
Abstract
Background and Aims:
Massive transfusion protocol seems to improve outcome in massively bleeding trauma patients, but not pelvic fracture patients. The aim of this study was to evaluate the effect of massive transfusion protocol on the mortality and fluid resuscitation of shocked pelvic fracture patients.
Material and Methods:
This is a trauma register study from a single hospital. From the trauma registry patients with pelvic fracture, injury severity score >15, admission base excess below −5, age >15 years, blunt trauma, and primary admission from the scene were identified. Patients were divided into two groups: Group 1—pre-massive transfusion protocol (2006–2009) and Group 2—post-massive transfusion protocol (2010–2013). Basic characteristics and intensive care unit length of stay, mortality, and fluid resuscitation data were retrieved from the registry. Standardized mortality ratio was assessed using revised injury severity classification, version II methodology.
Results:
Altogether, 102 patients were identified. Group 1 (n = 56) and Group 2 (n = 46) were comparable in their basic characteristics. The observed mortality was 35.7% and 26.1% in Groups 1 and 2, respectively. The standardized mortality ratio failed to reveal any difference between observed and expected mortality in either group. In the emergency room, the use of crystalloids decreased from 5.3 ± 3.4 to 3.3 ± 1.8 L (p = 0.002) with increased use of fresh frozen plasma (2.9 ± 4.4 vs 5.1 ± 5.3, p = 0.007).
Conclusion:
No improvement in the adjusted survival of shocked pelvic fracture patients is apparent after implementation of massive transfusion protocol. Implementation of massive transfusion protocol is associated with a higher use of fresh frozen plasma and improved ratio of fresh frozen plasma:red blood cell toward the targeted 1:1 and decreased use of crystalloids.
Keywords
Introduction
Pelvic ring fractures after high-energy blunt trauma are seen in 10%–20% of patients (1). Pelvic ring fracture patients with hemodynamic instability experience mortality in up to 60% of cases (2). Local protocols are common for the treatment of these injuries, and there are no universally accepted protocols regarding the use of early angioembolization or pelvic packing (2).
Massive transfusion protocols (MTPs) in massively bleeding trauma patients are commonly used in order to improve the delivery of blood products from blood bank (3). Improved survival has been observed with the implementation of MTP and this has been attributed to increased fresh frozen plasma to red blood cell ratio (FFP:RBC) (4–7). However, many of these studies are biased toward the group of patients receiving high blood product ratios. Patients surviving longer receive higher FFP:RBC, but these patients may be less critically injured than those receiving lower ratios due to earlier death (3).
Damage control resuscitation with early coagulation factor replacement, limiting the use of crystalloids, reversal of acidosis and hypothermia, and early control of bleeding have been demonstrated to improve patient survival (4, 8–13). However, the use of MTP does not necessarily correct coagulopathy during the ongoing traumatic hemorrhage (14). Also, in a recent meta-analysis of massive-bleeding patients, the implementation of MTP failed to improve pooled mortality (3).
Implementation of MTP on the outcome of pelvic fracture patients requiring massive transfusion failed to show any effect on early or late deaths or on overall mortality (15). The majority of these patients died of exsanguination (15).
The MTP was implemented at the end of 2009 in the Trauma Unit of Helsinki University Hospital. The aim of this study was to evaluate the effect of MTP on the resuscitation and outcome of severely injured pelvic fracture patients. Our hypothesis was that the implementation of MTP improves the resuscitation and decreases the mortality of these patients.
Material and Methods
This is a trauma register study from a single trauma and tertiary referral center over an 8-year period (1 January 2006–31 December 2013). We identified all patients with pelvic ring fractures from the registry using Abbreviated Injury Scale (AIS) codes 8526xx.x (AIS version 1998 update and 2005). Other inclusion criteria were injury severity score (ISS) over 15, age over 15 years, primary admission from the scene, blunt mechanism of injury, and admission base excess (BE) below −5.
