
Abstract
Background and Aims:
To describe the incidence of and risk factors for postoperative infections and the correlation between postoperative hyperglycemia despite tight blood glucose control with infectious and other complications after contemporary cardiac surgery.
Material and Methods:
The study comprised 1356 consecutive adult patients who underwent cardiac surgery between January 2013 and December 2014 and were followed up for 6 months. Patients surviving the first 2 days were included in the analysis. Preoperative demographic information, medical history, procedural details, and the postoperative course were recorded. The target range for blood glucose levels was 4–7 mmol/L and repeated arterial blood samples were obtained during the intensive care unit stay. The associations of blood glucose levels during the first postoperative day and the occurrence of postoperative infections and other significant complications were analyzed.
Results:
Of the study cohort, 9.8% developed infectious complications which were classified as major surgical site infections in 2.2%, minor surgical site infections in 1.1%, lung infections in 2.0%, unclear fever or bacteremia in 0.3%, cannula or catheter related in 2.6%, multiple in 1.5%, and other in 0.2%. The incidence of deep sternal wound infection was 2.0%. Repeated hyperglycemia occurred in 39.7% of patients and was associated with increased rates of postoperative infections, 12.1% versus 8.2%, p = 0.019; stroke, 4.9% versus 1.5%, p < 0.001; and mortality, 6.1% versus 2.1%, p < 0.001, when compared to patients with single or no hyperglycemia.
Conclusion:
Every 10th patient develops infectious complications after cardiac surgery. Repeated hyperglycemia is associated with increased rates of infectious complications, stroke, and mortality.
Keywords
Introduction
Infectious complications are a significant cause of morbidity, mortality, and increased healthcare costs after major procedures such as cardiac surgery. Besides operation-related factors, including extensive operations, long procedure times, and the use of cardiopulmonary bypass, cardiac surgery patients are subjected to prolonged intubation and mechanical ventilation, numerous vascular and urinary catheters, and chest tubes contributing to risk of postoperative infections. Furthermore, evolution of surgical techniques and cardiac anesthesia enables surgery in older patients presenting with substantial comorbidities, possibly influencing the susceptibility for postoperative complications. The incidence of postoperative infections in previous studies ranges from 5.0% to 14.1% (1, 2).
Acute physiologic stress induced by major surgery may elevate blood glucose levels even in patients without diabetes (3). Hyperglycemia, in turn, is associated with impaired wound healing, leukocyte function, and phagocytosis and has been found to increase rates of infectious complications after cardiac surgery (4, 5). Implementing tight glycemic control has been shown to reduce mortality and morbidity in a surgical intensive care unit (ICU) and the incidence of deep sternal wound infection (DSWI) after coronary artery bypass grafting (CABG) (6, 7). However, in the NICE-SUGAR study, comprising mostly non-surgical patients treated in the ICU, tight glucose control was associated with increased mortality (8).
The optimal target range for blood glucose levels after cardiac surgery remains unclear and merits further research. The aim of this study was to determine the incidence and risk factors of postoperative infections and the correlation between postoperative hyperglycemia with infectious and other complications after contemporary cardiac surgery, both in diabetic and nondiabetic patients.
Materials and Methods
Patients
This study was an analysis of a cohort of 1356 prospectively collected consecutive patients who underwent cardiac surgery in Heart Hospital, Tampere University Hospital, Tampere, Finland, between January 2013 and December 2014 and has been described in a previous study (9). The cohort included all adult open heart surgery performed at our clinic. Preoperative demographic information, previous medical history, and procedure-related details were recorded. The patients were treated according to clinical standards and were not subjected to any interventions for this study. Preoperative antimicrobial prophylaxis in all patients without contraindication for its use was Cefuroxime 3 g intravenously before surgical incision, and an additional 1.5 g was administered if the duration of the procedure exceeded 4 h. After surgery, all patients were followed up at the cardiac ICU at least until the morning of the first postoperative day, after which most patients were referred to either a regular or a high-dependency department. Mortalities and the occurrence of postoperative complications, including infections, need for reoperations, arrhythmias, and stroke, were recorded. The diagnosis of postoperative stroke was based on computed tomography performed in patients with clinical suspicion of intracranial pathology postoperatively and was confirmed by a neurologist in each case.
