
Abstract
Purpose:
We report 3- to 8-year follow-up results for the first tarsometatarsal joint derotational arthrodesis.
Methods:
A total of 70 patients (88 feet) with symptomatic flexible hallux valgus were operated between 2003 and 2009. In all, 66 patients (94.3%) with 84 (95.5%) feet were enrolled in retrospective analysis; of those, 58 (87.9%) patients with 76 (90.5%) feet were followed for a mean of 5.1 (range: 3.0–8.3) years. Preoperative, 6 week postoperative, and late follow-up weightbearing radiographs were evaluated along with clinical examination and questionnaires.
Results:
The mean hallux valgus angle improved 13.4° (95% confidence interval: 11.6–15.1, p < .001) at the latest follow-up, while the mean intermetatarsal angle correction was 4.5° (95% confidence interval: 3.7–5.2, p < .001). There were three (4.0%) nonunions, and seven (9.2%) feet needed reoperation during follow-up.
Conclusion:
First tarsometatarsal joint derotational arthrodesis is an effective procedure for correcting flexible hallux valgus deformity and provides a satisfactory long-term outcome.
Keywords
Introduction
Hallux valgus is a three-dimensional deformity that has a rotational component (1, 2). Over 130 different operative techniques for hallux valgus have been introduced (3), and reasonable clinical outcomes for different procedures have been reported (4–10).
In 1934, Lapidus (11) described the first tarsometatarsal arthrodesis procedure, accompanied with fusion of the first and second metatarsals, bony exostectomy, soft tissue release, and repair of the distal metatarsophalangeal joint. Lapidus (11–13) did not highlight the rotational correction of the first metatarsal. Several modifications have been published, all including a first metatarsophalangeal procedure (12–19).
First tarsometatarsal joint derotational arthrodesis (FTJDA) includes frontal plane rotational correction of the first metatarsal and axial correction of intermetatarsal angle between the first and second metatarsals (IMA 1-2) but does not include procedure to the first metatarsophalangeal joint or surrounding soft tissues (Fig. 1) (1). FTJDA aims at restoring the function of the windlass mechanism (1). The analogy with the Lapidus procedure and its modifications is the first tarsometatarsal arthrodesis (11–19).