The MTP was implemented at the end of 2009 to our hospital. We divided the study period to two groups: (1) pre-MTP group, years 2006–2009 (Group 1) and (2) post-MTP group, years 2010–2013 (Group 2). We will compare the treatment and outcomes of these two groups.
All the data were obtained from the registry. We retrieved data from prehospital and hospital care, values of vital signs on admission and prehospital, initial laboratory values, fluid resuscitation and length of intensive care unit (ICU) and hospital stay, injury scores, and mortality. In our trauma registry, the fluid resuscitation is described separately for the prehospital phase, for the emergency room (ER) (regardless of the length of stay (LOS) in ER), and for the following 48 h after leaving the ER.
Glasgow Coma Scale (GCS) values on admission were used in this study. For prehospital intubated patients, we used the prehospital value before intubation. This methodology is used in revised injury severity classification, version II (RISCII) score (16). For mortality comparison, we did not compare the groups to each other but obtained standardized mortality ratio (SMR) for each group according to RISCII (16). Missing values are incorporated into the RISCII model, and thus, their effect on mortality does not need to be addressed otherwise. The RISCII model takes into account the heterogeneity of the trauma patient population and removes the need for further adjustment when using the SMR.
SPSS Statistics 21.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. For comparison between categorical variables, we used Fisher’s exact test, and for continuous variables, we used Mann–Whitney U test. The limit for statistical significance was set to Alfa <0.05 (p < 0.05). Values are expressed as mean ± standard deviation or as median with 25% and 75% interquartiles, as appropriate. The study protocol was approved by the Institutional Review Board (Helsinki University Central Hospital), and an ethical board review was not necessary for this study according to Finnish Law.
Changes in the Treatment of Pelvic Fracture Patients during 2006–2013
The changes and their implementation to clinical practice are shown in Fig. 1. Before the study period, unstable pelvic ring fractures were initially stabilized in the ER by external fixation, but during the study period, the main technique has been a commercially available pelvic binder (T-POD®; Pyng Medical Corp., Richmond, BC, Canada). The access and availability of angioembolization have remained the same throughout the study period. Trauma team simulation trainings have been running in our institution since the beginning of 2006. The trauma team protocol has remained mostly the same throughout the study period. Massive transfusion and fluid warmer (Fluido®; Sebac, Gennevilliers, France) have been in use in the ER since the end of 2006. Regular trauma meetings addressed to resuscitation and initial emergency surgical treatment for the whole staff commenced in 2008. The lack of morbidity and mortality meetings in our institution was considered as a major deficit, and thus, the trauma meetings were initiated. MTP was introduced in November 2009 in order to restrict the use of crystalloids and to change the resuscitation toward FFP:RBC 1:1. Restricting the administration of prehospital fluids in blunt trauma patients has been supported since 2009. Placing a warming mattress (Astopad®; Stihler Electronic GmbH, Stuttgart, Germany) under each trauma resuscitation patient has been standard protocol since 2010, in order to prevent patients from cooling during the initial trauma resuscitation. Damage control surgery cadaver training for all residents was initiated in 2012. Each resident has one training session per year.

Changes in the treatment protocols of pelvic fracture patients in Töölö Hospital during the study period (2006–2013).
During the study period, the main change in clinical practice has been the implementation of MTP. The fluid resuscitation had changed toward the use of more FFP and platelets in early phase before the implementation of MTP, but this was very dependent on the physicians in charge of the resuscitation. The physicians developing the MTP for our institution, and senior trauma consultants, already started to change the resuscitation practice toward a 1:1 ratio of FFP:RBC some months before the official implementation of MTP protocol. In addition, it took some months to fully implement the protocol to clinical practice. Thus, we consider the years 2009–2010 to be an evolvement period for 1:1 resuscitation.
Results
During the study period, 102 patients fulfilled the inclusion criteria, including 56 patients in Group 1 and 46 patients in Group 2. The basic demographics of these groups are shown in Table 1. These basic variables were statistically similar between the groups.
Demographics of the study groups.
