
Abstract
Background:
To prospectively assess the functional effect of using the extended latissimus dorsi flap in immediate breast reconstructions.
Materials and Methods:
A total of 15 consecutive patients undergoing breast reconstruction with extended latissimus dorsi flap participated. Shoulder range of motion, muscle strength, lateral flexion of the torso, and position of scapula were measured pre-operatively and 1, 6, and 12 months post-operatively, in addition to donor-site post-operative complications.
Results:
At 12 months post-operatively, patients had achieved full range of shoulder movement, when compared to pre-operative values. Lateral flexion of the torso was, however, significantly reduced bilaterally at 1 and 6 months post-operatively (p = 0.001, p = 0.01) and to the not operated side at 12 months (p = 0.01). Muscle strength in flexion–extension–internal rotation was significantly (p = 0.01) reduced on the operated side 12 months post-operatively. All but one patient had numbness around the donor-site scar 12 months post-operatively, 33% had slight adhesions but all were pain free.
Conclusion:
Although invariably, patients having extended latissimus dorsi flap may expect to achieve full range of shoulder movement, they should be informed of possible functional consequences and the time and effort it takes to recover. Further research is needed to investigate the potential long-term functional implications that extended latissimus dorsi flap may have as a result of changes in the lateral flexion of the torso and scapula position.
Keywords
Introduction
Although breast reconstruction with latissimus dorsi flap (LDF) has been used for decades (1–4) and is considered to be associated with minimal donor-site morbidity (5, 6), relatively few studies on the functional consequences of its removal have emerged and with conflicting results (7–14). Furthermore, they have for the most part assessed the range of motion of the shoulder joint (15) although some studies have reported loss of muscles, strength and range in shoulder extension, and adduction (10, 15–17). These initial deficiencies have been suggested to resolve in the vast majority of women within 6–12 months (16, 17). No study has measured muscle strength in the combined movement of extension, adduction, and internal rotation of the latissimus muscle, or on other possible dysfunctions that could be expected from functional loss and decreased volume of the muscle together with scar tissue such as lateral flexion of the torso and position of scapula.
Latissimus dorsi (LD) muscle originates from the seventh to twelfth thoracic vertebrae, the thoracolumbar fascia, the posterior third of the iliac crest, from the tenth to twelfth ribs, and often from the inferior angle of the scapula (18). Its insertion is at the crest of the lesser tubercle (18). The function of the LD muscle is to lower the raised arm, adduct, extend, and internally rotate it so the back of the hand can touch the opposite buttock (18, 19) it also acts in downward rotation (19) and depression of the scapula together with lateral flexion of the torso (11). When both latissimi act together, they can pull the shoulders backward and downward (18).
Acting with pectoralis major and teres major, it helps in depressing the raised arm against resistance and to pull the spine upward and forward when the arms are fixed above the head, as in climbing (19).
Considering the widespread origin of the latissimus muscle from the lower thoracic spine and thoracolumbar fascia, it could be expected that lack of unilateral muscle tension from it would have an effect on the spine. This has not been assessed specifically in LDF studies, although Kim and Glazer (20) concluded in a case report that “latissimus harvest may have a destabilizing effect on the thoracolumbar spine in the long term, especially in patients with pre-existing scoliosis.” We, therefore, wanted to investigate whether removal of the latissimus muscle flap on one side together with adhesions can result in changes in lateral flexion of the torso.
Spinal curvatures including scoliosis have mainly been assessed by radiography. In order to decrease repeated radiation exposure, attempts to develop skin-surface instruments for examination of spinal curvatures have been developed. Several non-invasive measurements are now available ranging from tape measure to computerized motion analysis systems (21).
The purpose of this prospective follow-up study was to investigate the functional effects of immediate breast reconstruction with extended latissimus dorsi flap (E-LDF) on the shoulder joint range of motion, muscle strength in the combined action line of latissimus muscle, lateral flexion of the torso, position of scapula, combined with assessments of pain, skin sensation, and adhesions around donor site.