Diagnosis and Classification of Postoperative Infections
The occurrence and type of infectious complications, results of microbial culture, and the delay after which the first symptoms presented following surgery, both during the primary hospital stay and repeat hospitalizations within 6 months, were recorded. Patients surviving at least 48 h were included in the analysis, as those that did not survive the operation and the immediate postoperative period could not develop postoperative infections. Clinical signs of infection, such as local symptoms, fever, leukocytosis, and increase in the serum C-reactive protein concentration, along with positive findings in imaging studies and/or microbial culture were required for the diagnosis. Infectious complications were classified according to clinical presentation. DSWIs, empyema, and endocarditis after valve surgery were classified as major surgical site infections (SSI), while superficial sternal and other wound infections were classified as minor SSI. Other infections were considered as either pulmonary, cannula and catheter related, unclear fever or sepsis, or other infections. When more than one infectious complication occurred in the same patient, the patient was classified as having multiple infections and the delay in the onset of the first infection was recorded.
Glycemic Control and Measurements
During the ICU stay, repeated arterial blood samples were obtained every 4 h to follow up the hemoglobin, arterial gases, pH, glucose, and lactate levels (ABL90 FLEX blood gas analyzer; Radiometer Medical ApS, Brønshøj, Denmark). Additional blood samples were analyzed with a hand-held device (FreeStyle Lite; Abbott Diabetes Care Inc, Alameda, CA, USA) if frequent measurements were needed when values out of target range were treated. If insulin treatment was initiated in the ICU, we used a high initial bolus dose to provide enough insulin coverage to reduce blood glucose levels to the target range of 4–7 mmol/L followed by intravenous insulin infusion adjusted according to subsequent blood glucose measurements. This has been proved a safe and rapid manner to achieve compliance with the protocol (10). Any hypoglycemic values were treated promptly with glucose infusion. The amount of insulin given and blood glucose levels obtained by serial arterial blood samples during the first 24 h after surgery in the ICU were recorded. The associations between blood glucose levels and the amount of insulin given during the first 24 h and postoperative infections were analyzed using statistical methods. Type I and type II diabetics were grouped together in the analysis.
This is a descriptive study and consequently no preceding power analysis was performed. The study was carried out according to the Helsinki Declaration, and institutional review board approval was obtained. Statistical testing was done with SPSS 23.0 statistical software using the chi-square test and Fisher’s exact test to compare proportions in categorical data and the Mann–Whitney U test and the Kruskal–Wallis H test to compare the differences in medians between groups. Multivariable analysis was performed using binary logistic regression analysis and by including variables with statistically significant associations in univariable analysis. A p value <0.05 was considered statistically significant.
Results
Of the 1356 patients who underwent cardiac surgery during the study period, 1329 (98%) survived the first two postoperative days and were included in the analysis. The demographics of the study population are presented in Table 1. Altogether 7% of diabetics in the study population had type I diabetes. The main outcomes for the study patients include a combined 30-day and in-hospital mortality of 3.7%, a stroke rate of 2.9%, reoperations for bleeding and other complications in 13.2%, postoperative atrial fibrillation in 45.4%, and infectious complications in 9.8%. The median length of postoperative hospitalization was 6 (range 0–53) days including one patient referred for heart transplantation postoperatively.
Demographic data of study patients.
