
Abstract
Background and Aims:
Injuries are often missed during the primary and secondary surveys in trauma patients. Studies have suggested that a formal tertiary survey protocol lowers the number of missed injuries. Our aim was to determine the number, severity, and consequences of injuries missed by a non-formalized trauma tertiary survey, but detected within 3 months from the date of injury in trauma patients admitted to a trauma intensive care unit.
Material and Methods:
We conducted a cohort study of trauma patients admitted to a trauma intensive care unit between 1 January and 17 October 2013. We reviewed the electronic medical records of patients admitted to the trauma intensive care unit in order to register any missed injuries, their delay, and possible consequences. We classified injuries into four types: Type 0, injury detected prior to trauma tertiary survey; Type I, injury detected by trauma tertiary survey; Type II, injury missed by trauma tertiary survey but detected prior to discharge; and Type III, injury missed by trauma tertiary survey and detected after discharge.
Results:
During the study period, we identified a total of 841 injuries in 115 patients. Of these injuries, 93% were Type 0 injuries, 3.9% were Type I injuries, 2.6% were Type II injuries, and 0,1% were Type III injuries. Although most of the missed injuries in trauma tertiary survey (Type II) were fractures (50%), only 2 of the 22 Type II injuries required surgical intervention. Type II injuries presumably did not cause extended length of stay in the intensive care unit or in hospital and/or morbidity.
Conclusion:
In conclusion, the missed injury rate in trauma patients admitted to trauma intensive care unit after trauma tertiary survey was very low in our system without formal trauma tertiary survey protocol. These missed injuries did not lead to prolonged hospital or trauma intensive care unit stay and did not contribute to mortality. Most of the missed injuries received non-surgical treatment.
Introduction
Injuries are often missed during the initial management (primary and secondary surveys) of severely injured patients (1–6). Typical missed injuries include musculoskeletal/orthopedic injuries (1, 7), especially fractures (6,8). The most common body regions of missed injuries vary depending on the study, but many such studies frequently identify the head and neck (3, 7, 8), chest (3, 6, 7, 9), and extremities (3, 4, 6–12) as the most common regions of missed injuries.
Contributing factors to delayed diagnosis may be related to the patient or health care personnel (10, 11). The risk of a missed injury increases when the patient has multiple injuries and/or the patient is unstable (7, 13). Studies have shown that head injuries (4, 6, 13, 14), mechanical ventilation (5, 8), low scores on the Glasgow Coma Scale (GCS) (2, 4, 7, 15), and high Injury Severity Scores (ISS) (2, 4, 7, 15, 16) can lead to delayed diagnosis. Inadequate clinical examinations (9, 11), departures from clinical routines (11), and misinterpreted or inadequate radiographs (2, 4, 5, 8, 11, 17) also contribute to delayed diagnoses. In addition, patients from road traffic accidents are more likely to have missed injuries (4, 8, 11).
Delayed diagnoses can lead to changes in treatment (6, 18), longer stays in the intensive care unit (ICU) and hospital (2, 12), and, albeit rarely, to higher morbidity or even mortality (2, 4).
According to the current literature, the incidence of missed injuries in trauma patients varies across different studies from 0.6% to 39% (1–16, 18, 19). These differences in the results may stem from differences between the study populations and methods, and especially from differences in the criteria which determine whether an injury has been missed. Some studies of missed injuries or delayed diagnoses define an injury as missed if primary or secondary survey fails to detect it (1, 2, 4, 7, 10, 11).
Primary survey aims to identify and prioritize the most life-threatening injuries in the emergency room (ER). Secondary survey is typically a head-to-toe clinical examination before the patient leaves ER. The early 1990s saw the introduction of a tertiary survey to reduce the number of missed injuries (3). It is often done within the next 24 h in the ICU or in the ward. According to a study by Janjua et al. (8), 39% of the total number of injuries went undetected after the primary and secondary surveys. Conducting a tertiary survey within 24 h resulted in the detection of 56% of previously missed injuries and 90% of clinically significant missed injuries.
A recent systematic review of the effect of trauma tertiary survey (TTS) on missed injuries criticizes the current literature for its substantial heterogeneity. The review reports that the definition of missed injuries varies across studies, so any comparison of current and future studies will require a clear, consistent definition of a missed injury. Studies included in the review were classified into two groups depending on how they defined a missed injury. The most common definition (Type I) for a missed injury was the one missed by primary and secondary surveys, but detected by the TTS. A second definition (Type II) includes injuries missed by the TTS. The mean missed injury rate for Type I injuries was 4.3% (range: 1.26%–65%). Only one study reported Type II injuries, missed at a rate of 1.5% (20).
