
Abstract
Background and Aims:
The objective of this study is to analyze outcomes of the first experiences with drug-eluting balloons in native arteries, vein grafts, and vascular accesses. The study is also a pilot for our future prospective, randomized, and controlled studies regarding the use of drug-eluting balloons in the treatment of the stenosis in bypass vein graft and dialysis access.
Materials and Methods:
A total of 93 consecutive patients were retrospectively analyzed and in the end 81 were included in the study. Inclusion criteria included at least one previous percutaneous angioplasty to the same lesion. Patients were divided into three groups according to the anatomical site of the lesion: native lower limb artery, vein bypass graft, or vascular access. Time from the previous percutaneous angioplasty to the drug-eluting balloon was compared to the time from the drug-eluting balloon to endpoint in the same patient. Endpoints included any new revascularization of the target lesion, major amputation, or new vascular access.
Results:
The median time from the drug-eluting balloon to endpoint was significantly longer than the median time from the preceding percutaneous angioplasty to drug-eluting balloon in all three groups. This difference was clearest in native arteries and vein grafts, whereas the difference was smaller from the beginning and disappeared over time in the vascular access group. No significant differences were seen between the groups with regard to smoking, antiplatelet regime, diabetes, Rutherford classification, or sex.
Conclusion:
Although the setup of this study has several limitations, the results suggest that there could be benefit from drug-eluting balloons in peripheral lesions. Very little data have been published on the use of drug-eluting balloons in vein grafts and vascular accesses, and randomized and controlled prospective studies are needed to further investigate this field.
Keywords
Introduction
During the past decade, there has been a clear trend toward endovascular revascularization in the treatment of peripheral arterial occlusive disease (1, 2). Conventional transluminal balloon angioplasty (percutaneous angioplasty (PTA)) causes intimal trauma, which leads to migration and proliferation of smooth muscle cells, and eventually in many cases significant intimal hyperplasia, restenosis, and occlusion of the treated segment (3). This, in turn, leads to a fairly high rate of target lesion revascularizations (TLRs) and prolonged healing (4). Deployment of stents is also associated with intimal hyperplasia and stenosis of the adjacent native artery as well as in-stent restenosis (5, 6).
To combat these adverse effects, devices for local delivery of cytotoxic drugs have been developed and adopted in clinical use. Sirolimus and paclitaxel eluting stents were first described in coronary disease and are now in routine use in coronary artery restenosis (7–10). Drug-eluting stents (DESs) have also been applied with promising results in peripheral, even in below-the-knee (BTK) lesions (11–13). Recent developments in the treatment of restenosis and occlusions include drug-eluting balloons (DEBs), where the suppressant agent is locally delivered to the site of angioplasty without leaving foreign bodies (i.e. stents) in the artery. Early results on the use of DEBs have shown promising results in femoropopliteal and BTK arterial occlusions (14–17). Results on the use of DEBs in bypass vein grafts remain unclear but promising (18, 19). The use of DESs or DEBs in the failing vascular accesses seems beneficial in a small randomized trial (20).
The objective for this study was to retrospectively review the results of the first PTAs with DEBs in our institution and to analyze whether any benefit was gained with an almost 10 times more expensive device. A secondary objective was to use this review as a pilot study for future randomized prospective and controlled studies especially regarding the use of DEBs in the bypass vein grafts and vascular accesses.
Materials and Methods
Helsinki University Hospital takes care of the treatment of chronic lower limb ischemia and access surgery for a population of 1.5 million. Approximately 1200 endovascular procedures due to chronic limb ischemia and access surgery are performed annually in our hospital. The results of the endovascular treatment of limb ischemia have been published in several publications (21, 22).
All patients who received PTA with DEB at our institution between January 2012 and December 2013 were reviewed retrospectively (n = 93). Indications for DEB were restenosis or occlusion of a previously conventionally dilated lesion in native arteries, lower limb vein grafts, and vascular access sites in all cases. Collected data included patient’s age, sex, Rutherford classification, smoking, diabetes, coagulopathy, anticoagulant regime, number, and dates of previous conventional PTAs (PTAcon) to the same lesion, time from previous PTA to DEB, as well as primary and secondary patencies after the DEB treatment. Endpoints for primary patency were any revascularization of the treated segment (open or endovascular) and major amputation and those for secondary patency an occlusion of the treated segment without revascularization. For follow-up, death was included in the endpoints. Follow-up was performed retrospectively from the case records. If no endpoint was reached at the date of review (end of February 2014) according to hospital or population registries (for death), the lesion was presumed to be open and asymptomatic. Causes of exclusion included primary use of DEB (n = 3), use of DEB in a prosthetic bypass graft (n = 1), use of DEB in stenosis of complex brachiojugular vascular access (n = 1), and insufficient or unavailable patient data (n = 7). A total of 81 patients were eventually included in the study. Table 1 shows basic patient demographics.
