
Abstract
Background:
Intracranial complications of paranasal sinusitis have become rare due to widespread and early use of antibiotics. Potentially life-threatening intracranial complications of sinusitis include subdural empyema, epidural and intracerebral abscess, meningitis, and sinus thrombosis. Patients with intracranial complication of sinusitis can present without neurological signs, which may delay diagnosis and correct treatment.
Aims:
Our aim was to evaluate the diagnostics, treatment, and outcome of sinusitis-related intracranial infections at our tertiary referral hospital with a catchment area of 1.9 million people.
Materials and Methods:
We retrospectively collected data on all patients diagnosed and treated with an intracranial infection at the Helsinki University Hospital, Helsinki, Finland, during a 10-year period between 2003 and 2013.
Results:
Six patients were diagnosed to have a sinusitis-related intracranial infection. Four patients had an epidural abscess, one both an epidural abscess and a subdural empyema and one a subdural empyema. The most common presenting complaint was headache (100%) followed by fever (83%), vomiting (50%), nasal congestion (50%), forehead lump (34%), and neck stiffness (17%). All patients were managed surgically. Most (83%) patients recovered to premorbid state without neurological sequelae. One patient died intraoperatively.
Conclusion:
Patients with a sinusitis-related intracranial suppuration typically present with signs of raised intracranial pressure rather than signs of sinusitis. Most are likely to need neurosurgical intervention and evacuation of the abscess without delay.
Introduction
In the antibiotic era, intracranial complications of paranasal sinusitis have become rare (1, 2). A 3.7% complication rate has been reported in hospitalized patients with acute or chronic sinusitis (3). Potentially life-threatening sinusitis-related intracranial com-plications include subdural empyema, epidural and intracerebral abscess, meningitis, and venous sinus thrombosis (1–3). Most frequently, such complications are associated with frontal sinus and then, in order, with ethmoid, sphenoid, and maxillary sinuses (4).
Adolescents and children older than 6 years of age are considered to be at greater risk of complications from pyogenic upper respiratory tract infections for two reasons. First, the vascularity of their diploic system is at its peak, and second, there is a relative increase in blood supply to their still-developing frontal sinuses (1, 5). A male predominance has been reported, at a rate of roughly 2:1, for reasons not yet completely understood (2, 6–8). According to Reeves et al. (9), normal development of the paranasal sinuses in adolescent men may result in anatomical differences that predispose them to sinusitis.
Intracranial complications from the paranasal sinuses can occur as a direct extension through sinus wall erosion, existing foramina, or traumatic dehiscence, as well as through the valveless diploic venous drainage (10). Spread of infection through the posterior wall of the frontal sinus may result in the formation of an epidural abscess or subdural empyema. Spread of infection from the frontal sinus either through the anterior bony wall or through the venous drainage may result in osteomyelitis of the frontal bone and formation of a subperiosteal scalp abscess, “Pott’s puffy tumor” (PPT) (11). Teenagers are particularly prone to the latter complication as a result of increased diploic vein flow and a loose connection between the frontal sinuses and the bone marrow space compared with adults. Because diploic veins drain the frontal sinuses and communicate with the dural venous plexus, frontal sinus–related septic thrombi can propagate through this venous system (12). With PPT, intracranial complication is a common finding; it affects 60%–85% of PPT patients (13 –15). Still, long-term sequelae are uncommon following combined surgical and antimicrobial therapy, having been reported in less than 15% of cases (1, 7).
We describe the treatment and outcome in a series of six patients diagnosed with a sinusitis-related intracranial complication at our institution during a 10-year period.
Materials and Methods
As a tertiary care referral center, the Helsinki University Hospital and its Departments of Otorhinolaryngology—Head and Neck Surgery and Neurosurgery see patients from an area of approximately 1.9 million people. Our institution is the only tertiary care referral center in its catchment area, which makes population-based studies possible. We retrospectively collected data on all patients diagnosed and treated with intracranial infection at our hospital during a 10-year period between August 2003 and July 2013. Post-operative and post-traumatic intracranial infections were excluded from the search.
Our larger cohort consisted of 42 intracranial abscesses including 35 brain abscesses and 7 epidural/subdural abscesses. None of the 35 brain abscesses was related to sinusitis. Instead, 16 were related to a dental/oral infection, 6 to immunosuppression (HIV, lymphoma, and chemotherapy), 1 to a previous mastoiditis, 1 to a cholesteatoma, 1 to a combined maxillary sinusitis and dental work-up while 2 were hematogenic and 2 related to a soil infection. For six patients, the etiology of the infection was unclear. For six out of the seven patients with an epidural/subdural abscess, there was a relation to sinusitis, and for one, the infective focus was not determined.
