
Abstract
Background and aims:
Diagnostic performance of patellar position for patellar cartilage lesions remains unclear. The aim of this study was to assess the abnormal patella height and its correlation with chondral lesions of the patellofemoral joint in China.
Material and methods:
A total of 1703 consecutive patients who performed knee joint examination using an extremity-dedicated low-field magnetic resonance imaging were enrolled in this study. Patellar cartilage lesions were diagnosed based on the result of magnetic resonance imaging and clinical data. Patella height was defined as the ratio of patellar tendon length to patellar length according to Insall-Salvati index. Patella alta and infera were defined as tendon length/patellar length >1.2 and <0.8, respectively.
Results:
The total prevalence of patellar cartilage lesions was 38.0%. The prevalence in females was significantly higher than that in males (46.4% vs 28.8%, p < 0.001). Age notably increased the incidence of patellar cartilage lesions (p < 0.001). Logistic regression analysis showed that tendon length/patellar length ratio was significantly correlated with patellar cartilage lesions (odds ratio = 6.380, p < 0.001). Furthermore, patients with cartilage lesions showed significantly higher rates of patella alta and infera (p < 0.001). In addition, receiver operating characteristic curve analysis demonstrated that abnormal patella height had statistical significance in diagnosing cartilage lesions (p < 0.001). However, the area under the curve (0.596; 95% confidence interval: 0.568–0.624) and sensitivity (47.0%) were relatively low, while the specificity was 72.2%.
Conclusions:
Patients with patellar cartilage lesions have an increased tendon length/patellar length ratio. The abnormal patella height is significantly correlated with chondral lesions and can be used as a potential diagnostic marker.
Keywords
Introduction
Anterior knee pain is a common disorder of human beings with symptoms including deep-seated ache and retropatellar pain perceived in the anterior region of the knee (1). The anterior knee pain can be caused by chondral lesions of the patellofemoral joint due to trauma, osteochondritis dissecans, osteoarthritis, and chondromalacia patellae (CP) (2, 3). CP is defined as softening, fissuring, and fragmentation of the undersurface of the patella (4), as well as erosion of the cartilage to the subchondral bone in severe cases (5). As mild CP is often neglected, patients with CP are predisposed to osteoarthritis, a degenerative joint disease that is caused by breakdown of joint cartilage and the underlying bone. In elderly people, however, age-related osteoarthritis of the knee may lead to CP (6).
CP is the consequence of multiple factors including trauma to the knee, vascular insufficiency within the subchondral bone (5, 7), and misalignment of the extensor mechanism of the knee which could be caused by patella alta and infera, genu valgum, external tibial torsion, increased quadriceps (Q) angle, and deformities of the femoral condyle (8, 9). In order to investigate the etiology of CP and provide the theory basics for the early diagnosis and treatment of CP, some studies have evaluated the association of morphological features of the patellofemoral joint, such as lateral patellar tilt angle (LPTA), sulcus angle, trochlear depth, patella angle, lateral and medial patellar facet lengths, lateral-to-medial facet length ratio, interfacet angle, and anterior margin of the lateral femoral condyle, with CP (5, 10, 11). Also, in patients with patellofemoral joint osteoarthritis, patellar alignment, such as patellar height, sulcus angle and depth, lateral patellar displacement, and LPTA, was associated with cartilage lesions (12, 13).
Furthermore, correlation of patellofemoral geometry or alignment with patellar cartilage defects was also analyzed without regard for etiology (14, 15). Similar investigation was also conducted in China by comparing 111 patients with chronic patellofemoral cartilage lesions and anterior knee pain and 124 cases with isolated meniscus rupture without anterior knee pain (16). In consideration of the ethnic variation or limited sample size in these previous studies, it is necessary to assess the patellofemoral structural parameters and their relationship with cartilage lesions in a large Chinese population. Among the structural disorders, patella alta and patella infera refer to the two kinds of abnormal patellar height which could be directly estimated by the length of the patella and the patellar tendon using magnetic resonance imaging (MRI) (17, 18). Insall-Salvati index (ISI) is independent on the degree of knee flexion angle and consequently reliable for assessing the patellar height, as the ligamentum patellae is not elastic and its length determines the position of the patella (18, 19). Hence, we analyzed the correlation of patellar cartilage lesions with abnormal patellar height and assessed the diagnostic accuracy of patella alta and patella infera in China with a large sample size.