Basic patient demographics indications for the procedure.
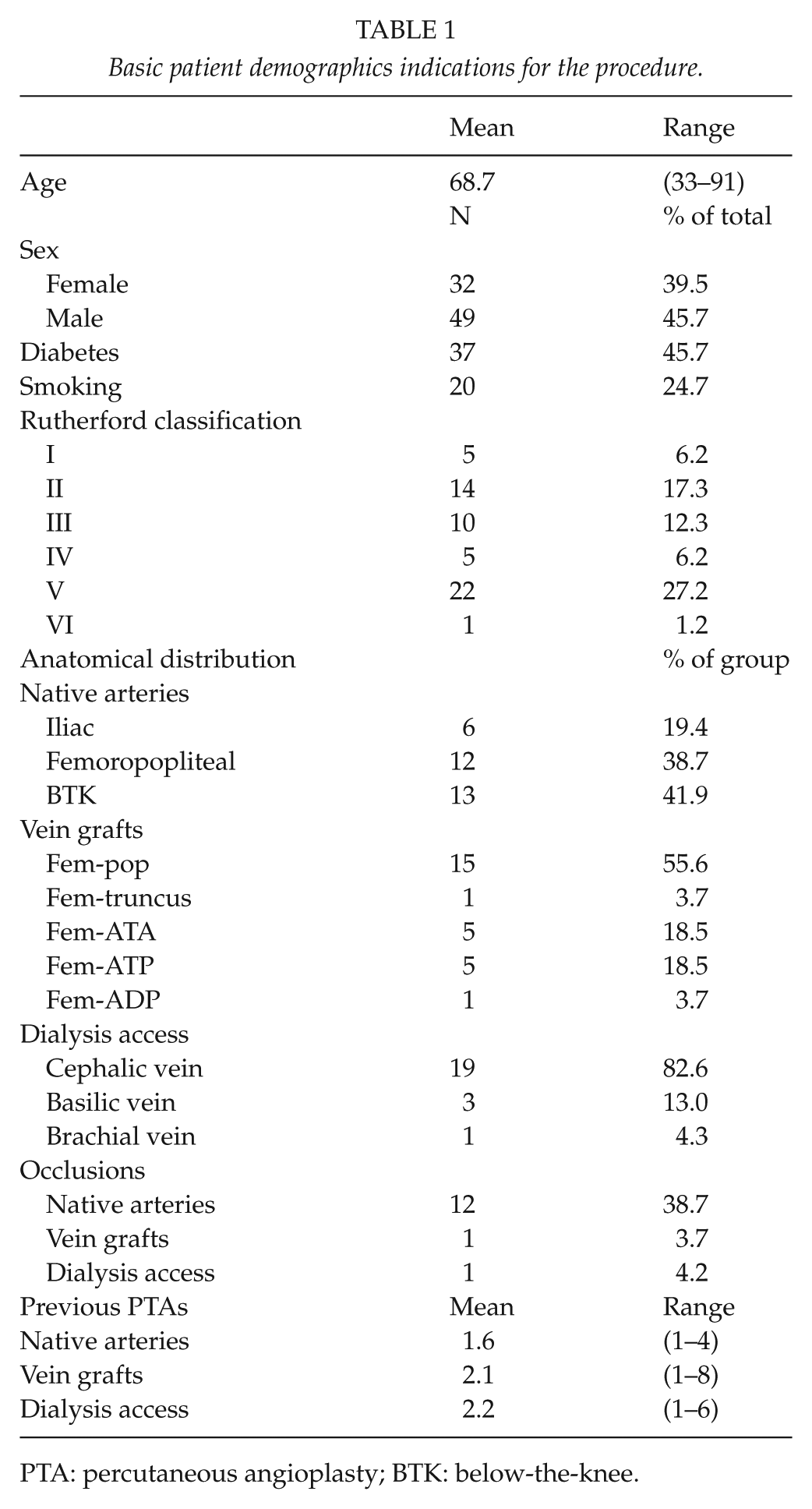
PTA: percutaneous angioplasty; BTK: below-the-knee.
PTA (DEB) was performed with In.Pact Admiral, Pacific and Amphirion paclitaxel-eluting balloons (Medtronic (Ex Invatec), Minneapolis, MN, USA). The Amphirion balloons were withdrawn from use in BTK lesions during the studied period of time. All the lesions were predilated with a conventional balloon prior to drug-eluting PTA.