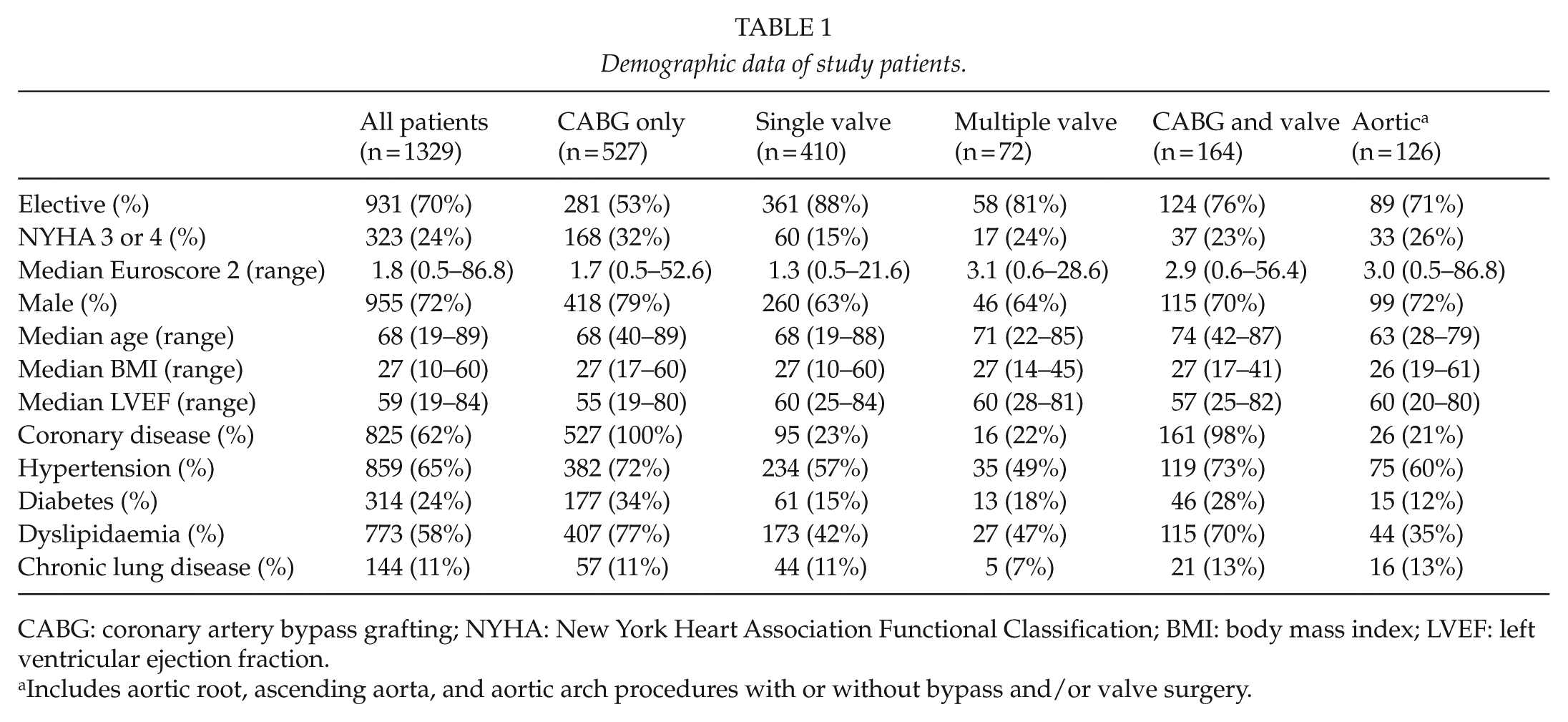
CABG: coronary artery bypass grafting; NYHA: New York Heart Association Functional Classification; BMI: body mass index; LVEF: left ventricular ejection fraction.
Includes aortic root, ascending aorta, and aortic arch procedures with or without bypass and/or valve surgery.
Postoperative Infections
The occurrence of postoperative infections and infection types is shown in Table 2, excluding unclear fever or bacteremia detected in 0.3% and other infections observed in 0.2% of patients. The most common pathogens detected per infection type are shown in Fig. 1. Increased infection rates were observed after urgent or emergency surgery, in patients with impaired left ventricular function, in those aged 70 years or more, and in patients with body mass index (BMI) ≥ 27 kg/m2. Pulmonary infections were more common in non-elective cases and in patients with higher New York Heart Association Functional Classification (NYHA) score and worse left ventricular ejection fraction. Higher BMI was associated with increased rates of SSIs, while females and patients aged 70 years or more showed higher rates of cannula and catheter-related infections. The rate of DSWI in the study was 2.0% and was not statistically significantly associated with the type of procedure.
The occurrence of postoperative infections and the most important infection types in study patients as well as the most important patient subgroups.
