
Abstract
Background and Aims:
Personality disorders are frequently associated with eating disorders in obese patients and may negatively affect weight loss and maintenance after bariatric surgery. This non-randomized study aimed to assess the effects of different psychotherapeutic interventions on weight loss in a sample of patients with borderline personality disorder who underwent laparoscopic gastric bypass or laparoscopic adjustable gastric banding.
Materials and Methods:
A total of 153 bariatric patients meeting borderline personality disorder criteria were chosen voluntarily and consecutively to undergo an interpersonal individual treatment (n = 50), a dialectical behavioral group treatment (n = 50), or treatment as usual (n = 53) for a year after surgery. Their body mass index was measured before and at the end of each treatment.
Results and Conclusion:
A total of 12 patients (7.8%) dropped out of the study. Significantly higher body mass index reductions were registered in both experimental groups (−14.2 and −9.4 kg/m2, respectively) compared with the treatment as usual group (−2.1 kg/m2; p < 0.01). Treated patients who underwent laparoscopic gastric bypass (total n = 94) showed better outcomes than those who underwent laparoscopic adjustable gastric banding (total n = 45), while no differences were observed in untreated patients. This study demonstrates the role of pre-operative psychological assessment and post-operative psychotherapeutic support in improving weight loss among bariatric patients with borderline personality disorder. A randomized controlled trial is needed to confirm these preliminary findings.
Keywords
Introduction
Obesity is a critical public health issue. In 2008, more than half a billion adults were affected by obesity, and its prevalence is still increasing. Several diseases are related to obesity and are associated with a consequent increase in mortality rate and reduction in the quality of life (1). A series of genetic, metabolic, hormonal, social, and psychological determinants are related to this condition (2, 3).
Due to its efficacy in reducing obesity, improving psycho-physical conditions and promoting well-being and quality of life, bariatric surgery is now the best treatment for individuals with extreme obesity or those with less severe obesity accompanied by significant comorbidities (2, 4–8). Several different surgical procedures are available. These procedures are effective via the restriction of intake or malabsorption of food, or a combination of these, and lead to a modification in the production of gastrointestinal hormones. Laparoscopic gastric bypass (LGB) and laparoscopic adjustable gastric banding (LAGB) are two of the most common procedures (2). Although LAGB is associated with fewer early complications and shorter operative time and length of stay, LGB shows greater efficacy in determining postoperative weight loss (9, 10).
The maintenance of postoperative weight loss and the improvement in obesity-related health problems make bariatric surgery the most effective treatment for people with obesity; nevertheless, psychosocial and behavioral factors contribute to determine post-intervention outcomes (11, 12). Frequently, psychological and behavioral aptitudes can influence surgical outcomes, even independently of weight loss (8, 13–19). In most cases, people with obesity and patients undergoing bariatric surgery present with eating disorders (20–22).
There is increasing evidence that not only disorders included in the axis I of the Diagnostic and Statistical Manual of Mental Disorders–fourth edition (DSM-IV), such as depression, but also axis II personality disorders such as borderline personality disorder (BPD) may promote the development of eating disorders in obese subjects and may be associated with health outcomes in bariatric surgery candidates (23). BPD is a personality dysfunction characterized by disinhibition, impulsivity, and self-regulation difficulties that may culminate in overeating behavior and eating disorders (13, 14, 24, 25). The average prevalence rate of BPD in bariatric patients was estimated to be at least four times higher than that of the general population (27 vs 2%–6%) (24, 26).
People with obesity presenting with eating and psychiatric disorders, especially personality disorders, report greater difficulties in adapting to the new condition after surgery (27). Therefore, the psychological evaluation of bariatric surgery candidates may be useful to highlight risk elements that can represent reasons to delay or deny surgery or to address post-intervention treatments (3, 28–30). There is existing evidence that cognitive behavioral therapy, a form of psychotherapy that helps the patient learn how to identify distorted beliefs and change behaviors accordingly, can be useful to treat possible psychological or eating problems in bariatric surgery candidates, improving post-operative outcomes (29–33).