Results
Six patients with a frontal sinusitis–related intracranial infection were included in the study. Five of these were men and one a woman with a median age of 21 years (range, 11–44 years). The most common presenting complaint was headache (n = 6), followed by fever (n = 5), vomiting (n = 3), nasal congestion (n = 3), forehead lump (n = 2), and neck stiffness (n = 1). At presentation, all patients had a high C-reactive protein (CRP) level (mean = 141; range; 29–219 mg/L). Both computed tomography (CT) and magnetic resonance imaging (MRI) were used to reveal pan- or frontal sinusitis–associated intracranial complications. Four (67%) patients had an epidural abscess, one (17%) had both an epidural abscess and a subdural empyema, and one (17%) had a subdural empyema. When intracranial suppuration was noted in imaging, five patients did not have neurological deficits, while one presented with dysphasia and hemiplegia. Later, one patient developed unilateral facial nerve palsy, and another developed dysphasia and hemiplegia. All patients were treated operatively. Five patients with frontal sinusitis and intracranial suppuration were initially treated with frontal sinus (Beck’s) trepanation in combination with endoscopic meatal antrostomies (1/5, 20%) and maxillary antral washout (3/5, 60%). Drainage of epidural abscess was done by burr hole (during the sinus operation 1/5 and later 2/5 (40%)) or by craniotomy (during the sinus operation 1/5, later 1/5). The patient with subdural empyema was treated with a burr hole only. The intraoperative samples grew bacteria from either Streptococcus (83%) or Haemophilus (17%) species. Most (83%) patients recovered to premorbid state without neurological sequelae. One patient died intraoperatively. Table 1 shows the data breakdown per patient. The population-based annual incidence of frontal sinusitis-related intracranial complication was 0.3 per million inhabitants.
The data breakdown per patient summarizing presentation and treatment details.
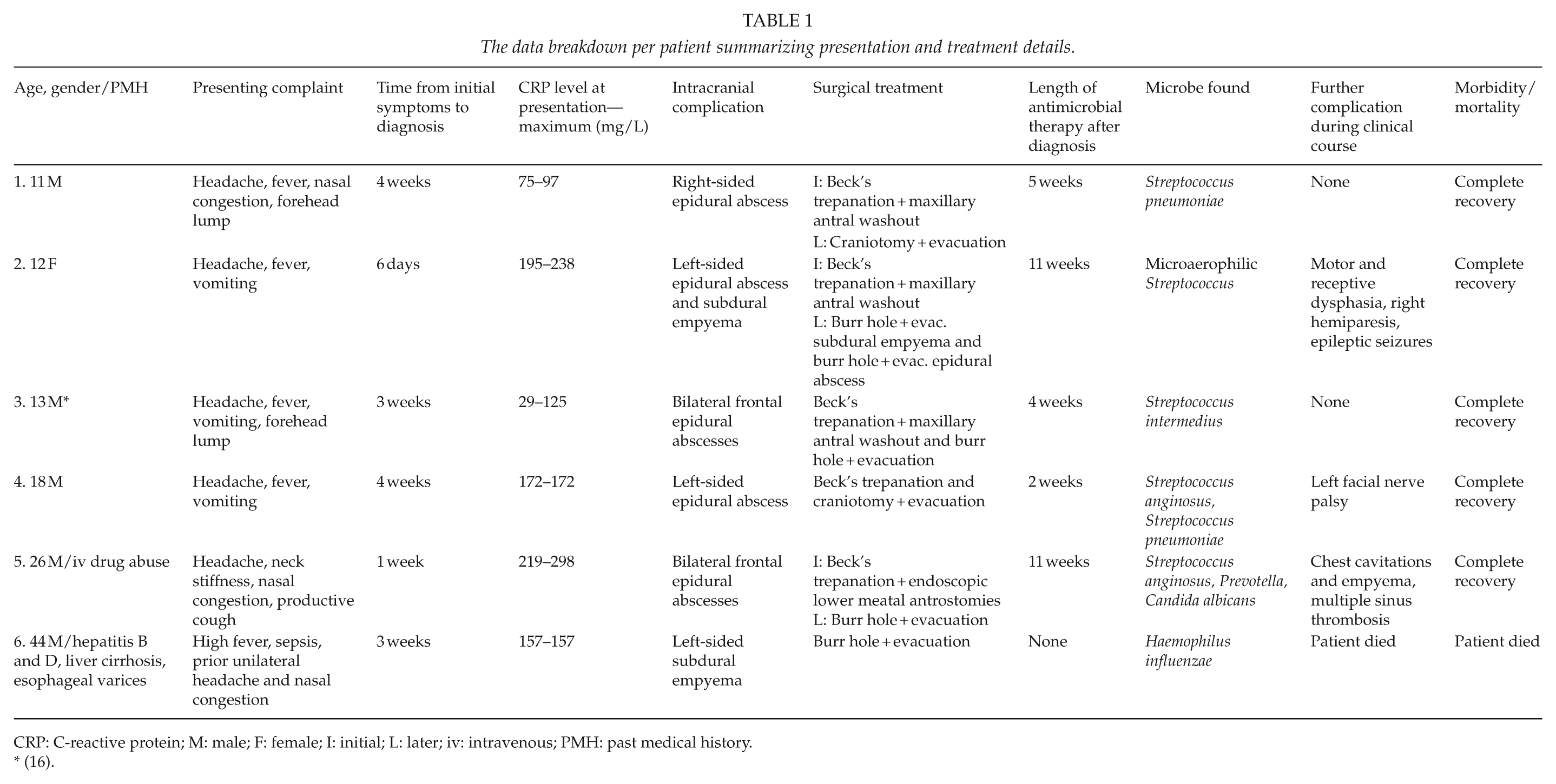
CRP: C-reactive protein; M: male; F: female; I: initial; L: later; iv: intravenous; PMH: past medical history.
(16).