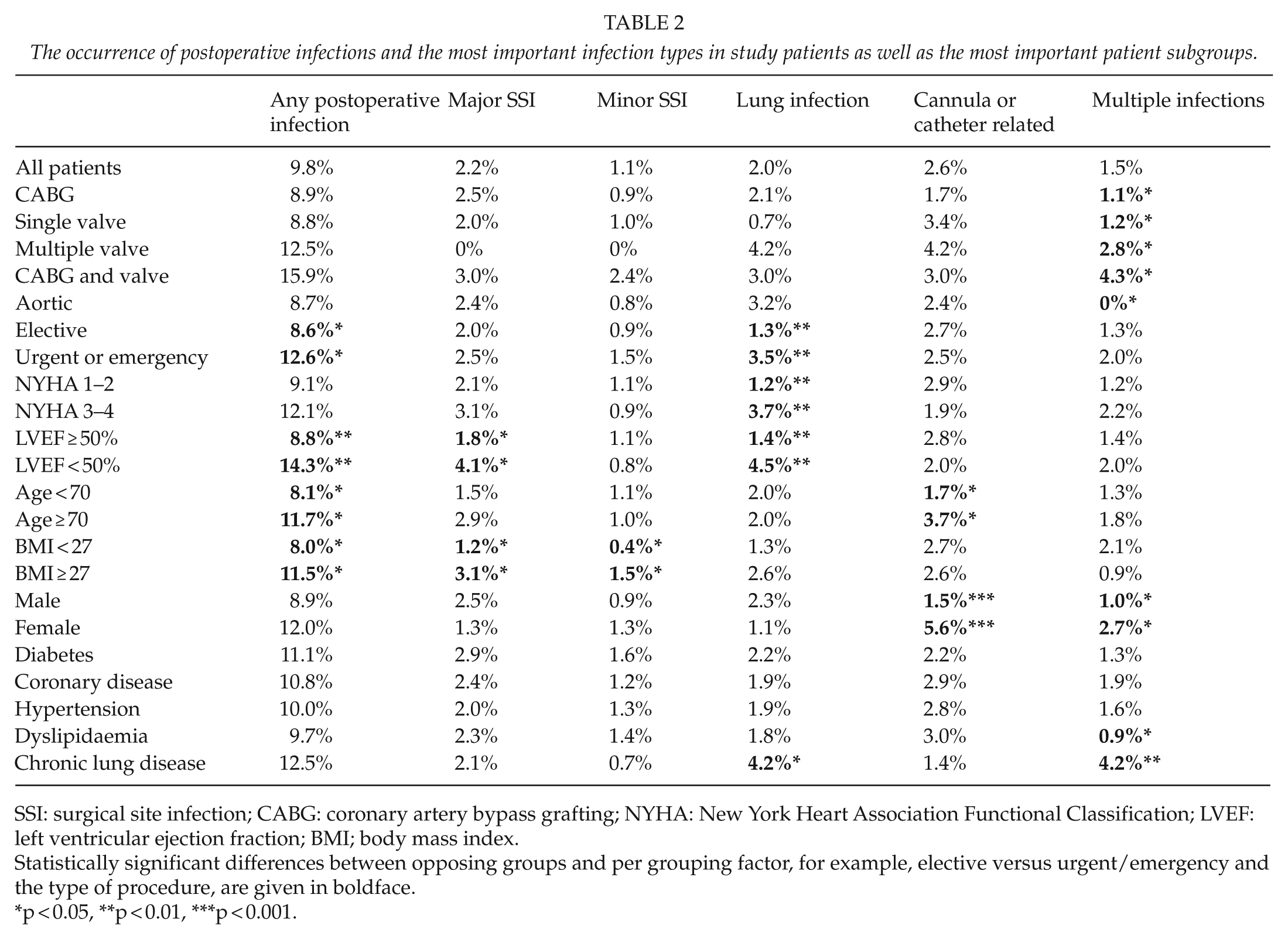
SSI: surgical site infection; CABG: coronary artery bypass grafting; NYHA: New York Heart Association Functional Classification; LVEF: left ventricular ejection fraction; BMI; body mass index.
Statistically significant differences between opposing groups and per grouping factor, for example, elective versus urgent/emergency and the type of procedure, are given in boldface.
p < 0.05, **p < 0.01, ***p < 0.001.