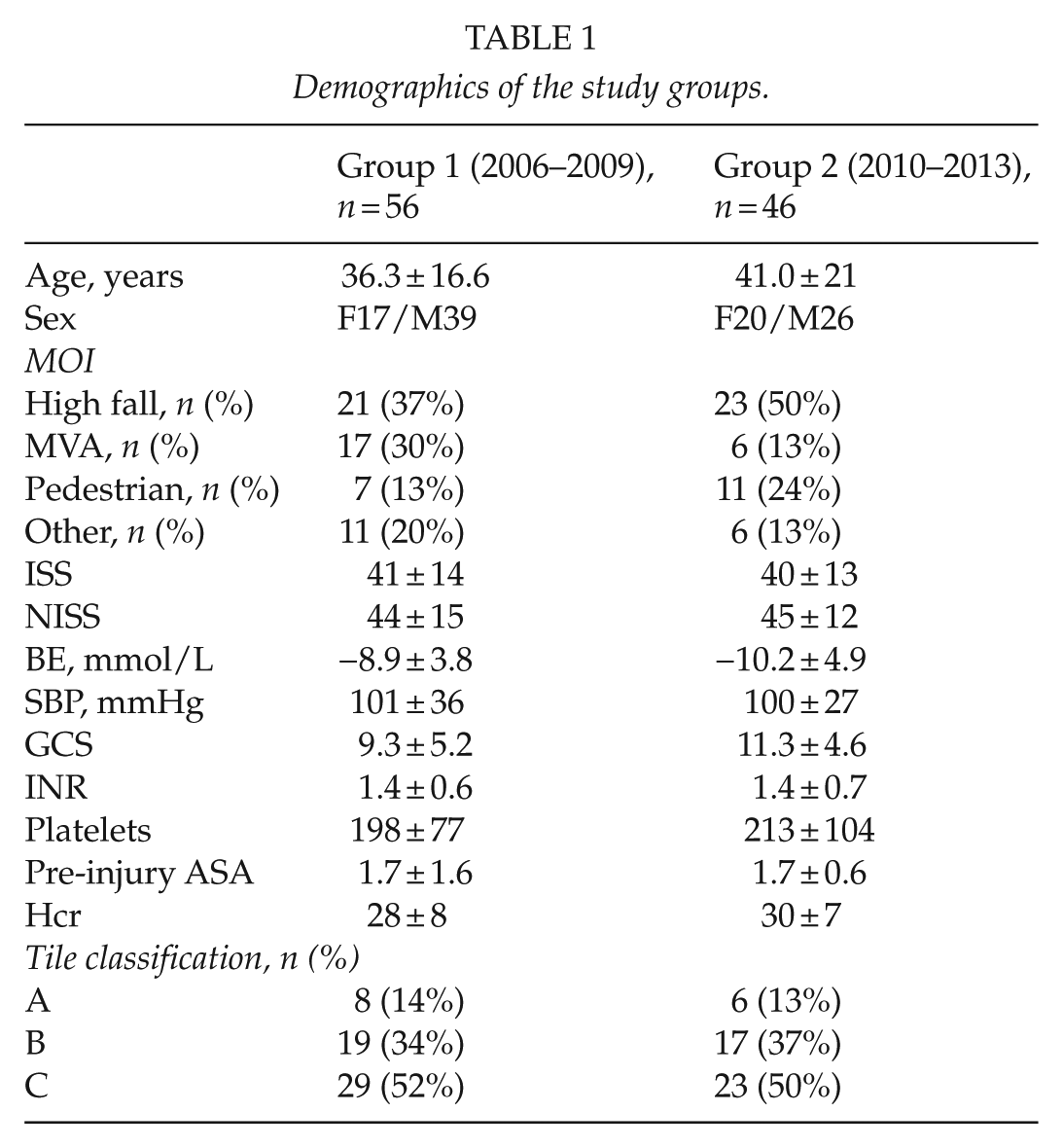
MOI: mechanism of injury; MVA: motor vehicle accident; ISS: injury severity score; NISS: new injury severity score; BE: base excess; SBP: systolic blood pressure; Hcr: hematocrit; GCS: Glasgow Coma Scale; ASA: American Society of Anesthesiologists physical status classification system.
