
Abstract
Background and Purpose:
Dislocation is one of the most common complications following total hip arthroplasty. The aim of our study was to assess failure rate of the Biomet Freedom constrained liner (Biomet, Warsaw, IN, USA) either in revision surgery for recurrent dislocation, or as a preventive method in high dislocation risk patients.
Patients and Methods:
We assessed retrospectively 105 consecutive surgical procedures in 103 patients where a Freedom constrained liner or cup was used in Turku University Hospital over a 7-year period from 2007 to 2014. The mechanical failure rate of the device was assessed based on medical records. The average age of the patients was 73.4 years. The number of male patients was 53 (51%). Mean follow-up time was 2.5 years. The association between failure of the device and potential risk factors—age, gender, indication, and approach—was analyzed with logistic regression. Results were expressed by odd ratios and 95% confidence intervals.
Results:
The mechanical failure rate of the Freedom device was 6 out of 105 (5.7%). None of the 11 preventive primary THAs against dislocation failed, 4 out of 52 (7.7%) preventive revision THAs against dislocation failed, and 2 out of 42 (4.8%) of the treated dislocation cases failed. Four out of six failures were dislocations due to impingement and failure of the locking mechanism. Two liners failed because of loosening. The risk factors assessed were not associated with failure of the device.
Interpretation:
We found out that the mechanical failure rate of a Freedom constrained device was low. These results encourage us to continue using the device.
Keywords
Introduction
Dislocation is one of the most common complications following total hip arthroplasty (THA). Dislocation rates from less than 1% to greater than 10% have been reported after primary THA, although most studies report a prevalence of 2%–5% (1–3). The dislocation rate after revision THA is higher than after primary THA ranging from 7% to 15% (2, 4). Patients with Down syndrome, cerebral palsy, Parkinson’s disease, and dementia, lack of compliance due to alcohol abuse or neuromuscular diseases like poliomyelitis have an increased dislocation risk (5). Surgical approach and the type of implant used are also associated with dislocation rate (6, 7). Components positioning is one of the most significant things (8). Dislocations may be single episodes that do not require revision surgery. Surgical intervention is indicated after recurrent dislocations, or when an explicit surgical cause for dislocation has been identified. Surgical treatments used to address instability may include inserting longer necks or larger diameter femoral heads, correction of malpositioned components, dual mobility devices, or placement of a constrained liner. However, recurrence rates of 2% to even 55% after revision surgery have been reported (9, 10).
The aim of our study was to assess the failure rate of the Biomet Freedom constrained liner (Biomet, Warsaw, IN, USA) either in revision surgery for repeated dislocation, or as a preventive method in high dislocation risk patients.
Patients and Methods
We assessed retrospectively 105 consecutive surgical procedures in 103 patients where a Freedom constrained liner or cup was used in Turku University Hospital over a 7-year period from 2007 to 2014. Forty-four Freedom constrained liner applications were performed as a treatment of recurrent dislocations in revision THA. Eleven of the preventive constrained liner cases were used in primary THA, and 52 in revision THA. Indication for using a constrained liner in primary THA in the preventive group was neurological disorder in one case (Down syndrome), alcohol abuse in one, abductor deficiency in six cases, and trochanter major fracture in three cases. Indication for using a constrained liner in revision THA in the preventive group was abductor deficiency due to infection or an adverse reaction to metal debris in 19 cases, trochanter major fracture in 24, poor gluteal muscles in 3, dysplastic hip in 2, previous proximal femoral fracture in 2 cases, and alcohol abuse in 1 case.
The information concerning operative reports and follow-up visits were collected retrospectively from the electronic medical record database of the Turku University Hospital. The mechanical failure rate and revision rate for any reason after the Freedom constrained cup and liner application were assessed. Data cut-off was set at mechanical failure, and revision (preventive Freedom cup in primary THA) or re-revision (preventive Freedom liner in revision THA and treatment of recurrent dislocations in THA) for any reason by 14 November 2014 (Table 1). A total of 14 patients died during the follow-up time. Data collected included demographic information, indication for using a constrained device, amount of previous dislocations, reason for revision, type of revision, surgical approach, diagnosis of a neurological disease like Parkinson disease and Alzheimer disease or alcohol abuse, complications, re-operations, and death of the patient. The number of male patients was 53 (51%). The average age at the time of constrained component insertion was 73.4 years (range 40.1–92.2 years). The mean follow-up time was 2.5 years (range 3 days–7.5 years).
Patient characteristics at index surgery.
THA: total hip arthroplasty.