Case Studies
Patient 1
A previously healthy 11-year-old boy presented to the emergency department with a 4-week history of nasal congestion, 1-week history of nasal discharge, and a 2-day history of high fever and headache. Earlier on the presentation day, a midline forehead swelling had been noted. On examination, this lump was small, tender, and erythematous. A CT scan showed unilateral maxillary, ethmoid, and frontal sinusitis. A small air-collection was seen behind the frontal sinus, but there was no definite perforation of the posterior wall of the frontal sinus or intracranial abscess (Fig. 1). His CRP level was 75 mg/L and white blood cell (WBC) count 14.5 E9/L. He was admitted to the hospital for intravenous (iv) cefuroxime (1.5 g three times a day (TDS)), metronidazole (500 mg TDS) and paracetamol (750 mg four times a day (QDS)). A nasal decongestant was also started (triprolidine + pseudoephedrine). A lumbar puncture, bilateral maxillary antral washouts, and left-sided frontal sinus trepanation (Beck’s) were performed and pus cultured. A catheter was kept in the frontal sinus for drainage and irrigation for 4 days. On the second post-operative day, the patient became increasingly somnolent. An MRI was carried out showing small frontal, bilateral epidural abscesses (8 mm thick (T) × 17 mm wide (W)). Cultures grew Streptococcus pneumonia, but the cerebrospinal fluid (CSF) was clear. The patient improved and was discharged 5 days post-admission with oral amoxicillin (500 mg TDS) and clindamycin (300 mg TDS).
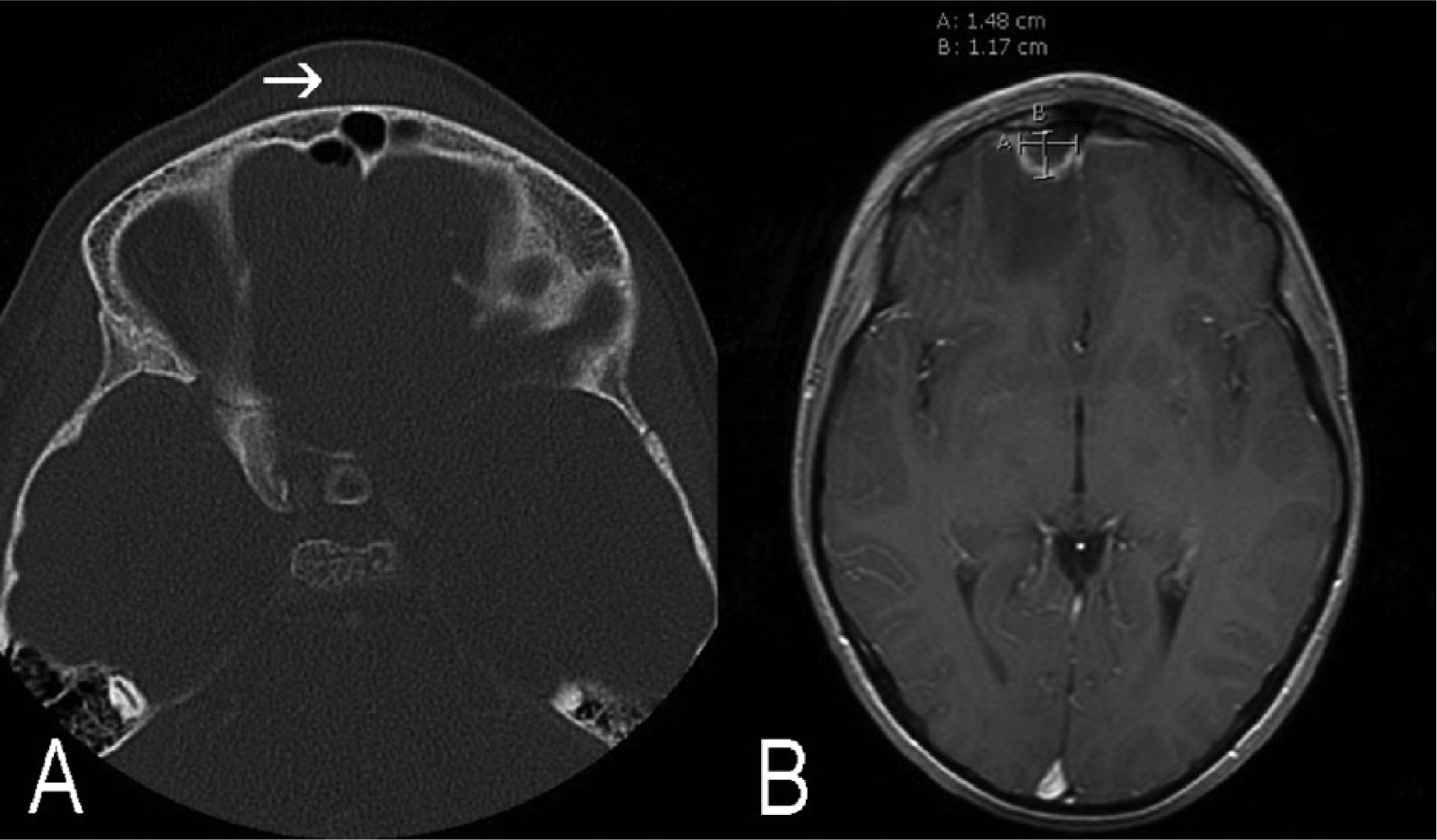
On the left (A), an axial CT scan shows a PPT (arrow) and air behind the frontal sinus but no perforation of the posterior wall of the sinus or osteomyelitis. On the right (B), an axial T1 weighted MRI with contrast, taken 12 days later, highlights a frontal 15 mm (W) × 12 mm (T) epidural abscess in the right frontal lobe surrounded by significant oedema.