Despite primary, secondary, and tertiary surveys, some injuries still go undetected (7, 8, 13, 21). Some of these injuries are diagnosed only after the patient is discharged (18, 21). Nowadays, the tertiary trauma survey is more common, and some trauma units have created their own protocol for tertiary surveys to decrease the incidence of missed injuries in trauma patients. According to the literature, a standardized TTS protocol reduces the incidence of missed injuries (20, 22, 23).
The aim of the study was to determine the number and severity of injuries missed in primary, secondary, and tertiary surveys, but which were diagnosed prior to discharge. We focused on required treatments and how these injuries affected the outcome of trauma patients admitted to trauma intensive care unit (TICU). The study was an internal validation of an existing outcome related to the use of a non-formalized TTS protocol in our trauma services.
Material and Methods
We conducted a prospective cohort study of patients who sustained multiple injuries and were admitted to the Töölö Hospital TICU between 1 January and 17 October 2013. We excluded patients with isolated brain injuries who were admitted to the neurological ICU in our hospital. Our study did include trauma patients admitted to the TICU from the emergency department, from an angiographic procedure after primary and secondary surveys in the emergency department or from the operating room (OR). We excluded patients admitted to the TICU from an inpatient ward, from the OR after undergoing elective surgery, patients discharged from an inpatient ward prior to surgery, and patients with severe infection. We also excluded patients who died prior to undergoing tertiary survey.
During the study period, no formal protocol was established for TTSs. One of the seven trauma consultants clinically examines trauma patients admitted to the TICU the morning after admission. Over the weekend, the on-call orthopedic surgeon (or trauma consultant) performs the tertiary survey based on an oral agreement of how to perform the TTS, which includes rechecking the radiological studies, laboratory test results, and medical case records beforehand and prior to performing a full clinical examination. Except for the two authors (T.S. and L.H.), physicians performing the TTS were uninformed about the on-going study.
We analyzed injuries identified in the TTS, after the TTS, but prior to discharge, or in 3 months (90 days) from the date of injury, according to the number and severity of missed injuries, the delay in their diagnosis, and factors which may have contributed to missing the injury. We used the Abbreviated Injury Scale (AIS) to evaluate the severity of injuries.
On TICU admission, the TICU nurses recorded all diagnosed injuries in a study file. During the stay in the TICU, the nurses took note of all new injuries, including the date of diagnosis, in the study file. One of the authors (E.T.) reviewed the electronic medical records for each patient up to 3 months from the date of injury to identify any injuries missed in the primary, secondary, and tertiary surveys. The electronic database in use covers only public sector in Southern Finland (approximately 1.6 million inhabitants). So, patients treated in other public hospital districts or in private sector after discharge from Töölö hospital were not included in the 3-month follow-up.
Data collected included age, sex, injury date, mechanism of injury, intubation status on TICU admission, reason for intubation, diagnosed injuries, date and time of injury diagnosis, length of stay (LOS) in the TICU, LOS in the hospital, and mortality prior to discharge. The person collecting all the data was uninvolved in treating the patients.
We classified injuries into four types: Types 0, I, II, and III (Table 1). Type 0 comprised injuries detected in the primary or secondary survey. Type I injuries were identified in the TTS. Type II injuries included any injury missed at the primary, secondary, and tertiary surveys but detected prior to discharge from the hospital. Type III injuries were detected within 3 months from the date of injury. Our main focus was on Type II injuries. We re-examined medical records for all Type II injuries to evaluate the effect of any delay in diagnosis on the clinical course during the hospital stay, whether the injury caused an extended LOS or surgical interventions. We evaluated the effect of a missed injury on a longer LOS based on whether the delayed diagnosis led to complications, the postponement of surgical interventions or morbidity, or prevented the patient’s discharge from hospital or transfer to another facility.
Injury classification.
