
Abstract
Objectives:
Gallstone disease shares certain risk factors with cardiovascular disease, particularly metabolic risk factors. Patients with gallstone disease may be at increased risk of cardiovascular disease. Several recent studies exploring the effect of gallstone disease on cardiovascular disease outcomes demonstrated inconsistent results.
Design:
We conducted a systematic review and meta-analysis of cohort, case–control, and cross-sectional studies that compared the risk of developing cardiovascular disease events in patients with gallstone disease versus non-gallstone disease controls. Data from each study were combined using the random-effects, generic inverse variance method of DerSimonian and Laird to calculate the pooled hazard ratio, odd ratio, and 95% confidence interval.
Results:
Data were extracted from six studies involving 176,734 cases and 803,714 controls. The pooled hazard ratio of cardiovascular events in patients with gallstone disease was 1.28 (95% confidence interval: 1.23–1.33, I2 = 42%). The pooled odd ratio of cardiovascular events in patients with gallstone disease was 1.82 (95% confidence interval: 1.47–2.24, I2 = 68%).
Conclusions:
Our study demonstrated a statistically significant increase in the risk of cardiovascular disease among patients with gallstone disease.
Introduction
Gallstone disease (GD) is a common condition worldwide. The prevalence of GD varies greatly by the ethnicity and geographic location ranging from 4%–73%, especially in the Western countries (1). A majority of patients (up to 80%) will remain asymptomatic throughout their lifetimes (2). Although the mortality rate of GD is relatively low, this disease is one of the highest health care cost burdens of digestive diseases (3) and also the leading cause of hospitalization in the United States (4).
Cholesterol gallstone formation is the multifactorial process involving a multitude of metabolic pathways. The hypersecretion of free cholesterol into bile is the primary pathogenic factor. Accelerated cholesterol crystallization, hypersecretion and accumulation of mucin, high efficiency of intestinal cholesterol absorption, and impaired gallbladder and intestinal motility are the secondary events involving in the pathogenesis of cholelithiasis (5, 6). The etiology is multifactorial with interaction of genetic and environmental factors. Intake of high energy, saturated fat, and simple sugar also favors gallstone formation (7).
GD shares certain risk factors with cardiovascular disease (CVD), particularly age, obesity, diabetes mellitus, hypertension, hyperlipidemia, insulin resistance, sedentary lifestyle, non-alcoholic fatty liver disease, and metabolic syndrome (8–10). Additionally, cholesterol is the main component of GD that is also the main pathogenic factor for artherosclerotic plaque formation that will further progress to several CVDs including stroke and coronary heart disease (11). In light of sharing risk factors, patients with GD may be at increased risk of CVD.
Several recent studies exploring the effect of GD on CVD outcomes demonstrated contradictory results. Thus, to further investigate this possible risk, we conducted a systematic review and meta-analysis of observational studies that compared the risk of CVD in patients who had GD versus patients who did not have GD.
Methods
This systematic review and meta-analysis was conducted and reported according to the Meta-analysis Of Observational Studies in Epidemiology statement (12) and was registered in PROSPERO (International Prospective Register of Systematic Reviews) (registration number: CRD42015030065).
Data Sources and Search Strategy
Two authors (Sikarin Upala (SU) and Veeravich Jaruvongvanich (VJ)) independently searched published studies indexed in PubMed/MEDLINE and EMBASE databases from the date of inception to November 2015. References of all selected studies were also examined. The following main search terms were used: Cardiovascular disease, stroke, coronary heart disease, myocardial infarction, gallstones, cholelithiasis. The full search strategy is detailed in Item S1 in supplementary material, available at http://sjs.sagepub.com. A manual search of references of selected retrieved articles was also performed.
