrospectively. For the purpose of this study, patients were allocated to two cohorts: cohort 1 included 90 patients who were operated by one of 19 residents under supervision, and cohort 2 included 43 patients who were operated by one of four specialized senior surgeons. The scheduling of the surgical team and the patient was randomly by means of organizational or duty-plan-dependent presence of the respective operators. Inclusion criteria included elective surgery of ascending colon carcinoma, no distant metastases, and curative intention of the surgery. Exclusion criteria included emergency surgery, palliative surgery, and stapler anastomosis instead of hand-sewn anastomoses. In this patient population, 71 (53.4%) were male and 62 (46.6%) were female. The average age was 72 years (male: 70.6 years; female: 73.6 years; range: 43–99 years).
Surgical procedure
Open right hemicolectomy was performed by radical resection of the right ascending colon, including a radical lymphadenectomy up to the central ligation of the right colic artery and right colic vein, close to the upper mesenteric vein. Anastomosis was performed using a single-layer continuous hand-sewn end-to-side ileotransversostomy.
Outcome parameters
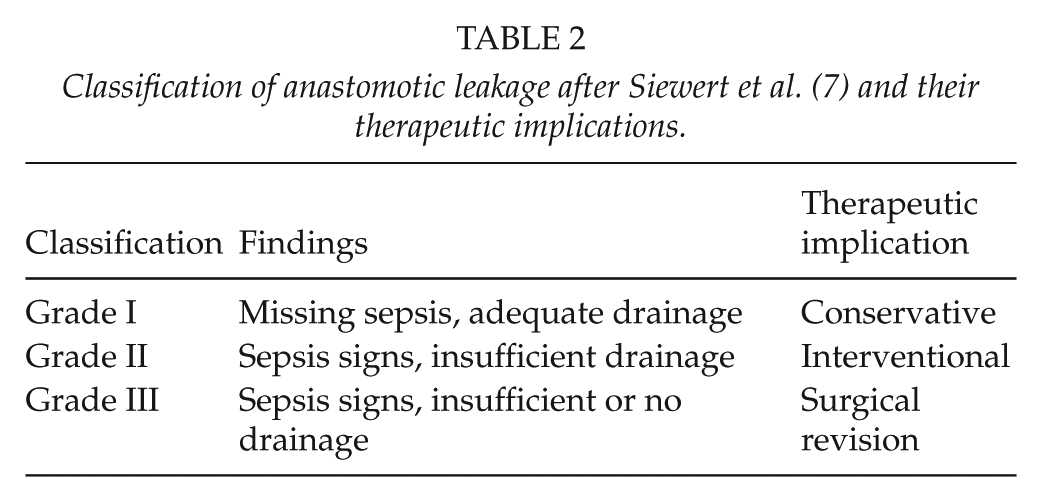
Mortality rate, complication rate, anastomotic leakage rate, and operation time were analyzed as surrogate parameters of surgical quality. The rate of anastomotic leakage was classified into grade I–III (Table 2) according to Siewert et al. (7). Postoperative complications were analyzed based on the classification of Younan et al. (8) as follows: grade I: no complications, grade II: minor complications (e.g. wound infection, urinary tract infection, paralytic ileus, deep vein thrombosis), and grade III: major complications (reoperation, intensive care unit (ICU) care, interventions). The operative time was measured in minutes from the cut-seam time onwards.
Classification of anastomotic leakage after Siewert et al. (7) and their therapeutic implications.
Oncological quality was evaluated by the pathohistological resection status and lymph node status according to the pathological reports. Oncological criteria were fulfilled by a margin-free status (R0) and at least 12 resected lymph nodes. The circumferential safety margin was considered negative (R0) if it was 1 mm or more. The circumferential safety margin was positive (R1) if it was less than 1 mm (1).
Other parameters included risk factors for surgical complications, such as the American Society of Anesthesiologists (ASA) classification, the pre-operative body mass index (BMI), previous abdominal surgery, peripheral arterial vascular disease, smoking, and diabetes mellitus (9–11). We defined appendectomy, cholecystectomy, hysterectomy, adnexectomy, cesarean section, hernia operations, and transurethral prostatectomy as minor previous operations. Splenectomy, pancreatic resections, nephrectomy, operation of an abdominal aortic aneurysm, and large or small bowel resections were considered major operations.
Statistics
Data were collected and analyzed using Statistical Package for Social Sciences software, version 16.0. Fisher’s exact test was used to compare binary data from unrelated samples. The chi-square test was used when comparing more than two variables. Ordinal categorical variables were compared using the Mantel–Haenszel test. In the absence of normal distribution, the non-parametric Mann–Whitney U-test was performed. The level of significance was set at p < 0.05.