The protocol for follow-up varied depending on the indication for the procedure and was performed according to the standard protocol at our institution: lower limb native artery lesions causing claudication without critical limb ischemia (CLI) were not routinely followed up, whereas CLI prompted follow-up at 1–2 months and the surveillance lasts until the ischemic wound is healed. Vein grafts were followed up with duplex ultrasound (DUS) by a vascular nurse, which also led to the treatment of asymptomatic graft stenoses found by DUS. Vascular access patients were not under routine surveillance in the department of vascular surgery. However, all patients continued dialysis therapy and were referred back to the vascular clinic by nephrologists as needed, usually due to problems in dialysis through the treated access.
Statistical analysis was performed using Microsoft Excel (Microsoft, Redmond, WA, USA) and SPSS version 22 (IBM, Armonk, NY, USA). Survival correlations were calculated using log-rank testing.
All patients had undergone at least one previous PTAcon to the same lesion before DEB. The time (in days) from the latest PTAcon to the PTA with DEB was determined for each patient. Thereafter the time from DEB to any primary endpoint (any revascularization of the treated segment (open or endovascular), major amputation or death) was determined from case records. Median time from the last PTAcon and the median time from DEB to the primary endpoint were then compared. This means that the cohort effectively functioned as its control group, with DEB being the endpoint in the PTA group. The study setup is illustrated in Fig. 1.
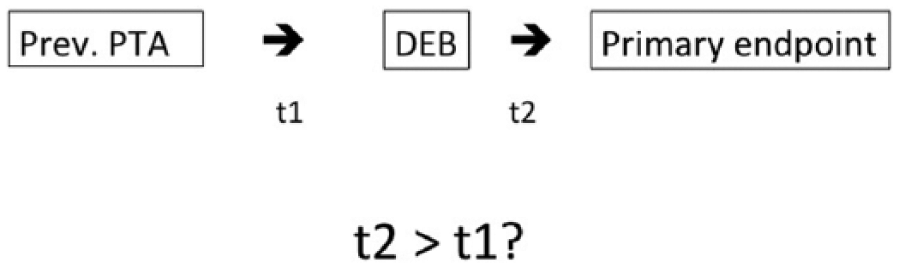
Study setup.
All treated bypass vein grafts were under continuous DUS surveillance in our outpatient clinic and all vascular accesses were in active use several times a week. Only native artery lesions were not routinely followed up.
Results
A total of 81 cases were eventually included in the analysis. The statistical comparison was made in for the whole group as well as in three separate groups based on the anatomical site of the treated lesion: native arteries (n = 31), bypass vein grafts (n = 27), and vascular accesses (n = 23). The patients in the native artery group were on average 7 years older than patients in the other groups. Males were clearly overrepresented in the vascular access group, as is, unsurprisingly, kidney disease and diabetes. There was no statistical significance for sex and age, smoking, or medication between the subgroups. The groups were not compatible with regard to total occlusions, as these were clearly overrepresented in the native artery group. There was no change in the standard medication protocol during this period: the routine was dual antiplatelet therapy ((DAPT), ASA + clopidogrel) 1–3 months after the treatment or if patients were on warfarin, acetylsalisylic acid (ASA) was added for 1–3 months. At the DEB procedure, 23 patients were already on double antiplatelet therapy, 44 patients were on ASA alone and all of these received DAPT postoperatively, nine patients were on ASA and warfarin and eight on warfarin only. Comprehensive medication data at the previous procedure could not be gathered for all patients.
In the overall series, the median time from the PTAcon to DEB was 240 days when compared to 572 days from the DEB to an endpoint (p < 0.01). The time from the DEB to endpoint was significantly longer in all three groups compared to the time from previous PTA to DEB (Table 2). Figs 1 to 4 show the Kaplan–Meier plots for the different groups. There is a marked difference in endpoint-free survival in both lower limb groups, whereas the difference vanishes over time in treated vascular accesses. The 1-year freedom-from-primary-endpoint with PTAcon versus DEB in the entire cohort was 19.5% versus 53.7%, respectively. The corresponding figures at 2 years were 4.9% and 12.2%. No correlation was seen between restenosis and antithrombotic regime, smoking, diabetes, or Rutherford classification in this group.
The mean and median time between the first PTA and DEB (PTAcon) and between DEB and endpoint (DEB).
