
Abstract
Introduction:
Foreign body injuries are common in children. Most of them are not serious but they can be fatal. A suspected foreign body injury in a child results in a high rate of hospitalizations, exposure to radiation, and need for intervention. This study aimed to analyze the current epidemiology of in-hospital or out of hospital treated foreign object injuries and suspected foreign body injuries in children.
Material and Methods:
All children <16 years of age (N = 152) who suffered or were suspected to suffer (N = 63) from a foreign body injury and were treated in a pediatric trauma unit of Oulu University Hospital, Oulu, Finland, over a 6-year study period (2008–2013) were included. A comprehensive chart review was completed in order to evaluate injury history, age at the time of trauma, treatment and characteristics of the foreign objects.
Results:
The majority (57.9%, N = 88) of the injuries were found in children <3 years of age. There was a male predominance (60.5%, N = 92). The most common anatomical site where the foreign body was found was the nose (28.9%, N = 44), followed by the esophagus (20.4%, N = 31) and the eye (11.2%, N = 17). Foreign objects were also found in the lower airways (10.5%, N = 16), ear (10.5%, N = 16), bowel (9.9%, N = 15), throat (3.9%, N = 6), stomach (3.9%, N = 6), and urethra (0.7%, N = 1). Various household items were the most common foreign bodies (33.6%, N = 51). Toys in particular caused 22.4% (N = 34) of the injuries. In-hospital intervention was necessary for 38.5% of the patients (N = 58). Intervention was needed in 39.7% (N = 25/63) of the patients who were suspected to suffer from foreign body but did not. There were no fatalities.
Conclusion:
Foreign body injuries treated at the pediatric trauma unit were most common in the youngest children (<3 years of age). Majority (61.8%, N = 94) of the patients were treated non-operatively, without any in-hospital intervention.
Introduction
Despite all interventions in their prevention, foreign body injuries are still common in children. They comprise about 7% of all visits to pediatric trauma units (1). Similar to most injuries in children, foreign body trauma is more common among boys than among girls (2). The injuries in children are almost exclusively accidental, rather than intentional (3). The risk of injury is highest in children between 1 and 3 years of age (4). In younger children, ingestion or aspiration of foreign bodies is the most common pattern of injury, while older children often present with foreign bodies in other areas (5), typically out of curiosity while exploring their body (6). The foreign objects vary largely, while vegetables, other parts of food, pearls, small toys, stones, and buttons are common objects (7).
Pediatric foreign body injuries can be inconsequential (8): Ingested objects usually migrate throughout the stomach and intestine if they have passed the esophagus. On the contrary, foreign body injuries may also be severe, or even fatal, and cause long-lasting morbidity and the need of treatment and hospitalization (9, 10).
There is no wide understanding about the epidemiology of foreign body injuries in children (2, 11). The aim of this study was to comprehensively analyze the epidemiology of foreign bodies entering through natural orifices in children, <16 years of age, through a hospital-based study setting in a pediatric trauma center. The aim was to analyze the backgrounds of the injuries, clinical findings, treatments, and outcomes, as well as the rate of suspected foreign body injuries, in which no foreign object can be confirmed. The fundamental purpose was to acquire a better understanding of foreign body injuries and therefore make it possible to improve prevention.
Material and Methods
Study Design
The study was performed in the geographic area of Oulu city and its surroundings in Finland, covering all children <16 years of age who were treated for foreign body injury entering through natural orifices in the pediatric trauma unit of Oulu University Hospital at Oulu, Northern Ostrobothnia, Finland, during 2008–2013. The study center is the only pediatric trauma center at the area. The cases who were treated for slight foreign bodies in the primary healthcare centers or private clinics were not included. International Classification of Diseases (ICD), version 10, was used to recognize the patients with a foreign body accident using the institutional hospital registry data. The potential inhabitant patients treated for foreign body injuries at any other trauma centers in the country or abroad during the study time were not recognized for the study purpose and thus not included. The diagnoses T15–T19 including all foreign bodies entering through natural orifices were included. Both patients treated in hospital and out of hospital at the study center were included in the study. All potential patients were considered for inclusion, regardless of the department they were admitted under. Children with a confirmed foreign body injury were included. Furthermore, those who were treated at the study center on the basis of a reasonable suspicion of foreign object were also analyzed separately. Medications taken improperly and ingested liquid chemicals were not included.