Results
A total of 153 patients underwent oncological open right hemicolectomy to treat an adenocarcinoma in the ascending colon between 2009 and 2013. A total of 20 patients (13%) were excluded because of an emergency operation, stapler anastomosis, or palliative indication. Cohort 1 (n = 90) included 44 females (48.9%) and 46 males (51.1%), and the mean age was 71.8 years (range: 46–90 years). Cohort 2 (n = 43) contained 18 females (41.9%) and 25 males (58.1%), and the mean age was 72.2 years (range: 43–99 years). There were no significant differences in gender (p = 0.447) or age (p = 0.870) between the groups.
Following surgery, only one patient died (overall surgery-related mortality rate: 0.8%). This patient was from cohort 1 (subgroup specificity: n = 1/90, 1.1%) and died due to sepsis after anastomotic leakage. There was no significant difference in overall mortality rate between the two cohorts (p = 0.544).
The nonsurgical-related mortality rate was 3.3% in cohort 1 (n = 3/90) and 7.0% in cohort 2 (n = 3/43). In cohort 1, one patient died due to decompensated liver cirrhosis and two patients died from an acute myocardial infarction. In cohort 2, one patient died from fulminant pancreatitis, one patient from acute myocardial infarction, and one patient from global respiratory insufficiency.
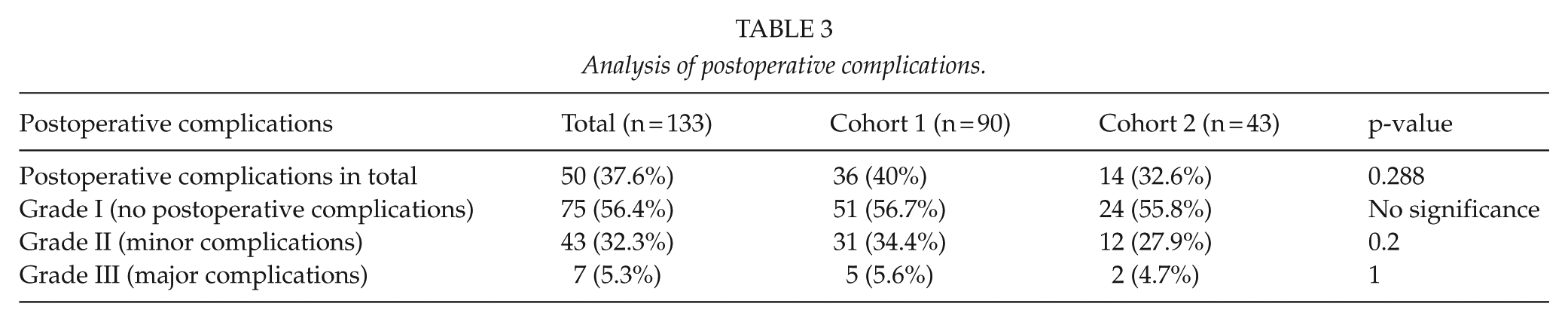
The rate of postoperative complications (minor and major) was 37.6% in the total study population (n = 50/133). The postoperative complication rate was 40% (n = 36/90) in cohort 1 and 32.6% (n = 14/43) in cohort 2. The rates of grade II and grade III complications did not differ significantly between the two groups (grade II: p = 0.2; grade III: p = 1.0). Furthermore, there was no significant difference in the total complication rate between the two cohorts (p = 0.288) (Table 3).
Analysis of postoperative complications.
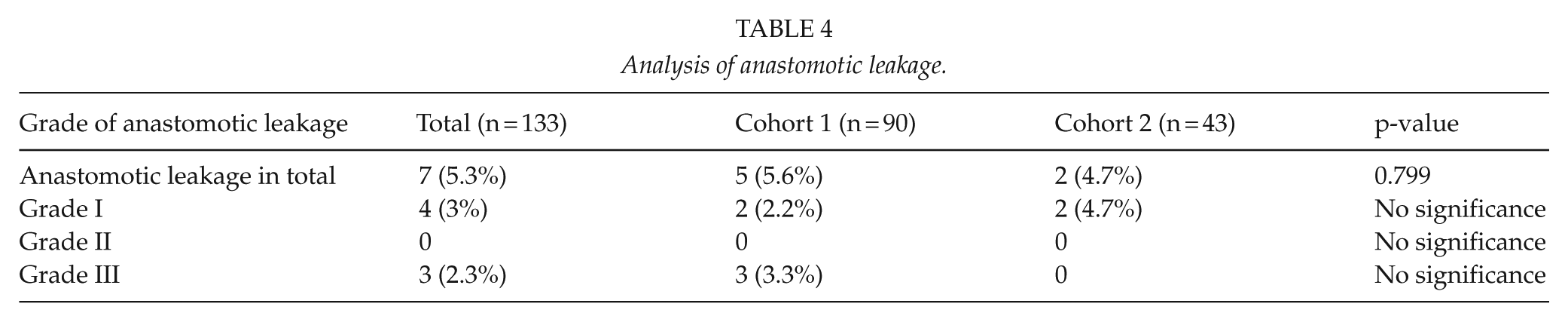
The overall anastomotic leakage rate was 5.3% (n = 7/133). Subgroup analysis revealed an anastomotic leakage rate of 5.6% (n = 5/90) in cohort 1 and 4.7% (n = 2/43) in cohort 2 (Table 2). In cohort 1, two patients had grade I anastomotic leakages and three patients had grade III anastomotic leakages. In cohort 2, two patients had grade 2 anastomotic leakages. There was no significant difference in anastomotic leakage between cohort 1 and 2 (p = 0.799) (Table 4).