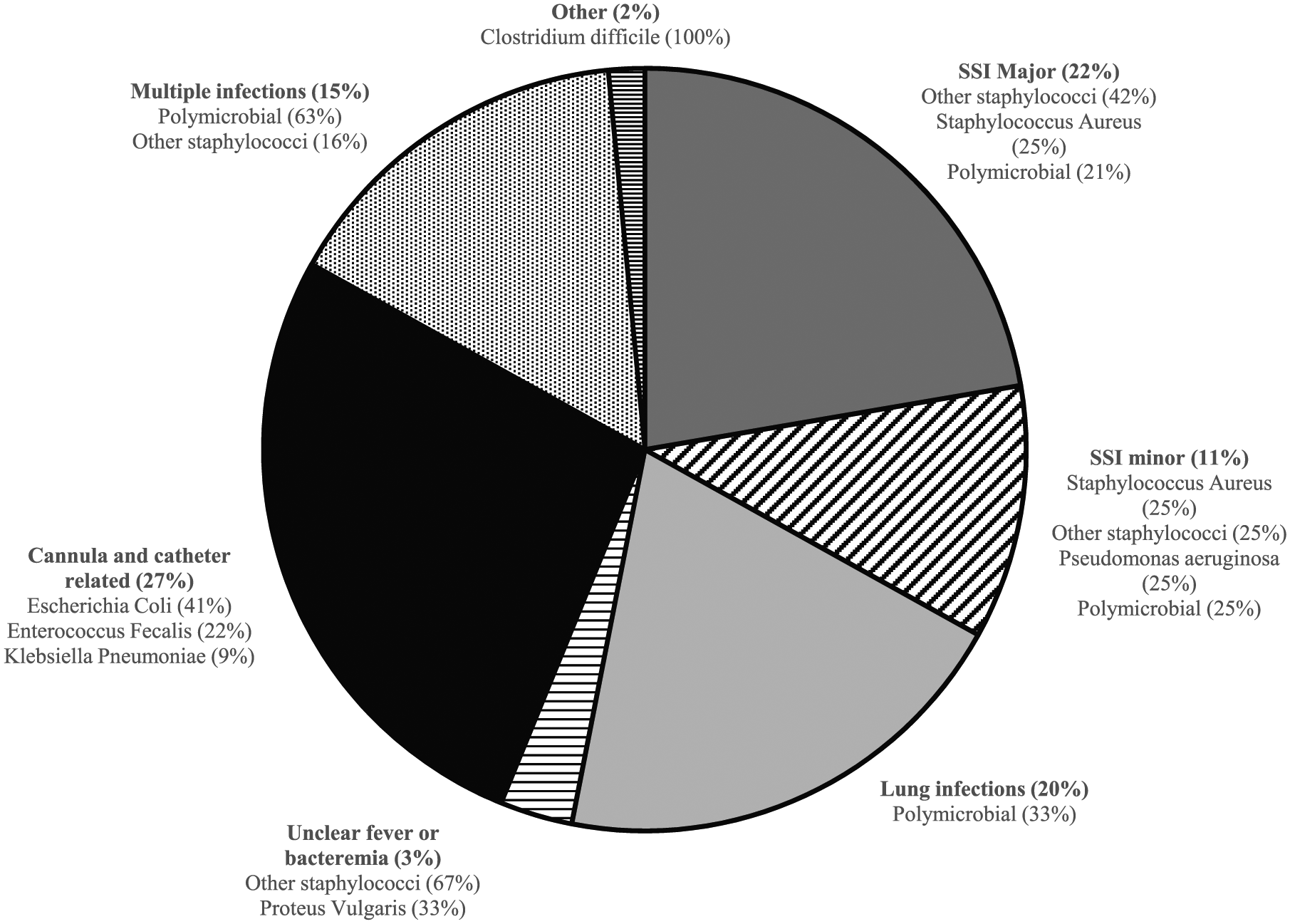
Classification and distribution of postoperative infectious complications and the most common pathogens detected by bacterial culture.
The median delay in the development of the first symptoms of postoperative infections was 6 (range: 0–174) days after surgery, 8 (range: 2–174) days for major SSI, including one prosthetic valve endocarditis presenting within 6 months after operation, 7 (range: 2–26) days for minor SSI, 3 (range: 1–10) days for lung infections, 8 (range: 4–15) days for unclear fever or bacteremia, 6 (range: 0–20) days for cannula- and catheter-related infections, 7 (range: 3–177) days for multiple infections, and 3 (range: 2–3) days for other infections (p < 0.001). Altogether 17 (1.3%) patients were readmitted due to infectious complications after primary referral or hospital discharge. In patients with postoperative infections, bacterial culture was positive in 97 (75%) and blood cultures in 18 (14%) patients. Patients who developed postoperative infections had longer postoperative length of intubation, median 5.8 versus 4.3 h, p < 0.001; longer primary ICU stay, median 1.7 versus 0.9 days, p < 0.001; longer hospitalization, median 11 versus 5 days, p < 0.001; and higher combined in-hospital and 30-day mortality, 10.8% versus 2.9%, p < 0.001. Mortality was 20.7% in patients with major SSI, 15.4% in patients with lung infections, 5.7% in patients with cannula- and catheter-related infections, 10% in patients with multiple infections, and 0% in patients with other infections (p < 0.001).