In the 1-week follow-up, the patient reported no headache or other complaints. The CRP level was 5 mg/L and the WBC count 9.3 E9/L. However, the MRI showed a slightly enlarged epidural abscess (12 mm T) on the right side with significant edema in the frontal lobe, while the left-sided abscess had been resolved (Fig. 1). Iv antibiotic therapy (ceftriaxone and clindamycin) recommenced. A right-sided frontal craniotomy and evacuation of the epidural abscess were performed. No perforation was found in the posterior wall of the frontal sinus, but the wall was nevertheless covered with a piece of temporal muscle, fascia, and fibrin clue. Due to antimicrobial therapy, there was no forehead lump or osteomyelitis of the frontal bone to take care of. After an uneventful 4-day recovery, the patient was discharged on oral clindamycin (300 mg TDS). In the follow-up 33 days after primary admission, the repeat MRI showed no PPT or abscess. The patient remained neurologically intact, and antibiotics were discontinued.
Patient 2
A 12-year-old previously healthy girl presented with a 6-day history of high fever, frontal headache, and vomiting. On clinical examination, she was irritable and in pain. After a lumbar puncture, a complete motor and partial receptive dysphasia occurred. Her CRP level was 195 mg/L and WBC count of CSF 111 E9/L; based on a working diagnosis of meningitis, she was started on iv dexamethasone and benzylpenicillin. A head MRI was ordered which showed left-sided maxillary and frontal sinusitis, left-sided frontal epidural abscess (13 mm × 13 mm), 3 mm thick subdural empyema around the left hemisphere, and wide leptomeningeal enhancement. The antibiotics were thence changed to ceftriaxone (2 g once a day (OD)) and metronidazole (500 mg TDS). Immediate left-sided maxillary antral washout and Beck’s trepanation were performed, and frontal catheter was left for drainage and irrigation for 4 days.
Nevertheless, during the following 12 h, the patient’s dysphasia did not improve and she developed partial right hemiparesis. A control MRI showed enlarged frontal epidural abscess as well as increased thickness of the subdural empyema (7 mm) with a 1- to2-mm midline shift (Fig. 2). A temporal burr hole and evacuation of the subdural empyema were carried out, as well as a re-washout of the left maxillary sinus. Two days later, she had epileptic seizures for which phenytoin (300 mg twice a day (BD)) and dexamethasone (4 mg TDS) were started. Aphasia and right-sided hemiparesis re-occurred. Epidural abscess was still unchanged in MRI, and thus, a frontal left-sided burr hole evacuation and re-washout of the maxillary sinus were carried out. Pus cultures revealed microaerophilic Streptococcus, but CSF did not grow any bacteria. She was discharged on day 12 post-admission on a 2-month course of oral doxycycline (150 mg OD), while phenytoin (75 mg morning, 100 mg evening) and hydrocortisone (7.5 mg morning, 5 mg evening) continued for 2 weeks post-discharge. The right-sided hemiparesis had resolved by the 4-week follow-up appointment. The ensuing speech therapy continued for altogether 5 months after which also her speech had improved to a normal level.
An axial T1 weighted MRI with contrast showing a large left-sided frontal epidural abscess and left-sided subdural empyema with a 1–2 mm midline shift.
Patient 3
A 13-year-old normally healthy boy presented to an emergency otorhinolaryngology clinic with a 3-week history of headache, fever, vomiting, and an enlarging forehead lump. He had been managed with amoxicillin (750 mg BD) in the primary care setting a week earlier based on the radiological diagnosis of maxillary sinusitis and elevated CRP (114 mg/L) but no clear symptoms of sinusitis. On admission, the only finding was a 3 × 3 cm non-tender, non-erythematous swelling on the upper part of his forehead. His CRP level was 29 mg/L and WBC count 11.9 E9/L. A consequently performed maxillary sinus lavage produced yellow, purulent discharge. Ultrasound (US) and CT scans revealed a subperiosteal fluid collection (4 mm T × 30 mm W) as mark of a PPT on top of the frontal bone, with two very small bony erosions in the posterior wall of the frontal sinus. Subsequent MRI highlighted a large (30 mm T × 80 mm W) frontal, mainly right-sided, epidural abscess compressing the frontal lobe and frontal part of the superior sagittal sinus. Figures have been published earlier (16). Iv metronidazole (500 mg TDS) and cefuroxime (750 mg TDS) as well as decongestant nasal drops (xylometazoline) were started. The epidural abscess was evacuated through a right-sided frontal burr hole, where an epidural drainage was left in situ for 1 day. During the same operation, the left frontal sinus was drained through an external Beck’s trepanation. A post-operative CT scan showed no residual epidural abscess, subperiosteal swelling, osteomyelitis, or brain edema. Cultures from the frontal sinus grew Streptococcus intermedius. He was discharged neurologically intact 5 days after admission on iv ceftriaxone (2 g OD) and per oral metronidazole (400 mg TDS) that continued for three more weeks. The patient remained well at the 4-month follow-up.