Materials and Methods
Subjects in this cross-sectional cohort study were recruited from 27 February 2012 to 9 September 2013. All consecutive breast cancer patients undergoing mastectomy and E-LDF reconstruction were asked to participate in the study until 15 were included.
The Data Protection Authority and the Ethical Committee of Landspitali-National and University Hospital (SN 13/2011) approved the study protocol. All patients gave written informed consent prior to participation. All patients were operated on by the same surgeon (K.S.A.) and functional measurements were performed by the same physiotherapist (H.E.).
Surgical Procedure
Drawings on the breast and back were done pre-operatively. On the back, the drawings were made so that the scar was positioned in line with the bra strap on the back. Initially, drawings were made so that the scars would be oblique on the back, but in the latter half of the study the scars were drawn so that they would be more transverse, extending obliquely toward to axilla to minimize the risk of dog-ear formation. A skin-sparing mastectomy through a circumareolar or circumareolar/vertical incision and an axillary sentinel node or lymph node dissection was performed with the patient in a supine position. The patient was then positioned on the side and the thoracodorsal pedicle better identified and side branches clipped to minimize tension on transposition of the flap. The serratus anterior branch of the thoracodorsal pedicle was routinely clipped. Although theoretically conceivable, that clipping of the serratus branch of the thoracodorsal pedicle may affect blood supply to surrounding tissues and add to scar tissue formation; it was done primarily to reduce kinking of the pedicle, thereby decreasing possible venous congestion and also increasing the mobility of the flap on transposition into its new position. The immediate E-LDF mobilization was then performed in the manner described by Delay et al. (22). The flap was then transposed from the back to under the breast skin via the axilla and the tendon of the muscle at its highest possible level was then transected and sutured to the lateral border of pectoralis major and serratus anterior muscles. The thoracodorsal nerve was always left intact. Quilting sutures between the superficial fascia of the skin of the back and underlying muscle fascia was performed in all cases, and skin closed in three layers with 2.0 PDS and 3.0 and 4.0 monocryl. The patient was then again put in a supine position; the shaping of the flap was then performed and all patients had immediate nipple reconstructions.
Shoulder Range of Motion
Bilateral range of motion of shoulder joint was assessed visually and measured with goniometry. In the standing position, patients were asked to actively move their arms through full flexion–extension, abduction–adduction and then rotate laterally and medially with elbows flexed 90°. When motion was assessed to be incomplete, the range was measured with goniometry. Reliability of shoulder joint goniometry has been tested, and inter-test reliability and intra-test reliability were found to be excellent (23, 24).
Muscle Strength Measurement
Muscle strength through the range of motion of LD muscle action (from 100° anatomical flexion through extension, adduction, and medial rotation) was measured using pulleys and weights. The maximum weight the patient could move through the whole range without bending the spine or elbow was recorded.
Push-up from a chair
Sitting in a straight back chair with arm rests, patients were asked to push up with their knees extended. The result was rated on a scale from 0 = could not do it, 1 = could free the behind from the seat, and 2 = could complete the push-up with straight elbows.
Lateral flexion of the torso was measured bilaterally using the Spinal Mouse (Idiag, Switzerland), which is a computer-aided skin-surface device housing accelerometers which records distance and changes of inclination with regard to a plump line as it is rolled along the length of the spine (21).
Procedure
The patients were undressed to the waist, barefoot, and asked to stand upright, facing forward in a relaxed position. The spinal processes were marked with cosmetic pencil from C7 to S3. The Spinal Mouse was placed over C7 and glided down all spinal processes down to S3 holding the Spinal Mouse perpendicular to the spine ensuring that both wheels were in contact. Data recorded were transmitted via bluetooth to a computer. Then, the patients were asked to perform bilateral flexion and the procedure with the Spinal Mouse was repeated.