Furthermore, dialectical behavioral therapy (DBT), a form of cognitive behavioral therapy, is an effective treatment for people with BPD, but other psychotherapies, such as interpersonal therapy, based on the improvement of communication and relational patterns to change behaviors, seem to be promising in this field (30).
Little is known about the potential effects of different psychotherapeutic approaches on bariatric surgery outcomes in patients with BPD, and no previous studies have evaluated the effect of treatment on weight loss outcomes.
Ours is the first study to evaluate the effects of interpersonal and DBT on weight loss in a non-randomized sample of surgery patients with BPD after a 1-year post-intervention treatment, comparing their results with those receiving the usual treatment with the aim of establishing the feasibility and preliminary effectiveness of such an intervention.
Materials and Methods
Study Design
This prospective, non-randomized study was conducted over the years 2009–2015. Candidates for LGB or LAGB were interviewed consecutively before the surgical intervention to analyze the presence of BPD. The following three types of post-bariatric protocols were proposed by psychologists to each patient who showed BPD: an individual interpersonal treatment, a dialectical behavioral treatment, and treatment as usual. The choice of the treatment was taken freely by patients. At the end of the treatment, body mass index (BMI) differences were evaluated retrospectively, considering the type of treatment and the possible differences between LGB and LAGB patients.
The University of Naples Parthenope approved the study protocol. All participants were provided with a written informed consent.
Setting and Participants
Caucasian patients seeking a first bariatric intervention at the evangelical hospital “Villa Betania” in Naples were considered for the study. Patients were contacted consecutively during the standard pre-intervention medical examination and asked to participate in the study. Inclusion criteria included adults (⩾18 years of age) and candidates for LGB or LAGB. Patients who reported psychiatric/psychological disorders during the meeting, such as psychotic disorders, bipolar I disorder, delusional disorder, delirium, dementia, and cognitive disorders, and who were already under psychiatric/psychological treatment were excluded. Those with substance dependence were also excluded, although patients who reported current episodes of substance abuse were included.
A psychologist explained the aims of the study to the eligible participants and guaranteed the anonymity of results. Patients meeting BPD criteria were invited to take part in the prospective study after surgery, and a psychologist explained the main contents and organizational features of the proposed treatments; those who agreed by signing the informed consent chose to undergo interpersonal therapy (n = 50), DBT (n = 50), or treatment as usual (control group, n = 53).
Assessments and Outcomes
Participants who gave their informed consent provided demographic information; height and weight were measured to determine their BMI. BPD was assessed by experienced psychologists using the Structured Clinical Interview for DSM-IV Axis II Disorders (SCID-II): v (34).
Intra- and inter-group differences in BMI assessed at the start (T0) and at the end (T1) of the study were considered as primary outcomes, together with decreases in the BMIs of LGB and LAGB patients. The secondary outcome was the improvement in BPD, evaluated on the basis of SCID-II responses.
Interventions
For each participant, psychotherapeutic treatment started 1 month after the surgical intervention and consisted of at least 60-min weekly sessions conducted for 12 months by advanced therapists. The interpersonal individual treatment was focused on the evaluation of interpersonal relationships to reinforce individual functioning. According to Markowitz, the initial phase (first 16 weeks) of the treatment aimed to establish a therapeutic alliance, to control impulsive and self-destructive conduct and to promote an initial improvement of symptoms. The following sessions aimed to strengthen the initial results and to develop stable and appropriate interpersonal relationships (35).