Patient 4
A normally fit and well 18-year-old man was transferred to the emergency department with a 2-day history of frontal headache, fever, and vomiting. On presentation, his CRP level was 172 mg/L, his blood cultures grew Streptococcus anginosus while the CSF showed an elevated amount of WBCs but failed to grow bacteria. With a working diagnosis of bacterial meningitis, dexamethasone and ceftriaxone (both iv) were started. Echocardiogram showed normal heart and valvular function. A dental review and consecutive orthopantogram (OPG) revealed no dental abscess or infection. The antibiotics continued for 2 weeks after which he remained well until his headache and fever started again 1 week later. Iv ceftriaxone was re-started. After he developed left facial nerve palsy on the second in-patient day, a head CT and MRI scans were organized revealing a large left-sided frontal sinusitis–associated epidural abscess (50 mm W × 21 mm T). The ceftriaxone dose was doubled (2 g BD) and metronidazole added to the regimen (500 mg TDS).
A small left-sided frontal craniotomy and Beck’s trepanation were performed by a neurosurgeon to evacuate the epidural abscess and to drain the frontal sinus. There was a tiny perforation in the posterior wall of the frontal sinus. The bacterial cultures grew Streptococcus pneumonia. A CT scan, performed on the third post-operative day, revealed no residual abscess. He was discharged on the fourth post-operative day on a 10-day course of oral metronidazole (500 mg TDS) and cephalexine (500 mg TDS) and a week’s course of methylprednisolone (32 mg OD). At the 2-month follow-up, the patient’s CT scan remained normal and he was neurologically intact with normal facial nerve function.
Patient 5
A 26-year-old man presented with a 1-week history of productive cough, nasal congestion, neck stiffness, and high fever. He had a long history of iv drug abuse and was at the time on buprenorphine (24 mg) and varied doses of benzodiazepines. Echocardiogram of his heart was normal. Laboratory tests revealed a CRP level of 219 mg/L and a WBC count of 33.7 E9/L, while CSF and blood cultures revealed no systemic infection. Chest and sinus CT scans as well as a head MRI scan were performed showing varied size chest cavitations resembling Staphylococcus infection as well as pansinusitis and bilateral frontal epidural abscesses, respectively. Endoscopic inferior meatal antrostomies and Beck’s bilateral trepanation were carried out on the day of presentation. Drainage and irrigation of the frontal sinus continued for 10 days. In the post-operative MR venography, a multiple sinus thrombosis (superior sagittal and bilaterally in the transversal, sigmoid, and internal jugular veins) was seen and patient started on iv low-molecular-weight heparin (dalteparin). The initially commenced iv cefuroxime was first changed to ceftriaxone, then to ertapenem, and further on to iv meropenem (1 g TDS). An OPG revealed Class III caries throughout, periodontitis, as well as several periapical abscesses, suggesting a likely concurrent dental infection focus. After all his teeth were extracted and, subsequently, Candida albicans sepsis discovered, both iv levofloxacin (500 mg OD) and fluconazole (400 mg OD) were added to the treatment.
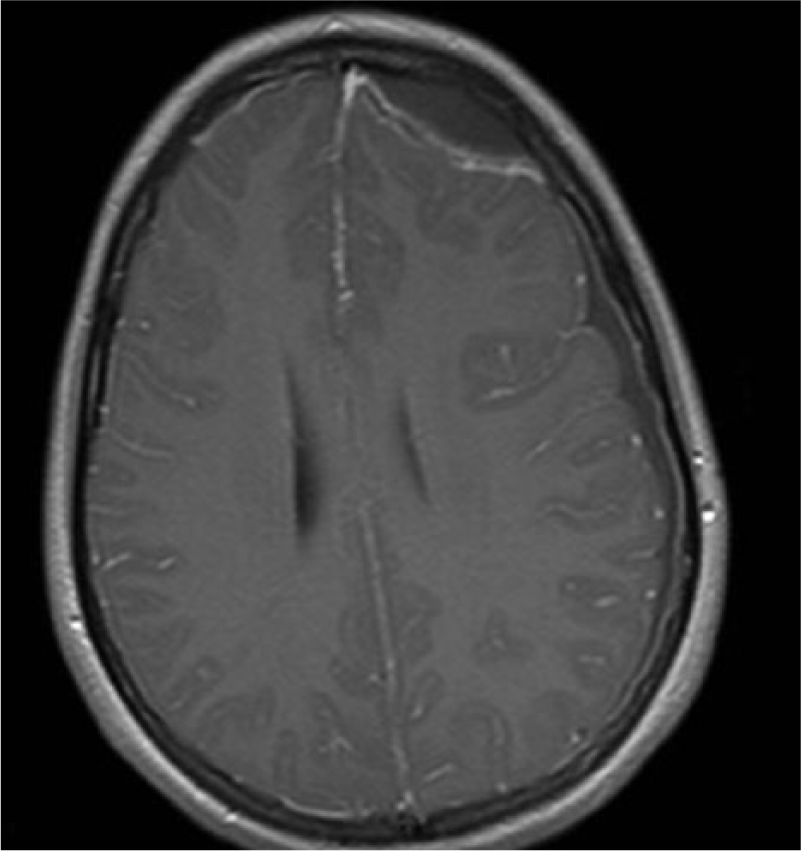
In the control MRI on day 23, after the initial presentation the bilateral frontal epidural abscesses had enlarged particularly concerning the interhemispheric amount (Fig. 3). Frontal midline burr hole and evacuation of the enlarged bifrontal epidural abscesses followed. The ensuing in-patient period went well, and the patient was discharged home 5 weeks after the initial presentation. At the 1-month follow-up, the patient remained well and the control CT scan did not reveal venous infarction or other complication. The patient failed to attend his 6-month follow-up appointment.