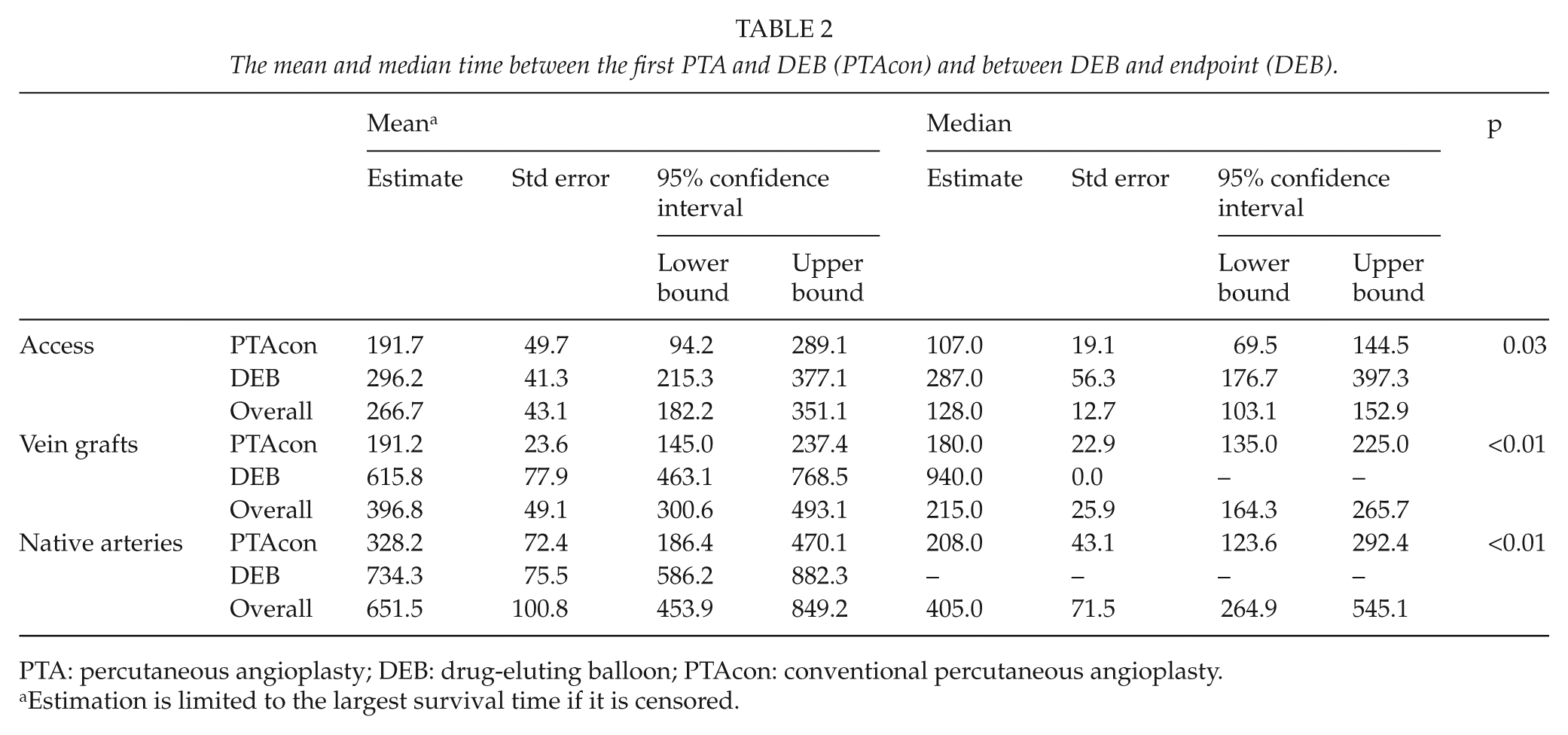
PTA: percutaneous angioplasty; DEB: drug-eluting balloon; PTAcon: conventional percutaneous angioplasty.