Considering previous experiences in the development of core beliefs, the dialectical behavioral treatment aimed to promote strategies for behavior modifications and to provide motivation to tackle post-surgery difficulties. According to Linehan et al. (36), this behavioral treatment was implemented to address the following functions: increasing behavioral capabilities, improving motivation for skillful behavior, assuring generalization of gains to the natural environment, structuring the treatment environment so that it reinforces functional rather than dysfunctional behaviors, and enhancing therapist capabilities and motivation to treat patients effectively. To comply with patients’ needs and improve their participation, only weekly group sessions were provided. Weekly therapist consultation team meetings were held. Patients were asked to undertake homework in between sessions. If needed, a telephone consultation was offered to the subjects from both therapy groups. Treatment as usual consisted of a preoperative medical and psychological evaluation and a meeting with bariatric surgeon at 1 month and at 12 months after surgery.
Statistical Analysis
Statistical analyses were carried out using the software IBM SPSS version 21 for Windows (SPSS, Chicago, IL, USA). A descriptive analysis was carried out to evaluate the characteristics of each treatment group. Differences among groups were evaluated through a χ2 test or analysis of variance (ANOVA). A Pearson’s correlation was carried out to highlight a possible role of BPD score resulting from SCID-II in determining the choice of the treatment.
Differences in BMI measured at T0 and T1 for each group were evaluated through Student’s t test. Differences in mean BMI among treatment groups were analyzed through ANOVA. The comparison among mean BMI in patients undergoing LGB and LAGB was performed through t test for each treatment group and through ANOVA among the three groups. A significance level of p = 0.05 was assumed.
Results
Among a total of 584 surgery candidates consecutively interviewed, 162 (27.7%) met SCID-II criteria for BPD. They were mostly women (78%) and had a mean age of 31 years (standard deviation (SD) ± 8.99; range, 18–56) and a mean BMI of 45.8 kg/m2 (SD ± 6.38).
Among these subjects, 153 females (94.4%) agreed to participate in the study and chose interpersonal therapy (n = 50), dialectical cognitive therapy (n = 50), or treatment as usual (n = 53). The correlation between BPD scores and study group chosen was not significant (r = 0.018, p = 0.826). A total of 139 subjects completed interventions (adherence rate > 65%) and follow-up, and 94 of these subjects underwent LGB and 45 underwent LAGB. They were divided among experimental and control groups without significant differences. Fig. 1 shows the flowchart of patients’ participation. The baseline characteristics of the treatment groups are reported in Table 1.

Flowchart for enrollment, treatment, and follow-up of participants in the prospective, non-randomized study.
Baseline characteristics of experimental and control groups.

SD: standard deviation; LGB: laparoscopic gastric bypass; LAGB: laparoscopic adjustable gastric banding; ANOVA: analysis of variance.
χ2; **ANOVA.
The mean BMI values registered at T0 and T1 in the three treatment groups and in the surgery subgroups are shown in Table 2.
Mean BMI values ± SD measured at T0 and T1 in experimental and control groups, LGB and LAGB subgroups with correspondent differences and p values.
