
Abstract
Background and Aims:
The wear of metal-on-metal hip implants may increase chromium or cobalt ion blood level. This phenomenon may depend among other things on the particularity of spinopelvic anatomy. The effect of pelvic incidence angle on the wear of metal-on-metal hip implants is not known. The objective of the study was to investigate whether such effect does exist.
Material and Methods:
The pelvic incidence and inclination of acetabular component angles of 89 patients after unilateral metal-on-metal hip replacement were compared with blood level of chromium and cobalt ions using Pearson correlation coefficient.
Results:
No significant correlations between pelvic incidence angle and the metal ion blood levels were observed. The correlation coefficients varied from −0.02 to 0.2 and all p values were >0.05.
Conclusion:
No evidence was found on the effect of pelvic incidence angle on metal wear after metal-on-metal hip replacement when measured by the blood levels of chromium and cobalt ions. It is reasonable to assume that other factors than pelvic tilt may affect the rate of implant wear.
Introduction
Elevated chrome (Cr) and cobalt (Co) ion blood concentration may serve as a marker for the metal-on-metal (MoM) hip implants wear (1, 2). Currently, MoM bearing surfaces are not suggested to be used in hip surgery due to the metal wear and adverse reactions to metal debris (3). The connection between metal ion concentrations and the rate of implant wear offers an opportunity for investigating implant wear indirectly. This may provide an opportunity to measure quantitatively the links between wear rate and the different potential sources of wear.
Pelvic incidence (PI) (Fig. 1) is a measure describing pelvic anatomy and lumbar lordosis independent of the position of pelvis (4). Varying widely from 33 to 85°, PI affects the capacity of rotation of pelvis around femoral heads (5). While small PI angle limits the capacity to backward pelvic tilt, increased PI angle enlarges it (6). Pelvic tilt, determined by PI angle defines, in turn, the entire sagittal spinopelvic balance (4). Previous research has well established the important role of measuring adequate anteversion and lateral opening of the prosthesis acetabular component (7). The correct position of implant enhances clinical success, joint stability, good range of motion, and the absence of impingement (7, 8). It has been found that non-optimal implant position may contribute to the development of hip impingement and the increased wear of polyethylene liner or MoM bearings (2, 9).
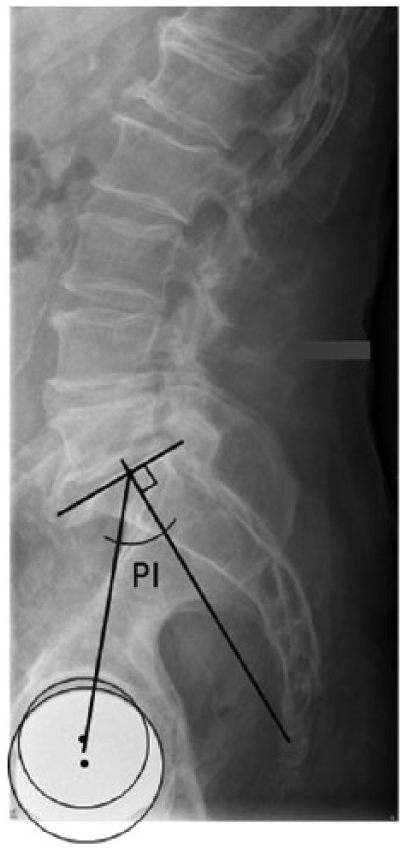
Measuring the value of pelvic incidence (PI).
Previously, it has been stated that there may be a correlation between PI, pelvic tilt, and acetabular orientation (10, 11). Additionally, high PI may cause the wider sagittal range of motion of total hip prosthesis and increased change of acetabular orientation when the patient moves (12). The relation between acetabular orientation and wear rates has previously been reported (2, 13). It is not known whether PI angle has any significant effect on pelvic and acetabular position, as well as on the range of movement of the prosthesis, and whether it is significant enough to cause the observable wear of hip prosthesis.
The objective was to investigate whether there is any correlation between the markers of MoM wear—Cr and Co ion blood levels—and PI angle. If such relationship exists, then PI measure might play an important role in positioning the acetabular component.