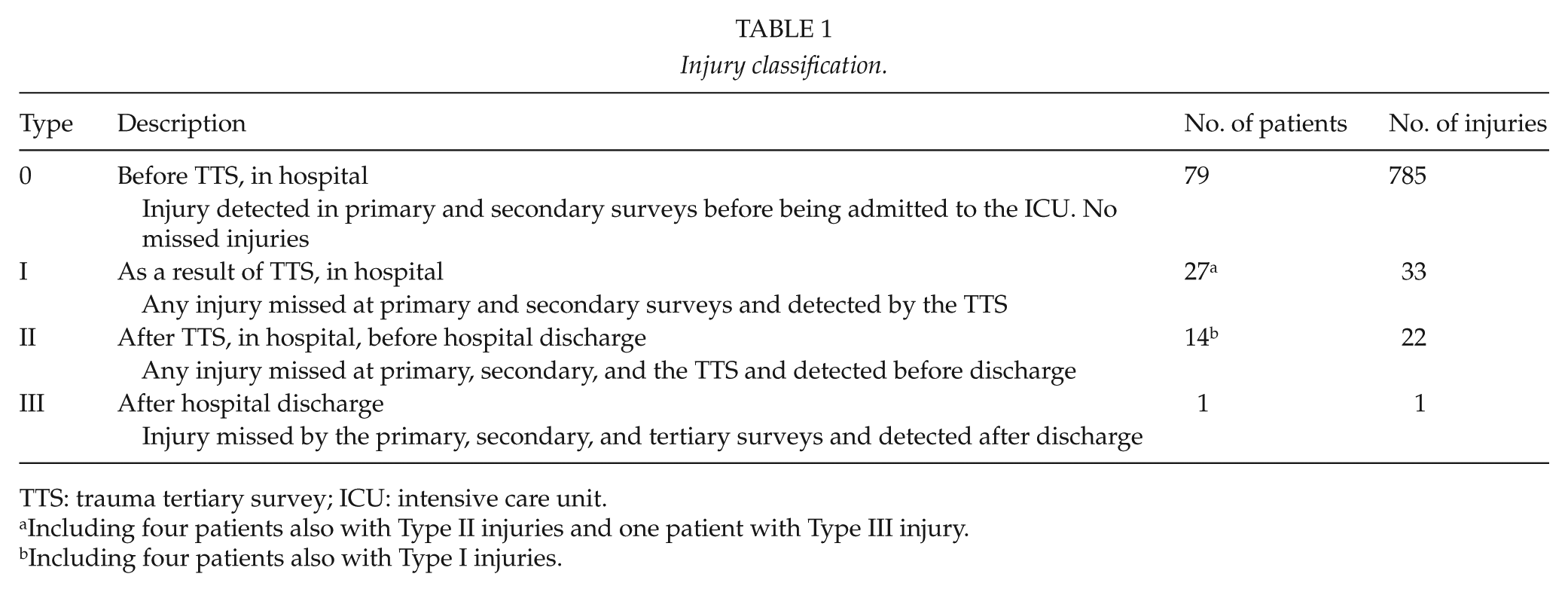
TTS: trauma tertiary survey; ICU: intensive care unit.
Including four patients also with Type II injuries and one patient with Type III injury.
Including four patients also with Type I injuries.
SPSS Statistics 21.0 (IBM Corp, Armonk, NY, USA) served for the statistical analysis when appropriate. The Institutional Review Board (Helsinki University Central Hospital) approved the study protocol, and according to Finnish Law, no ethical board review was necessary for this study.
Results
Demographics
Of the 360 patients admitted to the TICU during the study period, 115 met the inclusion criteria of our study. The majority of the patients were men (n = 88, 77%) with the mean age of 46 ± 19 years (range: 27–65 years), and the mean age of the female patients was 52 ± 19 years (range: 33–72 years). Two most common mechanisms of injury were high fall (25%) and motor vehicle accident (MVA) (23%). The average TICU LOS was 8 ± 7.6 days (median: 5, range: 1–48 days), and overall hospital LOS was 16 ± 13 days (median: 12, range: 1–64 days). A total of 37 patients underwent intubation prior to TICU admission, and 6 were intubated in the TICU prior to TTS. Thus, 43 (37%) patients were intubated and sedated when the clinical TTS was conducted. Most of the patients were admitted to the TICU directly from the emergency department (n = 79, 69%), and 18 (16%) patients were transferred to the TICU directly from another hospital. Altogether 17 (15%) of the patients underwent surgical or angiographic procedures prior to the TICU admission, and 85% underwent trauma computed tomography (CT) (head, neck, and body CT). Of the 115 patients, 1 (a Type 0 patient) died during the hospital stay. The demographics of the study population appear in Table 2.
Characteristics of the study population.