Estimation is limited to the largest survival time if it is censored.
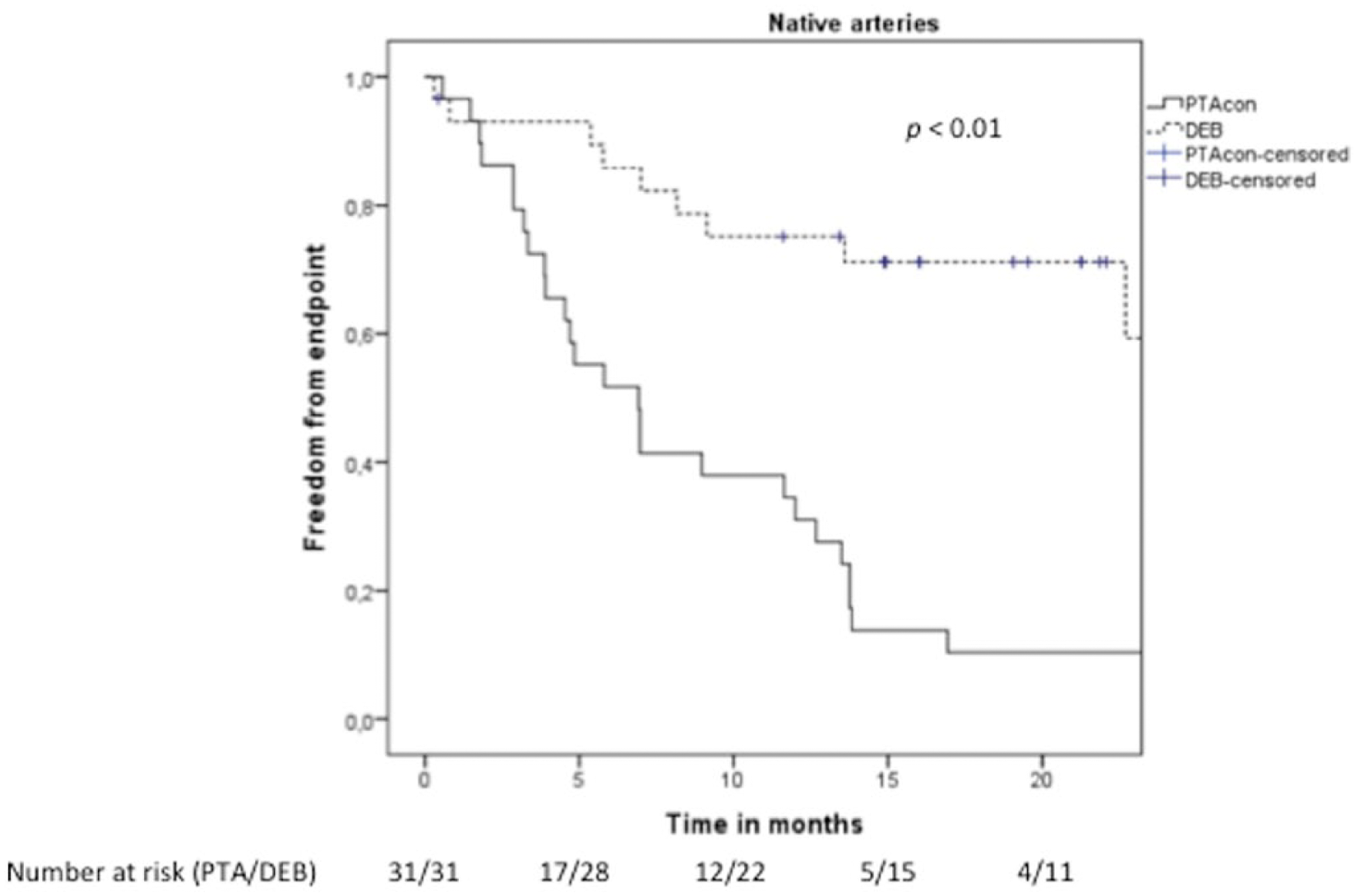
Kaplan–Meier graph for native arteries.