Material and Methods
Data were collected on the consecutive patients who underwent unilateral ReCap Magnum/Bimetric large-diameter head MoM total hip replacement (THR) or ReCap resurfacing arthroplasty (Biomet, Warsaw, IN, USA) in a university orthopedic clinic (3) during 2007–2011. Of the 93 eligible patients, 3 were excluded due to the absence of lumbar spine radiograph and 1 was excluded due to the absence of blood test results. The final sample included 48 male and 41 female patients with age on average 65.4 (standard deviation (SD) = 8.5) years. Of the 89 patients, 3 had a MoM resurfacing and 86 had a MoM THR. Additionally to MoM, 15 patients had earlier been exposed to other types of hip replacement on the contralateral side. All the radiographs and blood tests were taken between April 2014 and February 2015. The radiography for PI measurement was done while standing straight and comfortably with the arms either crossed over the chest or resting on a horizontal stand. The patients had their lumbar spine and both hips radiographed from the direction of right to left with the left side against the film cassette. PI was defined as the angle between the line perpendicular to the sacral plate at its midpoint and the line connecting this point to the center of the axis of the femoral heads (Fig. 1). PI was measured by an orthopedic surgeon as suggested by Legaye et al. (4). The center of the replaced hip was marked similar to the marking of the center of a non-operated hip. When the replaced hip covered the sight of the other hip, the center of the femoral head was defined as the center of the replaced hip. The inclination of acetabular component was assessed from pelvis anteroposterior radiographs by a radiologist. Acetabular component inclination of 30–50° has earlier been considered optimal (7). All the radiographic measurements were done using Carestream PACS® imaging software (Version 11.3 turpacs, 2011; Carestream Health, Inc. (Onex Corp.), Rochester, NY, USA). The hospital ethics committee approved the study.
Statistical Analysis
We ran a Shapiro–Wilk test for data normality appropriate for dataset smaller than 2000 elements. Therefore, to constructing a regression curve, abnormally distributed data were transformed into lognormal form. The estimates from normally distributed data were reported as means, SDs, and ranges. Otherwise, the results were reported as medians and ranges. Pearson correlation coefficient was used along with two-tailed p values (level of significance set at
Results
The two-tailed p values were 0.148 for PI, for inclination 0.857, and <0.001 for chrome and cobalt blood contents, respectively. We concluded that the PI and inclination data came from a normal distribution and the chrome and cobalt content data were abnormal. Therefore, to constructing a regression curve, chrome and cobalt data were transformed into lognormal form. Time between surgery and imaging and between surgery and blood test were also abnormal with Shapiro–Wilk test p values <0.001.
No dislocations had occurred and none of the patients needed a revision surgery for any other complication of arthroplasty. The time between operation and imaging and between operation and blood test was on median 41.6 (range 32–101) months.
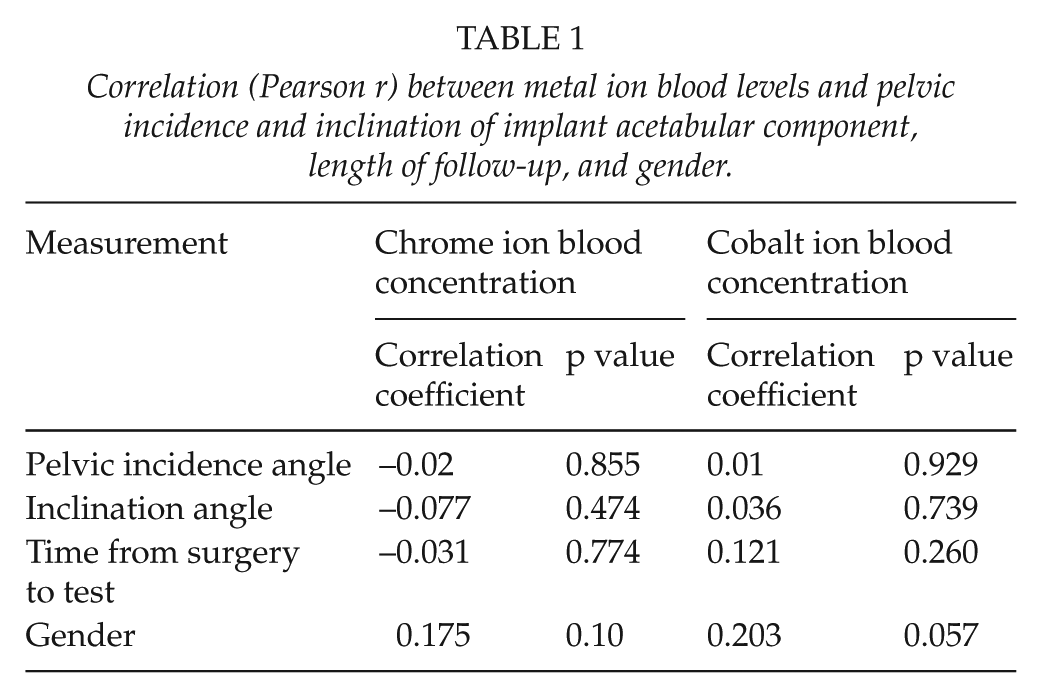
The mean angle for PI was 55.8° (SD = 11.2°, range = 35°–83°). The respective figures for inclination of acetabular component were 41.5° (SD = 7.4°, range = 22°–60°). The Cr ion blood level was on median 1.6 (range = 0.7–13.6) µg/L. The respective median value for Co ion blood concentration was 1.5 (range = 0.4–29.6) µg/L. No significant correlations between PI or inclination angles and Cr or Co ion blood levels were observed (Table 1). There were also no correlations between metal ion blood levels and length of follow-up and/or gender. The correlation coefficients varied from −0.02 to 0.2 and all p values were >0.05.