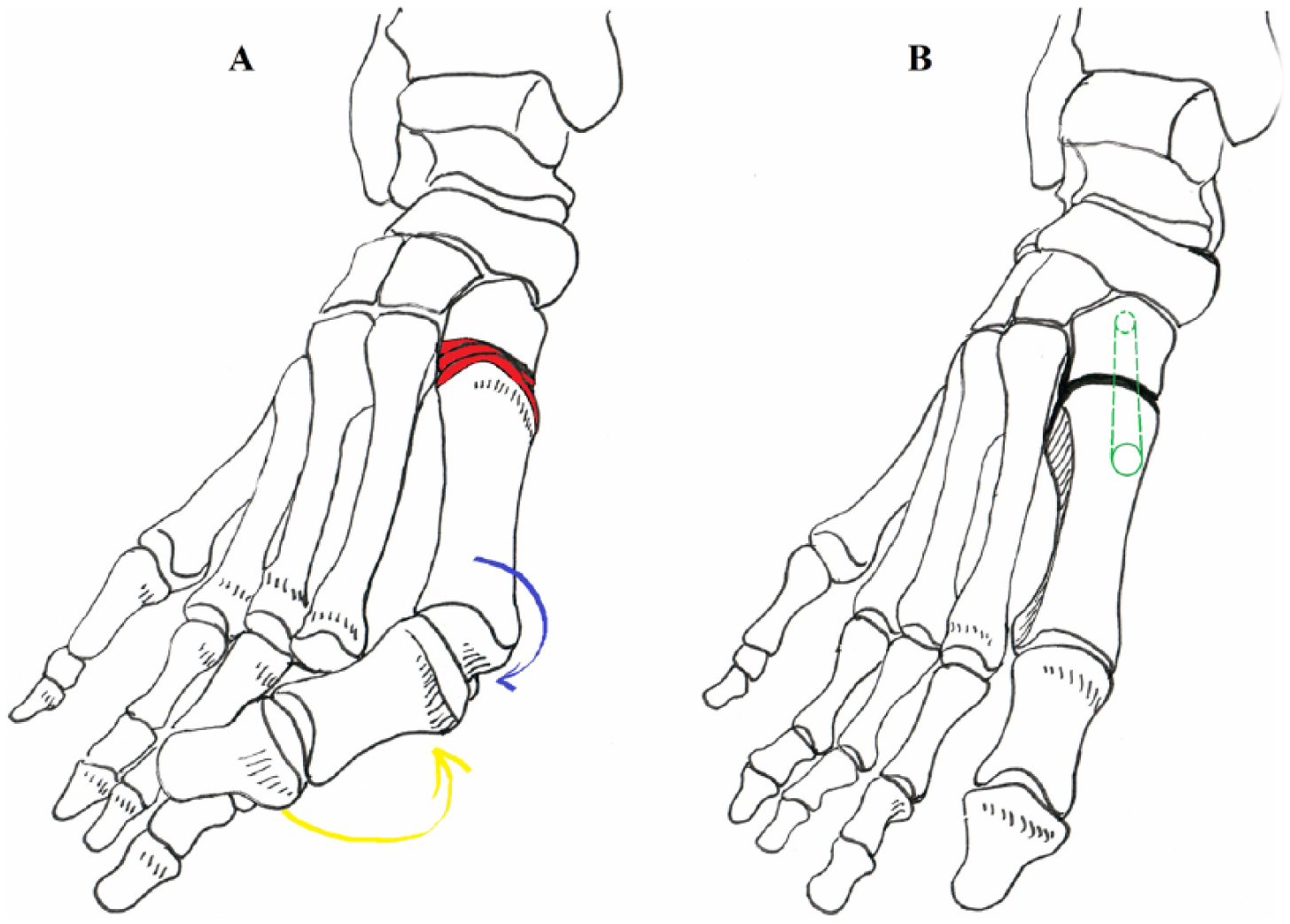
First tarsometatarsal joint derotational arthrodesis: (A) Correction of the flexible hallux valgus can be made without any distal soft tissue release or realignment. Resections of the metatarso-cuneiform joint surfaces (red color) are made in sagittal plane according to the original joint line, without extra plantarization of the first metatarsal (no plantar-based wedge). Intermetatarsal angle (IMA 1-2) correction in horizontal plane is performed when medial cuneiform joint surface is removed (lateral-based wedge). In flexible deformity, the maximal eversion and abduction (relative to the midline of the body) of the first metatarsal (blue bowed arrow) derotates the first toe from pronated position and straightens the toe (yellow bowed arrow). (B) After fixation (green screw), the base of the first metatarsal is everted in the frontal plane under the second metatarsal base (mimicking peroneus longus function) and the first metatarsal head is placed back on the sesamoids. The windlass mechanism is reduced, hallux valgus angle (HVA) and IMA 1-2 are corrected, and “the bunion” disappears without touching the first metatarsophalangeal joint.
No previous mid- or long-term results of FTJDA have been published. We report 3- to 8-year follow-up results of this technique.
Materials and Methods
A total of 70 patients (88 feet) with flexible symptomatic hallux valgus were operated with FTJDA at our university hospital between January 2003 and December 2009. Four feet (4.6%) were lost from the radiological analysis. In all, 66 patients (94.2%) (84 feet, 95.4%) were enrolled in the retrospective cohort (Table 1). During the follow-up, eight patients (12.1%) with eight feet (9.5%) were lost; two of them were men (50%) and six (9.7%) women. Two of the nonparticipants could not be reached, three were not able to participate, and three declined. There were two reoperations among nonparticipants: one corrective osteotomy of the first metatarsal because of malunion (declined follow-up) and one screw removal.
Preoperative demographic data of 66 patients with 84 operated hallux valgus feet followed up a mean of 5.1 years.