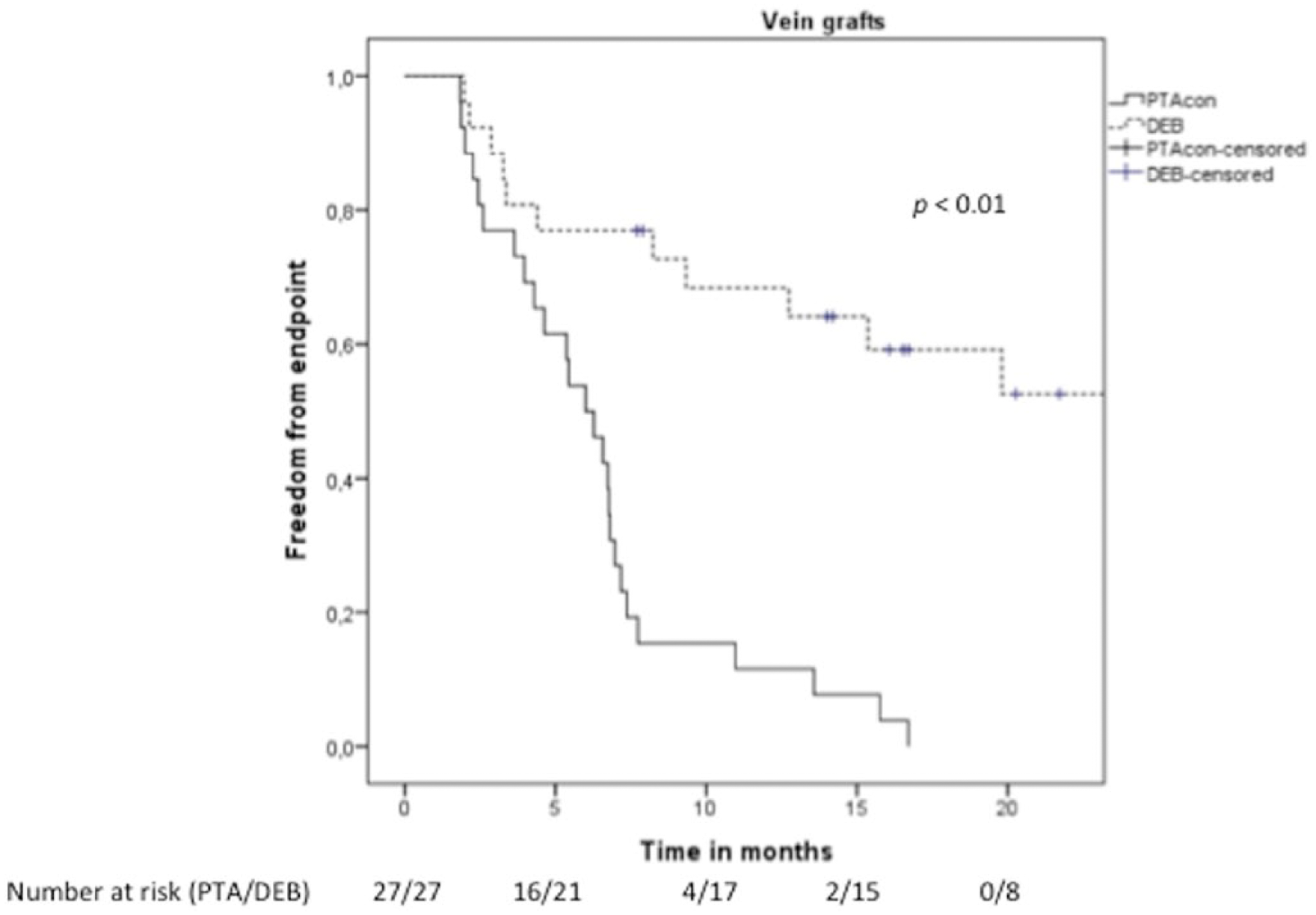
Kaplan–Meier graph for bypass vein grafts.
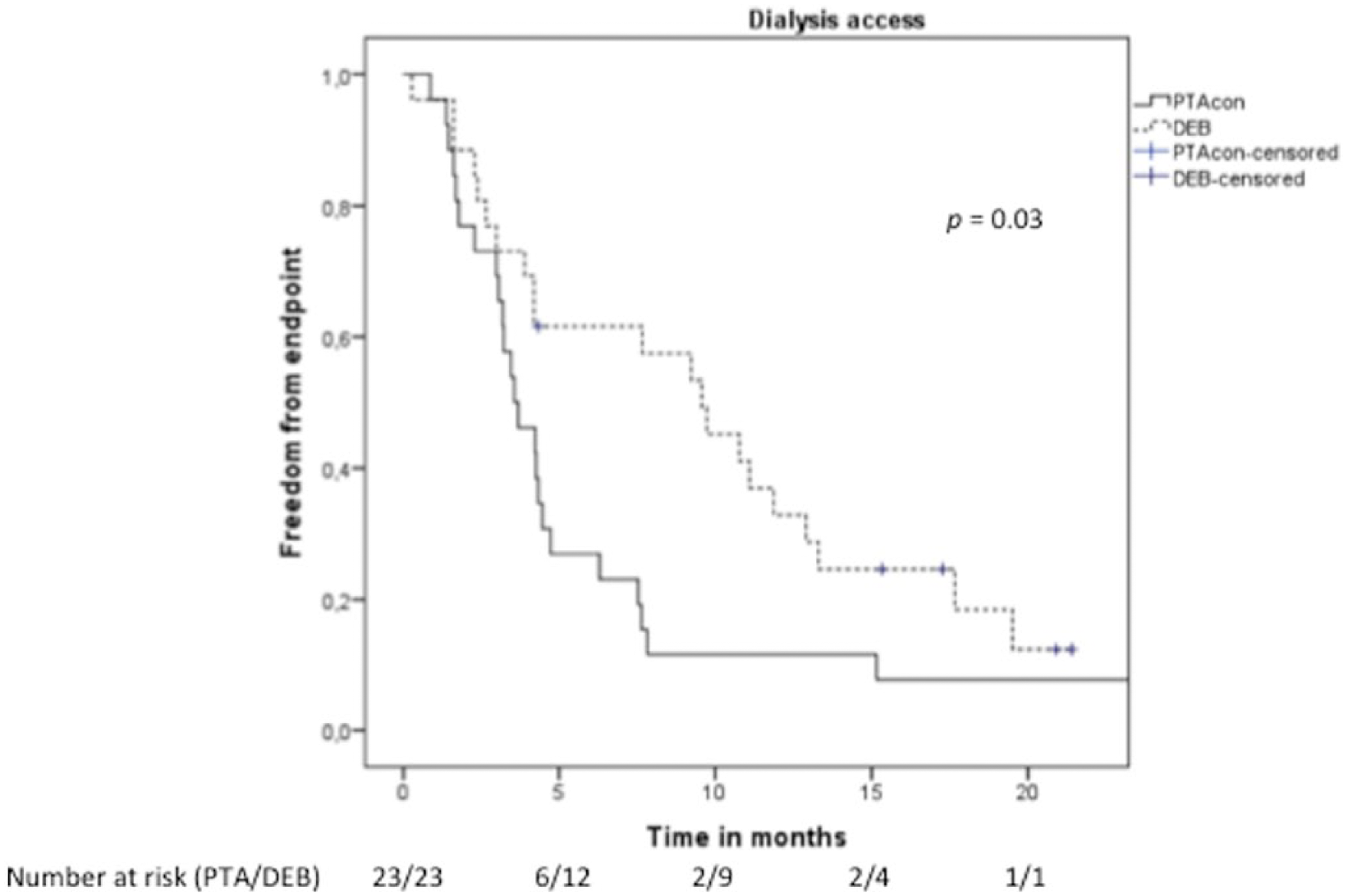
Kaplan–Meier graph for dialysis accesses.