Study Selection
Our inclusion criteria were (1) published observational studies including cross-sectional, cohort, and case–control studies assessing the risk of GD on CVD incidence, prevalence and/or mortality, (2) participants aged 18 years or older, (3) relative risks (RRs), odds ratios (ORs), hazard ratios (HRs) or standardized incidence ratios with 95% confidence intervals (CIs) were provided, (4) participants without GD or participants without CVD were used as a reference group. GD is defined as the presence of gallstones or history of cholecystectomy. We excluded review articles, case reports, abstracts, and unpublished studies. CVD is defined as coronary heart disease, heart failure, and stroke.
Two authors (SU and VJ) independently reviewed titles and abstracts of all citations that were identified. After all abstracts were reviewed, data comparisons between the two investigators were conducted to ensure completeness and reliability. The inclusion criteria were independently applied to all identified studies. Differing decisions were resolved by consensus between the two authors.
Data Extraction
Full-text versions of potentially relevant articles identified in the initial screening were retrieved. If multiple articles from the same study were found, only the article with the most complete data was included. Data concerning author, year of publication, study design, study location, participant characteristics, diagnosis of GD, definition of CVD, confounder adjustment, and quality assessment were independently extracted by two authors. We contacted the authors of the primary reports to request any unpublished data. If the authors did not reply, we used the available data for our analyses.
Assessment of Quality
A subjective assessment of methodological quality for observational studies was evaluated by two authors (SU and VJ) using the Newcastle–Ottawa Scale (NOS). The NOS is a quality assessment tool for non-randomized studies. It used a “star system” based on three major perspectives: the selection of the study groups (0–4 stars), the comparability of the groups by controlling for first and second most relevant factors (0–2 stars), and the ascertainment of outcome of interest (0–3 stars). A total score of three or less was considered poor, 4–6 was considered moderate, and 7–9 was deemed high quality (13). We excluded poor quality studies in the sensitivity analysis. Discrepant opinions between authors were resolved by consensus.
Statistical Analysis
We performed meta-analysis of the included studies using Comprehensive Meta-Analysis 3.3 software from Biostat, Inc. We calculated pooled effect estimates (OR, HR, or RR) of CVD with 95% CIs comparing between the groups of gallstones and non-gallstones individuals using the random-effects model. We used effect size (OR, HR, and RR) from the multivariate model with confounding factors adjusted in each study. We reported the pooled effect estimate of a change in outcome using a fixed effects model if I2 < 50% and a random effects model if I2 ≥ 50%. A fixed-effect meta-analysis is based on the assumption that each study provides the same effect. While a random-effects meta-analysis model involves an assumption that the effects being estimated in the different studies are not identical, but follow some distribution. The heterogeneity of effect size estimates across these studies was quantified using the Q statistic, its p value, and I2 (p < 0.10 was considered significant). A value of I2 of 0%–25% indicates insignificant heterogeneity, 26%–50% low heterogeneity, 51%–75% moderate heterogeneity, and 76%–100% high heterogeneity. Publication bias was assessed using the funnel plot, Egger’s regression test, and its implications with the trim and fill method. A funnel plot is a simple scatter plot of the intervention effect estimates from individual studies against some measure of each study’s size or precision. Egger’s regression test is a test for asymmetry of the funnel plot with a significance level at 0.10. The trim and fill method is a non-parametric data augmentation technique used to estimate the number of studies missing from a meta-analysis due to publication bias.
Results
Description of Included Studies
The initial search yielded 1933 articles; 1896 articles were excluded based on title and abstract review. A total of 37 articles underwent full-length review. A total of 31 articles were excluded (15 articles did not report outcomes of interest, 10 articles did not study in subjects of interest, 3 articles were letters, and 3 articles were abstract). Data were extracted from six studies involving 176,734 patients with GD and 803,714 controls without GD. Item S2 in the supplementary material outlines the search methodology and selection process. Table 1 describes the detailed characteristics and quality assessment of included studies.
Characteristics of included studies.