Results are expressed as mean ± standard deviation or as percentage. Values of BE: Hcr, INR, Plt, and SBP are the first values measured on admission to hospital. GCS is the first value measured in admission. For prehospital intubated patients, we used the prehospital GCS value before intubation. In univariate analysis, we did not found statistically significant difference in any parameter between Groups 1 and 2.
The angioembolization of pelvic arteries was performed on seven (12.5%) and three (6.5%) patients in Groups 1 and 2 (p > 0.05), respectively. Whole-body computed tomography (CT) was done for 50 (89%) and 43 (94%) patients in Groups 1 and 2 (p > 0.05), respectively. The number of pelvic bleeders (defined as pelvic AIS 5) was 14/56 (25%) and 16/46 (35%) for Groups 1 and 2 (p > 0.05), respectively. Thus, we found no statistically significant changes in these parameters between the groups.
The rate of intubation increased from Group 1 to Group 2; however, there was no statistically significant difference in the rate of prehospital intubations (41% vs 63%) or intubations on admission (18% vs 30%) between Groups 1 and 2. When comparing the number of intubated patients leaving the ER, a significant difference was observed between Groups 1 and 2 (59% vs 94%, p = 0.001). There were no changes in the airway management protocols during the whole study period.
The patients stayed in the ER for an average of 165 ± 75 min (range: 35–430 min, median 148 min).
Changes in Fluid Resuscitation
The volumes of prehospital fluids decreased from Group 1 to Group 2, but this did not reach statistical significance (Table 2). The use of RBCs in the ER was unchanged between the groups, but the use of FFP was significantly higher in the ER in Group 2 (2.9 ± 4.4 vs 5.1 ± 5.3 units, p = 0.007). At the same time, the volume of crystalloids administered in the ER decreased almost 40% (5.3 ± 3.4 vs 3.3 ± 1.8 L, p = 0.002). The mean total resuscitation volume (all blood products and crystalloids) changed from 8.9 to 7.7 L with fraction of blood products increasing from 40% to 57%. In the 48 h after ER treatment, a large decrease (52%) in the crystalloids volume was evident, from 12.7 to 6.6 L (p = 0.001). There was a tendency for less RBC use in the 48-h period after ER in Group 2, but this failed to reach statistical significance (p > 0.05) due to the large scatter in the number of administered units.
Fluid resuscitation and outcome measures of the whole study population.
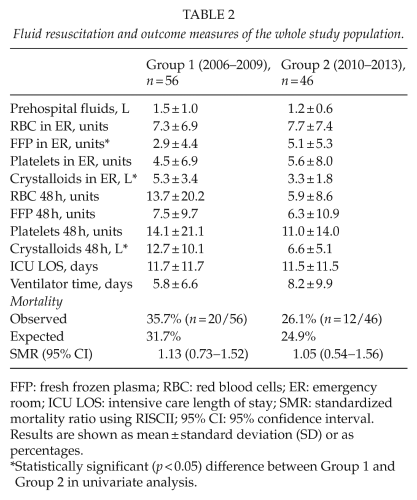
FFP: fresh frozen plasma; RBC: red blood cells; ER: emergency room; ICU LOS: intensive care length of stay; SMR: standardized mortality ratio using RISCII; 95% CI: 95% confidence interval.
Results are shown as mean ± standard deviation (SD) or as percentages.
Statistically significant (p < 0.05) difference between Group 1 and Group 2 in univariate analysis.
Changes in the Outcomes
The ICU LOS and time in the ventilator were similar between the groups (Table 2). Observed mortality decreased from 35.7% to 26.1% from Group 1 to Group 2. However, the expected mortality (by RISCII) also decreased (Table 2). There was a small decrease in SMR from Group 1 to Group 2 (Table 2). In both groups, the SMR was higher than 1, indicating higher mortality than expected. However, the 95% confidence interval spanned value is 1. This suggests that the observed mortality did not differ from expected mortality in either group.
