
Abstract
Background and Aims:
Cardiopulmonary bypass induces a systematic inflammatory response, which is partly understood by investigation of peripheral blood cytokine levels alone; the lungs may interfere with the net cytokine concentration. We investigated whether lung ventilation influences lung passage of some cytokines after coronary artery bypass grafting.
Material and Methods:
In total, 47 patients undergoing coronary artery bypass grafting were enrolled, and 37 were randomized according to the ventilation technique: (1) No-ventilation group, with intubation tube detached from the ventilator; (2) low tidal volume group, with continuous low tidal volume ventilation; and (3) continuous 10 cm H2O positive airway pressure. Ten selected patients undergoing surgery without cardiopulmonary bypass served as a referral group. Representative pulmonary and radial artery blood samples were collected for the evaluation of calculated lung passage (pulmonary/radial artery) of the pro-inflammatory cytokines (interleukin 6 and interleukin 8) and the anti-inflammatory interleukin 10 immediately after induction of anesthesia (T1), 1 h after restoring ventilation/return of flow in all grafts (T2), and 20 h after restoring ventilation/return of flow in all grafts (T3).
Results:
Pulmonary/radial artery interleukin 6 and pulmonary/radial artery interleukin 8 ratios (p = 0.001 and p = 0.05, respectively) decreased, while pulmonary/radial artery interleukin 10 ratio (p = 0.001) increased in patients without cardiopulmonary bypass as compared with patients with cardiopulmonary bypass.
Conclusions:
The pulmonary/radial artery equation is an innovative means for the evaluation of cytokine lung passage after coronary artery bypass grafting. The mode of lung ventilation has no impact on some cytokines after coronary artery bypass grafting in patients treated with cardiopulmonary bypass.
Introduction
Coronary artery bypass grafting (CABG) induces trauma and subsequent inflammation (1). On the other hand, complement activation and the release of oxygen-free radicals and mediators such as cytokines are influenced by the vastly utilized cardiopulmonary bypass (CPB) (2). Although a myriad of information on individual cytokines is available for patients undergoing CABG, only few studies lean on favoring CABG without CPB as a means to avoid inflammation during surgery (1, 3). Circulating cytokines such as anti-inflammatory interleukin 10 (IL10) and pro-inflammatory interleukin 6 (IL6) and interleukin 8 (IL8) play an important role in orchestrating the complex inflammatory response early after CABG, and have been evaluated together with complement activation in patients with and without CPB (4). Therefore, rather than the increase in individual pro-inflammatory cytokines, a few studies suggest that the disturbed balance between the key pro- and anti-inflammatory cytokines IL6, IL8, and IL10 may be more important in terms of humoral immunity (1, 5).
It has been argued that most of the pro-inflammatory cytokines are produced in the heart during CABG as compared with the lungs (2, 6). The lungs may play an important role in regulating circulating cytokines during CABG with CPB (2, 7–10). The period with no major blood flow through the pulmonary artery (PA) during CPB without assisted ventilation may affect the degree of endothelial reperfusion injury of the lungs (11). On the other hand, assisted ventilation during CPB ameliorates pulmonary endothelial function (10). A pulmonary endothelium-dependent vasodilation reactive to acetylcholine infusion in patients without CPB with maintained ventilation suggests preserved vascular endothelial function (12). The altered but reversible dysfunction of the PA endothelium may thus impact on the circulating cytokines during CPB with various lung ventilation modes.
CPB impacts on the pulmonary vasculature in patients undergoing CABG with different ventilation modes (13). It is still controversial as to whether surgery with CPB has an impact on the net inflammatory cytokine profile during CABG (4). We investigated whether lung passage alters the net concentration of some cytokines after CPB with various lung ventilation modes. We therefore studied the induced inflammatory cytokine lung passage of IL6, IL8, and IL10 in patients with different ventilation approaches as the net cytokine concentration may add to the decision concerning CABG.