Hypoglycemia
Altogether 16 (1.2%) patients did not receive any insulin, and hypoglycemia did not develop in any of these patients. A total of 101 (7.6%) patients were hypoglycemic (B-gluc < 4 mmol/L) during the study, and of these, 91 (6.8%) patients were hypoglycemic once, 9 (0.7%) patients twice, and 1 (0.1%) patient three times. Hypoglycemia was not associated with the type of procedure performed or with postoperative infections, in-hospital mortality, stroke rate, length of hospitalization, or postoperative atrial fibrillation.
Hyperglycemia
Hyperglycemia (B-gluc > 7 mmol/L) occurred in 915 (68.8%) patients and was detected once in 388 (29.2%) patients, twice in 237 (17.8%) patients, and three or more times in 290 (21.8%) patients. Repeated hyperglycemia was observed more frequently in patients with diabetes than in other patients, 53% versus 36%, p < 0.001, respectively. The median BMI was also higher in patients with repeated hyperglycemia compared to other patients, 27.7 versus 26.3 kg/m2, p < 0.001, respectively. Repeated hyperglycemia was associated with increased occurrence of postoperative infections, 12.1% versus 8.2% in patients with single or no hyperglycemia (p = 0.019; Fig. 2). There were no statistically significant associations with the type of infection. The median average blood glucose concentration in all