Position of scapula
The horizontal distance between the basis of scapular spine and spinous process of third vertebra was measured bilaterally with tape measure and the vertical distance between the inferior angle of scapula and the highest point of the iliac crest (Fig. 1).
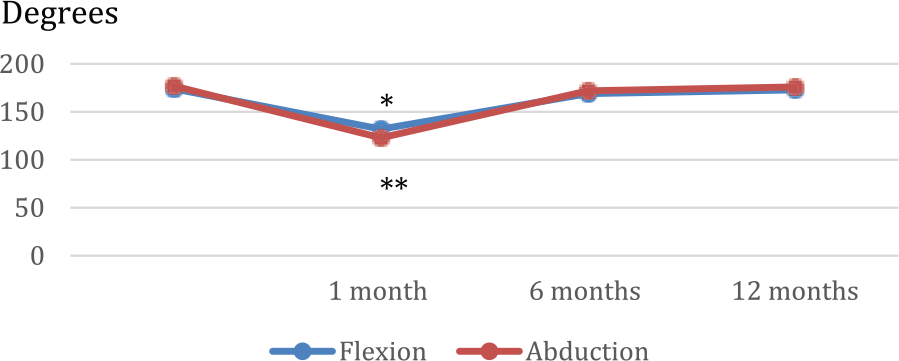
Post-operative range of shoulder flexion and abduction following E-LDF compared to pre-operative range.
Measurements of shoulder and spine motion, muscle strength, and position of scapula were repeated 1, 6, and 12 months post-operatively and when analyzed, grouped into results from the operated side and the not operated side.
The following assessments were also performed 1, 6, and 12 months post-operatively: pain was assessed using a numeric rating scale where 0 = no pain and 10 = worst possible pain. Altered sensation on the back was assessed with palpation and recorded as either present = 1 or not = 2 and if present the type and location was recorded. Adhesions were assessed by palpation of the wound and surrounding area while mobilizing the tissue and were scored semi-quantitatively according to the following: no adhesion = 0, slight adhesions = 1, medium adhesions = 2, and severe = 3. The location of the adhesion was also recorded.
Post-operative physiotherapy
On the second post-operative day, the same physiotherapist (B.H.) provided instructions on exercises to do daily, both personally and on-paper, and on exercises to do daily while an inpatient. On discharge, they were instructed to do these exercises twice daily. Four weeks post-operatively, they received individual physiotherapy during the same visit, after the abovementioned measurements were performed.
The physiotherapy consisted of myofascial release of the donor area, mobilization of the shoulder on the operated side, exercises and stretches to increase flexibility, and muscle strength of the back and shoulder.
Statistical analysis
Descriptive statistics were used for calculating means and standard deviations of demographic data and range of shoulder flexion and abduction. For comparison of shoulder joint movements, Wilcoxon signed-rank test was used as the data were not normally distributed. The SPSS computer program was used for calculations. Significance was set at p ⩽ 0.05.
Results
Study group demographics are presented in Table 1. One woman was excluded because she had surgery for pulmonary metastasis. Among the 15 included, 2 women had previously had a contralateral mastectomy 2 years previously and 2 had fibromyalgia, one of which had prolapsed lumbar disk 12 years prior to inclusion in the study. She had been symptom-free for several years. All women were right-handed. Axillary node clearance was performed in seven patients, and sentinel node biopsy in seven. All patients had a fully autologous breast reconstruction, that is, none had implants in addition to the flaps. The mean inpatient hospital stay was 3.5 days.
Study group demographics.