Analysis of anastomotic leakage.
Tumor-free resection was achieved in all patients from both cohorts. In all, 12 or more lymph nodes were resected in 89/90 (98.9%) patients from cohort 1 and 42/43 (97.7%) patients in cohort 2 (p = 0.544).
The ASA classification did not differ significantly between the two groups (p = 0.131). The BMI was 26.5 ± 4.3 in cohort 1 and 26.2 ± 7.2 in cohort 2 (p = 0.507). A total of 79 patients had received previous abdominal surgery (n = 79/133; 59.4%). In total, 48 of these patients had minor surgery (n = 48/133; 36.1%) and 31 received major operations (n = 31/133; 23.3%). In all, 52 of the patients who received previous surgery were in cohort 1 (n = 52/90; 57.8%; minor: n = 34/90; 37.8%; major: n = 18/90, 20%), while 27 patients were from cohort 2 (n = 27/43; 62.8%; minor: 14/43; 32.6%; major: 13/43; 30.2%). The number and type of previous operations did not differ significantly between the cohorts (p = 0.426). Risk factors for wound healing were not significantly different between cohort 1 and 2 (peripheral arterial vascular disease: p = 0.544, smoking: p = 0.468, diabetes mellitus: p = 0.288) (Table 5). Regarding the postoperative TNM/UICC (Union for International Cancer Control) staging system, there was no significance between both cohorts (p = 0.670).
Analysis of risk factors for wound healing, perioperative data.
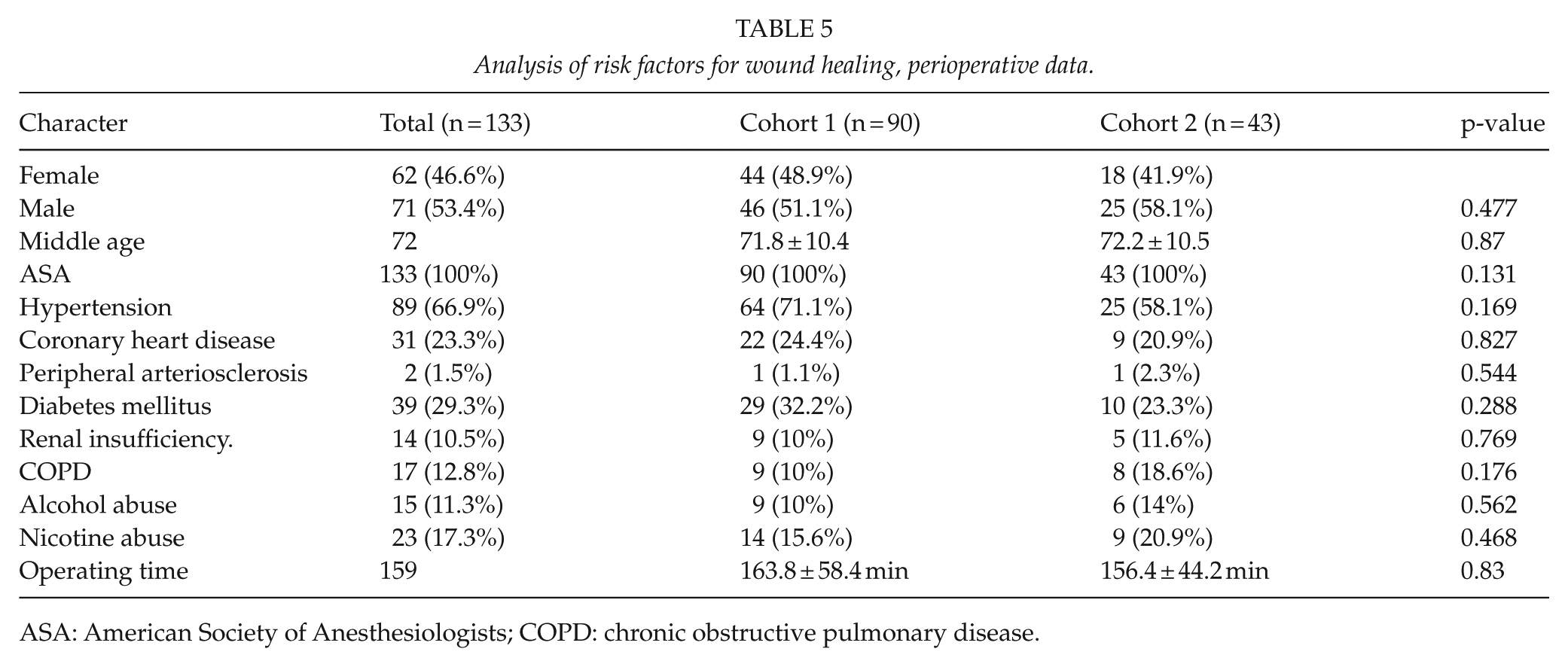
ASA: American Society of Anesthesiologists; COPD: chronic obstructive pulmonary disease.