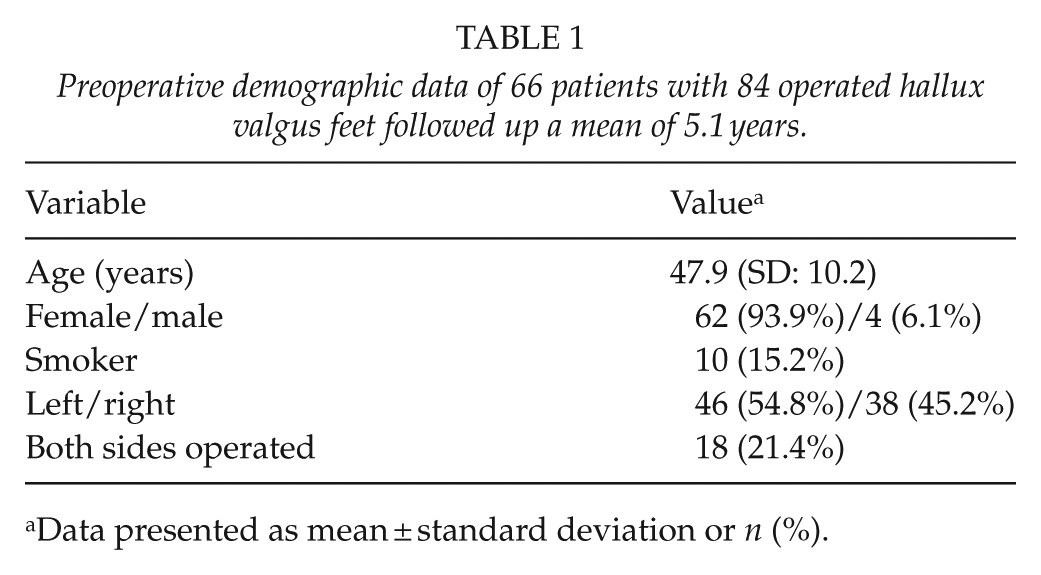
Data presented as mean ± standard deviation or n (%).
After a mean follow-up of 5.1 (range: 3.0–8.3) years, 58 patients (87.9%) with 76 feet (90.5%) took part in the clinical and radiological follow-up.
The inclusion criteria for FTJDA were symptomatic and flexible hallux valgus deformity with uninjured windlass mechanism. The windlass was assessed to be uninjured when flexor hallucis brevis, sesamoids, and plantar fascia were intact. A total of 3 (3.7%) feet had mild hallux valgus (hallux valgus angle (HVA) less than 20°), 70 (86.4%) feet had moderate hallux valgus (HVA: 20°–39°), and 8 (9.9%) feet had severe hallux valgus (HVA: 40° or more). Five (6.0%) of the feet had been previously operated for hallux valgus. Two (2.4%) distal chevron osteotomies and three (3.6%) bunionectomies had been performed in four (6.1%) patients as primary surgery.
A senior orthopedic surgeon (T.K.) examined all the patients for the latest follow-up. Participants completed the following questionnaires per operated foot: American Orthopaedic Foot and Ankle Society first toe metatarsophalangeal-interphalangeal (AOFAS MTP-IP) scale (20, 21), visual analog scale (VAS) for pain (from 0 for no pain to 10 points for worst pain), and functional results (from 0 for no restrictions to 10 points for worst restriction) at the time of recent follow-up. All complications were recorded. One (T.K.) of the five surgeons that operated on patients, involved also in the follow-up visit by filling the AOFAS MTP-IP questionnaire. Other questionnaires were filled by the patient with a research assistant, who did not participate in the treatment of these patients.
Patient Selection
Patients were selected using the peroneus longus activation test (Fig. 2) (Supplemental Video S1) (1). If the hallux valgus deformity was reduced axially and rotationally by lifting the toes and increasing the floor contact under the first metatarsal head, hallux valgus was classified flexible and FTJDA was performed. Possible gastrocnemius tightness was noted. If stretching did not help as a conservative treatment, an elongation was performed (1).