Discussion
The estimated rate of clinically significant coronary artery restenosis after PTAcon is approximately 10% and in angiography restenosis can be seen in 30%–50% (3). One of the latest innovations to prevent restenosis after PTA is the DEB, where paclitaxel is delivered to the site of PTA with a balloon coated with the drug. The use of DEBs in peripheral arteries is a field with more intensive research, although findings remain inconclusive. The DEBATE series even reported striking benefit from use of DEBs in various femoropopliteal lesions, whereas 12-month results from the IN.PACT DEEP trial only show similar efficacy with even a trend toward higher amputation rates in the DEB-group (23). The latter study examined PTAs to BTK. In our study, the target was BTK in only 13 cases. Sponsoring from companies manufacturing DEBs biases some of these studies. In the treatment of coronary artery disease, DEB is routinely indicated in the treatment of in-stent restenosis. However, no guidelines exist on the treatment of peripheral arterial disease (PAD) with DEB. In one prospective trial, the use of DEBs increased patency in failing dialysis accesses. In one study, DEBs were proven a safe and efficient choice for treatment of venous and prosthetic bypass grafts (18). So far, much less data are available on DEB use in grafts and accesses than in native lower limb arteries and our study implies that there could benefit from drug elusion even in these target vessels. Our study is independent and objective, attempting to establish preliminary results on whether there is any benefit from DEBs in peripheral arteries, bypass vein grafts, and dialysis access. We saw a beneficial effect in DEB compared to conventional balloons. The difference between conventional balloons and DEBs seemed to be most significant in native arteries and bypass vein grafts and interestingly the benefit was limited in dialysis access.
Our study has several limitations. Primarily, the number of patients is low, especially in the subgroups. Secondly, we do not have a true control group, as we created two groups with each patient being in both groups simultaneously. This may cause severe bias to the results and has to be borne in mind when doing interpretations. The subgroups are not comparable with regard to occlusions and follow-up. It is also true that, at the time of DEB, the patients were older than in the first round, they all had had a higher number of PTAs to their arteries and they had had a longer period of ischemia than when they underwent PTAcon. As these were the very first PTAs with DEB we can assume some learning curve in the DEB group but surely not in PTAcon group as PTAcon have been done 20 years in our institution. Amputation and death were also included to the endpoints after DEB, which could be reflected in the outcome. In many cases, DEBs were used as a last resort when lesion had been treated with multiple PTAs before with no long-term success. Furthermore, as many of the patients were already on DAPT at the time of DEB, and with no data on medication at the previous procedure, it is possible that pre-procedural DAPT is overrepresented in the DEB group. However, as the DAPT was started at the time of procedure with a 300 mg loading dose of clopidogrel, the influence of the difference in preoperative DAPT did probably not impact the results (Table 3).
Endpoints by group.