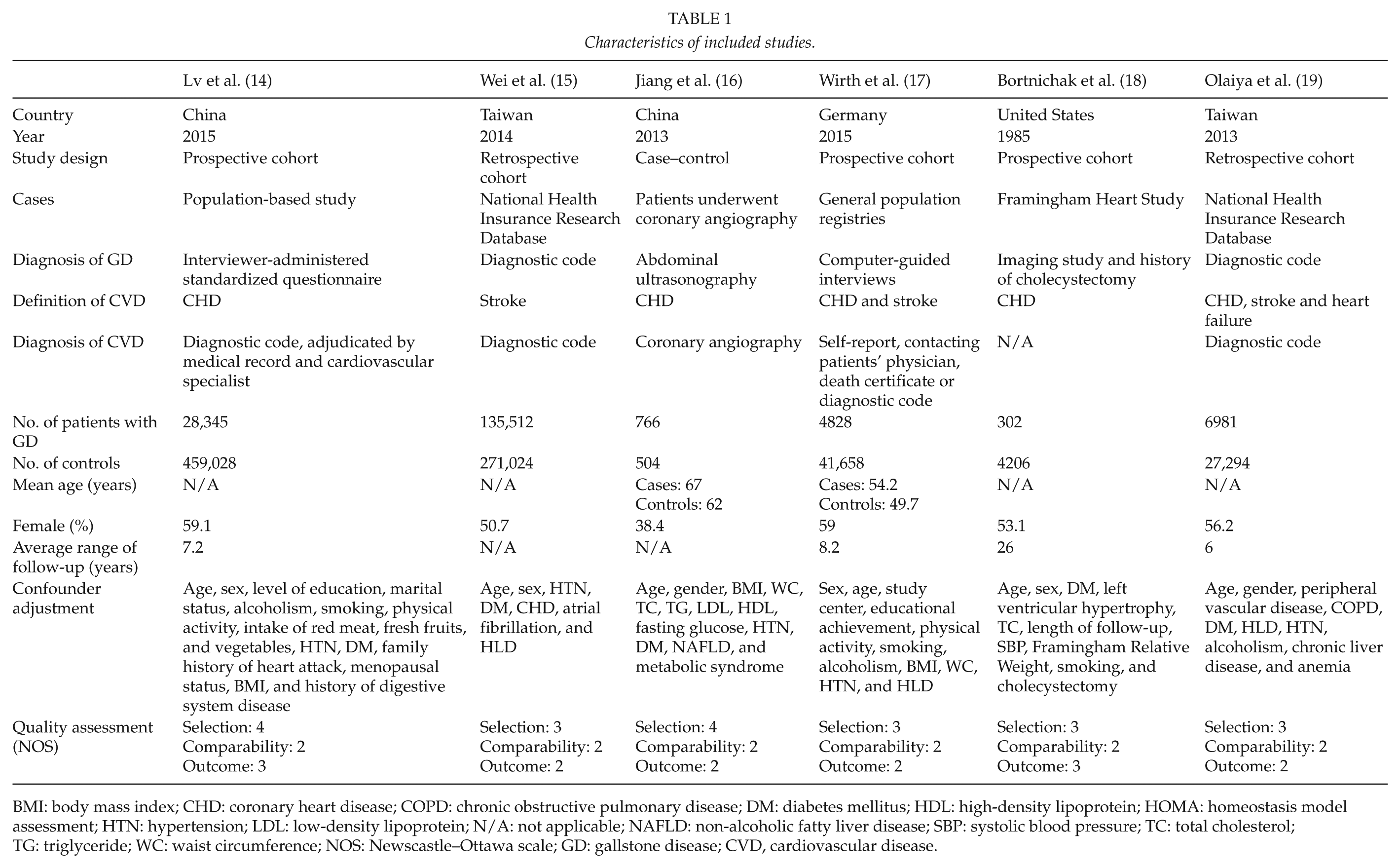
BMI: body mass index; CHD: coronary heart disease; COPD: chronic obstructive pulmonary disease; DM: diabetes mellitus; HDL: high-density lipoprotein; HOMA: homeostasis model assessment; HTN: hypertension; LDL: low-density lipoprotein; N/A: not applicable; NAFLD: non-alcoholic fatty liver disease; SBP: systolic blood pressure; TC: total cholesterol; TG: triglyceride; WC: waist circumference; NOS: Newscastle–Ottawa scale; GD: gallstone disease; CVD, cardiovascular disease.