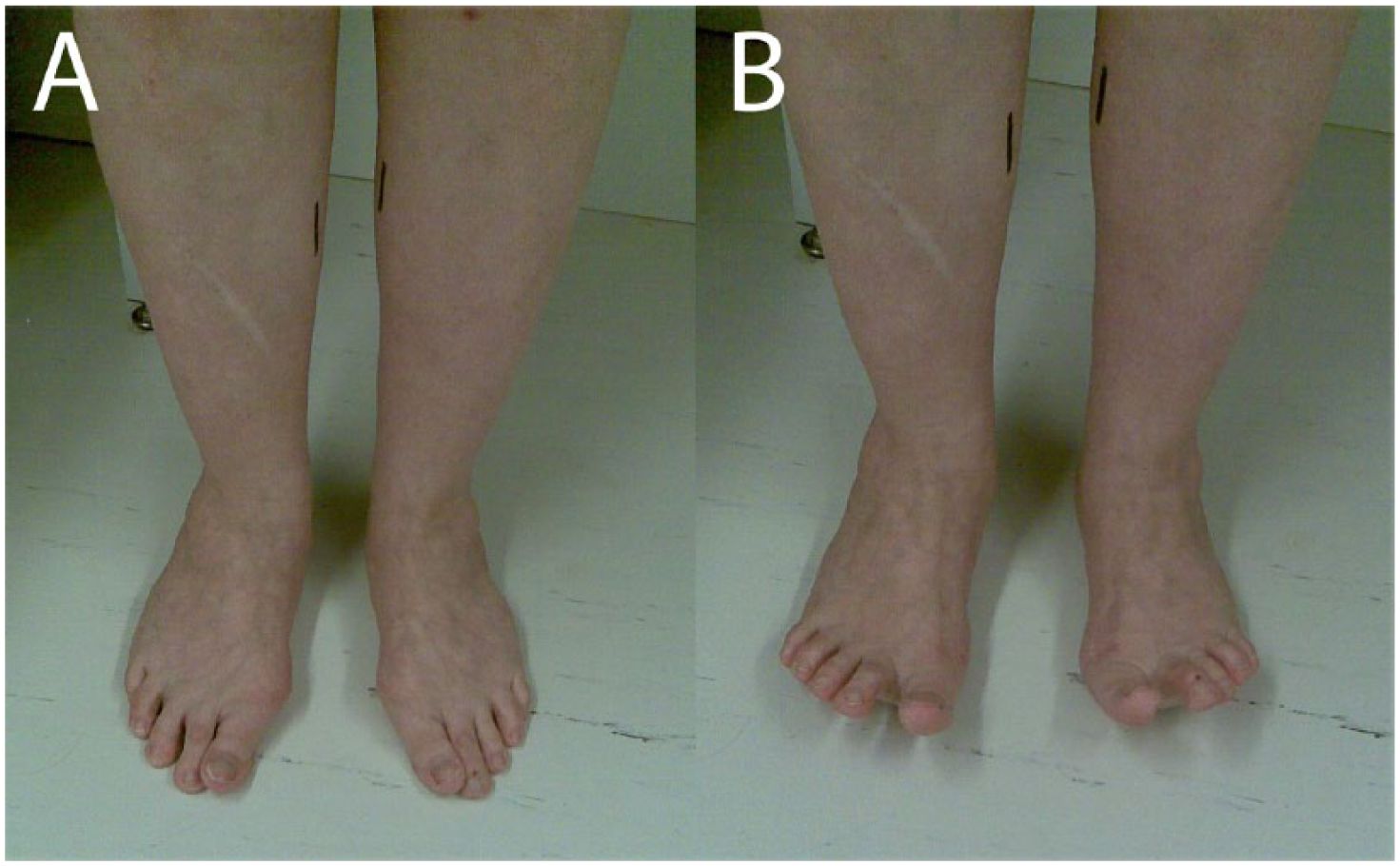
Peroneus longus activation test: (A) typical hallux valgus deformity with a “bunion” and marked pronation of the first toe. (B) When the first metatarsal head contact to the floor is increased and long toe flexor activity is eliminated by toe extensors, hallux valgus deformity is reduced in case of flexible hallux valgus, both axially and rotationally. A total correction of hallux valgus deformity with this test (as seen on the patient’s right foot) predicts good correction with first tarsometatarsal joint derotational arthrodesis, despite the radiological severity of the hallux valgus deformity.