The pediatric population-at-risk in the study area was determined according to the official statistics of Statistics Finland bureau. It varied between 85,731 (2008) and 87,727 (2013) during 2008–2013, being in mean 86,681.
Patients
There were in total 152 patients <16 years of age identified during the 6-year study period, who were admitted to the pediatric trauma center for foreign body injury and who were confirmed to suffer from a foreign object. All their chart notes were reviewed to confirm the inclusion. All particulars of the patients such as the patient characteristics, injury history, symptoms, findings, treatment, and outcomes were reviewed. Operative records and anesthesia notes were also reviewed. All treatment procedures performed at an operating theater were classified as operative intervention, including, for example, esophago-gastroscopies, bronchoscopies, and otomicroscopies. Furthermore, in addition to 152 patients with a confirmed foreign body injury, there were 63 patients who were admitted to the trauma center on the basis of suspected foreign body injury, though no foreign body was found during their hospital stay, and they were analyzed separately.
Statistical Procedures
The information was first recorded manually, and then entered into the computer database. IBM SPSS Statistics software, version 22.0, was used for the analysis. Background characteristics are presented as frequencies and mean values with standard deviation (SD) for normally distributed variables and as medians for non-normally distributed variables. Patient age was classified into four groups: <1, 1–3, 4–6, and >7 years. The nature of the foreign objects was analyzed using the classification with seven subgroups modified from Rimell’s classification (12). Univariate associations of independent variables were analyzed using the chi-square test and the change of incidence during the study period by using regression analysis test. p-value of <0.05 was taken to be statistically significant.
Ethical Aspects
This was a registry-based study and the patients were not contacted. No ethical board approval was needed. Institutional permission to use hospital registries was obtained prior to initiation of the study.
Results
Patients’ Characteristics and Incidence
There were in total 152 foreign body injuries in the study period. The majority (60.5%) of the patients were boys and 39.5% were girls (p = 0.01). The proportion of boys was 61.1%, 61.7%, and 59.5% in the age groups <3, 4–6, and ⩾7 years, respectively.
The mean age of the patients with a foreign body injury was 4.6 (range: 0–15; SD: 4.2) years and median age was 3.0 years. A slight majority (57.9%, N = 88) of all injuries were found in children <3 years. One in four (23.7%, N = 36) of all injuries were found in older children (⩾7 years); six of whom (16.7%) were previously known to suffer from a psychiatric disorder (Fig. 1).
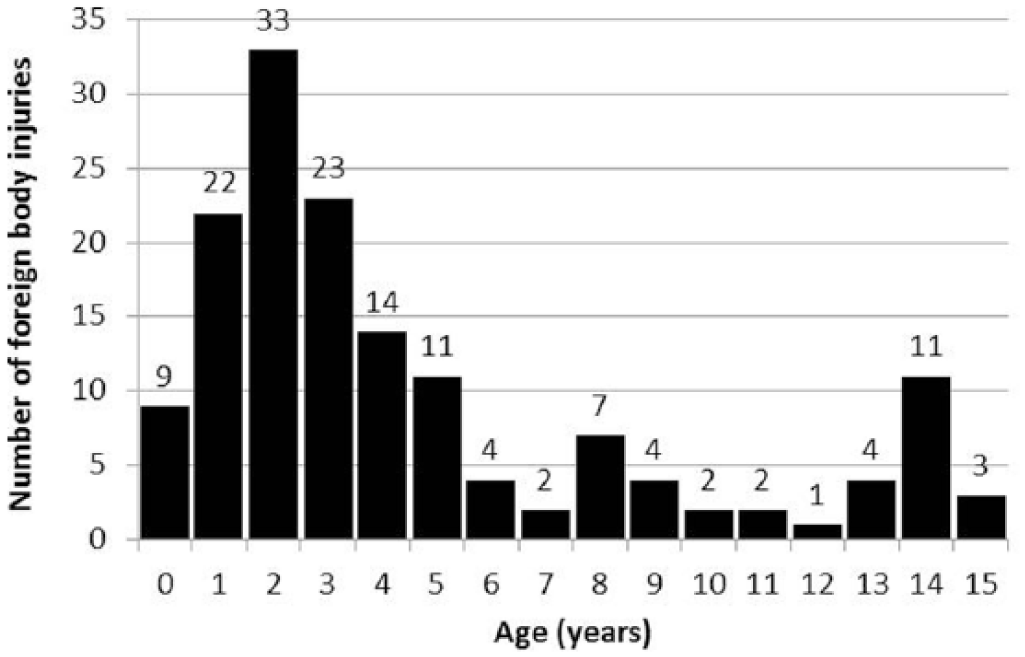
Half of the foreign object injuries happened in young children <3 years of age. There were some isolated injuries still in schoolchildren.