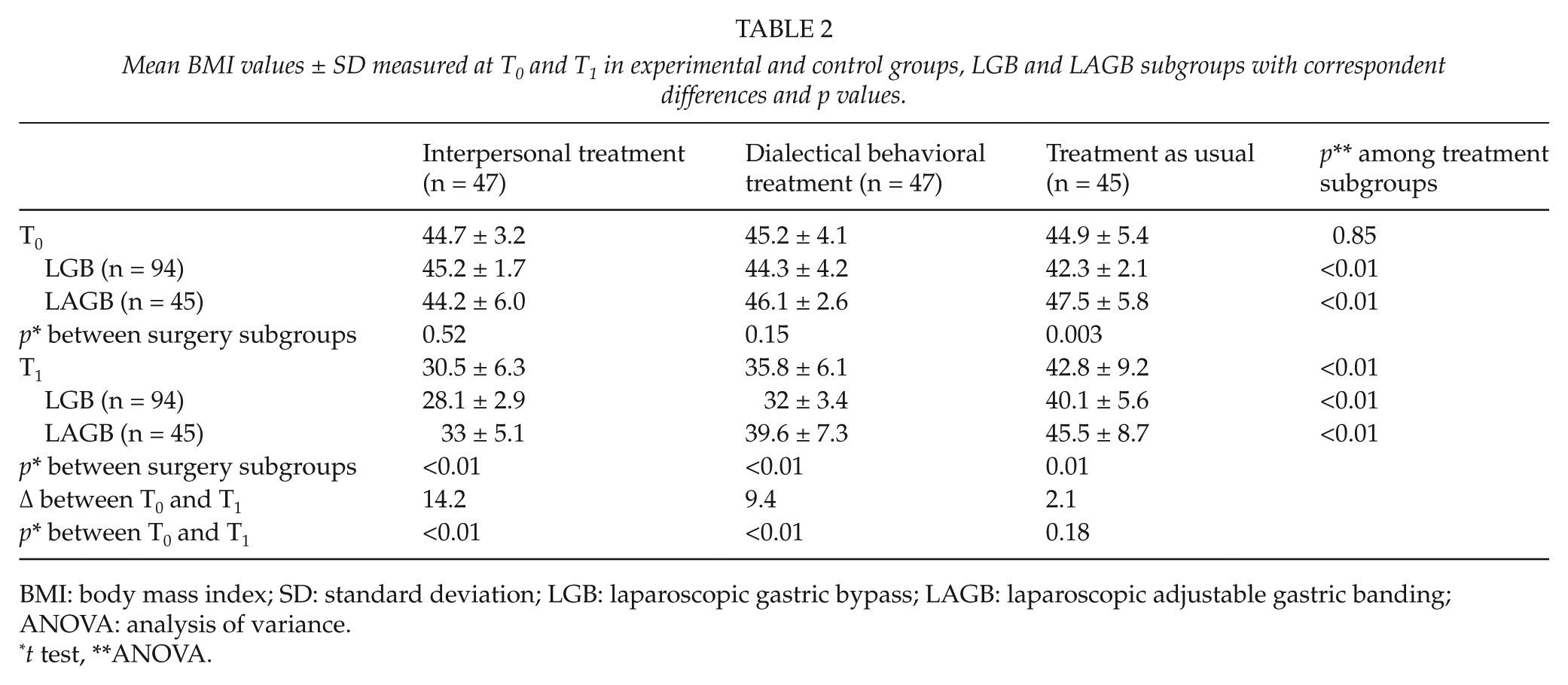
BMI: body mass index; SD: standard deviation; LGB: laparoscopic gastric bypass; LAGB: laparoscopic adjustable gastric banding; ANOVA: analysis of variance.
t test, **ANOVA.
At the end of the year of treatment, significant differences in mean BMI values were registered among experimental and control groups (p < 0.01), with better results observed in interpersonal therapy patients (−14.2 kg/m2).
LGB patients showed increased weight loss compared with LAGB patients in both the experimental groups, while the reduction was quite similar between the subgroups who underwent usual treatment (p < 0.01).
At the end of the study, a total of 88 patients (63.3%) did not meet the SCID-II BPD criteria (41 from the interpersonal treatment group, 40 from the dialectical cognitive treatment group, and 7 from the control group, p < 0.01).
Discussion
This study aimed to evaluate the effects of two different psychotherapeutic approaches, interpersonal and dialectical behavioral, on weight loss in a sample of bariatric surgery patients with BPD.
The number of patients meeting SCID-II BPD criteria in our sample was higher than that shown in other studies (23, 37–39). However, it should be considered that the BPD assessment is typically undertaken prior to surgery; therefore, it is possible that a proportion of participants under-reported the classic symptoms of BPD, such as self-mutilation, suicide attempts, or alcohol/substance abuse, to secure the surgery. Thus, the previously reported averaged prevalence rates are likely to be underestimated (26).