The Biomet Freedom constrained liner system is intended for use only in special situations where the patient has a high risk of dislocation due to a previous history of dislocation, severe joint laxity, and/or palsy of surrounding musculature and abductor muscle deficiency. The device incorporates an equatorial flat section at 15 degrees to the vertical axis along the sides of the Freedom liner and modular chrome–cobalt head, which is always 36 mm in diameter (Fig. 1A). The components are manufactured so that fluid creates a suction effect between the head and liner. The Freedom device provides 110 degrees range of motion, and lever-out strength of 198 inch-lbs (11). The acetabular liner can be locked into a standard locking mechanism for use in primary and revision acetabular components. A cemented version (Fig. 1B) is available for cementing into a well-fixed acetabular shell of differing locking design, or in cases when the locking mechanism is no longer functioning properly.
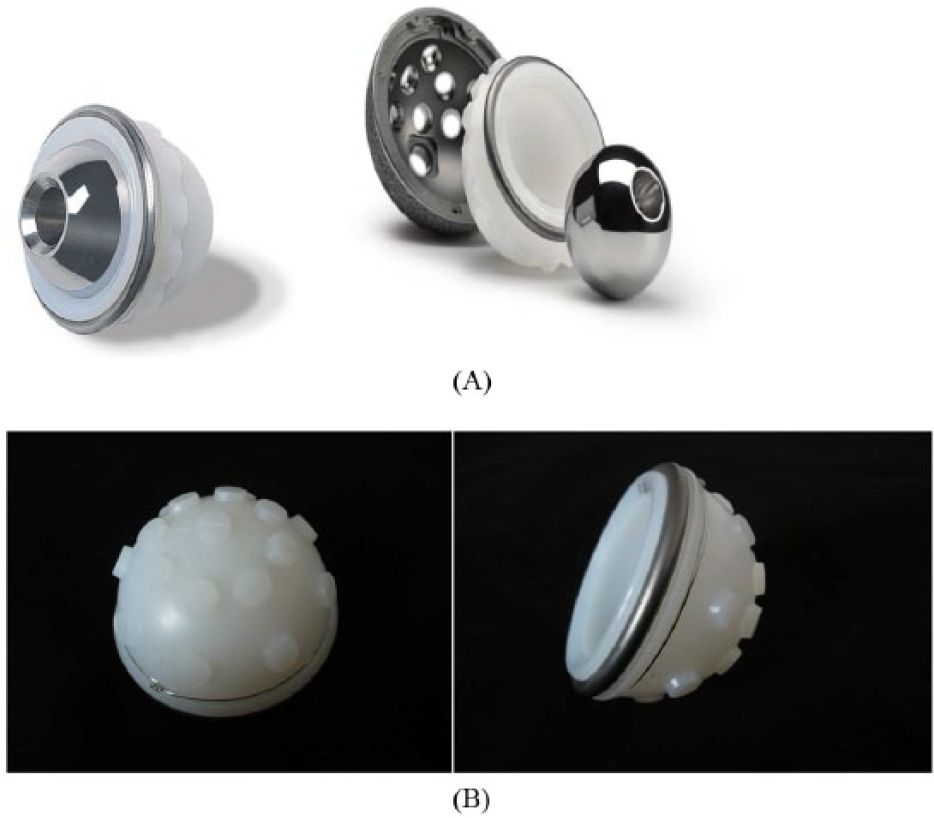
A) The Freedom constrained liner made of ArCom isostatically molded polyethylene, and a titanium constraint ring. B) The Freedom constrained cemented cup.
Fifty-eight Freedom liners were inserted into a Regenerex cup (Biomet, Warsaw, IN, USA), 15 into a Vision cup (Biomet, Warsaw, IN, USA), 10 into a Universal cup (Biomet, Warsaw, IN, USA), 16 were cemented into a Trabecular Metal revision shell (Zimmer, Warsaw, IN, USA), 4 were cemented directly into the acetabulum, 1 was cemented into an revision shell of another manufacturer, and 1 into a Universal cup.
In the preventive revision group, 32 Freedom liners were inserted into a Regenerex cup, 4 into a Vision cup, 3 cases into a Universal cup, 10 were cemented into a Trabecular Metal revision shell, and 3 were cemented directly into the acetabulum.
In the recurrent dislocation group 15 Freedom liners were inserted into a Regenerex cup, 11 into a Vision cup, 8 into a Universal cup, and 7 were cemented into a Trabecular Metal revision shell, and 1 into a Universal cup. Fourteen hips had dislocated once or twice, nine hips 3–4 times, three hips 5–10 times, and 16 hips more than 10 times when the Freedom device was inserted.