Materials and Methods
Patients
From October 2006 to October 2008, 1703 consecutive patients (916 males and 887 females) who underwent knee joint inspection with MRI equipment in Department of Radiology, Huashan Hospital affiliated to Fudan University and Tongren Hospital affiliated to Shanghai Jiaotong University were recruited in this study. The enrolled patients met the following inclusion criteria: no history of surgery on the knee such as joint replacement and ligament reconstruction before MRI; no history of patellar, femoral, and tibial fractura. These patients were aged from 12 to 89 years (45.46 ± 17.82 years) at the time of MRI examination. The clinical data and results of MRI examination were used for diagnosing patellar cartilage lesions. Patients with patellar cartilage lesions were included in defect group, while those without patellar cartilage lesions were defined as control group. In addition, 16 cases also performed arthroscopy. This study was approved by the Ethics Committees of the two hospitals. In addition, the written informed consent was obtained from each study participant.
MRI Examination
A 0.2T extremity-dedicated MRI system (Artoscan, Esaote, Genoa, Italy) was used to perform MRI at supine position with a knee flexion angle of 30°. The scanning parameters were set as follows: the repetition time (TR) and echo time (TE) of sagittal T1-weighted spin echo, sagittal T2-weighted spin echo, coronal gradient echo-short time inversion recovery (GRE-STIR), axial GRE-STIR, and fat-suppression GRE-STIR were 3000 and 28 ms, 3000 and 90 ms, 740 and 26 ms, 680 and 16 ms, and 1360 and 16 ms, respectively; slice thickness, 5 mm; interslice gap, 5 mm; field of view, 16 cm × 16 cm; matrix, 256 × 192.
Measurement of Patellar Height
The patellar height was defined as ISI (19) using the ratio of patellar tendon length to patellar length (TL/PL). PL was measured from the superior articular margin to the distal anterior tip of the patella, and TL was measured from the distal anterior tip of the patellar to tibial tubercle along the inner margin of the tendon using a clear midsagittal MRI image (18). MRI pictures were analyzed on the Merge eFilm (Milwaukee, Wisconsin, USA) workstation using electronic calipers. The measurements were conducted by a single trained observer who was blinded to the diagnosis results of patellar cartilage lesions. To analyze the interobserver and intraobserver variability, 100 subjects were further randomly selected and their MRI images were re-measured by the observer and a second observer.
Analysis of Patellar Cartilage Lesions
The presence of patellar cartilage lesion was diagnosed by two experienced musculoskeletal radiologists based on the MRI images, including T1-weighted, T2-weighted, axial GRE-STIR, and fat-suppression GRE-STIR images. Discrepancies existed in 9 (0.5%) cases and were resolved by consensus. The lesions were staged according to the classification criteria of Rose et al. (20). Stage 1 indicated focal areas of altered signal intensity, which presented as non-uniform low signal in T1-weighted images and high signal in T2-weighted images and fat-suppression GRE-STIR images. Stage 2 indicated mild irregularity, or thinning cartilage of the articular surface. Stage 3 indicated deep fragmentation, “crabmeat” appearance of cartilage, or substantial thinning. Stage 4 indicated ulceration of cartilage with exposure, or signal intensity alteration of subchondral bone which was revealed by cystic, high-signal areas. Stage I and II were mild lesions, while Stage III and IV were severe lesions.