The annual incidence of the confirmed foreign body injuries treated in-hospital or out of hospital at the study center varied between 20.5 (2013) and 36.7 (2012) per 100,000 children, but the incidence rates are not population based. There were on average 29.2 per 100,000 children suffering from the injury during the study time (2008–2013), treated at the study center, and there was no change in that incidence rate during the study period (p = 0.634).
Anatomical Site
The most common site of a foreign object was in the nose (28.9%, N = 44). The second most common location was esophagus (20.4%, N = 31), followed by the eye as the third most common location (11.2%, N = 17). Foreign bodies were also found in lower airways (trachea/bronchi) (10.5%, N = 16), ear (10.5%, N = 16), bowel (9.9%, N = 15), throat (3.9%, N = 6), stomach (3.9%, N = 6), and urethra (0.7%, N = 1). No foreign objects were found in the rectum or vagina (Fig. 2).
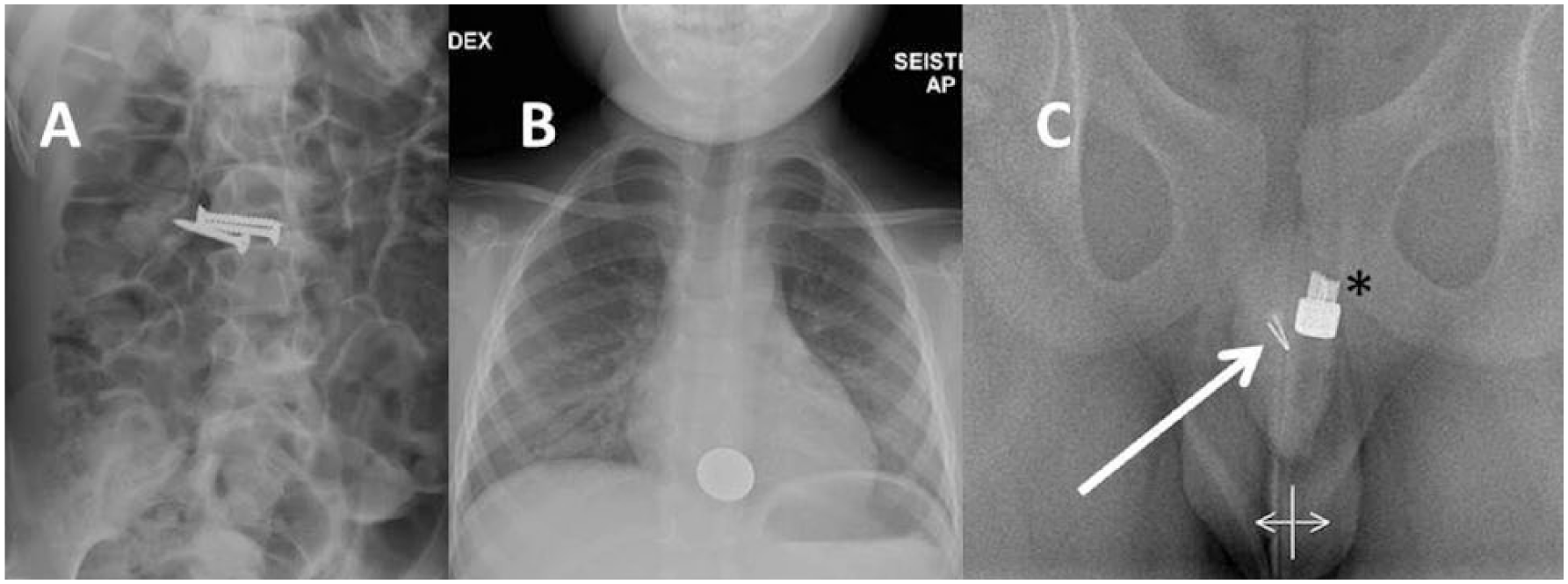
Foreign object injuries in children vary regarding the items and locations. A) A 10-year old girl who had ingested three screws. The child had mental retardation. B) A coin in esophagus in a boy, 4 years. C) A pin (arrow) in the penile urethra in a boy, 9 years. Asterisk (*) indicates the head of catheter.