Statistical Analysis
Continuous variables were described by means and standard deviations (SDs) and categorical variables by frequencies and percentages. The associations between mechanical failure and risk factors were analyzed with logistic regression. Results were expressed by odd ratios (ORs) and 95% confidence intervals (95% CIs). The cumulative percentages for implant survival were estimated with the Kaplan–Meier technique for any reason of revision. P-values less than 0.05 were considered statistically significant. Statistics were run on the Statistical Analysis System (SAS) for Windows, Version 9.3 (SAS Institute, Inc., Cary, NC, USA).
Results
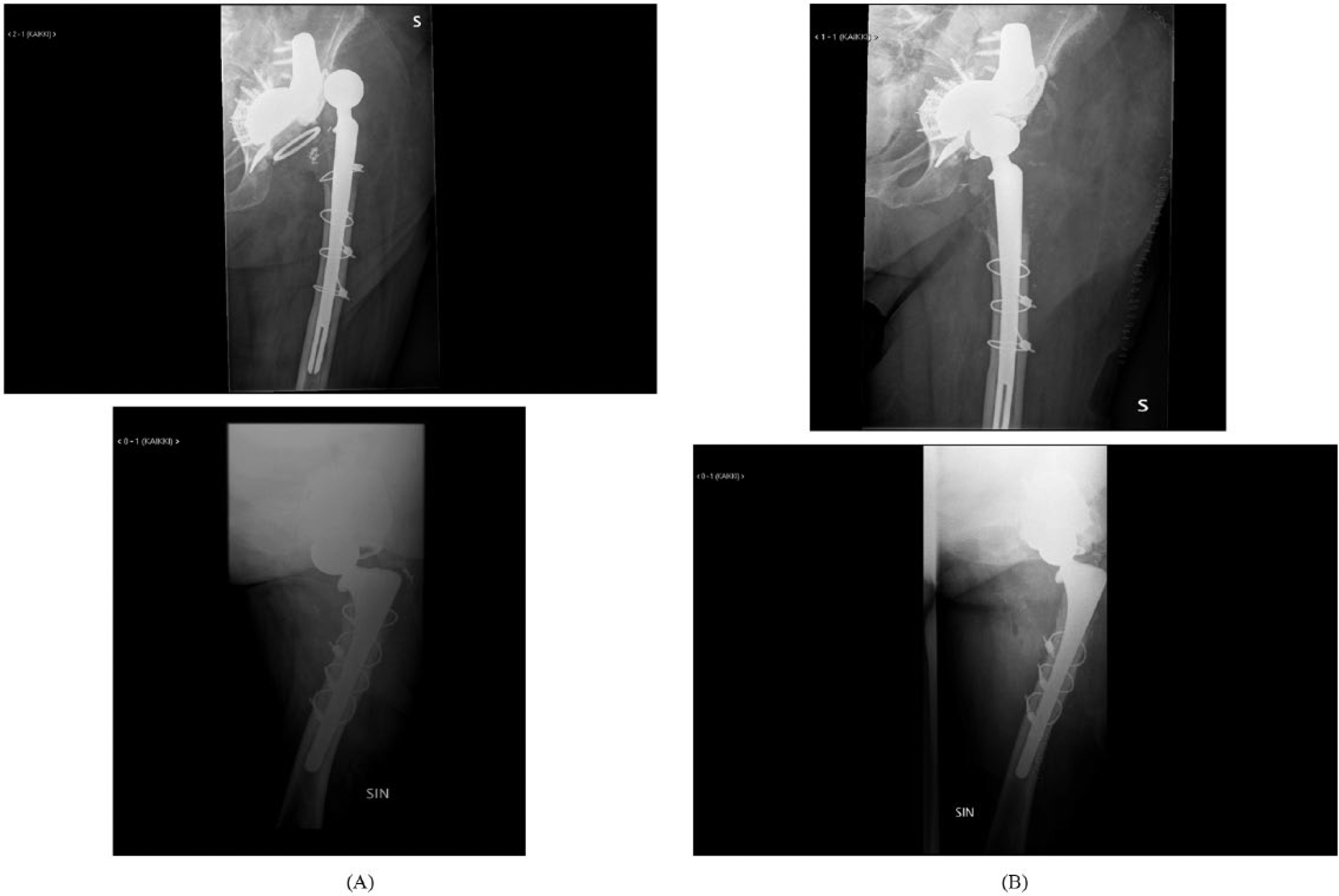
A total of 4 out of 105 Freedom constrained hips dislocated due to impingement and failure of the locking mechanism (Table 2, Figs 2 and 3). One Freedom liner, which was cemented directly into the acetabular bone loosened. One liner attached normally with the Ringloc mechanism into an uncemented cup loosened, probably due to impingement of the remaining osteophytes. So the mechanical failure rate of the Freedom device was 6 out of 105 (5.7%). None of the 11 preventive primary THAs failed, 4 out of 52 (7.7%) preventive revision THAs failed, and 2 out of 42 (4.8%) of the treated dislocation cases failed.