Materials and Methods
Patient Population
The protocol for this prospective randomized study was approved by the Tampere University Hospital Ethics Committee. A total of 47 elective primary CABG patients offered their informed consent. Randomization was made using sealed blinded envelopes as previously described according to the ventilation technique and CPB (13). Briefly, three groups of patients were scheduled for elective CABG using on pump CPB technique: In the no-ventilation (NV) group, the intubation tube was detached from the ventilator after achieving full flow CPB. In the low tidal ventilation (LTV) group, continuous mechanical ventilation (3–4 mL/kg) was employed. In the continuous positive airway pressure (CPAP) group, a CPAP level of 10 cm H2O was applied, using an adjustable flow generator, WisperFlow (Respironics, Inc., Youngwood, PA). Ten additional patients suitable for CABG without CPB were selected to represent a referral group. In these patients without CPB, stabilization and exposure of the target vessel were achieved using a combination of pericardial stay sutures, a deep pericardial stitch and a mechanical stabilator, Octopus (Medtronic, Minneapolis, MN). Intra-coronary shunts were utilized whenever needed. A surgical blower-humidifier device (Axius™, Maquet, NJ) was employed routinely. In all patients, a manual recruitment maneuver was carried out at the end of CPB, keeping airway pressure up to 40 cm H2O for 15 s. The rest of the time, a positive end-expiratory pressure (PEEP) level of 5 cm H2O was applied. The exclusion criteria for all patients were as follows: previous malignancy, pre-existent pulmonary disease, pulmonary hypertension with systolic pulmonary arterial pressure (PAP) > 40 mmHg, depressed left ventricular ejection function (LVEF) < 50%, smoking or myocardial infarction during previous three months, cardiac decompensation period, acute coronary syndrome, infection, and use of corticosteroids or cyclooxygenase-2 (COX-2) inhibitors within one month. Anesthesia was induced with propofol (0.5–1.0mg/kg), sufentanil (0.8–1.0mg/kg) and rocuronium. Halogenated anesthetic gases were avoided due to possible influence on pulmonary hemodynamics. Occasional hypertensive episodes were controlled with nitroglycerin or labetalol.
Hemodynamic Measurements
Technically, surgery was uneventful for all patients. As previously reported, there were no differences between the groups considering preoperative variables (13). Postoperatively, there were no statistical differences between the groups observed at each time-point in terms of oxygenation index, alveolar-arterial oxygen gradient, and pulmonary shunt. Regardless of ventilation protocol, pulmonary vascular resistance index (dynes-sec-cm−5) decreased during CPB but remained elevated in patients without CPB despite any correlation with the cytokines.
Sample Collection and Elisa for Il6, Il8, and Il10
For evaluation of IL6, IL8, and IL10, arterial blood was collected from both radial artery (RA) and PA immediately after the induction of anesthesia (T1), 1 h after restoring ventilation/return of flow in all grafts (T2), and 20 h after restoring ventilation/return of flow in all grafts (T3). Elisa at every time-point was available in all but two out of 47 patients: For technical reasons, one PA sample at T2 was missing in a patient with CPB and LTV, while both PA and RA samples were missing in a patient with CPB and CPAP at T2. Altogether 840 samples were collected from 47 patients (421 RA and 419 PA samples). All samples were anticoagulated with ethylenediaminetetraacetic acid, immediately cooled at 4°C, and centrifuged within 30 min (1200 × g for 10 min); plasma was transferred to polypropylene test tubes and stored at −70°C until analyzed. IL6, IL8, and IL10 levels in plasma samples were determined by enzyme immuno assay (EIA) by using commercial reagents (IL6 and IL10: PeliPair ELISA, Sanquin, Amsterdam, the Netherlands; IL8: Opt EIA BD Biosciences, Erembodegem, Belgium). No adjustment was made for hemodilution. The detection limits were 0.3 pg/mL for IL6 and IL10 and 0.8 pg/mL for IL8, respectively.