Patients Receiving Blood Products in the Er
Only 44 (79%) and 35 (76%) patients in Groups 1 and 2 received blood products in the ER. The only statistically significant difference between Groups 1 and 2 in patients receiving blood products in the ER was first measured Hb (87 ± 25 vs 101 ± 25 g/L, p = 0.027). The FFP:RBC ratio was calculated only for patients receiving RBC in the ER. The median FFP:RBC ratio changed from 1:3.2 to 1:1.5 from Group 1 to Group 2 (p < 0.0001) in the ER. There was a large change in the relative volumes of the crystalloids versus blood products (RBC + FFP + platelets) given in the ER between the groups. In Group 1, the patients received a mean of 6.0 L of crystalloids and 3.8 L of blood products compared to 3.6 and 4.8 L in Group 2 (p < 0.0001). These changes caused the total resuscitation fluid volume (crystalloids and all blood products) in the ER to decrease from 9.8 ± 5.7 to 8.4 ± 4.2 L, and the fraction of blood products of this volume increased from an average of 39% to 57%.
The median FFP:RBC ratio in 48 h after leaving the ER changed from 1:1.6 (Group 1) to 1.1:1 (Group 2) (p = 0.002). The mean volumes for crystalloids in 48 h after ER were 13.8 ± 11.0 versus 6.8 ± 5.7 L for Groups 1 and 2 (p = 0.003), respectively. The median values of RBC administered in 48 h after ER were 5.0 units and 3.3 units in Groups 1 and 2, respectively. In both groups, 14 patients did not receive RBC during the 48 h following departure from the ER.
The total volume of blood products (RBC + FFP + platelets) in 48 h after ER was 7.7 ± 9.6 and 4.2 ± 6.0 L in Groups 1 and 2 (p = 0.188), respectively.
The use of blood products and crystalloids and mortality of the patients receiving RBC in ER are shown in Table 3. One elderly patient (85 years old) with multiple rib fractures and pelvic fracture died (due to pulmonary and cardiac failure) in the ICU without receiving any blood products in the ER. The observed and expected mortality were lower in Group 2 than in Group 1 (Table 3). Also, the SMR decreased from Group 1 to Group 2 (Table 3). However, the 95% confidence interval of SMR spanned 1 in both groups. Thus, there is no real difference between observed and expected mortality, or the number of cases is too low for detecting any real difference.
Fluid resuscitation and mortality in patients receiving RBC in the ER.

ER: emergency room; FFP: fresh frozen plasma; RBC: red blood cells; SMR: standard mortality ratio; 95% CI: 95% confidence interval.
Statistically significant (p < 0.05) difference between Group 1 and Group 2 in univariate analysis.
Discussion
We found a decrease in mortality in all shocked patients (admission BE below −5) with pelvic ring fracture from 2006–2009 to 2010–2013. However, the standard mortality ratio (assessed by RISCII) was unchanged during the study period for the whole study population. The results were similar in a subgroup of patients receiving RBC in ER. The observed mortality decreased from 2006–2009 to 2010–2013, but SMR was unchanged. The lack of difference in SMR may be due to the low number of cases.
In an earlier study by Fitzgerald et al. (15), the absolute mortality of pelvic fracture patients requiring massive transfusion (n = 100) showed a small (51% vs 45%) but statistically non-significant decrease after the implementation of damage control resuscitation. In this study, 79 patients required blood products in the ER. Among these patients, the absolute (crude) mortality decreased from 45.5% (Group 1) to 31.4% (Group 2). By considering unadjusted absolute mortality values only, it would seem that the implementation of MTP improved survival. We used RISCII (16) standard mortality ratio to overcome the possible differences in the basic characteristics of these small patient populations. The adjusted mortality (assessed by RISCII SMR) in shocked pelvic fracture patients receiving blood products in the ER was improved after the implementation of MTP, but this was not statistically significant.
A recent meta-analysis focused on studies comparing the results before and after implementation of MTP (3). All of these studies included only patients receiving 10 units of packed RBCs in 24 h. In the eight studies included (a total of 1586 patients), MTP associated with improved survival in only two studies (3). In our register, the amount of RBC within the first 24 h is not available.