patients was 6.1 mmol/L (range: 4.0–11.6 mmol/L) and higher in patients with postoperative infections (6.3 versus 6.1 mmol/L, p = 0.026) and in patients with diabetes (6.3 versus 6.1 mmol/L, p < 0.001). The average amount of insulin given was higher in diabetics than in other patients (1.9 versus 1.5 IU/h, respectively, p < 0.001), but was not statistically significantly associated with later infections. In addition, repeated hyperglycemia was also associated with increased rates of stroke (4.9% versus 1.5%) in patients with single or no hyperglycemia (p < 0.001) and combined in-hospital and 30-day mortality (6.1% versus 2.1%, p < 0.001, respectively). In multivariable analysis (Table 3), repeated hyperglycemia was independently associated with increased risk of postoperative infections.
Risk factors for postoperative infections in multivariable analysis.
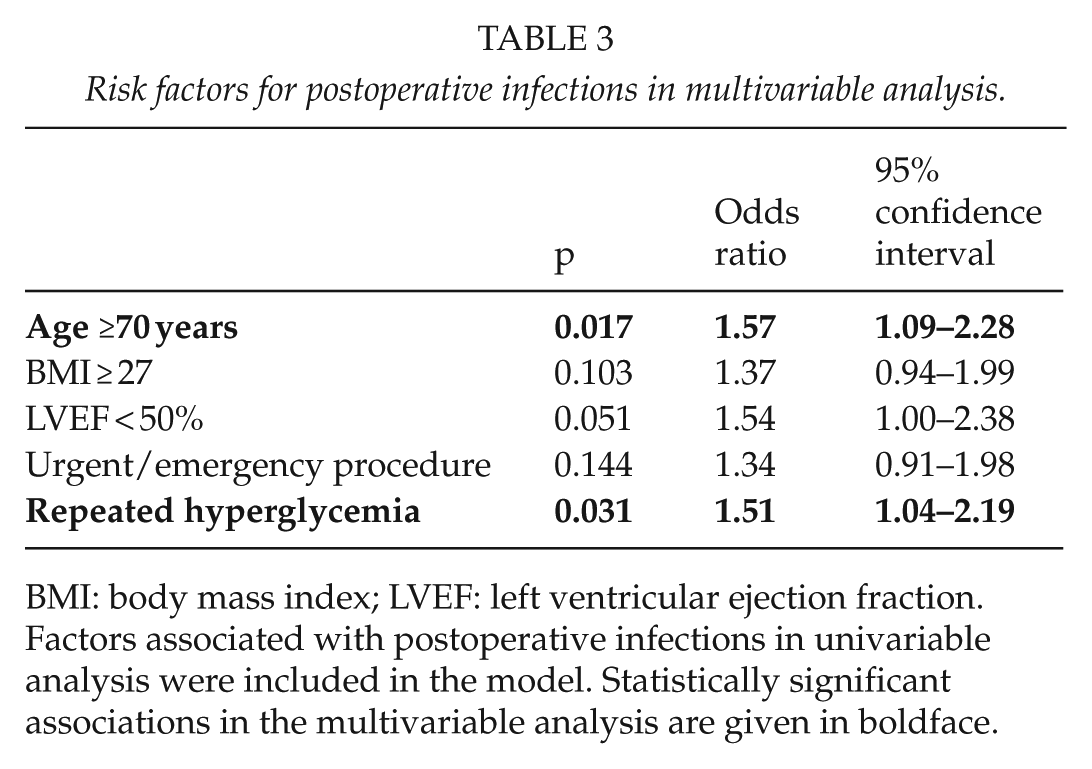
BMI: body mass index; LVEF: left ventricular ejection fraction.
Factors associated with postoperative infections in univariable analysis were included in the model. Statistically significant associations in the multivariable analysis are given in boldface.
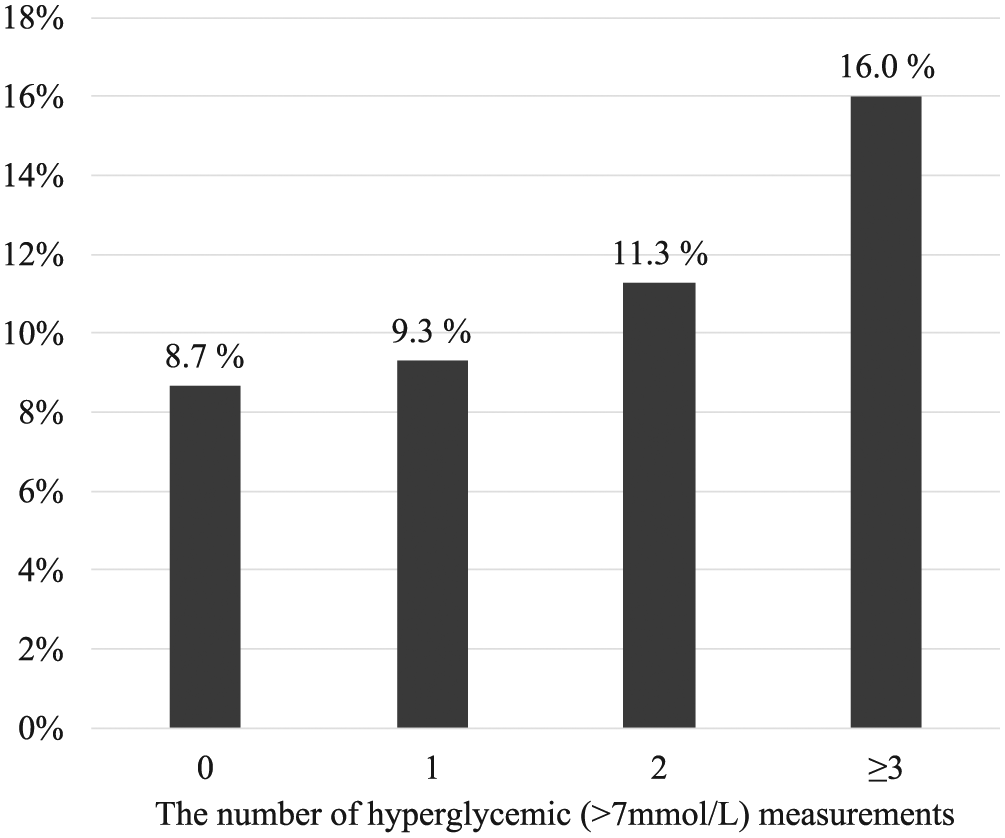
Proportions of patients with infectious complications according to the number of hyperglycemic samples during the first day after surgery.