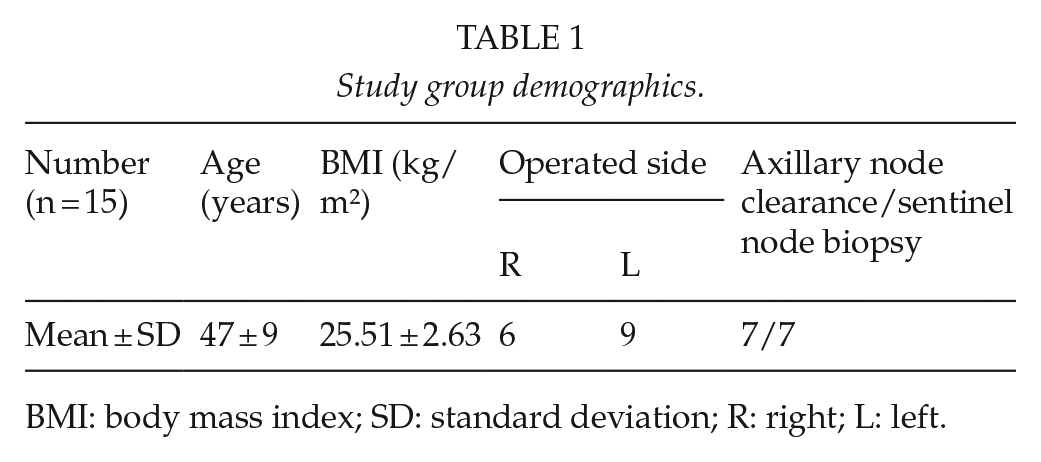
BMI: body mass index; SD: standard deviation; R: right; L: left.
Assessments at Baseline and 1, 6, and 12 Months following E-Ldf
Shoulder flexion and abduction
On the operated side, average shoulder flexion and abduction were the only movements that had changed significantly (p = 0.01 and p = 0.03, respectively) 1 month post-operatively compared with pre-operative values. At 6 months, average flexion and abduction was slightly (5°) but not significantly less than pre-operative values, and at 12 months, patients had achieved full range of shoulder movement when compared to pre-operative values (Fig. 1).
Muscle strength
Fig. 2 demonstrates differences in muscle strength in full range of the action line of the latissimus muscle between the operated side and not operated side pre-operatively and 1, 6, and 12 months post-operatively. Significant differences were found at 1 and 12 months (p = 0.001 and p = 0.01, respectively).
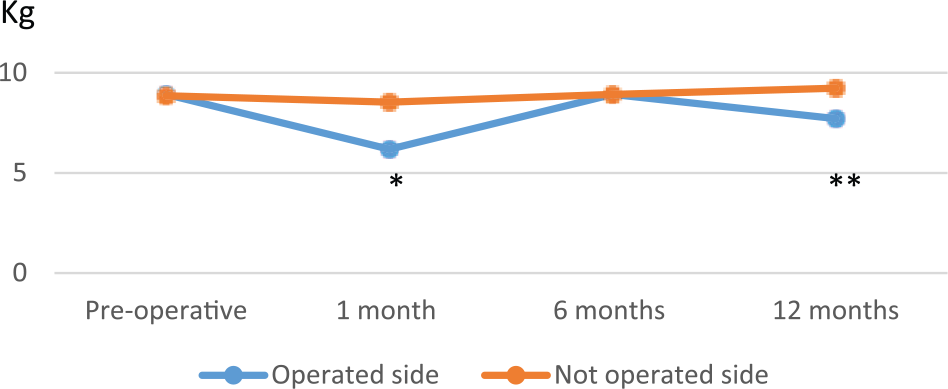
Muscle strength in shoulder extension, adduction, and lateral rotation of the operated side and the not operated side pre-operatively and 1, 6, and 12 months post-operatively.
Push-up from a chair
All women but one could perform the push-up from a chair successfully (mean 1.97 out of possible 2) pre-operatively but 1 month post-operatively the average score was 1.39 ± 0.53. Six months post-operatively, the mean rating was 1.86 and at 12 months 1.87, or four patients lacked few degrees to complete the test.
Lateral flexion of the torso
Average lateral flexion of the torso was significantly (p = 0.001) decreased bilaterally 1 month following E-LDF compared with pre-operative values and continued to be significantly decreased (p = 0.01) at 6 and 12 months post-operatively (Fig. 3).