Statistical Analyses
Continuous variables were expressed as mean ± standard deviation (SD), while categorical variables were expressed as percentage. The intraobserver and interobserver variability were assessed by using interclass and intraclass correlation coefficients (ICCs). The effects of gender and age range on the prevalence of patellar cartilage lesions were analyzed by Pearson chi-square test. The correlations of gender, age, and TL/PL ratio with the prevalence of patellar cartilage lesions were detected by using univariate and multivariate logistic regression analyses. According to the previous studies (18, 19), TL/PL > 1.2 was defined as patella alta and TL/PL < 0.8 as patella infera. The TL/PL ratio and abnormal patella height (patella alta and infera) between patients with and without patellar cartilage lesions were compared using t-test and Pearson chi-square test, respectively. The diagnostic value of patella height was assessed by using receiver operating characteristic curve (ROC) analysis. All statistical analyses in this study were performed using STATA 12.0 (Stata Corp, College station, TX) and SPSS 19.0 (IBM, Armonk, New York). Value with p < 0.05 was considered as significant difference.
Results
Prevalence Rate of CP
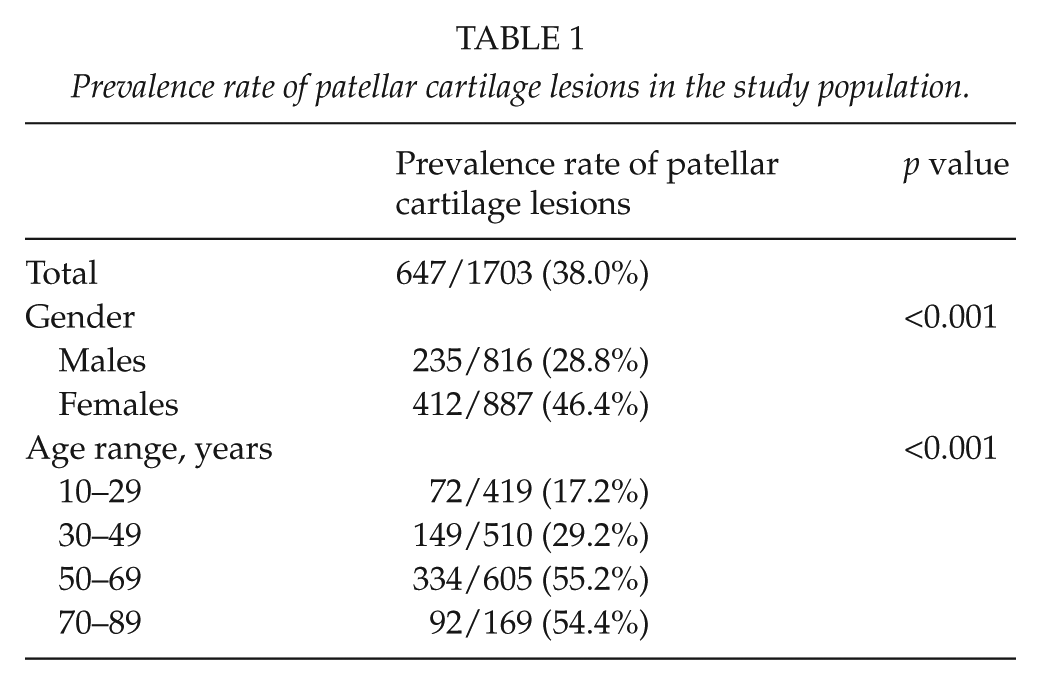
A total of 1703 patients (816 males and 887 females) met the inclusion criteria in this study. The median age of the patients was 46 years (ranged from 12 to 89 years). Patellar cartilage lesions were detected in 647 patients (38.0%), including 235 males and 412 females (Table 1). The prevalence rate in females was significantly higher than that in males (46.4% vs 28.8%, p < 0.001) (Table 1). The prevalence rates of patellar cartilage lesions in patients aged from 10 to 29, 30 to 49, 50 to 69, and 70 to 89 years were 17.2%, 29.2%, 55.2%, and 54.4% (p < 0.001) (Table 1), respectively, suggesting that age markedly affected the occurrence of patellar cartilage lesions.