Meta-Analysis Results
Six studies (five cohort studies (14, 15, 17–19) and one case–control study (16)) were included in the meta-analysis. We analyzed the pooled HR and pooled OR separately. The pooled HR of CVD events in patients who had GD was 1.28 (95% CI: 1.23–1.33, I2 = 42%) (four cohort studies (14, 15, 17, 19)) (Fig. 1). There was also statistically significant higher odds of cardiovascular events in patients with GD with pooled OR of 1.82 (95% CI: 1.47–2.24, I2
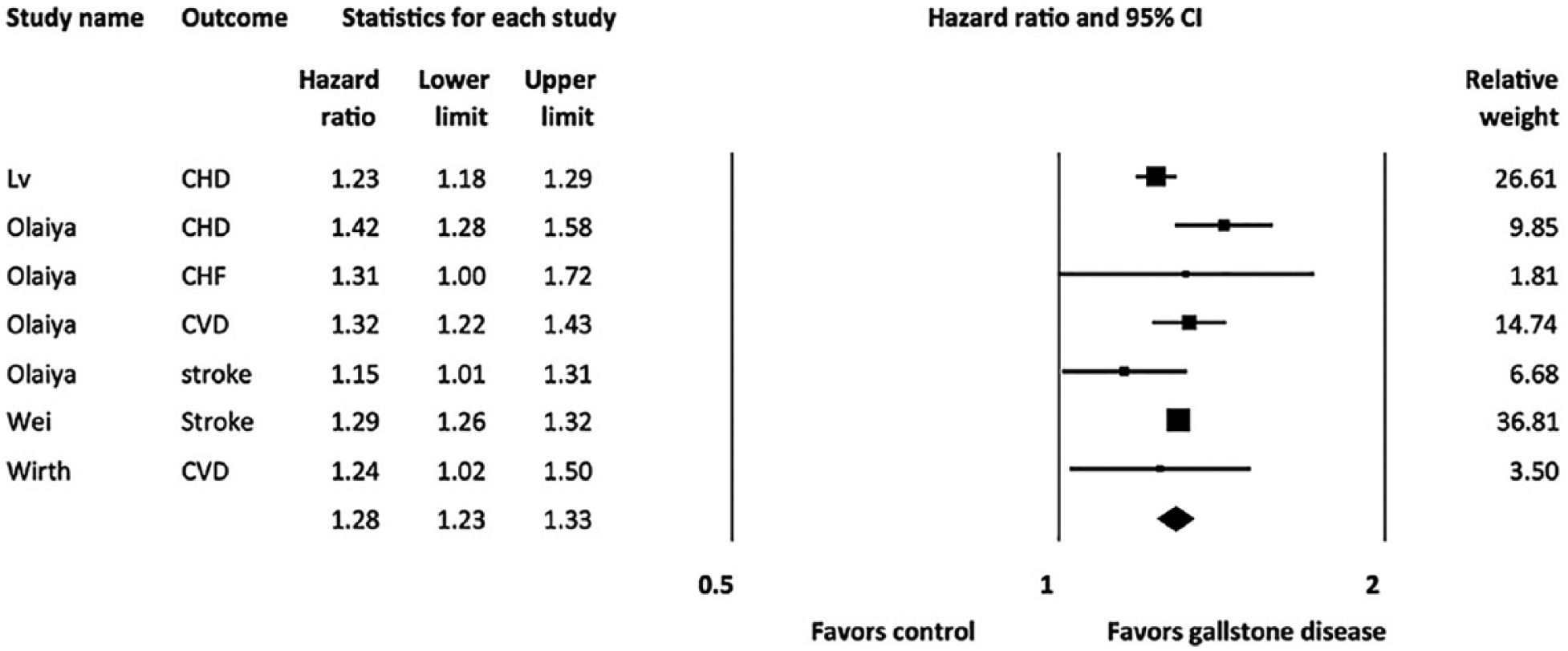
Forest plot of the included studies comparing risk of cardiovascular disease in patients with gallstone disease and those without gallstone disease; a diamond data marker represents the overall hazard ratios and 95% CI for the outcome of interest.