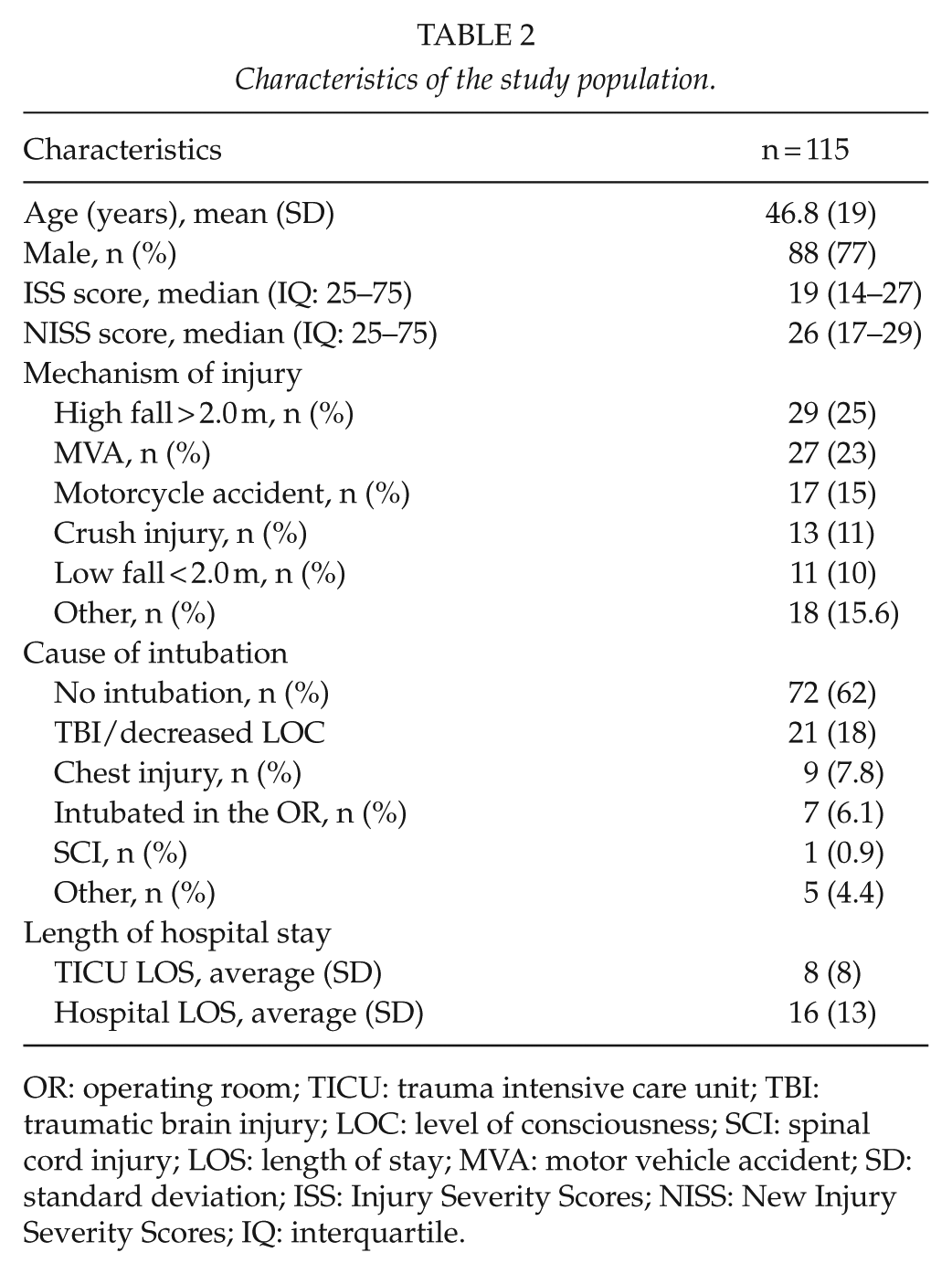
OR: operating room; TICU: trauma intensive care unit; TBI: traumatic brain injury; LOC: level of consciousness; SCI: spinal cord injury; LOS: length of stay; MVA: motor vehicle accident; SD: standard deviation; ISS: Injury Severity Scores; NISS: New Injury Severity Scores; IQ: interquartile.
Type 0 Injuries
The total number of injuries diagnosed during the hospital stay in 115 patients was 841 (average 7.3 injuries per patient). Of these injuries, 785 (93%) were Type 0 injuries that were detected prior to performing the TTS. In 79 (69%) patients, no additional injuries were found in the TTS or later during the hospital stay prior to or after discharge. Type 0 injuries occurred most often in the thoracic region (29% of all diagnosed injuries). The median AIS in Type 0 injuries was 2 (range: 1–5). The distribution according to body regions appear in Table 3. The distribution of AIS values appear in Fig. 1.
Injuries in different body regions in primary and secondary surveys (Type 0), in TTS (Type I), and after TTS (Type II) in 115 patients.