Prevalence rate of patellar cartilage lesions in the study population.
Intraobserver and Interobserver Reliability for Tl/Pl Ratio
According to the results of ICC analyses, the interclass correlation coefficients and ICCs were 0.939 (95% confidence interval (CI) = 0.911–0.959; p < 0.001) and 0.966 (95% CI = 0.951–0.977; p < 0.001), which demonstrated high interobserver and intraobserver reliabilities.
Associations of Gender, Age and Tl/Pl Ratio with Patellar Cartilage Lesions
To further analyze the influence of gender, age, and TL/PL ratio on the occurrence of patellar cartilage lesions, both univariate and multivariate logistic regression analyses were conducted. According to the results of univariate analysis, gender was significantly correlated with patellar cartilage lesions (odds ratio (OR) = 2.144; p < 0.001, Table 2) when using male as reference category, suggesting that females were more subjected to patellar cartilage lesions. Notable correlations were also found between age and patellar cartilage lesions (OR = 1.042; p < 0.001) as well as TL/PL ratio and patellar cartilage lesions (OR = 6.380; p < 0.001), which demonstrated that people with higher age or TL/PL ratio had more risk for the occurrence of patellar cartilage lesions. In addition, multivariate analysis showed that gender (OR = 1.297; p = 0.023), age (OR = 1.046; p < 0.001), and TL/PL ratio (OR = 12.455; p < 0.001) were independent risk factors for patellar cartilage lesions (Table 3).
Univariate logistic regression analysis for occurrence of patellar cartilage lesions.
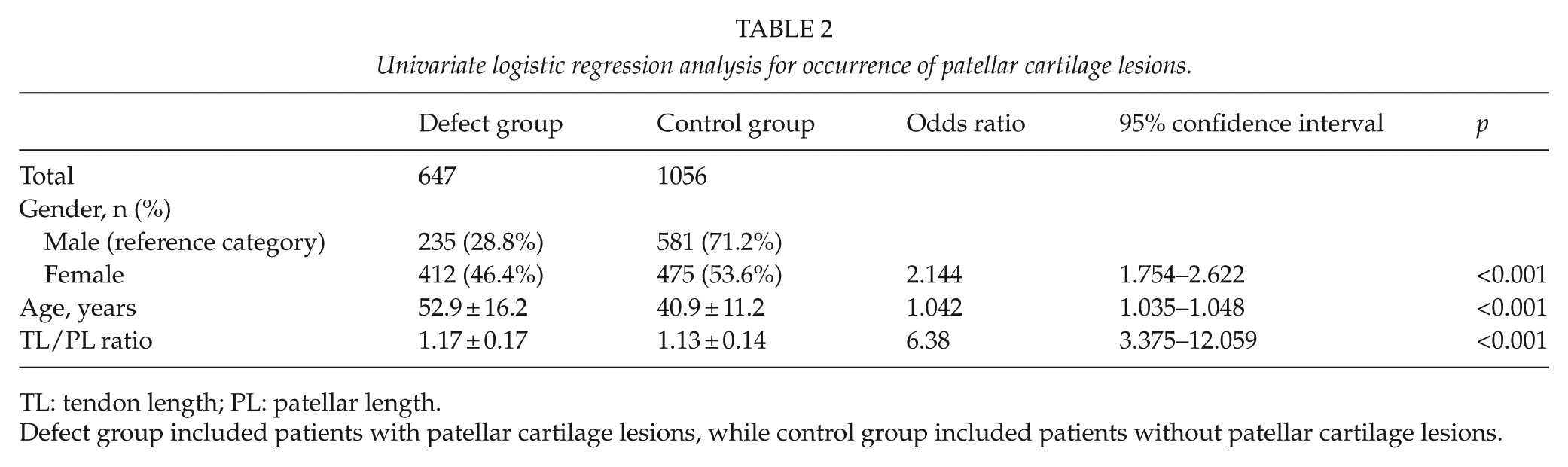
TL: tendon length; PL: patellar length.