Characteristics of the patients and study devices of the dislocated and re-operated hips.
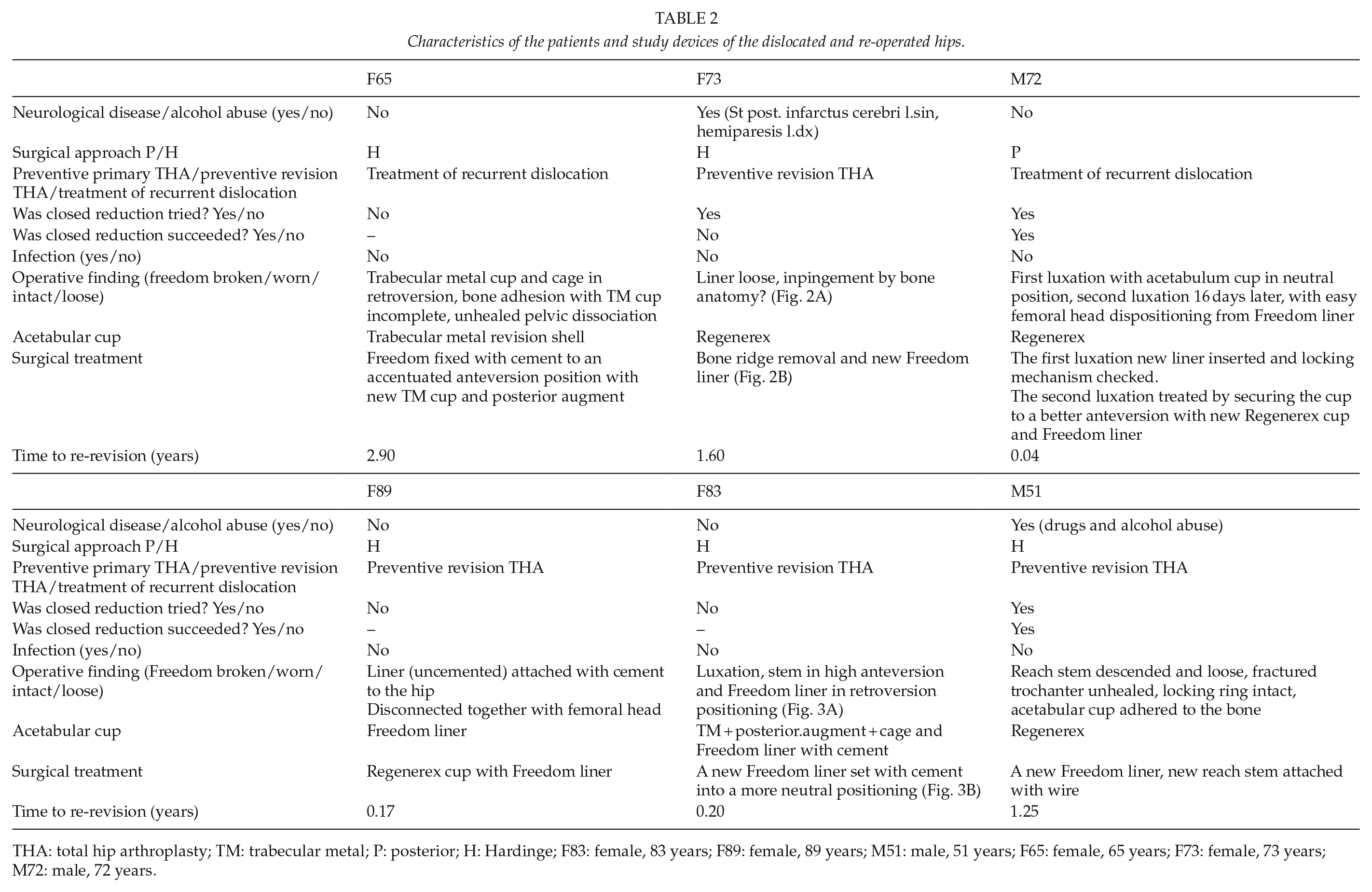
THA: total hip arthroplasty; TM: trabecular metal; P: posterior; H: Hardinge; F83: female, 83 years; F89: female, 89 years; M51: male, 51 years; F65: female, 65 years; F73: female, 73 years; M72: male, 72 years.