Correlation (Pearson r) between metal ion blood levels and pelvic incidence and inclination of implant acetabular component, length of follow-up, and gender.
Discussion
In this prospective observational study of 89 patients who underwent a MoM hip replacement, correlations between PI or inclination angles and Cr or Co ion blood levels were small
The Cr and Co ion blood levels have been proposed to be a reliable indicator of hip implants’ wear (1, 14). Additionally to pelvic tilt, factors such as trunnion–head interface and passive corrosion or the stem surface or high inclination may affect the rate of wear (1, 2, 13, 15). Matthies et al. (16) reported that acetabular orientation explains less than 30% of variation in metal ion levels, while the rest might be explained by other factors such as component size and design. Langton et al. (13) also reported the smaller component size to effect the metal ion concentration.
In line with earlier studies reporting stability of metal ion levels up to 9 years after MoM hip resurfacing operation, no correlation was found between the metal ion blood levels and length of follow-up (17). Both hip resurfacing and THRs were included in the present sample. However, the amount of resurfacings was small, only three cases. Furthermore, resurfacings and MoM THRs included were analogous models from the same manufacturer. No significant difference in metal ion levels between hip resurfacings and different types of MoM THRs overall has previously been stated (18). However, when comparing blood metal ion levels between ASR resurfacing and ASR THR (DePuy Orthopaedics, Warsaaw, IN, USA), higher ion levels in patients with the ASR THR compared to ASR resurfacing have been reported (19). Of the patients, 15 had also exposed to metal-on-polyethylene replacement of contralateral hip. It is, though, unlikely that this could significantly affect the results as no increase in metal ion levels after metal-on-polyethylene hip replacement has previously been found (20).
Two-dimensional imaging used in this study might miscalculate the true three-dimensional acetabular component orientation and particularly the anteversion. Acetabular component may be well positioned with relation to inclination but not in relation to ante- or retroversion. This way, the lack of anteversion assessment in this study may affect the results. The range of the inclination of the acetabular component in this study was relatively wide that, in theory, may increase the wear of MoM bearings. However, it has previously been stated that inclination angle is not associated with adverse reaction to metal debris when using ReCap Magnum THR (21). Even though, increased femoral head size of ASR THR is a known risk factor for adverse reaction to metal debris (22), no reports have been published on the association between increased femoral head size of ReCap Magnum THR and increased blood metal ion levels. Therefore, measuring femoral head size was out of scope of this study.
A sample of less than 90 patients may be insufficient to achieve significant results when recognizing such weak correlations between PI and hip implant wear. Further research on larger sample size and longer follow-ups may reveal whether there is a weak correlation. As being potentially relevant, gender, inclination, and follow-up might be included in a multivariate model. Plain correlations may be insufficient to make any definitive conclusions since relevant risk factors may affect one another.
Conclusion
No evidence was found on the effect of PI angle on metal wear after MoM hip replacement when measured by the blood levels of chromium and cobalt ions.
Footnotes
Approval Of Institutional Review Board
This study was approved by Research Ethics Committee of the University of Turku (License ETMK 78/2013).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Turku University Foundation.