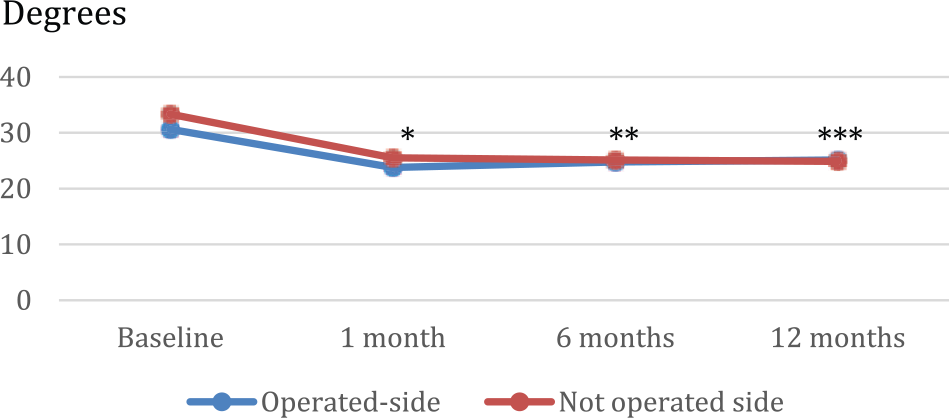
Lateral flexion of the torso to the operated side and not operated side pre-operatively and 1, 6, and 12 months post-operatively.
Position of scapula
The scapula on the operated side was significantly (p = 0.03) retracted 6 months post-operatively, but the difference between pre-operative values and 12 months post-operative values was not significant (p = 0.08). The distance between the inferior angle of the scapula and the highest point of the iliac crest did not change.
Pain, numbness, and adhesions
Nine women were pain free 4 weeks post-operatively, but six (40%) had pain rated between 3 and 8 on a numeric scale from 0 to 10. Three patients (20%) had pain at the donor site 6 months post-operatively rated 4–5.5 on a numeric scale from 0 to 10, but at 12 months all patients were pain free except one who complained of pain in the lower back rated 5.5. All but one (93%) had numbness around the donor-site scar, six (40%) had slight adhesions at 6 months, and five (33%) at 12 months. A total of 12 patients had adhesions 1 month post-operatively, 2 had no adhesions, and one could not be tested because of hyperesthesia. At 6 months, seven patients had adhesions and five at 12 months.
Discussion
In this study, we show that although full range of motion of the shoulder joint is invariably achieved in patients having E-LDF breast reconstructions, these operations cause a significant decrease in bilateral lateral flexion of the torso and significant retraction of the scapula on the operated side, which to the best of our knowledge has not been previously reported. Also, muscle strength in shoulder extension, adduction, and internal rotation is significantly decreased on the operated side compared with the not operated side.
We postulate that back pain and adhesions of the back scar to the chest wall may be the predominant factors causing the decrease in the lateral flexion of the torso observed. Average lateral flexion of the torso was significantly decreased bilaterally 1 month following E-LDF compared with pre-operative values when 40% of our patients had pain at the donor side and 80% adhesions. Lateral flexion of the torso showed some recovery but continued to be significantly decreased bilaterally at 6 and 12 months post-operatively when 47% and 33% of our patients, respectively, had adhesions. Therefore, we believe that measures to identify and decrease adhesion formation should be assessed and considered important for functional recovery of the spine. In this study, 33% of our subjects had adhesions 12 months post-operatively, while only 5% in a study by de Oliveira et al. (11), the only other study we could find that reported adhesions at this point in time. This large difference is difficult to explain. It may be that adhesion was assessed only of the scar in the study by Oliveira et al, while we assessed the area above and below the scar as well. Another explanation could be that all their patients received physiotherapy during the first post-operative month (content and number of sessions not reported) and thus tissue mobilization was probably started earlier than in this study, where treatment of adhesions started 1 month post-operatively although the average number of sessions was 15 (range, 1–53). Finally, differences in surgical procedure in closure of the donor site could be an explaining factor, but all our patients had quilting sutures in the back, in order to minimize the risk of seroma formation.