When analyzed according to the age at the time of injury, the most common anatomical site of foreign part was esophagus (44.4%, N = 4) in children <1 year, nose (47.4%, N = 37) in children 1–3 years of age, and gastrointestinal tract (25.0%, N = 7) in preschool children (4–6 years). In school-age children (⩾7 years), the objects were most frequently found in both the eye (25.0%, N = 9) and the gastrointestinal tract (25.0%, N = 9).
There was no statistically significant difference in the anatomical site of foreign bodies between the genders (p = 0.139). There seemed to be a male (82.4%, N = 14 vs 3 in girls) predominance of foreign body injuries to the eyes but the finding did not reach statistical significance. A total of 6 out of 14 foreign objects in the eye were pieces of metal and two of them the result of grinder use.
Type of Foreign Objects
One in five of the foreign bodies in children were a small toy or a part of a toy (22.4%, N = 34). A piece of food caused 14.5% (N = 22) of the injuries and the same number was caused also by coins (14.5%, N = 22). A miscellaneous fragment or particle of nature (organic or inorganic material) caused 7.9% (N = 12) of all injuries. Unspecific metallic particle of various home appliances or metallic waste was found in 6.6% of the patients (N = 10). A high number of patients (N = 51, 33.6%) had ingested miscellaneous household items, including nine batteries. Otherwise, these mixed items could not be classified in any defined groups above. No magnetic toys were found in the study population (Table 1).
The foreign objects found in children <16 years of age during 2008–2013 in the study area, according to the age group.