The implementation of MTP did not change the administration of RBC in the ER but caused a significant increase in the early use of FFP in all shocked patients with pelvic fracture. The use of platelet concentrates increased slightly, but this was statistically non-significant in the whole study population. In the subgroup of patients receiving blood products in the ER (n = 79, 77%) the FFP use in the ER increased in Group 2 as well.
In patients receiving blood products in the ER, the FFP:RBC ratio changed from 1:3.2 to 1:1.5 and in the following 48 h from 1:1.6 to 1.1:1. The target FFP:RBC ratio is 1:1, and thus, this theoretical ratio was not reached in the early phase (ER). The ratio of FFP:RBC was reported unchanged after implementation of MTP by Sisak et al. (17) at 6 h after admission. In this study, the average time spent in the ER was 165 min, and only one patient stayed in the ER over 6 h. During this time, 77% of the patients received blood products. In these patients, the FFP:RBC ratio changed significantly from 1:3.2 to 1:1.5. An improvement in the FFP:RBC ratio after implementation of MTP has been reported in several studies (18–21). The main reason for the change of FFP:RBC ratio in this study was the increased use of FFP in the ER. This has been the reason for improved FFP:RBC ratios in other studies as well (18–21). The mean volume of blood products (RBC + FFP + platelets) administered in the 48 h after ER admission in patients receiving RBC decreased from 7.7 ± 9.6 to 4.2 ± 6.0 L. However, this was not statistically significant and may be explained by seven patients each receiving over 40 units of RBC.
The implementation of MTP included a principle of limiting crystalloid infusions in addition to improved blood product ratios. A significant reduction in crystalloid volumes was seen after implementation of MTP. In the ER, the volume of crystalloids decreased from 5.3 to 3.3 L in all patients. This effect was also seen in all patients in the following 48 h when the volume of crystalloids reduced from 12.7 to 6.6 L. A similar decrease in crystalloid infusion after MTP implementation has also been reported previously (10, 19). A similar decrease in crystalloid use was evident in patients receiving RBC in the ER. In these patients, crystalloid use decreased from 6.0 to 3.6 L in the ER and from 13.8 to 6.8 L in the following 48 h. We are not able estimate the effect of lower crystalloid volumes on patients’ overall tissue swelling, which could cause abdominal compartment syndrome or delay the open reduction and internal fixation of extremity fractures, from the registry data. Thus, the possible beneficial effect of smaller volume resuscitation on these parameters cannot be assessed in this study.
In this study, an obvious limitation is the low number of patients. Using the RISCII trauma risk adjustment model, we sought to overcome the limitation of the small number of patients on the effect of mortality. Thus, no adjusted comparison was made using only our patients, but we used the standard mortality ratio of RISCII, which was built using 30,866 cases and validated by another 21,918 cases (16). Missing values are a problem in registries when data are collected retrospectively (as in our register). The RISCII model includes missing values, and thus, no imputing or exclusion of these cases was required for SMR calculations. Due to the small number of cases, statistically significant differences are likely to be real. On the other hand, type 2 error, the lack of power to detect real differences, is possible as well. The lack of improvement in the SMR could present type 2 error. We collected all of the changes in the management of shocked pelvic fracture patients in our unit during the 8-year study period in Fig. 1. In our opinion, the main change in the treatment of pelvic fracture patients during the study period was the implementation of MTP. The effect of new protocols, such as MTP, needs to be critically evaluated after implementation. Also, reporting of negative or no effect of new protocols on outcome is important in order to reduce the risk of publication bias.
In conclusion, the implementation of MTP appears to have no impact on the adjusted survival of shocked pelvic fracture patients. Implementation of MTP is associated with higher use of FFP and improved ratio of FFP:RBC toward the targeted 1:1 and decreased use of crystalloids. Due to rapid improvements in the diagnosis and treatment of massive bleeding, and acute trauma coagulopathy, the impact of management changes requires frequent evaluation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.