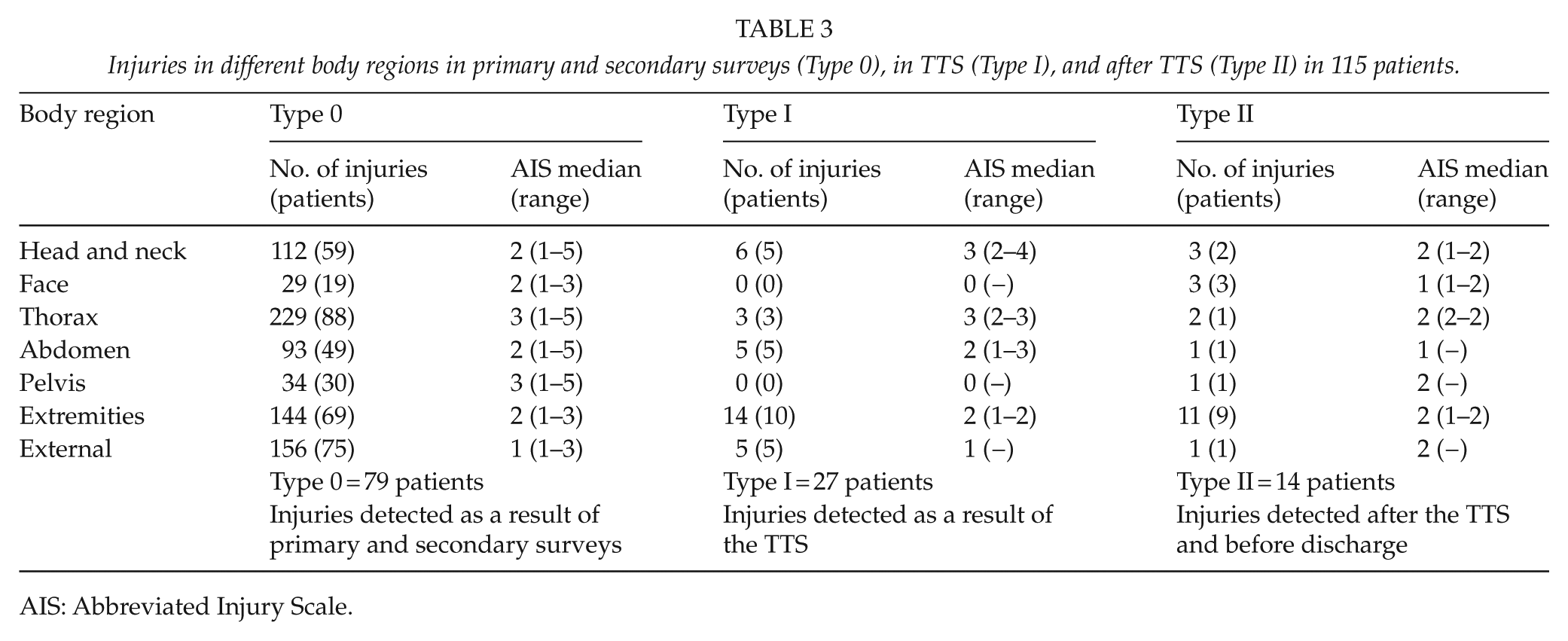
AIS: Abbreviated Injury Scale.
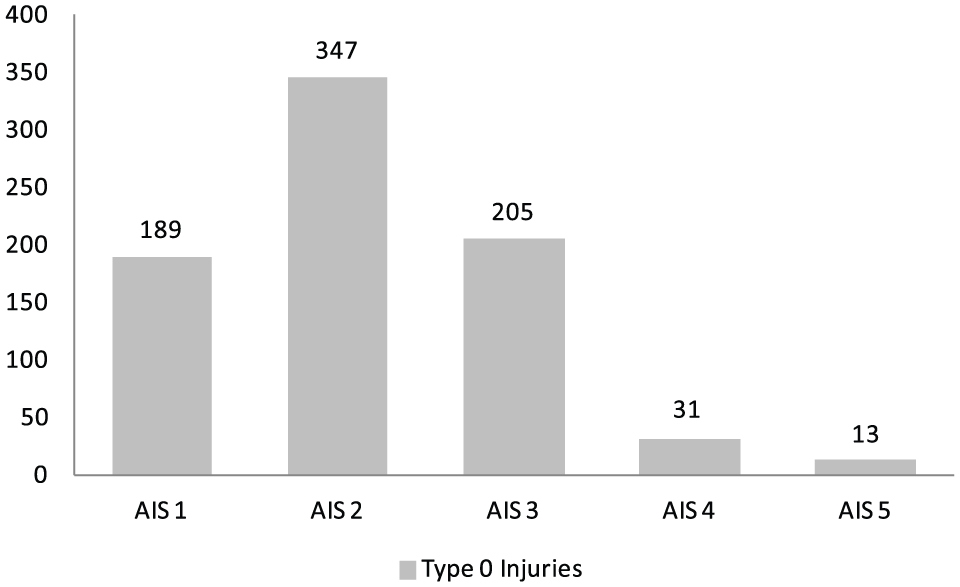
Distribution of AIS values in Type 0 injuries.