The average duration of the operation was approximately 160 min in both cohorts (cohort 1: 163.8 ± 58.4 min; range, 57–285 min; cohort 2: 156.4 ± 44.2 min; range, 89–347 min). There was no significant difference in operation time between the two cohorts (p = 0.83) (Table 5).
Discussion
Surgical residency training is a controversial topic. Expertise is acquired mainly through supervised training in the operating room with a specialist or senior operator, while some skills can be self-taught in training laboratories outside the operating theater. Operational training is characterized into three phases. In the first phase, the resident assists the specialist or senior physician and studies the individual operation steps. In the second phase of training, the resident acquires more surgical competency and begins to perform individual surgical steps and learn basic skills, including the use of instruments, different suture techniques, and the principles of preparation. Depending on the educational level of the individual resident, complete operations are carried out under supervision in the third training phase (12).
Nowadays, there is considerable economic pressure to increase the workload and reduce operation time. This has reduced the capacity for teaching in most centers. Furthermore, quality certifications have limited the number of surgeons allowed to perform certain procedures. It is generally assumed that trainee surgeons require longer to complete a procedure, leading to poorer outcomes and higher costs. In this study, we demonstrated that oncological open right hemicolectomy is a safe and suitable procedure for residency training in our department. The safety and feasibility of procedures performed by resident surgeons have been validated in the past (13), but data from oncological and colorectal surgical procedures are still lacking.
Worthy of discussion is the exclusion of laparoscopic right hemicolectomy in this study because this procedure may be regarded as the standard procedure in a range of other departments or countries. In our opinion, right hemicolectomy represents an ideal procedure for teaching oncological colonic resections because it entails a steeper learning curve than laparoscopic colonic resections. Furthermore, several randomized trials and meta-analyses have revealed no oncological differences between laparoscopic and open surgery of carcinomas in the ascending colon (14, 15). In two prospective studies, Braga et al. (16) and Veenhof et al. (17) demonstrated a poor cost–benefit effect and no advantages of laparoscopic right hemicolectomy compared with an open surgical approach. Therefore, we routinely operate carcinomas of the ascending colon with an open right hemicolectomy in our department.
The rate of postoperative complications and mortality were similar following right hemicolectomies performed by trainee surgeons and senior operators. The postoperative complication rate of 37% was slightly higher than reported in a recent study (29%) (18). This may be explained by the smaller cohorts analyzed in our study. The rate of anastomotic leakages for the entire patient population was 5.3%, which is difficult to compare with previous literature. Frasson et al. (18) reported an anastomotic leakage rate of 8.4% following right hemicolectomy in a multivariant analysis. Other authors have found leakage rates between 1% and 3% for different types of colonic anastomoses (19). Our leakage rate of 5.3% is within the scope of the published literature. We observed no differences in the rate of anastomotic leakage (p = 0.799) or the severity of leakage between cohorts. In our opinion, this was because all procedures performed by trainee surgeons were properly instructed by an experienced surgeon, who corrected technical failures such as too much tension or too little blood supply during the anastomosis.
Demographics and other risk factors were similar between the two cohorts, therefore were unlikely to have affected the outcomes.
As expected, operations performed by residents took longer than those performed by senior physicians. However, these differences were small and not significant. This illustrates that resident surgeons operate faster after gaining more experience (20).
There were some limitations to this study that should be considered. This was a retrospective single-center study; therefore, the allocation of patients to cohorts and procedural characteristics were not random and may be biased. However, there were no differences in demographic data or risk factors between the groups indicating no general pre-selection. It would be interesting to validate our findings in a multi-center study with larger cohorts in the future.
Conclusion
Resident surgical trainees can perform an open right hemicolectomy with similar outcomes (mortality, complications, and oncological safety) as those performed by a senior physician. Our findings justify further validation by larger, multi-center studies.
Footnotes
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was in accordance with the Declaration of Helsinki and the local Ethics Committee of Mainz, Germany.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.