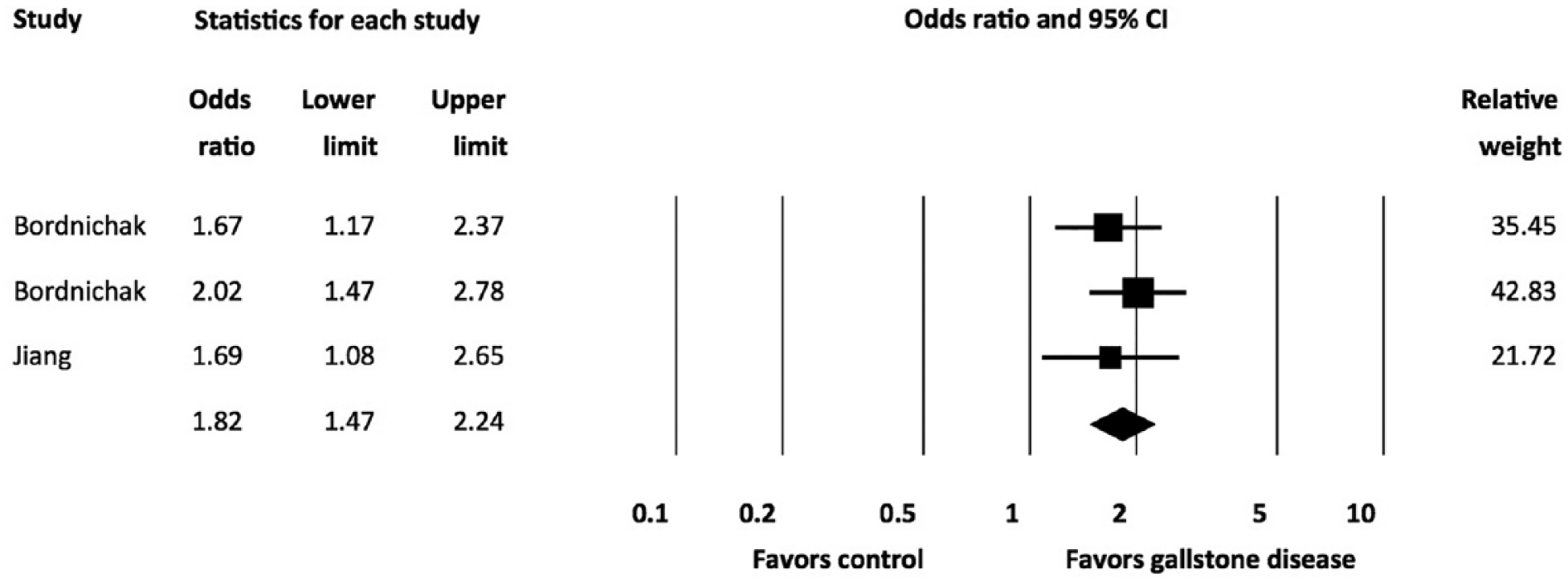
Forest plot of the included studies comparing risk of cardiovascular disease in patients with gallstone disease and controls; a diamond data marker represents the overall odds ratios and 95% CI for the outcome of interest.