Statistical Analysis
Data are presented as mean ± standard deviation (sd) and expressed as pg/mL. The ratio of blood cytokine concentration measured in the PA and the RA and adjusted to baseline describes the net production or elimination during passage through the lungs (1). PA/RA > 1 indicates a decrease of production of cytokines in the lungs, while PA/RA ⩽ 1 indicates that the cytokines are released after passage through the lungs (1). Statistical analysis was performed with SPSS software (SPSS Inc., Chicago, IL). A nonparametric Kruskal–Wallis test was employed to account for comparison of changes in cytokine levels between all groups at different time-points. The changes in cytokines in patients with CPB were compared with patients without CPB and within all groups at different time-points by the nonparametric Mann–Whitney U test. Repeated measures test was applied to study the interaction of the ventilation techniques and the three time-points on the PA/RA cytokine levels. A mixed between–within subjects analysis of variance was conducted to assess the impact of three different ventilation techniques with CPB, including CPAP, LTV, and NV on the PA/RA cytokine levels, across the three time-points. P-values less than 0.05 were considered statistically significant.
Results
Cardiac Index
For patients with CPB, cardiac index remained statistically stable throughout observation. After induction of anesthesia (T1), at 1 h after surgery (T2), and at the end of the study 20 h after restoring ventilation (T3), cardiac index was 2.1 ± 0.4, 2.6 ± 1.6, and 3.0 ± 0.6; 1.9 ± 1.0, 3.0 ± 0.7, and 2.6 ± 0.8; 2.1 ± 0.8, 3.1 ± 1.4, and 2.7 ± 1.0 in patients with CPAP, LTV, and NV, respectively.