A sagittal T1 weighted MRI with contrast highlighting large bifrontal epidural abscesses compressing the superior sagittal sinus.
Patient 6
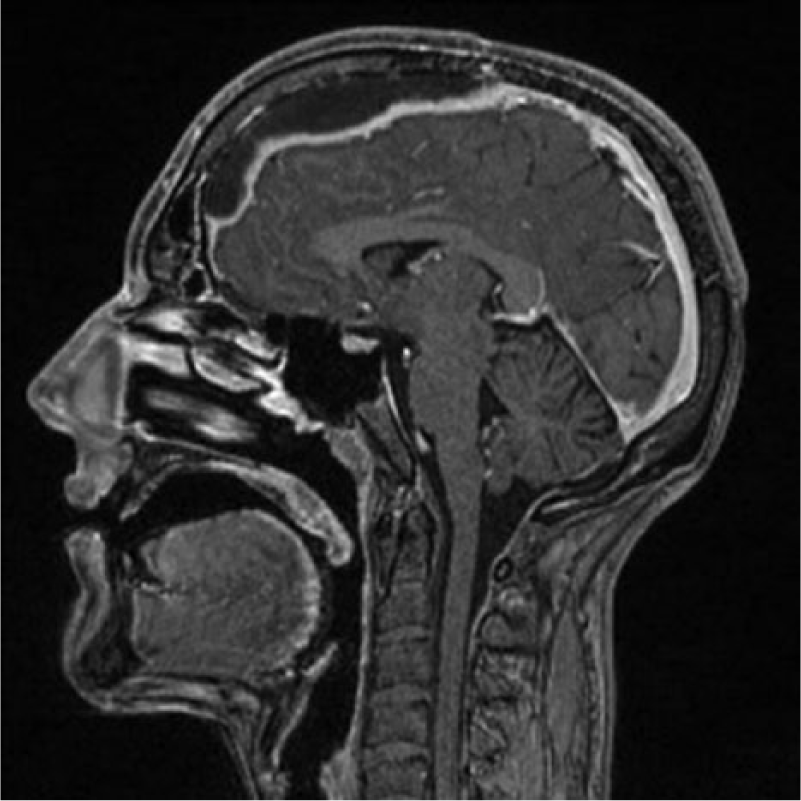
A 44-year-old man with a history of Hepatitis B and D, liver cirrhosis, and esophageal varices was found lying on the floor. He previously had nasal congestion for 4 weeks and headache for 2 weeks. For these, a nasal spray (beclometasone dipropionate) and oral desloratadine–pseudoephedrine had been prescribed in the primary care setting. Follow-up should have been on the same day when he was found on the floor. A CT scan revealed a left-sided subdural hematoma or empyema (5 mm T) with a 3-mm midline shift (Fig. 4). On admission to the emergency room, he was conscious but barely able to follow commands. He had right hemiparesis and was unable to speak. The initial blood pressure was 80/60 mmHg, pulse 100/min, and body temperature +39.5 °C. His CRP level was 157 mg/L. The chest X-ray showed no abnormalities, and electrocardiogram (ECG) showed normal sinus rhythm with no ST changes. Iv ceftriaxone (2 g BD) and vancomycin (1 g BD) were started. Because of his poor coagulation profile, he received vitamin K (5 mg iv) and 12 units of thrombocytes and was taken immediately to an operating room with a suspected subdural empyema. Just before the operation was started, the patient had a sudden cardiac arrest. With cardiopulmonary resuscitation (CPR), including defibrillation, intubation, and adrenaline boluses, ventricular tachycardia was seen to return. The operation commenced and thick, green mucous exudate was seen to ooze out through the left-sided burr hole after opening the dura. While closing the wound, the patient had another cardiac arrest. CPR including adrenaline boluses and infusion did not return his heartbeat. The cultures grew Haemophilus influenzae. A medico-legal autopsy was performed which determined the immediate reason for death to be Haemophilus influenzae infection in subdural and subarachnoidal abscesses and meningitis.