Publication Bias
To investigate potential publication bias, we examined the contour-enhanced funnel plot of the included studies that assessed the ORs of CVD events (Fig. 3). The plot excludes bias since there is symmetrical distribution of studies on both sides of the mean. Furthermore, Egger’s test was non-significant (p = 0.91). Using the trim and fill methods in the random-effects model, there was no difference of the imputed OR of 1.28 (95% CI 1.23–1.33).
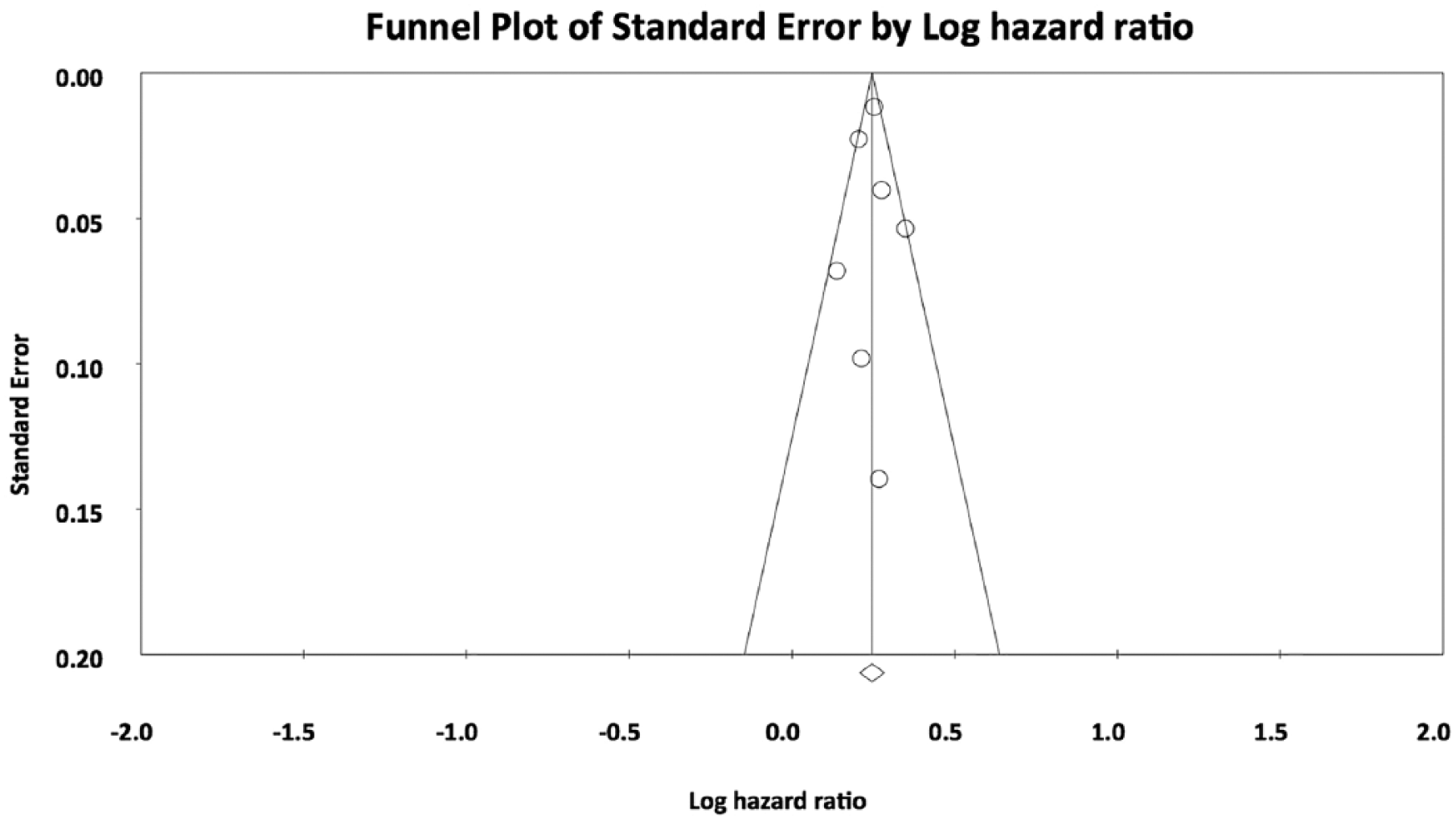
Funnel plots showing publication bias in the studies reporting number of participants with cardiovascular disease in patients with gallstone disease and controls. Circles represent observed published studies.