Levels of Cytokines
An increase of all the cytokines, IL6, IL8, and IL10, was observed in all groups in both RA and PA samples (Tables 1 and 2). A temporary decrease of anti-inflammatory IL10 in the RA at T2 was observed in all groups, presumably owing to surgical trauma. In the PA at 1 h after surgery (T2), IL10 was 38.0 ± 30.5 in patients without CPB, while it was 17.2 ± 12.2, 11.4 ± 6.2, and 19.4 ± 20.4 in patients with CPAP, LTV, and NV, respectively (p = 0.049). In the RA at 1 h after surgery (T2), IL10 was 40.9 ± 33.2 in patients without CPB, while it was 16.3 ± 12.4, 11.2 ± 6.2, and 20.0 ± 22.2 in patients with CPAP, LTV, and NV, respectively (p = 0.007).
Perioperative and postoperative pulmonary artery cytokines IL6, IL8, and IL10 in patients undergoing coronary artery bypass surgery.
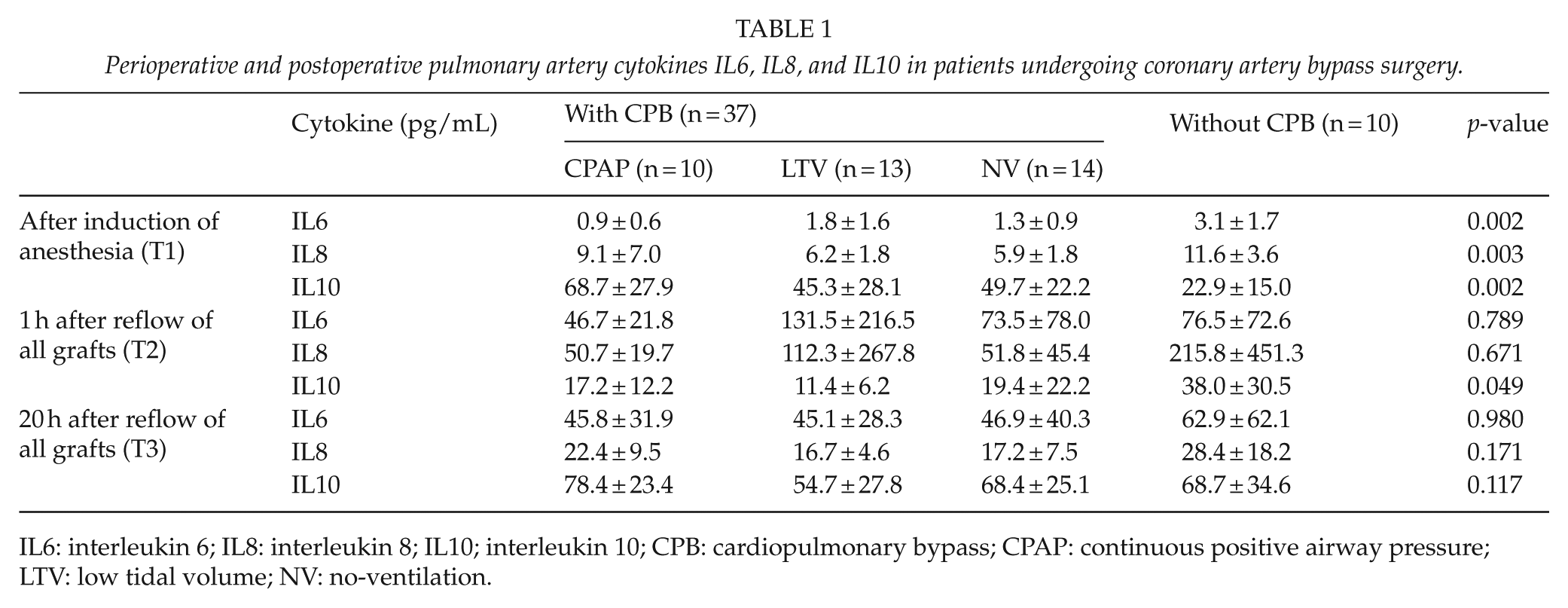
IL6: interleukin 6; IL8: interleukin 8; IL10; interleukin 10; CPB: cardiopulmonary bypass; CPAP: continuous positive airway pressure; LTV: low tidal volume; NV: no-ventilation.
Perioperative and postoperative radial artery cytokines IL6, IL8, and IL10 in patients undergoing coronary artery bypass surgery.
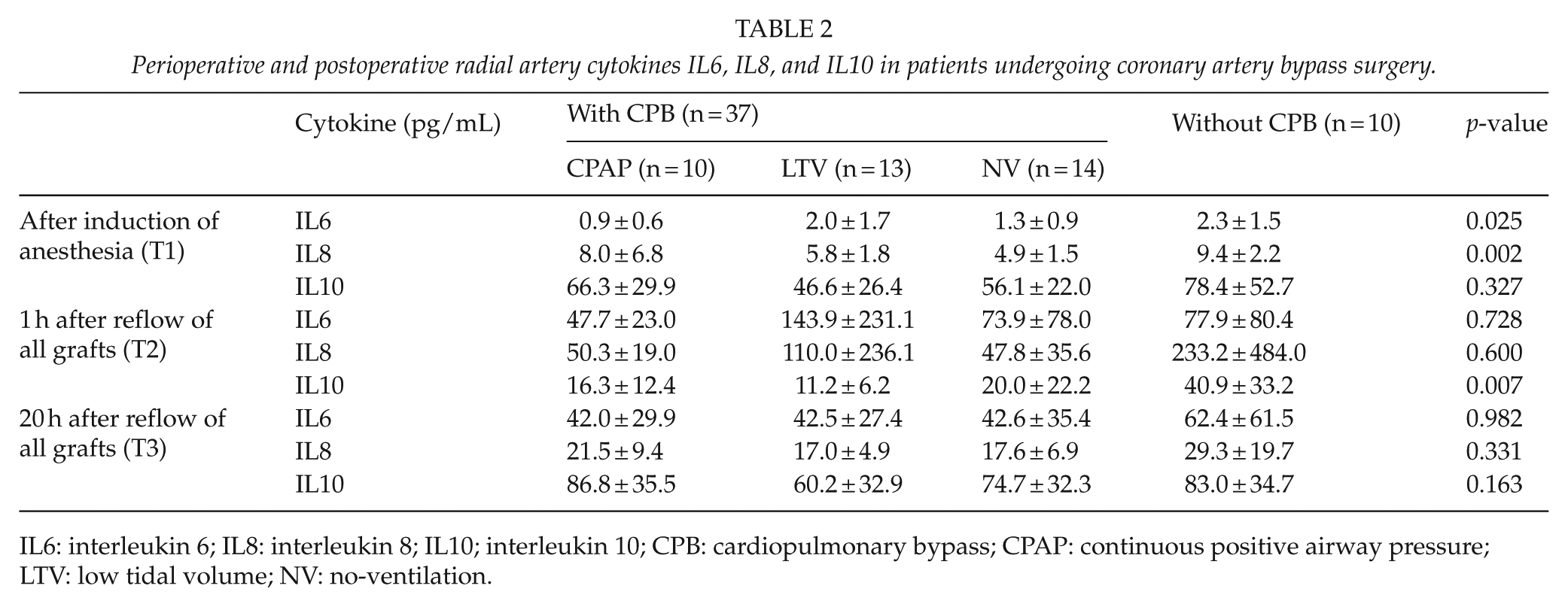
IL6: interleukin 6; IL8: interleukin 8; IL10; interleukin 10; CPB: cardiopulmonary bypass; CPAP: continuous positive airway pressure; LTV: low tidal volume; NV: no-ventilation.
Levels of Cytokines in Relation with PA and RA