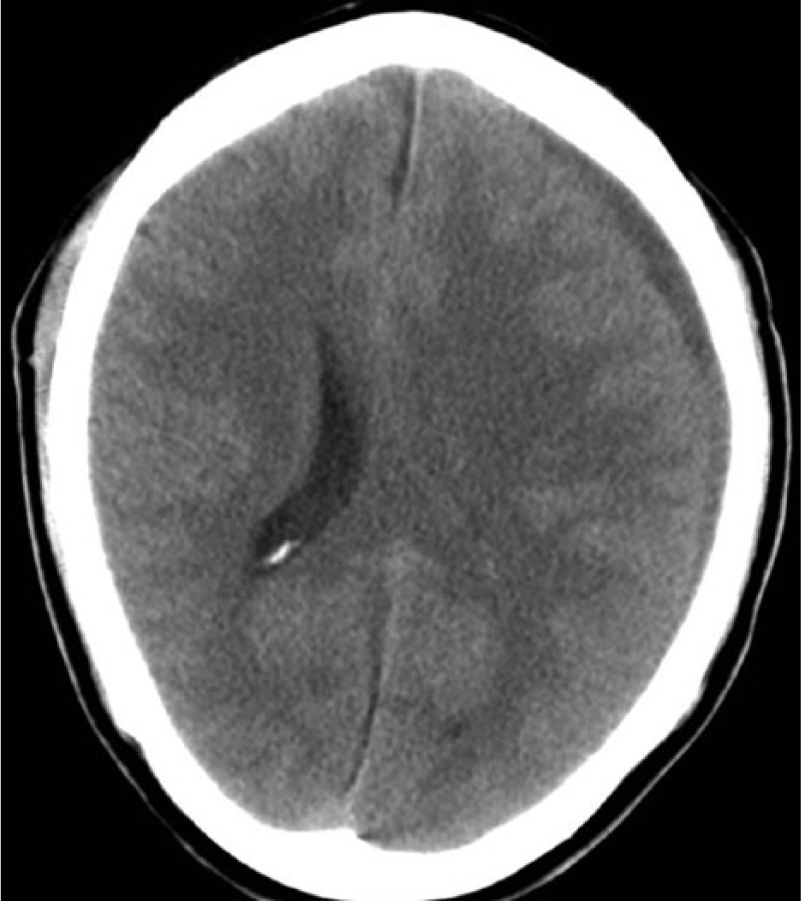
An axial CT scan showing a left-sided subdural empyema (5 mm) and midline shift (3 mm).
Discussion
We report a series of six patients diagnosed and treated for sinogenic intracranial suppuration at our institution within a 10-year period. Based on our findings, patients with a sinusitis-related intracranial complication most commonly present with signs of raised intracranial pressure rather than signs of sinusitis. The initial neurological examination may be normal and the inflammatory markers surprisingly low, particularly if the patient has been on antibiotics. All our patients needed neurosurgical evacuation of the intracranial abscess. While infection in the other sinuses was also seen, frontal sinusitis was always associated with an intracranial complication in the series. Our findings support the male predominance noted in earlier publications. We are unaware of any other studies reporting the incidence of sinogenic intracranial suppurative complications per population.
The largest case series of sinusitis-related epidural abscess and subdural empyema has been reported out of Africa. This may be a reflection of a greater burden of disease due to lack of early antibiotic treatment and consultation possibilities (15). In the United States, the incidence of intracranial suppuration associated with sinusitis or otitis has been estimated to be 3–4 per million children per year (17). This and our minuscule incidence of 0.3 per million explain why no precise guidelines exist on how to treat sinogenic intracranial infections. Geography-dependent seasonal pattern has been described earlier in sinogenic but not in otogenic cases (17). Pediatric cases of complicated sinusitis peak in March in Central Europe and in winter in the United States (18, 19). Four of our six patients (68%) had complicated sinusitis during winter (December–March).
Most patients presented with Streptococcus pneumoniae, intermedius, or anginosus, while one presented with Haemophilus influenzae. Patient 5 additionally harbored Prevotella and Candida species, which were assumed to originate from a concurrent dental infection. This is in line with earlier studies. The most common isolates of sinogenic intracranial infection have been reported to be both monomicrobial and polymicrobial with Streptococcal and Staphylococcal species being the main culprits (1, 7, 8). Interestingly, Brook (20) has demonstrated that anaerobic organisms such as Prevotella and Peptostreptococcus are more frequently cultured in chronic frontal sinusitis, whereas Haemophilus influenza and Streptococcus pneumonia often underlie acute frontal sinusitis. As patients in our study presented with acute sinusitis only, no differentiation could be made between acute or chronic infection causative pathogens.
When an intracranial suppuration is suspected, a CT scan of the sinuses combined with an MRI scan of the brain is the recommended imaging modality (2, 6). CT is sufficient for most cases, especially in preparation for urgent neurosurgical procedures. It is known that CT demonstrates the osseous pathology in calvaria, bones, and facial sinuses better than MRI. On the other hand, CT has poorer image clarity and lower sensitivity. In both, the focal biconcave morphology indicates epidural abscess where subdural empyema spreads wider (Fig. 2). Pachy- and leptomeningeal contrast enhancement may be seen surrounding the collection. MR venography and diffusion-weighted imaging may be useful in detecting sinus thrombosis and ischemic injury adjacent to suppurative collections. Frequent brain imaging is crucial for monitoring response to antimicrobial therapy. In our patient cohort, chest and abdominal X-ray/CT as well as abdominal and forehead US scans were also initially utilized to look for focus of infection when the presenting symptoms were vague or the clinical status of the patient unusually good.