Type I Injuries
Of all the injuries diagnosed during the study period, 33 (3.9%) were Type I injuries, that is, new injuries identified by the TTS. Type I injuries appeared in 27 (23%) patients. Of these 27 patients, 4 also had injuries (Type II) found after the TTS and 1 also had an injury detected after hospital discharge (Type III injury). Extremity injuries accounted for the highest number of Type I injuries (missed in the primary and secondary surveys, but identified in the TTS; 42%). The TTS revealed no additional injuries (Type I) in the face or pelvic region. The most severe Type I injuries (highest AIS) occurred in the head and neck regions and in the chest region, with a median AIS of 3 (range: 2–4) and 3 (range 2–3), respectively. The distribution of Type I injuries appear in Table 3. The distribution of AIS values of Type I injuries appear in Fig. 2.
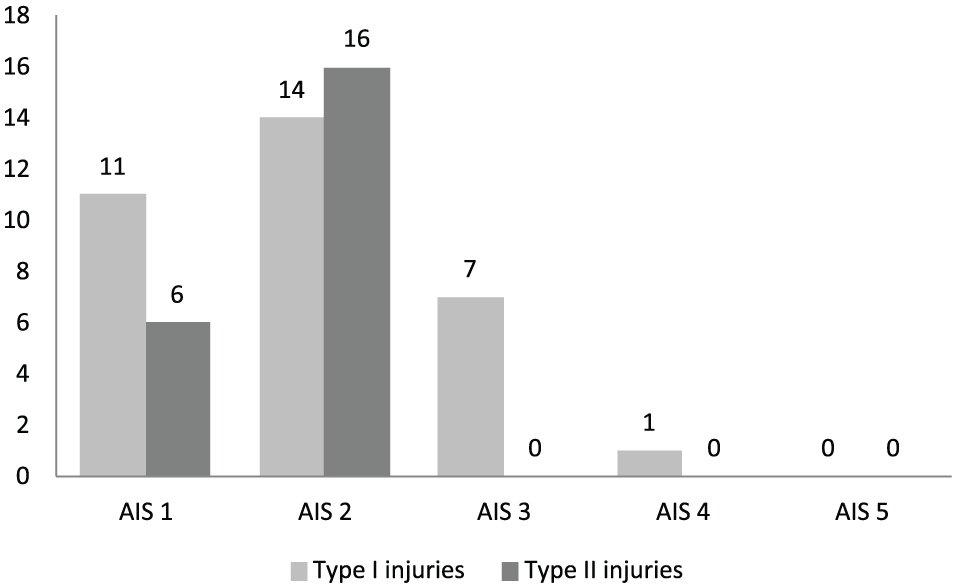
Distribution of AIS values in Type I and Type II injuries.
Type II Injuries
The number of Type II injuries was 22 (2.6% of all diagnosed injuries), and these injuries occurred in 14 patients (12% of the entire study population). Four patients had both Type I and II injuries. The highest concentration (48%) of Type II injuries occurred in the extremities. The median AIS in extremity injuries was 2 (range: 1–2). All Type II injuries had an AIS value <3. Most of the injuries that the TTS missed were fractures (11/22, 50%), especially in the region of the hand and wrist (6/22, 27%). Nerve injuries accounted for 18% (4/22) of Type II injuries. These injuries included a contusion of the sciatic nerve presenting as peroneal nerve paresis, contusion of brachial plexus presenting as a defect in the function of axillary nerve, peripheral facial nerve paresis, and paresis of the oculomotor nerve. Two of the latter occurred on an intubated patient, which precluded diagnosis during the TTS. Two of the Type II injuries required surgical intervention (a loosening of two tooth with small fragment of maxilla bone and a fracture of the first metacarpal bone).
A list of Type II injuries appears in Table 4. No Type II injuries were deemed to have caused extended LOS in the TICU or in hospital. Due to the low number of Type II injuries, we performed no statistical analysis between patients with and without Type II injuries; the possibility of β-type error was considered too high.
Patients with type II injuries.