As individual levels of cytokines do not reveal the net cytokine concentration after their passage through the lungs, we evaluated the simultaneous pulmonary arterial and radial arterial blood cytokine ratio (PA/RA) during CABG. The PA/RA ratios were adjusted to fold changes according to baseline values at time-point 1 to eliminate the effect of baseline differences in patients without CPB. PA/RA IL6 and PA/RA IL8 ratios decreased, while PA/RA IL10 ratio increased in patients without CPB as compared with patients with CPB (0.81 ± 0.20 vs 1.13 ± 0.33, p = 0.001; 0.88 ± 0.15 vs 0.91 ± 0.20, p = 0.055; and 4.17 ± 3.21 vs 1.04 ± 0.19, p = 0.001, respectively).
After surgery (T2), PA/RA for IL6 decreased in patients without CPB as compared with patients with CPAP, LTV, and NV (p = 0.001, Fig. 1A). At the end of the study 20 h after restoring ventilation (T3), PA/RA for IL6 remained 0.77 ± 0.19, indicating decreased PA/RA for pro-inflammatory IL6 in patients without CPB, while it was 1.16 ± 0.28 (p = 0.002), 1.21 ± 0.24 (p = 0.001), and 1.27 ± 0.51 (p = 0.001) in patients with CPAP, LTV, and NV, respectively. PA/RA for IL8 decreased at T2 in patients without CPB (0.77 ± 0.11) as compared with patients with LTV and NV (0.98 ± 0.21 and 0.90 ± 0.18, p = 0.004 and p = 0.04, respectively, Fig. 1B). In contrast, for the anti-inflammatory cytokine IL10, PA/RA increased after surgery in patients without CPB in contrast to patients with CPB despite CPAP, LTV, or NV. At the end of the study at 20 h after restoring ventilation (T3), PA/RA for IL10 remained increased with a significant range (4.08 ± 3.06) in patients without CPB, while it was 0.90 ± 0.22 (p = 0.001), 0.94 ± 0.22 (p = 0.001), and 1.11 ± 0.24 (p = 0.001) in patients with CPAP, LTV, and NV, respectively (Fig. 1C).