Defect group included patients with patellar cartilage lesions, while control group included patients without patellar cartilage lesions.
Multivariate logistic regression analysis for occurrence of patellar cartilage lesions.
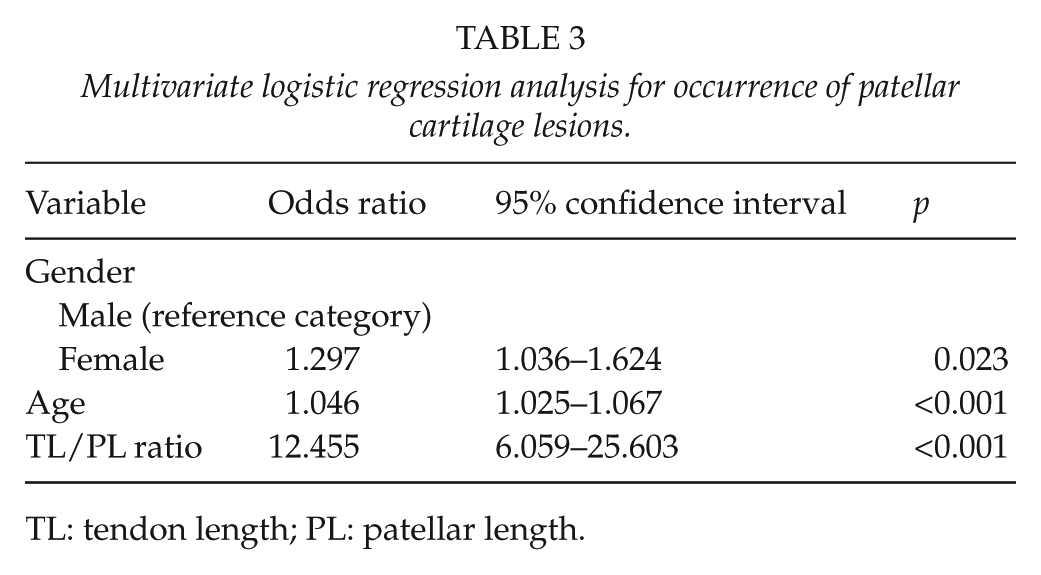
TL: tendon length; PL: patellar length.
Effects of Gender and Age on Tl/Pl Between Patients with and without Patellar Cartilage Lesions
The ratio of TL/PL in the defect group was 1.17 ± 0.17, which was significantly higher than that in the control group (1.13 ± 0.14) (p < 0.001) (Table 2). The effects of gender and age on TL/PL were also evaluated (Table 4). For male patients, the value of TL/PL was slightly higher in patients with patellar cartilage lesions (1.13 ± 0.18) than that in patients without patellar cartilage lesions (1.11 ± 0.15), but the difference was not statistically significant (p = 0.057). However, the female patients with patellar cartilage lesions had a notably higher level of TL/PL compared with those without patellar cartilage lesions (1.20 ± 0.16 vs 1.16 ± 0.14, p < 0.001). There was significant difference in the ratio of TL/PL between patients in the defect and control group aged from 10 to 29 (1.25 ± 0.20 vs 1.16 ± 0.16), 30 to 49 (1.18 ± 0.17 vs 1.12 ± 0.14), and 50 to 69 years (1.17 ± 0.16 vs 1.11 ± 0.12) (p < 0.001), while patients aged from 70 to 89 years showed similar levels of TL/PL (1.14 ± 0.18 vs 1.11 ± 0.13, p = 0.2973).
The ratio of TL/PL in patients with and without patellar cartilage lesions.