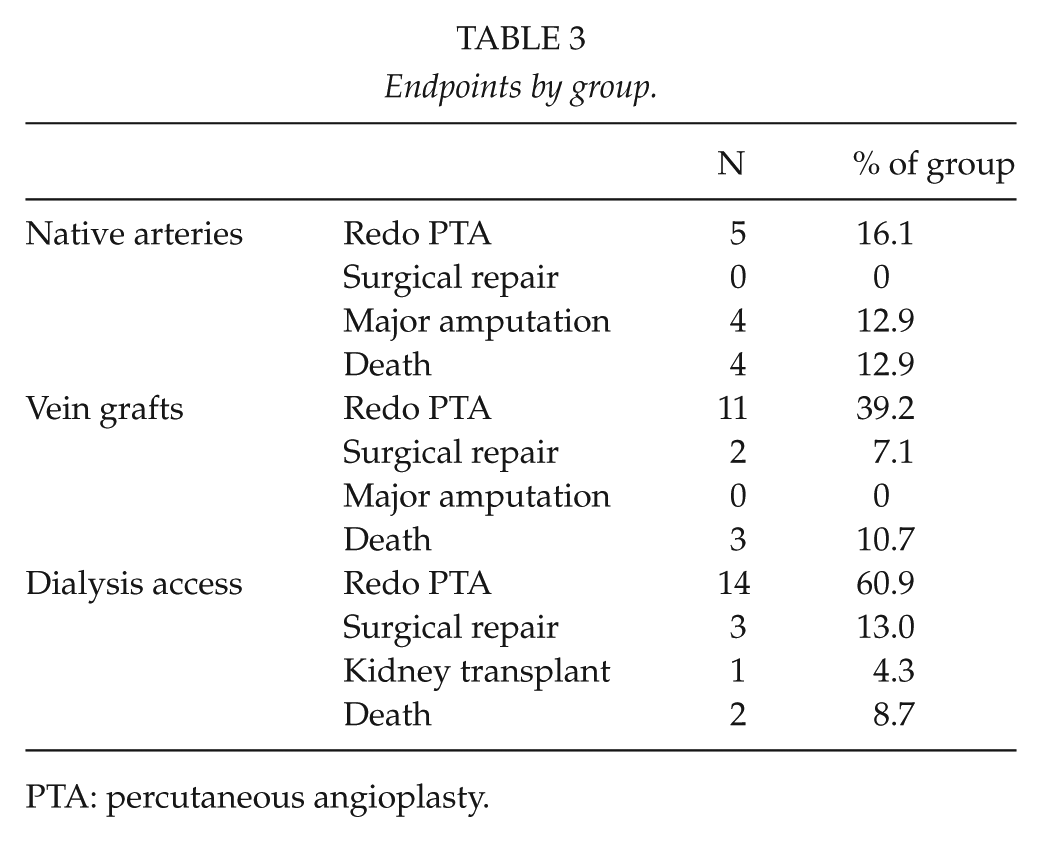
PTA: percutaneous angioplasty.
The study is comprehensive with regard to the population, as these patients are not treated in other clinics in the area. Follow-up is comprehensive in the bypass group with regular screening with DUS, and in the access group by continuous dialysis through the access. The follow-up was poorest among claudicants who are not under routine surveillance at all. However, all patients that undergo endovascular treatment due to claudication are advised to contact the department of vascular surgery if they get recurrent claudication. As our hospital is the only institution in the region that provides treatment of vascular pathologies, we are relatively confident with the basic assumption on the outcome, although all criticism toward it is understandable. The three analyzed subgroups are not directly comparable with each other as the physiology and biology of the stenosis is different and there are differences in follow-up. However, it is interesting that the difference between DEB and PTAcon was limited in the access sites. Perhaps the fact that the access vein is under continuous stress due to repeated punctures during dialysis decreases the positive impact of DEB. It is also interesting to note that DEB treatment has a positive outcome in the native artery group, even if these patients have an overrepresented rate of total occlusions and are not followed up as meticulously as the two other groups. This finding underlines the notion that the nature of the disease is quite different between the groups. A specific problem with the analysis of native artery disease is that all Rutherford classes (i.e. claudication and CLI) are often pooled together, whereas the clinical urgency, prognosis, and follow-up demands are quite different.
Our results imply clinical significance for drug elusion. At the moment there are no generally accepted indications for the use of DEB in PAD or vascular access salvage. In our hospital we have accepted the use of DEB in cases of recurring and persistent restenosis. DEBs are considerably more expensive than conventional balloons, and based on this limited study, routine use of DEBs beyond the current indications cannot yet be justified. In addition, there are still many unanswered questions in the use of DEBs, mainly considering anatomical and clinical indications for use. However, these results motivate and call for further research, especially regarding DEBs in vein grafts and vascular accesses. Furthermore, as these results are promising, we feel that the randomized trial is justified.
Conclusions
A significant difference was seen in freedom-from-endpoint in both lower limb groups. The difference vanished over time in the vascular access group, although overall survival in this group is still markedly better at 1 year after treatment. These findings suggest that drug elusion could be effective in the treatment of peripheral restenosis. Many factors play a role in the recurrence of vascular stenosis, and in this study there is risk of selection bias as indications for were not firm. The authors acknowledge that this study is limited by its small sample size, its unconventional design, and retrospective nature. The results are still intriguing, and larger, randomized, and controlled prospective studies are needed for validation and clinical implementation of DEBs especially in vein grafts and vascular accesses. Serving this purpose, we have designed a randomized study for grafts and accesses with thorough and standardized surveillance and follow-up.
Footnotes
Acknowledgements
The abstract has been presented at the Charing Cross Symposium in London, 28–30 April 2015.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was partially funded by the Finnish Society for Angiology.