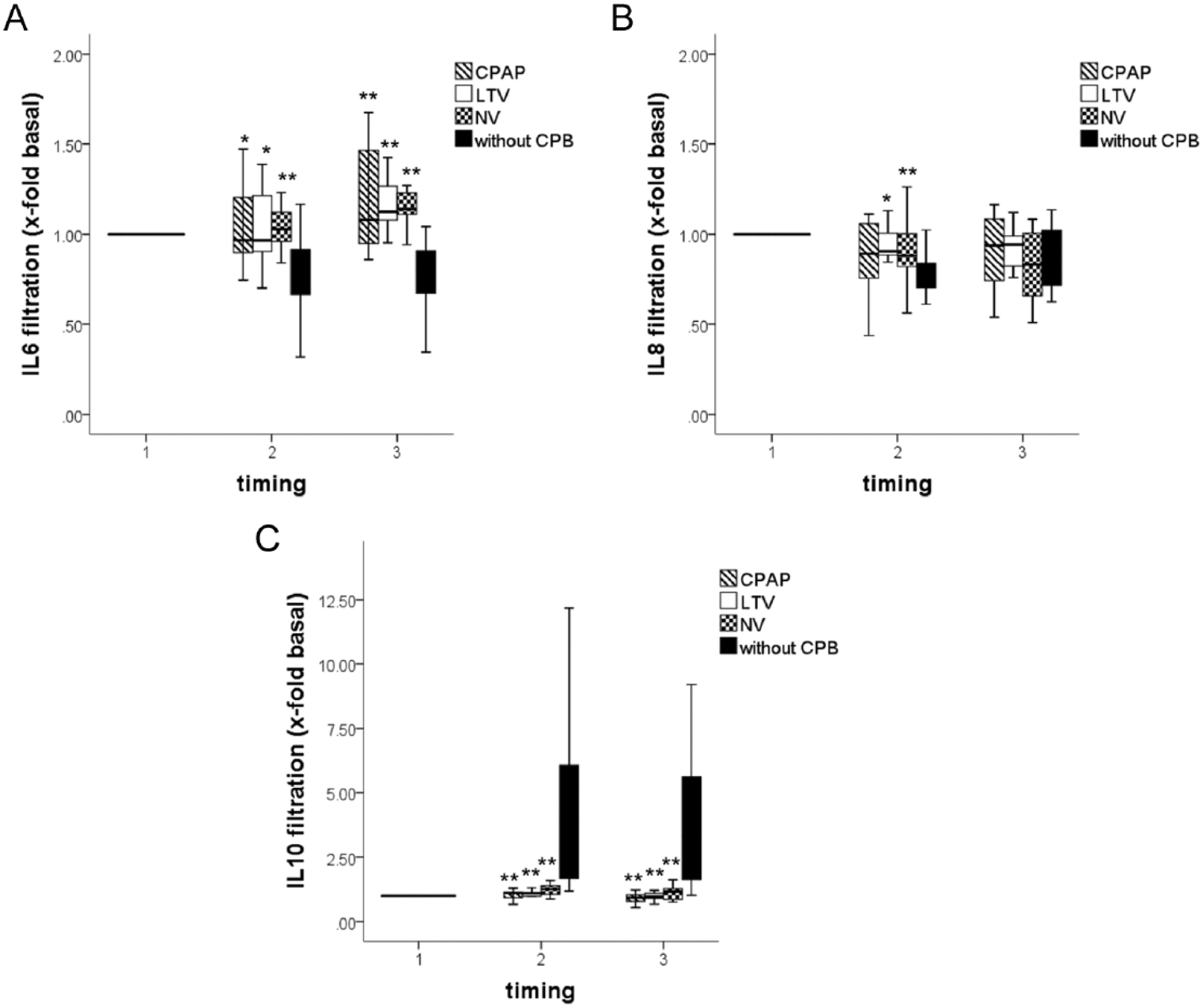
Calculated ratio of the pulmonary artery (PA) interleukin 6 (IL6), interleukin 8 (IL8), and interleukin 10 (IL10) divided by the radial artery (RA) IL6 (A), IL8, (B) and IL10 (C) after induction of anesthesia (T1), 1 h after restoring ventilation (T2), and 20 h after restoring ventilation (T3) in patients with CPAP, LTV, and NV with CPB (hatched, white and checked columns, respectively) and without CPB (black columns). Horizontal lines of the box show the median. Lines above and below the box indicate the 75th and 25th percentiles, respectively. Note decreased PA/AR value ⩽ 1 in patients without CPB, indicating decreased filtration in the lungs of pro-inflammatory IL6 cytokine (A). In contrast, PA/AR IL10 value > 1 in patients without CPB suggests excessive filtration of anti-inflammatory IL10 (C).