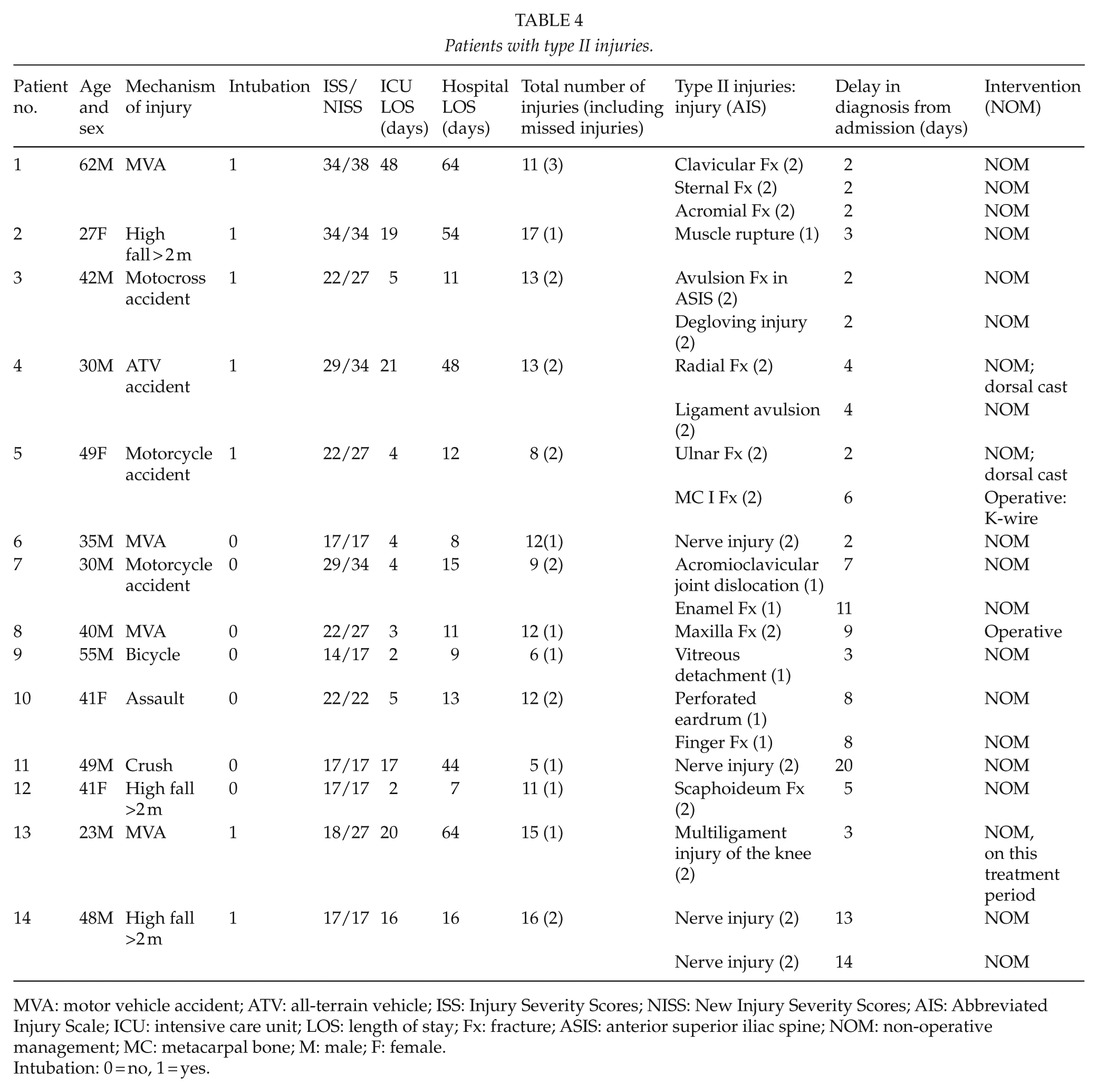
MVA: motor vehicle accident; ATV: all-terrain vehicle; ISS: Injury Severity Scores; NISS: New Injury Severity Scores; AIS: Abbreviated Injury Scale; ICU: intensive care unit; LOS: length of stay; Fx: fracture; ASIS: anterior superior iliac spine; NOM: non-operative management; MC: metacarpal bone; M: male; F: female.
Intubation: 0 = no, 1 = yes.
Most Type II injuries (59%) were diagnosed within 5 days of the admission to the hospital. The median delay in detecting these injuries was 4 days (range: 2–20 days). Four of the injuries were diagnosed after 10 days in hospital; of these, three were nerve injuries.
Type III Injuries
The 3-month follow-up data were available in 92 patients (80% of all patients). In these patients, one (0.1% of all diagnosed injuries) injury was diagnosed after the discharge and within 3 months of date of the injury. The injury was diagnosed outside the public health care system. The injury was a partial rupture of rotator cuff, and as a consequence of this, the patient was incapable to return to work at the time of the diagnosis (78 days from injury).
Discussion
In this study of TICU patients without formal TTS protocol, primary, secondary, and tertiary surveys missed 2.6% of all injuries diagnosed in hospital and within 3 months after trauma. None of these missed injuries were life-threatening or extended the LOS in TICU or in hospital. The AIS range from Type 0 injuries to Type II injuries narrows, from 1–5 to 1–2 (Table 3), indicating that Type II injuries were less severe. This result suggests that the lack of a formal TTS does not prevent achieving a low incidence of missed Type II injuries in TICU patients.
Only one Type III injury came to light within the 3-month follow-up period. This injury was quite trivial by nature (partial rupture of rotator cuff) and did not require operative treatment. However, it prolonged the patient’s absence from work.
The strength of our study was that missed injuries and any delays in diagnosis were double-checked, first by the TICU nurses who prospectively compiled this information in a study file and second by one of the authors (E.T.) reviewing the electronic medical records.