Operative Technique
The aim of FTJDA was the axial and rotational correction of the first metatarsal bone without involving the first metatarsophalangeal joint or surrounding soft tissue (Fig. 1) (1). The original tarsometatarsal joint line was maintained in sagittal direction. The amount of rotational correction varied individually as eversion was limited by the second metatarsal base. Fixation was made in all cases with a single, headless, fully threaded cannulated screw with variable threads (Acutrak 4/5; Acumed® Corp., Portland, OR, USA). Hallux valgus was derotated from the pronated position to neutral, the first metatarsal head was reduced back on the sesamoids, and axial correction of the hallux and the first metatarsal were achieved when the correction was successful.
Postoperatively, a removable below-ankle-cast covering the first ray was used. Nonweightbearing was advised for 6 weeks. Immediate postoperative nonweightbearing radiographs were taken. Passive range of motion (ROM) of the first metatarsophalangeal joint was allowed 10 days after the operation, and weightbearing radiographs were obtained at 6 weeks. Peroneus longus and intrinsic muscle exercises, along with a gastrocnemius stretching program were advised at the 6-week control.
Radiological Measurements
Radiological measurements were supervised and in the latest follow-up done by a senior radiologist (R.O.) who did not participate in the clinical examination or operative treatment. Weightbearing radiographs in dorso-plantar and lateral projections were taken preoperatively, 6 weeks postoperatively, and at the late follow-up control. HVA and IMA 1-2 were measured from dorso-plantar images according to the guidelines of the AOFAS ad hoc Committee on Angular Measurements (22). Calcaneal pitch angle and Meary’s angle were measured from lateral weightbearing radiographs (23). The tibial sesamoid position was evaluated using the LaPorta classification (24, 25).
Statistical Methods
Summary measurements are presented as mean and standard deviation (SD) or as median with 25th–75th percentile unless otherwise stated. A linear mixed model (LMM) was used for repeatedly measured data. If the LMM showed significant change over time (ptime < .05), pairwise comparisons were performed. In LMM analyses, patient was set as random effect to take account that the operation was performed for both feet for some of the patients. The 95% confidence interval (95% CI) is presented with the mean change. Student’s t-test was used for groupwise comparisons. Two-tailed p values are reported. SPSS (IBM Corp. Release 2010, IBM SPSS Statistics for Windows, version 20.0 Armonk, NY: IBM Corp.) and SAS (version 9.3, SAS Institute Inc., Cary, NC, USA) were used for statistical analyses.
Results
Mean correction of HVA from preoperative to follow-up period values was 13.4 (95% CI: 11.6–15.1, p < .001), and mean IMA 1-2 correction was 4.5° (95% CI: 3.7–5.2, p < .001), respectively (Table 2, Fig. 3). The position of the tibial sesamoid relative to metatarsal bisector (LaPorta classification) was degraded by 1.1 units (95% CI: 0.9–1.4, p < .001) from 6 postoperative weeks to the end of follow-up. One (1.3%) foot was classified as LaPorta 7 when preoperatively 10 (12.7%) feet were in this group (Table 3).
Radiological results.