For PA/RA IL6, there was no significant interaction between ventilation modes and time (Wilks’ Lambda = 0.98, F(4, 64) = 0.19, p = 0.95, partial eta squared = 0.01). There was a substantial main effect for time (Wilks’ Lambda = 0.38, F(2, 32) = 26.15, p = 0.0005, partial eta squared = 0.24), with the groups showing an increase in PA/RA IL6 across the three time periods. The main effect comparing the three types of intervention was not significant (F(2, 33) = 0.334, p = 0.72, partial eta squared = 0.02), suggesting no difference in the effectiveness of the three ventilation modes for PA/RA IL6.
For PA/RA IL8, there was no significant interaction between ventilation modes and time (Wilks’ Lambda = 0.83, F(4, 64) = 1.23, p = 0.31, partial eta squared = 0.07). There was a substantial main effect for time (Wilks’ Lambda = 0.66, F(2, 32) = 8.03, p = 0.001, partial eta squared = 0.34), with the groups showing an overall decrease in PA/RA IL8 across the three time periods. The main effect comparing the three types of intervention was not significant (F(2, 33) = 0.87, p = 0.43, partial eta squared = 0.05), suggesting no difference in the effectiveness of the three ventilation modes for PA/RA IL8.
For PA/RA IL10, there was no significant interaction between ventilation modes and time (Wilks’ Lambda = 0.84, F(4, 64) = 1.51, p = 0.21, partial eta squared = 0.86). There was a substantial main effect for time (Wilks’ Lambda = 0.70, F(2, 32) = 6.99, p = 0.003, partial eta squared = 0.31), with the groups showing a reduction in PA/RA IL10 across the three time periods. The main effect comparing the three types of intervention was not significant (F(2, 33) = 3.21, p = 0.05, partial eta squared = 0.17), suggesting no difference in the effectiveness of the three ventilation modes for IL10.
Discussion
This study shows that CABG exerts a major inflammatory response despite different modes of lung ventilation during CPB, as assessed by the estimation of pulmonary passage of IL6, IL8, and IL10. The net cytokine concentrations of IL6, IL8, and IL10 were estimated by comparing the peripheral RA blood sample with the simultaneous PA blood sample. As being in between these two samples, the pulmonary vasculature may be responsible for producing excessive pro-inflammatory IL6 and IL8 in contrast to anti-inflammatory IL10 during CPB.
The individual plasma cytokine levels reflect poorly the cytokine expression at any organ level, least to say the effect of lung passage (1). Surgery without CPB is associated with decreased individual cytokine responses (3). Mainly based on the interpretation of individual cytokine changes, a burden of previous studies emphasizes the importance of inflammatory processes due to CPB itself. It was soon found, however, that the type of operative technique including CABG without CPB did not always prevent postoperative inflammation (4). The circulating inflammatory cytokines of the patient undergoing CABG may be altered by CPB (1); a pulsatile CPB strategy has been shown earlier to decrease peripheral endothelial cytokine levels (14). The anti-inflammatory IL10 in patients with CPB remained elevated as compared without CPB, but several other cytokines, such as IL4, interferon-γ (IFN-γ), IL8, and IL6, must also be involved in the complex cytokine network (14). A combination of low expression of pro-inflammatory cytokines together with a high expression of anti-inflammatory cytokines may also favor good outcome after surgery (14).
With the aid of calculating the simultaneous PA/RA ratio during CABG, it was demonstrated that the concentration of some cytokines is strongly altered during their passage through the lungs (1); it was postulated that the fully perfused lungs may actively produce cytokines during surgery without CPB. We investigated whether different lung ventilation impacts on the lung passage of pro-inflammatory IL6, IL8, and anti-inflammatory IL10 cytokines during CABG. We meticulously controlled the various ventilation modes and established three separate subgroups for patients with CPB. Lung ventilation had no additional effect on the net concentration of IL6, IL8, or IL10 during CABG in our study. Instead, the PA/RA values of IL6, IL8, and IL10 reflected the increased production of pro-inflammatory cytokines in the lungs.