The influence of loss of tissue volume and latissimus function on the spine among LDF patients has not previously been studied, although Kim and Glazer (25) reported a case study of progressive back pain and thoracolumbar scoliosis in a young woman 4 years after breast reconstruction with LDF. This is interesting as balanced latissimus muscle function is considered important for appropriate spine alignment and stability through the tension it generates to the thoracolumbar fascia (25, 26). Furthermore, several anatomical and biomechanical studies indicate that the LD muscle plays an important role in both active motion and stabilization of the torso and spine (20, 27, 28).
According to Vleeming et al. (26), hip, pelvic, and leg muscles interact with so-called arm and spinal muscles via the thoracolumbar fascia and allows for effective load transfer between spine, pelvis, legs, and arms in an integrated system which results in stabilizing the lower lumbar spine and sacroiliac joints (26). Loss of a flap of LD muscle could therefore result in imbalance in this system which could result in low back and pelvic pain (22, 23). Among our patients, decreased arm muscle strength is likely to add to this problem.
Twelve months following E-LDF breast reconstruction, muscle strength in extension, adduction, and internal rotation were significantly less at the operated side than at the not operated side. The reason why we chose to compare sides rather than pre- and post-operative values in this case was that the patients might have been training arm muscles during this period and we did not control for that factor. We, however, assumed that they had trained both upper extremities equally. Comparison between this study and three studies found on muscle strength following LDF breast reconstruction is difficult due to different measurement methods and line of action measured. In the first 2 studies, muscle strength was measured using spring balance; the first measured shoulder adduction and extension separately in standing position at 6 weeks, 6 and 12 months follow-up and found 0.06 kg loss in extension and 0.3 kg in adduction at 12 months. The second had 6 months follow-up, measured in supine and side lying and found significant muscle weakness in adduction and internal rotation (12, 13). The third study measured muscle strength manually and found no definite decrease at 12 months, but related it to low sensitivity of manual muscle testing (12–14).
In our study, shoulder joint range of motion had reached 95% of pre-operative values 6 months post-operatively and 100% at 12 months, which is in line with previous studies (11, 13, 14). However, studies on shoulder range of motion including this study have measured total scapula-humeral motion, and it is unclear whether a compensatory increase in scapular (11, 13) and spinal (13) motion has occurred. Reports declaring that “the latissimus muscle is totally expendable” and LDF has “no detrimental effects on shoulder motion” together with the “results to demonstrate no significant loss of ROM, strength, function and pain” (9, 12, 13) can lead to the presumption that use of LDF for reconstruction is without any functional sequelae. However, a study using the Disability of Arm, Shoulder and Hand (DASH) questionnaire showed that 33% of patients had mild to moderate global impairment (19), and in a recent study, Yang et al. (14) found that DASH scores had not reached pre-operative values at 12 months post-operatively. They also used the 36-item Short-Form Health Survey questionnaire and found that the physical component summary was lower than pre-operative values at 12 months post-operatively (14). Although the former study had a 3-year follow-up, in general, the literature lacks more long-term assessments of shoulder function following LDF reconstructions. In a study by Giordano et al. (29), shoulder function was significantly impaired when assessed at a median follow-up of 7.6 years following LD-free flap for lower limb or head and neck soft-tissue reconstruction. This was, however, a retrospective study on only eight patients.
Further long-term prospective studies on the effects of E-LDF on shoulder function and strength are needed in order to properly counsel patients so that they can take well-informed decisions on having these types of breast reconstructions.
In summary, this study shows that although patients having E-LDF breast reconstructions may expect to achieve a full range of movement of the shoulder joint at 12 months from their surgery, some significant measurable changes do occur and persist in the mobility of the spine and muscle strength. Further studies are needed to find out if these changes cause clinically relevant problems with time, such as low back pain and scoliosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.