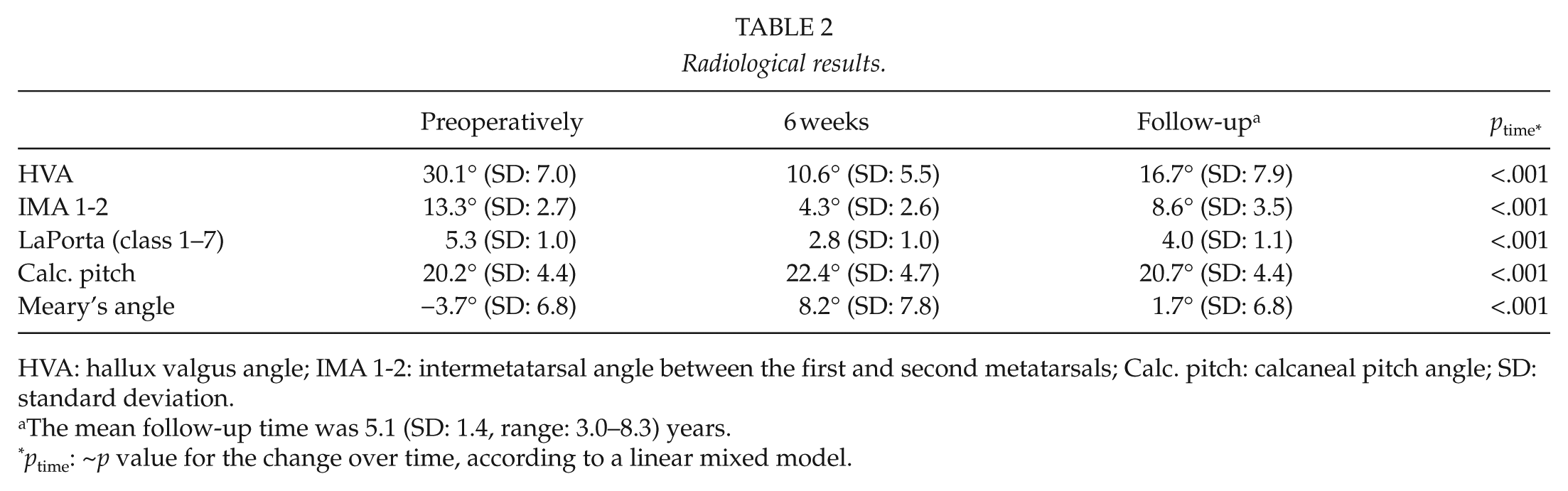
HVA: hallux valgus angle; IMA 1-2: intermetatarsal angle between the first and second metatarsals; Calc. pitch: calcaneal pitch angle; SD: standard deviation.
The mean follow-up time was 5.1 (SD: 1.4, range: 3.0–8.3) years.
ptime: ~p value for the change over time, according to a linear mixed model.

Radiological results: the left foot was operated with first tarsometatarsal joint derotational arthrodesis in 2005 (preoperative radiograph on the left). The late follow-up weightbearing radiograph was taken in 2012 (postoperative radiograph on the right). Preoperatively, HVA was 33° and LaPorta class 6. At the follow-up, HVA was 8° and LaPorta class 3. The AOFAS MTP-IP scale follow-up result was the maximum of 100 points. The metatarsophalangeal joint and surrounding soft tissues were left intact.
Effect of the operation on LaPorta classification in the long-term follow-up.
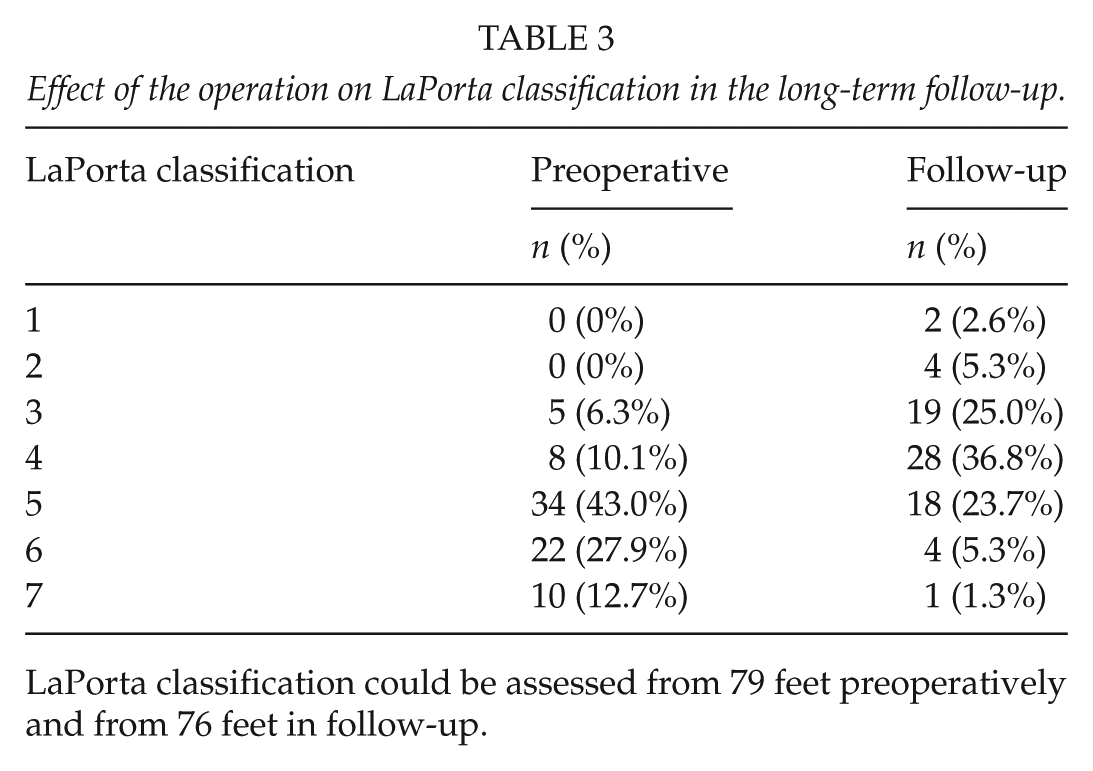
LaPorta classification could be assessed from 79 feet preoperatively and from 76 feet in follow-up.