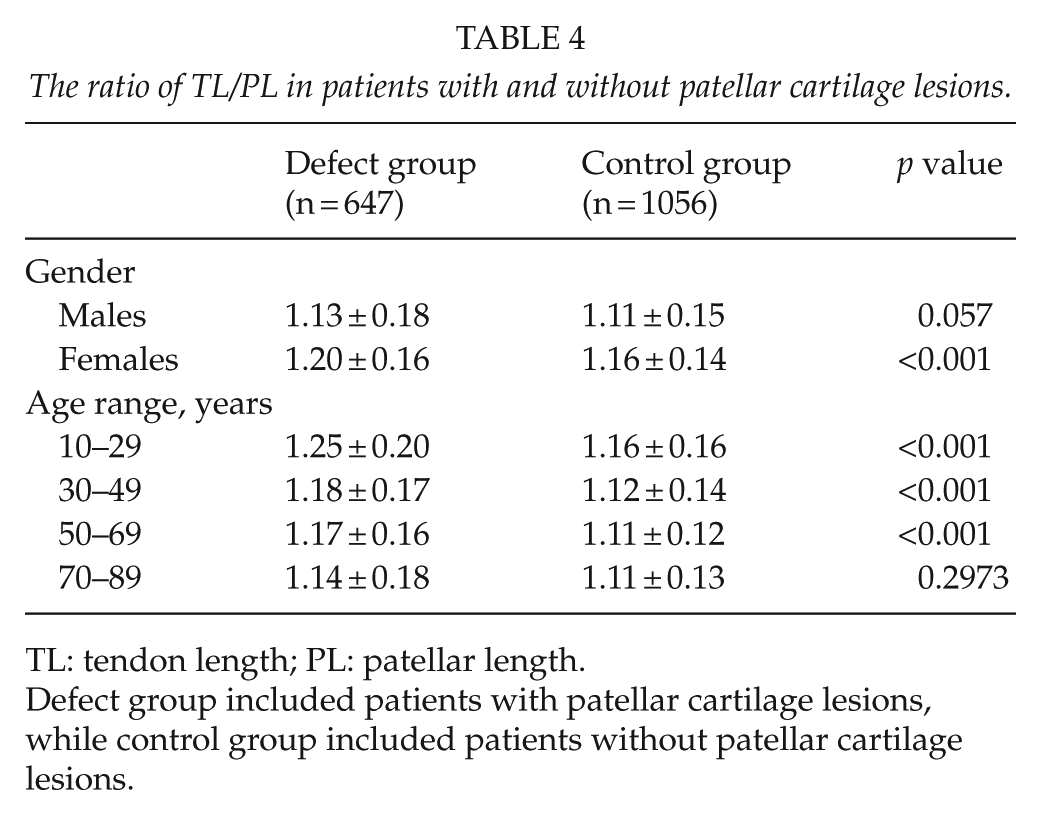
TL: tendon length; PL: patellar length.
Defect group included patients with patellar cartilage lesions, while control group included patients without patellar cartilage lesions.
Comparison of the Patella Height in Patients with and without Patellar Cartilage Lesions
A total of 598 abnormal patellae were detected, including 587 patella alta and 11 patella infera (Table 5). In the defect group, 297 (45.9%) patients were patella alta and 7 (1.1%) had patella infera, while 290 (27.5%) had patella alta and 4 (0.4%) had patella infera in the control group. Patients with patellar cartilage lesions showed significantly higher rate of patella alta and infera (p < 0.001). Similar results were observed in male (p < 0.001) and female (p < 0.001) patients, as well as in patients aged from 10 to 29 (p < 0.001), 30 to 49 (p < 0.001), 50 to 69 (p < 0.001), and 70 to 89 (p = 0.007) years.
Comparison of patella height in patients with and without patellar cartilage lesions.