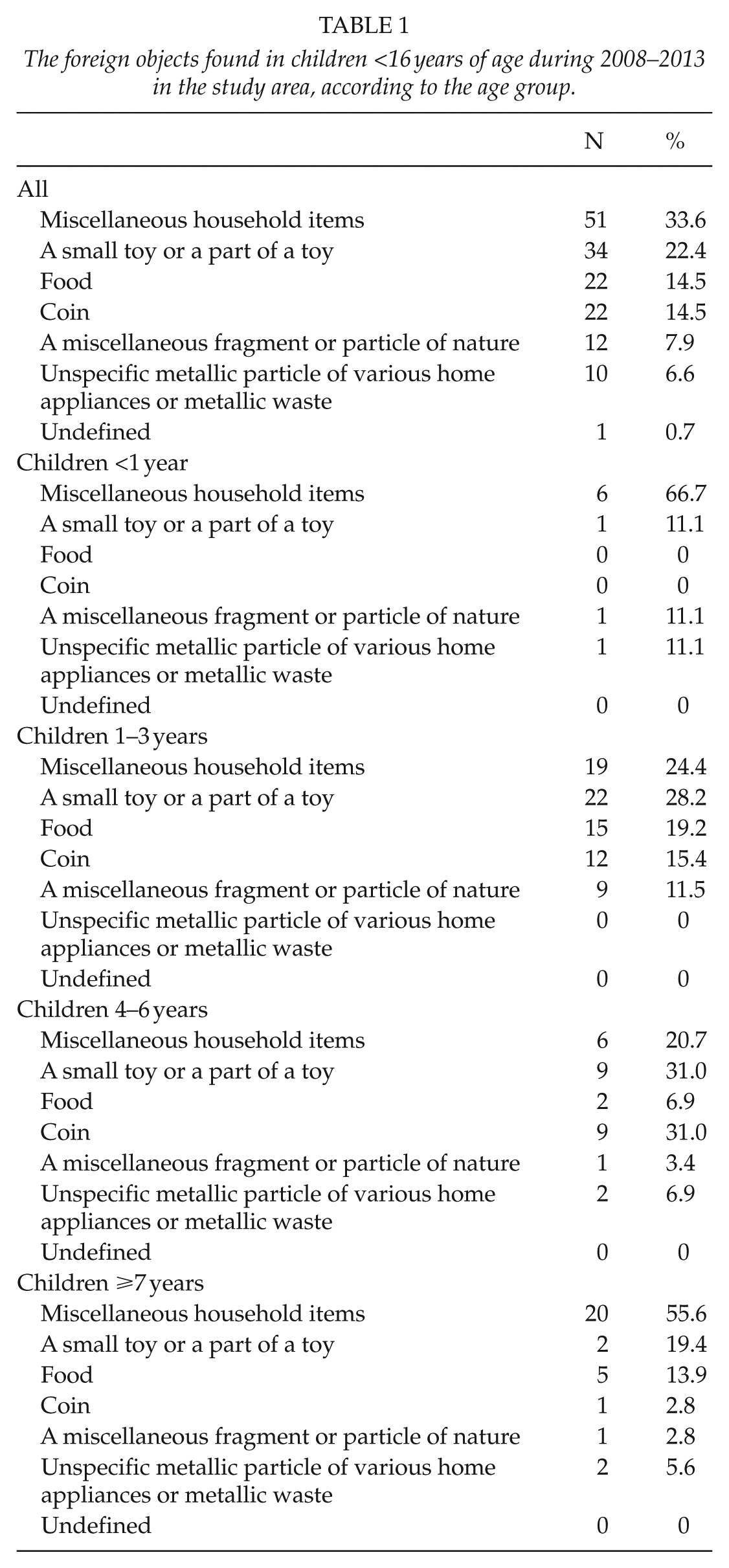
Infants (<1 year of age) were most commonly (66.7%, N = 6) injured by a miscellaneous industrial household object. In children between 1 and 3 years of age, toys and parts of toys were the most common foreign objects (28.2%, N = 22). In preschool children (4–6 years), the most common foreign objects were toys (31.0%, N = 9) and coins (31.0%, N = 9). Children ⩾7 years most frequently suffered from miscellaneous household items (55.6%, N = 20).
Treatment
In total, 38.5% (N = 58) of all patients with a foreign body required hospital intervention for their foreign objects, resulting in that the rate of interventions was 11.2/100,000 per year in this study setting. The majority of interventions needed (56.9%) were esophago-gastroscopies (N = 33). Bronchoscopy was performed for 19 cases (12.5%). Two otomicroscopies, two ophthalmic microscopies, one rhinoscopy, and one cystoscopy were performed. One patient out of 58 patients (1.7%) required re-operation (esophago-gastroscopy) and that was based on a new foreign body injury immediately during the postoperative care while the patient intentionally ingested a new foreign object. That patient had previously been treated for pschychiatric disorders. No open surgery was needed during the study time.