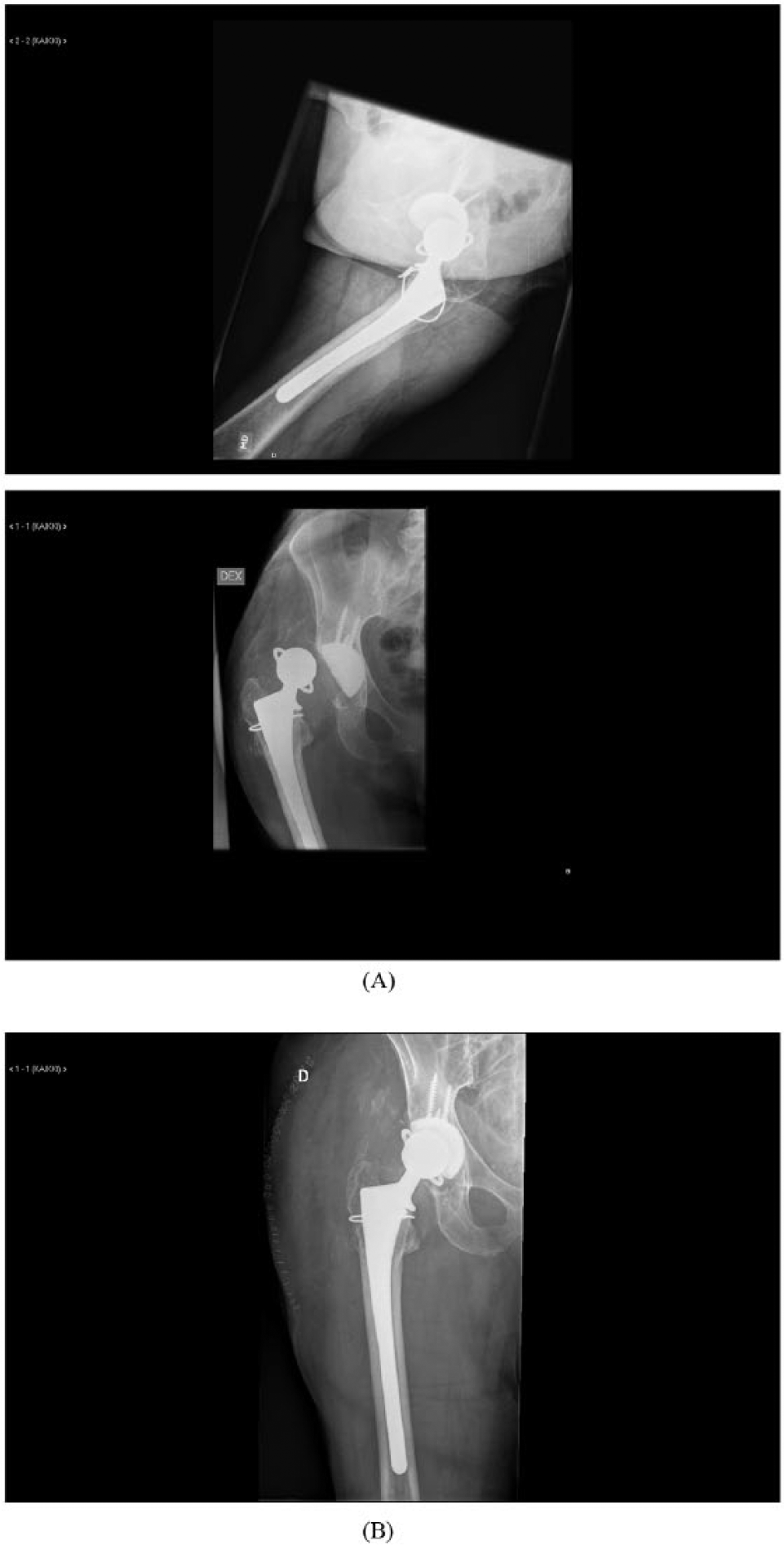
Female, 73 years.
Female, 83 years.
There were two infections which were treated by lavation and exchange of the modular parts, including Freedom liner and femoral head. Five-year Kaplan–Meier survivorship of the Freedom device for any reason of revision was 74% (Fig. 4). Mean time for failure after the index Freedom operation was 0.9 years (range 0.04–2.9 years).