As we did not study different ventilation modes for patients without CPB, the mixed between–within subjects analysis of variance was only applied for patients with CPB to investigate for the interaction of ventilation techniques and PA/RA cytokine levels. We utilized the PA/RA ratio adjusted to the baseline for all patients. The patients without CPB were postoperatively treated by recruitment of lung ventilation, including low PEEP and relatively high tidal volumes after mechanical ventilation; increased production of pro-inflammatory cytokines in the lungs may result from over distension of the lung alveoli during high tidal volumes, repeated closure, and reopening of the lungs. In contrast, avoiding over distension of lungs in patients with CPB including a lung-protective ventilation strategy (15) may explain the statistically non-significant changes in the PA/RA ratio of the studied cytokines among these patients. It may be interesting to study in the future different ventilation modes in patients without CPB.
It is tempting to speculate that the preserved vascular integrity of the endothelium of the lungs may explain these observations (5). The undamaged glycocalyx layer of the vascular endothelium serves as an indicator of impeccable endothelial function (16–18). While the heart, during CPB and related ischemia-reperfusion injury, is prone to release pro-inflammatory cytokines, the nearly normothermic and partially perfused lungs retain the capacity to act on cytokines (2, 6). The inflammatory cytokines may interact with polymorphonuclear cells during CPB (2). Similarly, the vascular endothelium of both the lungs and the heart in patients without CPB is under constant hemodynamic pressure-induced stress that may result in the excessive production of cytokines released during surgery (14, 17).
Angdin et al. (12) have analyzed endothelium-dependent reactivity by studying the acetylcholine response of the pulmonary vasculature; it was found in a cohort of patients undergoing aortic valve replacement and CABG that the vasculature did not react with acetylcholine in most of the patients after CPB. The changes of cytokines may be masked by the heterogeneity of the patients recruited in some studies. Importantly, the decrease of vascular reactivity does not exclude the possibility of complete reversible endothelial dysfunction and subsequent recovery. The pulmonary endothelial dysfunction due to CPB (19) may, over the long term, be reversible despite the effect of lung passage on the concentration of some cytokines.
Limitations of this study include the small sample size of our study that precludes assessing any differences in the clinical outcome. Only stable patients with preoperatively impeccable lung function were included. The clinical nature of our study excluded the possibility to perform vasculature histology. In future, the impact of pneumoproteins may be investigated to confirm plausible lung insult after CPB. The strict inclusion criteria provided comparable patients since smoking, anti-inflammatory medication, and recent acute events were among the exclusion criteria (13). We interpreted the PA/RA value to indicate the impact of lung passage to interfere on the net concentration of some cytokines as previously stated (1). The net cytokine concentration after CABG is increased during CPB despite different ventilation modes during surgery.
In summary, CABG has a major net impact on the concentration of some cytokines as observed by comparing pulmonary arterial cytokine levels with radial arterial levels despite different lung ventilation modes. Estimating cytokine lung passage with the PA/RA equation may provide a practical means for the evaluation of the net inflammatory response after CABG; it remains to be shown whether increased pro-inflammatory cytokines after lung passage may affect long-term clinical outcome after CABG. This study suggests that some cytokines pertinent for systemic inflammatory reaction after CABG and CPB are not impacted by additional lung ventilation maneuvers. This message may direct clinical practice on avoiding needless ventilation techniques during CABG with CPB.
Footnotes
Acknowledgements
This study has been presented at the Scandinavian Association for Thoracic Surgery annual meeting held in Gothenburg, Sweden, 3–5 September 2014.
Declaration of Conflicting Interests
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This study was financially supported by the Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital, the unit of Heart Center Co Grant Z60044, the Finnish Cultural Foundation, and the Tampere Tuberculosis Foundation.