There was no difference in the rate of interventions between the genders (39.1% of boys, N = 36 vs 36.7% of girls, N = 22; p = 0.384). An intervention was performed for 43.8% (N = 28) of children <3 years of age and 34.1% (N = 30) of children ⩾3 years of age (p = 0.268). Most of the patients (65.1%, N = 99) were treated on the day of hospital admission. A third (30.3%, N = 46) stayed overnight and they were discharged home the next day. Seven patients were treated in-hospital for a longer period of time.
Need for Intensive Care and Mortality Rate
Two patients were treated in the intensive care unit as a result of their foreign body injuries. They both had aspirated a foreign object several days in prior to presentation to the emergency care department (Fig. 2). There was no mortality in the study population.
Patients in Whom No Foreign Object was Found
A total of 63 children were admitted to the trauma unit due to suspected foreign body injury; 61.9% (N = 39) of them were boys. Some intervention was performed for 25 (39.7%) of them, without identifying or removing any object. Half (49.2%, N = 31) of the patients were <3 years of age and 14.3% (N = 9) were <1 year of age. A total of 17 out of 63 interventions (27.0%) were performed for children ⩾7 years. Food was the suspected object in 47.6% (N = 30) of the cases. A slight minority (41.3%) of the patients with a suspected foreign object were hospitalized at a ward: 24 patients (38.1%) stayed overnight and were discharged home the next day, while two (3.2%) were in-hospitalized for a longer period of time.
Discussion
We found a high incidence (29.2 per 100,000) of foreign body injuries in children during the 6-year study period, treated in hospital or as out-patient at the pediatric trauma unit of Oulu University Hospital. The total number and a proper population-based incidence of all foreign body injuries would have been even higher if all minor injuries treated at the primary health care were included. However, our finding of the high incidence of hospital-treated foreign body injuries is an important finding because there is no wide understanding of the recent epidemiology of foreign body accidents in children (2, 13). Previously, 6.3% of all visits by children to the trauma hospital were reported to be caused by the presence of a foreign body (14). The annual incidence of children requiring treatment for a foreign body injury was 50/1000 children in a rural area in Africa (15). There may have been the slight decrease in the incidence reported previously (16), but unfortunately our study was not such a population-based that any overall trend could be determined.
In addition to the burden foreign bodies cause for children patients and their families, they also have economical effect on the society. We found that in the study center the rate of in-hospital interventions was 11.2 per 100,000 children. Utilizing the size of respective children population-in-risk in the study country (955,000 in year 2015; Statistics Finland bureau), we expect that more than 100 operations (N = 106) are performed for children due to their foreign body injuries every year. Direct and indirect costs of 1-day surgical treatment of children have previously been determined at the study center (17). Keeping that in mind, we estimate that costs of operatively treated childhood foreign body injuries are more than €165,000 in Finland every year. Furthermore, if all out of hospital treated foreign body injuries in any healthcare units were inclusively recognized, overall costs would be much greater.
We also found that foreign body injuries were most common in children <3 years of age. That is similar to previous knowledge (2), while also mortality is highest among the youngest children (<3 years) (18). We reported no deaths. In regard to prevention, it is the very youngest children who are at the highest risk of both benign and fatal foreign body injuries. We still found a male predominance in this study, which is similar to the previous understanding of pediatric accidents in general (16). We therefore interpret that boys <3 years of age present the greatest risk of foreign object injuries.
Toys, miscellaneous objects at home, food, and coins were all important items causing foreign body accidents. This finding should affect the daily lives of all families with young children: cautions should be taken when making and serving food for children because food particles in the airway most commonly cause severe injuries (13). Toys comprise little components and coins should be stored out of young children’s reach, to avoid them being swallowed by children. Furthermore, manufacturers should make toys radio-opaque and appropriately shaped and sized to avoid injury (19). No magnetic items were found in this study. Previously, the magnetic parts of toys have been associated with intestinal problems, when they attract each other and cause pressure necrosis through the wall of bowel (20, 21). National regulation and the regulation by European Union have improved the safety of toys (22).