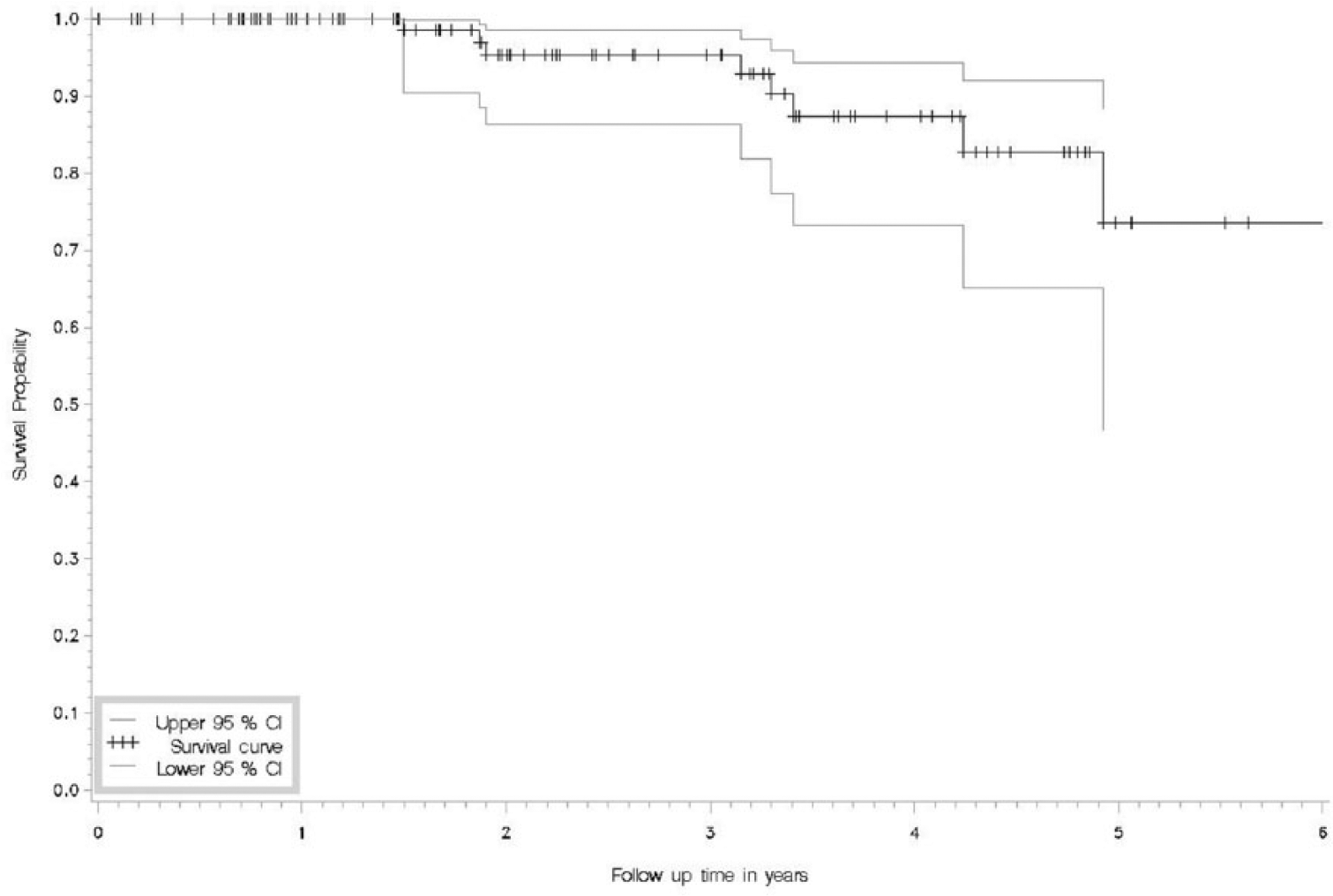
Kaplan–Meier survivorship of the Freedom device for any reason of revision with 95% confidence intervals.
The six mechanical failure cases are presented in Table 2. The results of logistic regression are presented in Table 3. Age, gender, indication, and approach were not associated with the failure of the implant.
Logistic regression results of the potential factors related to the failure of Freedom constrained device.