Discussion
In this systematic review and meta-analysis of approximately 200,000 cases and 800,000 controls, we demonstrate a significant increased risk of CVD events with an overall 1.28-fold increased risk and 1.82-fold increased odds among patients with GD compared with controls. We also demonstrated a 1.3-fold higher risk of coronary heart disease in patients with GD.
Several potential mechanisms may account for the association between GD and CVD risk. First, the presence of GD was found to be related to many CVD risk factors including age, obesity, diabetes mellitus, hypertension, hyperlipidemia, insulin resistance, sedentary lifestyle, and metabolic syndrome (8, 10, 20–22). However, in most of included studies, the risks were adjusted to the common risk factors (e.g. hypertension, hyperlipidemia, obesity, and diabetes mellitus) but the association of both conditions remained significant in our analysis suggesting that other pathogenic processes might play a role. Second, the abnormal regulation of hepatic cholesterol and bile acid is the primary pathological process of stone formation in the gall bladder (23). Gut microbiota are the large number of healthy microorganisms residing along the gastrointestinal tract, functioning to maintain the normal host physiology (24). They are able to regulate the composition of bile acid (25). The disruption of these organisms was found to be the potential key process of gallstone formation (26). Moreover, several studies showed that the altered gut microbiota was found to increase not only the CVD but also cardiovascular risk factors including insulin resistance, diabetes mellitus, and obesity (26, 27). The association of GD and CVD might be partly due this gut microbiota dysbiosis. Third, inflammation could be a central pathogenic process of this association; since there was an increased oxidative stress in the gallbladder mucosa resulting in altered bile saturation and further progress to gallstone (28). In the same manner, increased oxidative stress is the key factor of CVD development as a result of lipid peroxidation and endothelial dysfunction (29). Physicians should be aware of this potential association and appropriately provide the cardiovascular risk factor modifications to these patients. Moreover, it is still unknown whether any intervention could modify the risk including anti-platelet medications. A prospective study is warranted to address this issue.
Even though most of the included studies have good quality, several limitations in this study should be acknowledged. First, this is a meta-analysis of observational studies so we can at best demonstrate the association but not a causal relationship. A weakness inherent in observational studies is that they may be subjected to confounding; therefore we cannot draw a conclusion that GD itself or other confounders are the cause of the increased CVD risk. Second, statistical heterogeneity presents in this study. The possible sources of these heterogeneities include the differences in the study design, methodology, and population. However, there was no significant publication bias in our final analysis. Third, some of the included studies were conducted using medical registry–based databases and so there is the possibility of coding inaccuracy for both CVD and GD. Fourth, the subtypes of stones including cholesterol gallstone, black pigment gallstone, and brown pigment gallstone were not separately analyzed for the risk of CVD in included studies. Since the pathogenic pathway of the stone formation in each subtype is different, it might contribute to the difference in CVD risk (30).
Conclusion
Our meta-analysis demonstrates a significant elevated risk of CVD among patients with GD. GD could be the risk factor for developing atherosclerosis. Further studies are needed to identify the underlying mechanism and should assess this effect in patients with different subtypes of GD (cholesterol gallstones, pigmented gallstones, or mixed gallstones).
Footnotes
Acknowledgements
The authors thank Mathew Roslund for validation of the search.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.