A great majority (69.4%) of all interventions were performed due to ingested objects, which all have the potential to be life-threatening by obstructing airways. Other perilous complications can develop upon (button) battery ingestion, by means of several mechanisms: electrical discharge and the creation of hydroxide ions can cause mucosal burn, direct pressure can cause necrosis, leakage of alkalis can cause burns, and there is also a minor risk of mercury toxicity (18). These accidents can result in a permanent need for enteral nutrition and a tracheostomy tube (23). In this study, we found nine battery injuries (5.9% of all). Luckily, no severe complications developed as a consequence of ingested batteries. However, in order to prevent battery accidents, more contribution by many is needed, such as battery and packaging re-design, education, and governmental coordination of strategies and projects (24).
We studied not only the verified foreign body injuries but also those patients who were treated for a suspected foreign body. A great number (N = 63) of children were admitted to hospital and some intervention requiring general anesthesia was performed for 39.7%. Such a high number highlights a problem of childhood foreign body injuries; the injury history may be hard to elicit. An adult was present in just half of the (suspected) foreign body injuries (2). The difficulties in getting the injury history are understandable when the patients are young children, but we surprisingly found that 27% of all unnecessary interventions were performed for children ⩾7 years of age. In that age group, all effort should be focused in discussing the suspected injury directly with the patient, to make the interventions unnecessary. Discussing and interacting with young children can be challenging, and some guidelines for interviewing children with suspected foreign objects would be necessary.
There are some limitations in this study that need to be recognized. We could not analyze the subjective symptoms of the patients in this registry-based study because they were originally not systematically recorded. However, it is previously known that foreign object symptoms are very heterogenic and based on the foreign body type, location, size relative to the patient, and duration of impaction (25). Even the symptoms of fatal airway obstruction can be varied, including stridor, increased salivation, cough, dysphagia, pain, and foreign object feeling in throat (18, 26, 27). Therefore, a diagnosis of foreign object injury can hardly never be done on the basis of symptoms only. Furthermore, it is possible that subjects with minor symptoms may have been treated at primary healthcare centers or private clinics. They may not have been admitted to the study center and have therefore not been included. Isolated cases of the study population that have been treated for foreign body injury elsewhere in the study country or abroad may have been missed from the analysis, too. With these possible missed cases, the rates of in-hospital or out of hospital treatment may have been higher. As a conclusion, the findings of the study cannot be generalized to be population-based, and the reported rate of in-hospital or out of hospital treatment did not demonstrate the overall incidence of foreign body injuries among the entire children population. As a strength, the trauma center covers inclusively all children in the geographic area of about 86,000 children <16 years of age who were admitted for further investigation and treatment from primary healthcare physicians. We consider that the study coverage at the study center is comprehensive, and that the conclusions regarding in-hospital and out of hospital patients at the trauma unit are valid. Furthermore, all children fulfilling the inclusion criteria but living outside the geographic study area were systematically excluded, in order to make analysis valid and accurate. Furthermore, we also had access to the number of cases who were treated in-hospital on the basis of foreign body suspicion even if no object was found. As many as 41.4% of all children treated for suspected foreign body (63/215) did not have a confirmed foreign body diagnosed. To the best of our knowledge, this fact is a novel finding not previously reported. The finding highlights the difficulties in anamnesis and clinical documentation of suspected foreign object in children.
Conclusion
Children’s foreign body injuries remain to be an important cause of morbidity, hospital stay, and interventions, though any conclusion about the incidence of foreign body injuries among the population-in-risk could not be made in this study, due to its hospital-based setting. The hospital-treated injuries were more common in younger children and they most frequently involved the gastrointestinal tract or airways. About one in four patients treated in-hospital due to suspected foreign body injury were treated unnecessarily and no foreign item could be found.
Footnotes
Acknowledgements
M.D. Heidi Silven has contributed to data collecting. Ms Fiona Hanlon-Dearman has contributed to linguistic editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Alma and K.A. Snellman Foundation, Emil Aaltonen Foundation, Finnish Medical Foundation, Finska Läkaresäll-skapet Foundation, and Vaasa Foundation of Physicians have supported the study.