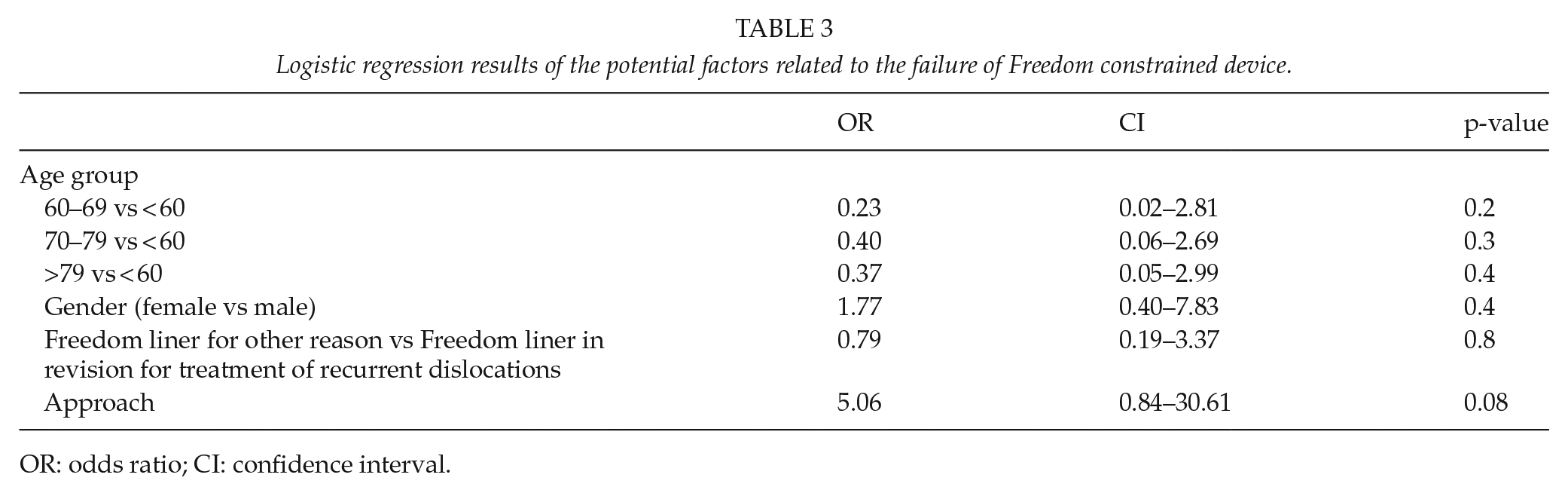
OR: odds ratio; CI: confidence interval.
Discussion
We found out that the mechanical failure rate of a Freedom constrained device was 5.7% in a mean follow-up of 2.5 years. These results encourage us to continue using the device.
Recurrent instability after THA is a challenge for the arthroplasty surgeon. Rates of dislocation after revision or primary hip arthroplasty for patients at risk of instability are still ranging from 6% to 20% despite various surgical solutions proposed (2, 12). Since constrained acetabular liners are used to resolve instability arising from various causes, they act as a mechanical substitute for poor biologic support and are subjected to mechanical overload. The higher forces transmitted through the constrained articulation can contribute to reconstruction failure. The four modes of failure of a constrained device are failure of fixation to the pelvis, liner dissociation, biomaterial failure, and femoral head dislocation (13, 14). Impingement is a common underlying cause in each mode of failure, and may occur with every constrained liner (15). The femoral head is captured deeper into the polyethylene, leaving the femoral neck vulnerable to contact against the comparatively elevated liner rim. High forces lead to liner dissociation and femoral head dislocation depending on the design. The repetitive impingement forces that occur within a reduced arc of motion generate polyethylene fatigue fractures and locking mechanism failure (14).
Noble et al. (15) retrieved 57 constrained components of 4 different designs (45 S-ROM® liners (DePuy Orthopedics, Warsaw, IN, USA), 8 Trilogy Longevity Constrained (TLC) liners (Zimmer, Warsaw, IN, USA), 3 Duraloc liners (DePuy Orthopedics), and 1 Freedom liner)) at revision THA and examined for the presence of rim impingement, cracks within the liner, and backside wear. Failure of the locking ring was responsible for 51% of failures, whereas 28% of revisions were the result of acetabular cup loosening, 6% backside wear, and 22% infection. Impingement damage of the rim of the polyethylene liner was seen in all retrievals. In the current study four out of eight (50%) Freedom failures were dislocations due to impingement and failure of the locking ring, two of the eight liners failed for loosening (25%), and two for infection (25%). Our data give support to findings of Noble et al. (15), although their study was composed of mainly other constrained devices. There are several reports of constrained liners that were cemented into the shell and subsequently dissociated from the cement (16–18). Failures at the acetabular bone–prosthesis interface due to inadequate fixation of the shell and increased bone-implant interfacial stress are also well described (13, 19). In our failure case, the Freedom liner, not the Freedom cemented cup, was cemented directly into the pelvic bone, and dissociated only after 2 weeks. This method may be inadequate.