The AOFAS (MTP-IP) clinical outcome score was excellent or good in 55 (72.4%) of the 76 operated feet at the latest follow-up. When the study cohort was divided into two groups by severity according to the preoperative HVA (⩽30° or >30°), mean postoperative AOFAS score was 88.9 (SD: 11.5) and 84.8 (SD: 14.8), respectively (p = .19). First metatarsophalangeal joint motion was normal or mildly restricted (ROM: 75° or more) in 72 (94.7%) of 76 operated feet according to the AOFAS (MTP-IP) clinical examination. The VAS showed a median of 0.2 points in pain (mean of 1.4 points; SD: 2.4) and a median of 0.3 points (mean of 1.3 points; SD: 2.1) in function as a follow-up result. For 66 (88.0%) of the 75 operated feet, patients reported a willingness to choose similar operative treatment under similar circumstances.
Seven feet (9.2%) needed eight (10.5%) reoperations during follow-up: three (4.0%) nonunions, one (1.3%) malunion, two (2.6%) hardware removals, and two (2.6%) recurrent hallux valgus. Additionally, there were three (4.0%) superficial wound infections and one (1.3%) sural nerve hyperesthesia related to surgery.
Discussion
This report is the first to describe the late follow-up outcome of FTJDA. The HVA decreased from a preoperative mean value of 30.1°–16.7° at a mean of 5.1 (SD: 1.4, range: 3.0–8.3) years postoperatively. The mean IMA 1-2 decreased from a preoperative value of 13.3°–8.6°, and LaPorta degraded by 1.1 units to a mean value of 4.0 at the final check-up.
In the prospective study of the Lapidus procedure, by Coetzee and Wickum (7), the HVA was reduced from 37° to 16° (mean of 3.7 years follow-up time). Another study by Pentikäinen et al. (26) of the distal chevron procedure showed a reduction in HVA from 26° to 20° with a mean follow-up time of 7.9 years. Faber et al. (27) compared Hohmann osteotomy and Lapidus in their prospective randomized trial with a mean follow-up time of 9.3 years. With the Hohmann procedure, HVA was improved from 32° to 11° at the latest follow-up, and with Lapidus, from 35° to 14° (27). Compared to this study, the patients were younger at the time of surgery in all of these studies with a mean age of 41, 39, 41, and 43 years, respectively (7, 26, 27) (Table 1). In this study, the mean HVA improvement was 13.4°, which is in good agreement with the earlier results (7, 26, 27).
Coetzee and Wickum (7) achieved notable correction of IMA 1-2 with the Lapidus procedure: a value of 18° was corrected to a mean of 8°. In a chevron cohort, IMA 1-2 was improved from 13° to 8° (26), with the Hohmann procedure from 13° to 7°, and with Lapidus, the reduction was from 14° to 7° (27). However, the effect of the nonanatomical shape of the first metatarsal on reliability of axial measurements after bunionectomy and/or metatarsal osteotomy should be considered critically. LaPorta was not reported in the mentioned studies (7, 26, 27). In our cohort, LaPorta was significantly (p < .001) corrected (Table 3).