Discussion
The overall incidence of postoperative infections in our patient population was 9.8%, the majority of which were cannula and catheter related, SSIs, pulmonary infections, and concordant with previous literature. The rate of DSWI in the series, 2.0%, was also standard. Significant variance in pre- and postoperative antibiotic prophylaxis protocols exists between different cardiac surgery programs and the issue is still controversial, perhaps subject to local circumstances, patient material, and clinical practices (11–13). Our protocol consisting of only a single dose of Cefuroxime in most patients is conservative compared to that of others, but was not associated with increased infection rates. Postoperative infections, particularly major SSIs, were significantly associated with increased mortality, as in other studies (14, 15). Previously, immunosuppression, high and low BMI, bilateral internal mammary artery grafts, poor cardiac reserve, red blood cell transfusions, and postoperative respiratory failure have been associated with infectious complications (1, 16–19). In this study, preoperative factors that were significantly associated with the development of postoperative infections were older age, lower left ventricular ejection fraction, higher BMI, and urgent or emergency surgery. Patients with longer ventilator support times had more postoperative infections, suggesting either a causative role or an association with other risk factors in these patients. In contrast to previous studies (20–22), we did not find diabetes to be significantly associated with postoperative infections. It is our impression that most diabetics in our study cohort were in good glucose control preoperatively and we suspect that variance in patients referred for surgery between studies might explain some of the observed differences. A significant portion (13%) of patients with infectious complications developed symptoms after primary hospital discharge or referral, emphasizing the importance of follow-up.
During the study period, we aimed at a strict 4–7 mmol/L glucose range during intensive care at our institution. The median average glucose level over the first postoperative day was 6.1 mmol/L in all patients and slightly higher, 6.3 mmol/L, in patients who developed infectious complications, well within target range. Despite that the average glucose level was acceptable in most patients, many had one or more hyperglycemic measurement. We found that repeated hyperglycemia and higher average blood glucose concentration despite significant effort toward normoglycemia was associated with increased rates of postoperative infections, while single hyperglycemia was not associated with adverse events. Previously, Furnary et al. (23) found 3 mmol/L increase in blood glucose to be an independent predictor of DSWI and mortality rate, while Omar et al. (24) reported higher percentage of out-of-range glucose values in diabetics and increased rates of wound infections in these patients. Some authors have reported that intensive glucose control may offer more benefit in nondiabetics compared to diabetics, while others report better outcomes in diabetics with tight glycemic control (25–28). In our study, repeated hyperglycemia was independently associated with later infectious complications, but whether it directly predisposes to later infections or is a surrogate marker of other comorbidities and a more severe clinical condition, as suggested by higher stroke and mortality rate, and how these patients should best be treated remain unclear. In a mixed ICU population, the benefits of tight glucose control are controversial (7, 8). Hypoglycemia is a potentially severe complication of glycemic control associated with worse prognosis. In this study, hypoglycemia occurred in 7.6% of patients, a smaller percentage than usually reported in patients treated with tight glycemic control (29, 30), and was not associated with adverse outcomes. Our results, and those of others, show that postoperative glycemic control is an important facet of patient care. Implementation of novel methods for glycemic control, such as continuous or semi-continuous blood glucose monitoring systems that offer therapeutic guidance, could improve clinical outcomes and should be explored.
The main strengths of this study are that we present a relatively large cohort of consecutive patients undergoing cardiac surgery including bypass, valve, aortic, and combined procedures. Also, we report the actual incidence of all postoperative infections in these patients, when many authors describe only the occurrence of SSIs. Furthermore, we describe real-practice-based encouraging results obtained with a single-dose conservative antibiotic prophylaxis regime and tight glucose control which both are still a controversial matter in cardiac surgery and intensive care. The main limitations of our study are heterogeneity of the study population limiting statistical power, the descriptive nature of this study, and the absence of a control group with alternative treatment.
In conclusion, we report that every 10th patient undergoing cardiac surgery develops an infectious complication and that mortality in these patients is significantly increased. Repeated hyperglycemia despite tight glycemic control during the first postoperative day is associated with increased risk of postoperative infections, stroke, and mortality.
Footnotes
Acknowledgements
K. M. J. and N. K. K. equally contributed to this article.
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.