The mechanical failure rate of Freedom constrained liner in the current study (six out of 105 (5.7%) at a mean follow-up of 2 years) compares favorably with other reported series of comparable devices. According to Berend et al. (11), the success rate of a Freedom constrained liner in a follow-up on average of 9 months was 98.8% when treating dislocation of primary THA (one dislocation of 81 THAs), and 93% for patients for whom a constrained device was placed during revision for recurrent instability . Four of 82 TLC devices inserted for primary (n = 10) or revision (n = 72) THA failed in a study of Munro et al. (20) with a mean follow-up of 34 months. Three of the liners failed due to dislocation, and one for loosening of the cup. Andersen et al. (21) stated that four TLC constrained devices of 32 inserted for recurrent dislocation failed due to dislocation, and one due to cup loosening at a 1.8-year follow-up. Zywiel et al. (22) studied Trident constrained liner (Stryker Orthopaedics, Mahwah, NJ, USA) in 33 revision THAs with a previous history of dislocation, and in 10 revision THAs with intraoperative instability. Thirty-nine of the 43 hips required no further re-operation of the acetabular component and/or liner over the study period, for an overall survival rate of 91% at a mean follow-up of 49 months. Berend et al. (23) have demonstrated the relationship between preoperative history of dislocation and recurrent dislocation rate using S-ROM constrained liner. Recurrent dislocation occurred in 14% of patients without a history of dislocation and 28% of those with a previous history. When the constrained device was inserted for with the diagnosis of recurrent dislocation, the re-dislocation rate was 29%. The failure rate of the Freedom device in the current study as a treatment of dislocation was only two out of 42 (4.8%), although there were 16 hips with a history of more than 10 previous dislocations. Della Valle et al. (24) reported a recurrent dislocation rate of 20% in those patients undergoing Duraloc liner insertion for recurrent dislocation. In the same report, they demonstrated that isolated exchange of the liner to a constrained mechanism without optimizing additional factors that may contribute to instability like malposition of femoral and acetabular component is associated with a high rate of failure (24). We agree that appropriate decision-making and optimal component positioning in dislocation revision surgery is mandatory for the success of preventing further dislocations using any device.
Hernigou et al. (5) compared primary THA performed on patients with neuromuscular disease with a constrained device (Groupe lepine, Genay, France) in 164 hips and conventional heads 132 hips. At a minimum follow-up of 5 years, the dislocation rate in the constrained group was 2% and 25% in the conventional group. None of preventive primary THA cases in the current study failed, which supports the finding of Hernigou et al. (5). However, the constrained device was not the same in these two studies. Furthermore, most of our cases were abductor deficiency or trochanter major fracture patients compared to neurological patients in the previous study. Anyhow knowing the high dislocation rate after THA in neurological and muscle deficiency patients, the use of preventive constrained liners should probably be further encouraged in these patient groups.
A major concern with any locking ring-style constraining device is that recurrent dislocation almost always requires open reduction and revision. Some reports have indicated that closed reduction of dislocated constrained THAs is possible in some cases at least using S-ROM (25–27), or Trilogy liner (28). Harman et al. (27) showed that six patients who had a successful closed reduction remained stable without any additional dislocations 7–72 months after reduction. Sonohata et al. (28) stated that the Trilogy hip remained stable for 10 months when the patient died for unrelated causes. These data suggest that closed reduction of constrained polyethylene liners can be successful without predisposing patients to additional dislocations. In our study, three out of six failed Freedom hips were tried to treat initially with a closed reduction, two out of three attempts were successful. However, all the three cases needed revision surgery later on due to continued dislocation problem. Clyburn et al. (29) reported a cadaveric biomechanical evaluation, which demonstrated that with recurring dislocation, the torque to dislocate was reduced. They recommended consideration of revision surgery if dislocation occurs. Our data support this recommendation.
A limitation of our retrospective study is that it lacks a comparison group. We did not have a defined list of indications for using a constrained liner. Some of our revision patients had complex acetabular and femoral reconstructions and multiple medical comorbidities. Some of the general complications (i.e. infection) were not related to the use of the constrained liners. The downside of the constrained devices include limitations of range of motion and an increased risk of impingement between the femoral neck and the constrained liner, potentially transferring high stresses at the bone–implant interface. This may change the mechanism of failure from dislocation to loosening and wear (15). The follow-up time in our study was relatively short and evaluation of the potential long-term complications like wear, osteolysis, and loosening was not possible. Furthermore, assessment of function or quality of life was not included, because this was not routinely recorded at subsequent follow-up visits. The strength of our study is that we were able to assess the outcome of an entire cohort of a single constrained device in one specialized joint arthroplasty center. We are aware of only one previous retrospective study of the dislocation rate of Freedom device (11).
Why it is wise to use this liner?
Mechanical failure rate of the Freedom device is low;
Easy to use;
Available both cemented cup and uncemented liner.
Why it is skeptical to use this liner?
The cup should be in good position when inserting the Freedom liner;
Data on durability of the locking mechanism in the long-term is not available yet;
Long term data of aseptic loosening of the cemented Freedom cup are not available.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.