The limitations in our study include its study population of 115 patients, which is statistically insufficient for broader generalizations. Low number of patients also makes the interpretation of the results more vulnerable to β-type error. Consequently, we can identify no significant difference between the two groups (Types 0 and I vs Type II and III) in possible contributing factors to missed injuries, such as age, sex, ISS and NISS scores, and intubation. In both groups, the most common mechanisms of injury were a high fall and MVA. Also, the percentage of patients undergoing trauma CT was approximately the same in both groups. Therefore, one cannot view these as contributing factors either.
In addition, our study period was relatively short, which was the main reason for its low number of patients. A longer follow-up would have yielded a higher number of patients, thus rendering the data more reliable.
Most of the studies reporting missed injuries define a missed injury as one that goes undetected in the primary or secondary survey; in other words, injuries detected by TTS qualify and are reported as missed injuries (1, 2, 4, 7, 8, 10, 11, 18). In only a couple of these studies does the number of missed injuries rise after TTS (7, 8). Unfortunately, the number of missed injuries appears as a percentage of injuries detected after the primary and secondary surveys; consequently, the results are incomparable to those of our study (7). From the study by Janjua et al. (8), Type II missed injury rate was 17%, which is considerably higher than our missed injury rate of 2.5%.
Only Biffl et al. (13) defined a missed injury in the same manner as we defined our Type II injuries. They evaluated the effect of a formalized TTS protocol on the missed injury rate. Before formalizing the TTS protocol, the missed injury rate in TICU patients was 5.7% (13), which is higher than in our study.
In the study by Biffl et al. (13), the rate of Type II injuries after formalizing the TTS protocol was similar to our non-formalized protocol (3.4% vs 2.6%). The decrease in the rate of missed injuries led to a suggestion by Biffl et al. that formalizing the TTS protocol may reduce the number of missed injuries detected after TTS. On the other hand, Keijzers et al. (21) found that formalizing the TTS protocol failed to reduce missed injury rates. They reported the rate of Type II injuries of 3.8% and 4.8% before and after implementation of formal TTS (21).
Keijzers et al. also reported Type III injuries at 1 month and 6 months after hospital discharge. They conducted a scripted follow-up telephone interview to figure out the missed amount of Type III injuries. This missed injury rate before and after formalizing the TTS was quite similar at 1 month (13.7% vs 11.5%) and 6 months (3.8% vs 3.3%). However, TTS was performed only to some of the patients in both pre- and post-periods. Their follow-up rates were about 50% at 1 month and about 40% at 6 months (21). In our study, the Type III missed injury rate was considerably lower (0.1% of all injuries) and the follow-up rate, respectively, higher (80%).
In our system, without formal TTS protocol, TICU patients undergo re-examination after they are stabilized. There is only oral agreement on the performance of TTS in TICU. Every physician has his or her own way of conducting the TTS, so it is in no way standardized. Formalization of the TTS would do more to standardize the performance of the TTS, but its effect on the clinical course of patients would be negligible. The incidence and severity of Type II injuries in the current system are very low, with 2.6 non-significant injuries per 100 injuries diagnosed.
In studies by Janjua et al. (8) and Roessle et al. (9), only one person performed TTS, which assures the repeatability of the TTS protocol, but also exposes the results to systematic error.
Keijzers et al. (21) found out that formalization significantly improved the rate of TTS performed, from 27% to 42%. In our study, all of the patients underwent TTS, so implementation of a formal TTS at our institution is unlikely to improve the compliance with TTS protocol.
Compared to the study by Biffl et al. (13), the injuries missed by the TTS in our study were considerably less vital. However, in our study, 86% (99/115) of all patients and 92% (12/13) of all Type II injury patients had undergone pan-scan CT (CT of the head, neck, and body) on arrival, whereas from 1997 to 2001, when Biffl et al. conducted their study, the availability or utilization rate of trauma CT may have been lower than it is now. However, this information was not included in Biffl et al.’s study (13). In our study, missed injuries usually came to light because of a patient’s complaints about pain, a patient’s altered sensory or motor function, an additional interpretation of pre-existing radiographs, or a decision to take more focused radiographic images off an already existing injury. Our study results indicate that the current non-formal TTS protocol is of high quality and should definitely continue.
In conclusion, the missed injury rate after non-formal TTS was very low, and these missed injuries did not lead to prolonged TICU or hospital stay, or contribute to mortality. Most of the missed injuries underwent non-surgical treatment. Consequently, we were unable to identify any strong indication that would require a change to a formalized TTS over the present protocol of consultant-driven “ad hoc” TTS. One could argue, however, that the formalized TTS protocol would not necessarily harm overall trauma care performance in our unit, although such formalization would have only a negligible impact on it.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.