In this study, the mean AOFAS MTP-IP scale value was 86.4 out of 100 points at the late follow-up. Mean AOFAS score did not differ significantly between HVA groups (preoperative HVA: ⩽30° and >30°), which suggests that the severity of hallux valgus is less important than the flexibility of the deformity. Coetzee and Wickum (7) reported an AOFAS MTP-IP score of 87 points as their late follow-up result, and Faber et al. (27) had a total of 82 points for Hohmann and 79 points for the Lapidus group at their late follow-up.
The median VAS for pain was only 0.2 points (mean of 1.4 points) and for function 0.3 points (mean of 1.3 points). Coetzee and Wickum (7) reported a mean VAS for pain of 1.3 points at their 3.7-year follow-up. In the study of Faber et al. (27) a mean late follow-up VAS for pain was 2 and 1 points in Hohmann and Lapidus groups, respectively. Comparison of the results of this study to the others has also limitations. Due to the retrospective nature of our study, we cannot present preoperative scores. Patient material also differs from the others because all the patients in this study had flexible hallux valgus.
A total of seven (9.2%) feet needed eight (10.5%) reoperations in this cohort. There were three (4.0%) nonunions during long-term follow-up. In addition, there was one (1.3%) malunion with a plantarflexed first ray that needed reoperation with corrective osteotomy. One (1.7%) patient had a too-long screw fixation, and one (33.3%) of the reoperated nonunions needed plate removal at a later stage. Two (3.5%) patients with recurrent hallux valgus were reoperated with metatarsophalangeal joint arthrodesis.
In this study, six (7.9%) feet were poor (scored less than 66 points) according to the AOFAS MTP-IP scale. Three (50.0%) of these were reoperated because of complications (two (33.3%) nonunions and one (16.7%) recurrent hallux valgus). One (16.7%) patient with an adjunctive Weil osteotomy had metatarsalgia of the second and third metatarsals at the late follow-up, and one (16.7%) patient had degenerative changes of the metatarsophalangeal joint in pre- and postoperative follow-up radiographs. There was no evident reason for a poor AOFAS result in one (16.7%) case.
We consider hallux valgus to be a severe dysfunction of the forefoot and windlass mechanism. The rotational component of hallux valgus deformity has been neglected in most, widely accepted hallux valgus correction methods. Operative treatment of hallux valgus should be aimed at restoring the forefoot stability and the function of the windlass mechanism. In the normal foot, first metatarsal head supports one-third of bodyweight during the propulsion (28). In their cadaver study, Perez et al. (29) demonstrated that frontal plane eversion of the first metatarsal increased sagittal stability, whereas inversion decreased it. In FTJDA, the eversion correction of the first metatarsal increased the sagittal stability according to the radiological results (Table 2).
The strengths of this study are the systematic clinical and radiological examinations of the patients, the mean of 5.1 (range: 3.0–8.3) years of follow-up and the high (90.5%) participation rate. Its limitations are its retrospective nature and the evaluation of outcome scores only at the latest check-up. The material of this study consists of clinically treated, FTJDA operated hallux valgus patients, who were not enrolled in any specific study protocol at the time of treatment. This is why the outcome scores were collected only at the latest follow-up.
This study took place at a single center, and operations were mostly done by a single surgeon (T.K.), who operated 74 (88.1%) of 84 feet. Altogether, five surgeons performed FTJDA procedures in the study group.
Patients who did not participate (eight (12.1%) patients, eight (9.5%) feet) in this follow-up study differed from the follow-up cohort in some respect. There were proportionally more men (two (25.0%) of men and six (9.7%) of women), nonparticipants were younger with a mean age of 38.6 (SD: 11.4) years, and their foot arches were more of the supination type (Meary’s angle 2.3°, SD: 7.5). Calcaneal pitch angle (24.4°, SD: 5.4) and IMA 1-2 (15.3°, SD: 2.8) were also slightly higher. The effects of these differences on the results were not considered clinically important. The results of this study indicate that flexible hallux valgus can be corrected without involving the metatarsophalangeal joint.
In conclusion, our clinical and radiological results indicate that FTJDA is an effective procedure for correcting flexible hallux valgus deformity and provides a satisfactory long-term outcome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the local ethical committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Level of Clinical Evidence
Level 4.