Our results demonstrate an improvement in the outcomes of bariatric surgery, as shown by follow-up results in control patients. Moreover, outcomes registered in the experimental groups confirm that psychotherapy treatment may induce an amelioration of BPD and support post-operative weight loss and maintenance.
In the study by Nijamkin et al., 24% of participants who received a comprehensive behavioral-motivational intervention reported a remission of depressive symptoms 12 months after surgery, compared with 6% of those who received standard care. Improvements in patients’ depressive mood were positively associated with the weight loss registered in the 80% of participants receiving the behavioral intervention (32). Our findings confirm the usefulness of behavioral interventions in motivating bariatric patients after surgery. The high rate of BPD improvement and the considerable weight reduction observed in patients treated with interpersonal therapy show that this approach may be as useful as DBT to achieve these objectives. Therefore, this treatment can also be considered as a valid post-bariatric support for overcoming mental disorders associated with nutrition and improving weight loss. Several controlled studies have shown the efficacy of psychotherapeutic treatments in improving BPD features, such as self-destructive behaviors, anger, or psychosocial functioning (36, 40, 41). By imparting interpersonal skills such as self-assertion, confrontation, and effective expression of anger or helping the patient to engage in functional, life-enhancing behavior even when intense emotions are present, interpersonal therapy and DBT can empower the emotional and behavioral control in patients with BPD, respectively, and reduce their symptoms (42, 43). Chen et al. (44) also reported an improvement in eating behaviors, which are considered as an expression of the loss of behavioral control, among patients with comorbid BPD and eating disorders treated with DBT. Furthermore, the literature shows overall improvements in psychopathology, depressive symptoms, eating behavior, and quality of life following bariatric intervention only (45). These improvements are related to weight loss and a consequent change in self-esteem and body image. Therefore, it is possible that in bariatric patients with BPD, the combination of surgery and psychotherapeutic treatments improves both psychological disorders and weight loss.
This study also has some limitations. First of all, the study does not have the reliability of a randomized controlled study because patients dispersed voluntarily into the three treatment groups. Therefore, it should be considered that patients who chose to refuse psychotherapy treatments may be neglecting their health and may be unwilling to change their eating behavior, which probably determined their lesser weight loss.
However, a possible correlation between BPD score and choice of the treatment was excluded, and it should be noted that a considerable number of patients who gave their consent to participate in the study were forced to decline the treatment offer due to organizational or logistical reasons (data not shown). Even if this issue was not investigated in depth, these motivations should also be taken in account. The choice between the two therapeutic treatments, which were performed with the same timing, was probably guided by the need to fight personal disorders alone, or by the contrary need to share common problems with others. This aspect could be useful for matching each patient to their more appropriate treatment.
Although the data elaboration was blinded, neither BMI nor BPD symptoms were assessed blindly, and this could have generated some collection bias. Furthermore, it has to be noted that in this study, we did not evaluate the possible effects of diet modifications adopted by patients during the post-operative period on the considered outcomes. Another limit of the study was the exclusive female composition of the samples, which did not allow for a gender comparison. Finally, to reach a wide and comparable size of the three subgroups, we enrolled patients consecutively.
The findings of this study provide preliminary data supporting further investigations about the use of interpersonal treatment and/or DBT to improve weight loss outcomes in patients with BPD. A randomized controlled trial and a longer follow-up could be useful for this purpose. The possible role of these types of treatment in improving eating disorders in bariatric patients with BPD should also be analyzed.
Conclusion
This study demonstrates that pre-operative psychological assessment and post-operative psychological support may improve weight loss in bariatric surgery patients showing BPD. By enhancing impulse regulation in these subjects, interpersonal treatment seems to be a good tool such as behavioral therapy to overcome BPD and enhance surgery outcomes. A randomized controlled study is needed to confirm these findings.
Footnotes
Acknowledgements
The authors gratefully acknowledge the staff of the evangelical hospital “Villa Betania” for the support they received throughout the study and the study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.