The primary treatment of intracranial suppurative complications of sinusitis is antimicrobial (21). Small epidural collections and brain abscesses with a diameter smaller than 2 cm may be managed non-operatively. In fact, one-fourth of sinogenic and otogenic intracranial infections in a children’s cohort study did not need an operation (17). The indication for neurosurgical intervention is either to relieve symptomatic intracranial mass effect or to sample collection for achieving a microbiological diagnosis. Up to 65% of intracranial pus samples lead to positive cultures (2, 7). Patients in this study received several different antibiotics based on the local antimicrobial agent guidelines and an occasionally wrong initial diagnosis. It is common for patients to be on antibiotic therapy when the subperiosteal and/or epidural abscesses develop (7). The continued development of the abscess can be due to misdiagnosis or lack of adequate local therapy. If there is strong clinical suspicion of an underlying frontal sinusitis and/or its related complication, antimicrobial agents should be started without delay after bacterial cultures have been obtained (if possible). Without evidence from controlled treatment trials, an advanced generation cephalosporin (e.g. ceftriaxone) along with an antianaerobic agent (e.g. metronidazole) has been proposed to be a sufficient combination (2, 8, 22). When methicillin-resistant Staphylococcus aureus has been isolated, vancomycin should be added to the regime. The antimicrobial therapy should be given for 4–8 weeks (2, 7). The role of corticosteroids remains controversial. Corticosteroids should be avoided unless the patient exhibits signs of meningitis or imaging (CT or MRI) demonstrates visible epidural/subdural infection—induced mass effect with the resulting risk of acute brain herniation. Corticosteroids effectively reduce cerebral edema and retard the encapsulation process. They also reduce antibiotic penetration into the abscess and increase both necrosis and risk of ventricular rupture (23, 24), which is why they are not recommended for the treatment of intraparenchymal brain abscesses. Without well-controlled randomized clinical trials to guide dosing and length of treatment, corticosteroids should generally be used for a short duration only.
Patients with intracranial suppurative complications of sinogenic origin commonly end up eventually needing sinus surgery. There are no consensus guidelines for the type or timing of operation. In our series, Beck’s trepanation—even in combination with either maxillary antral washout or lower meatal antrostomies—was not a potent enough procedure to resolve a sinogenic epidural abscess. Not even when a catheter was left in the frontal sinus for repeated drainage and irrigation. Thus, a multidisciplinary management by a neurosurgeon and an otorhinolaryngologist is necessary. This combined approach may take place concurrently or at different times. It may be argued that immediate neurosurgical involvement could reduce patients’ in-patient stay, lessen the need for further surgery, and, more importantly, improve patients’ prognosis. In agreement with a previous study, we advocate the drainage of both the source of infection and the intracranial suppuration in combination with antibiotic therapy to limit morbidity, mortality, and incidence of recurrence (25).
There are also no consensus guidelines regarding the recommended neurosurgical technique in the treatment of sinusitis-related intracranial suppuration. Our series did not have any brain abscesses. Leaving them out of the treatment options, the most important question is whether to perform a burr hole or a craniotomy. Burr hole drainage often suffices for an epidural abscess, but it has been reported to associate with increased recurrence when used to drain subdural empyemas (26). In our study, burr hole drainage was performed for the two subdural empyemas and two epidural abscesses, and craniotomy for two epidural abscesses without subsequent abscess recurrences.
If the frontal bone has necrotized as a result of osteomyelitis, an evacuation of infected areas including subperiosteal abscess, osteomyelitic bone, epidural abscess, and granular tissue is recommended. Furthermore, removal and exploration of the posterior wall of the frontal sinus are paramount if a cranialization procedure is attempted (3, 27). When evacuating granular tissue from the dura, caution must be taken to avoid dural tear and introduction of infection into the subdural space. The mortality rate is 30% in patients with subdural empyema (28), while isolated epidural abscesses can be treated without mortality (26). On the other hand, craniectomy of the frontal bone may have cosmetic consequences and is nowadays considered unnecessary since eroded frontal bone has the potential to heal with 6–8 weeks’ antibiotic therapy. In this study, two patients had a small PPT. In their operations, no osteomyelitic bone was noted or bone removed, nor was a cranialization procedure done. Instead, a piece of temporal muscle was used to cover the posterior wall of the sinus for one patient. In all intracranial complications of sinusitis, especially when a subdural empyema is found, an expedited neurosurgical consultation is paramount.
With reports mainly limited to treatment of chronic rhinosinusitis, the use of balloon sinuplasty is another treatment for complicated frontal sinus obstruction. Roland et al. describe a case where balloon frontal sinuplasty successfully treated an intracranial abscess of sinogenic origin in a 12-year-old patient (29). In a recent multicenter study, office-based multisinus balloon dilation was described as “safe, effective, and well tolerated” in the treatment of adults diagnosed with chronic or recurrent acute rhinosinusitis (30). The benefits of balloon sinuplasty include achievement of long-term patency of the outflow track and thereby effective clearance and irrigation of purulent secretions. While the results of balloon sinuplasty appear promising, long-term outcome data are needed to confirm its efficacy in the treatment of complicated acute frontal sinusitis.
The present series highlights the important clinical finding that patients with a sinusitis-related epidural abscess or subdural empyema typically present with signs of raised intracranial pressure rather than signs of sinusitis. Most are likely to need neurosurgical evacuation of the abscess without delay. Although their population-based incidence is remarkably low, sinogenic intracranial suppurative complications do occur and should be included in the differential diagnosis of relevant patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.