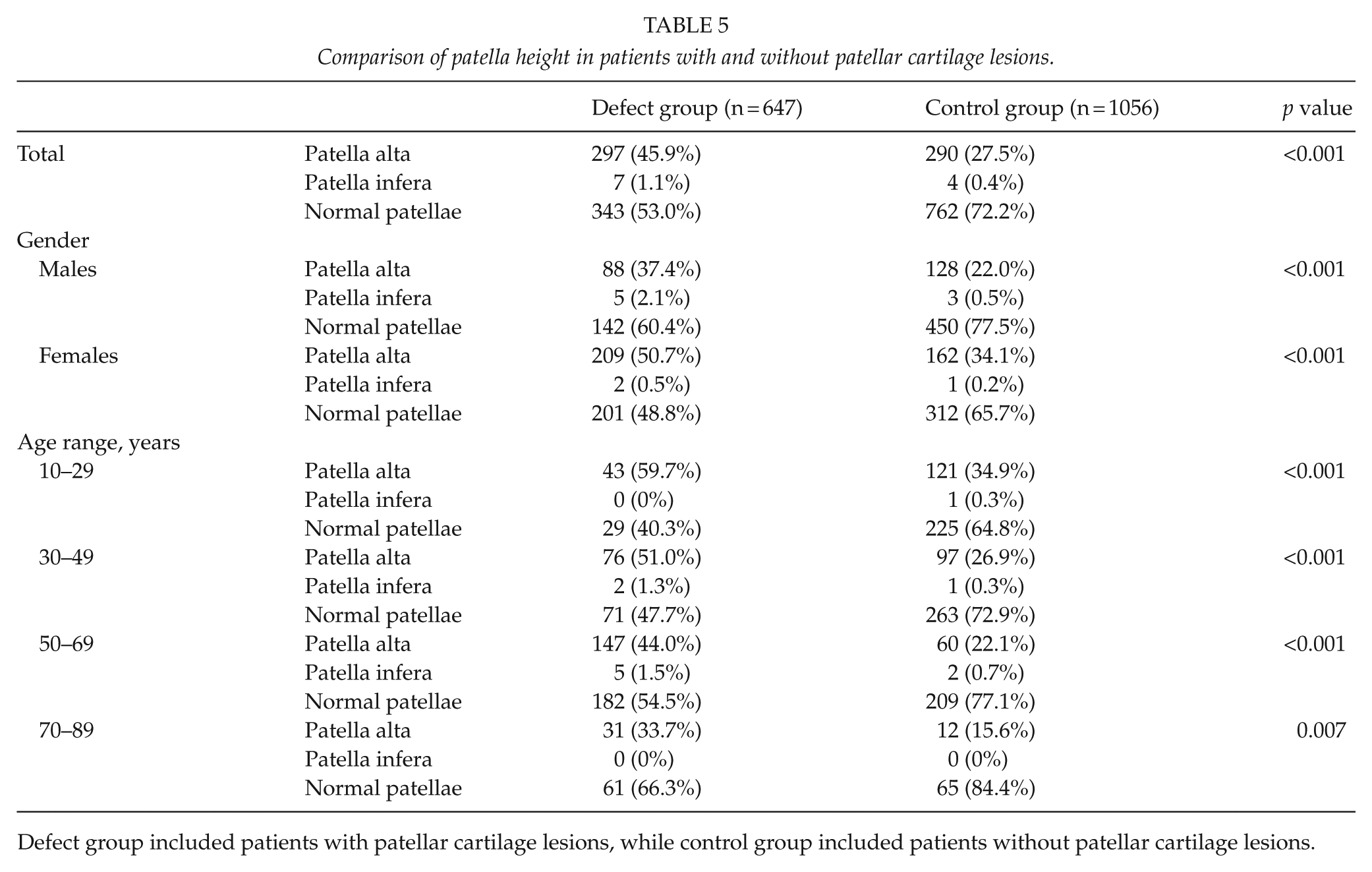
Defect group included patients with patellar cartilage lesions, while control group included patients without patellar cartilage lesions.
As significant difference in the rate of abnormal patella height was detected between the defect group and control group, we next analyzed the diagnostic accuracy. The ROC results showed that abnormal patella height had statistical significance in diagnosing patellar cartilage lesions (p < 0.001). However, the area under the curve (AUC) was relatively low (0.596; 95% CI = 0.568–0.624) (Fig. 1). The sensitivity was 47.0%, while the specificity was 72.2%.
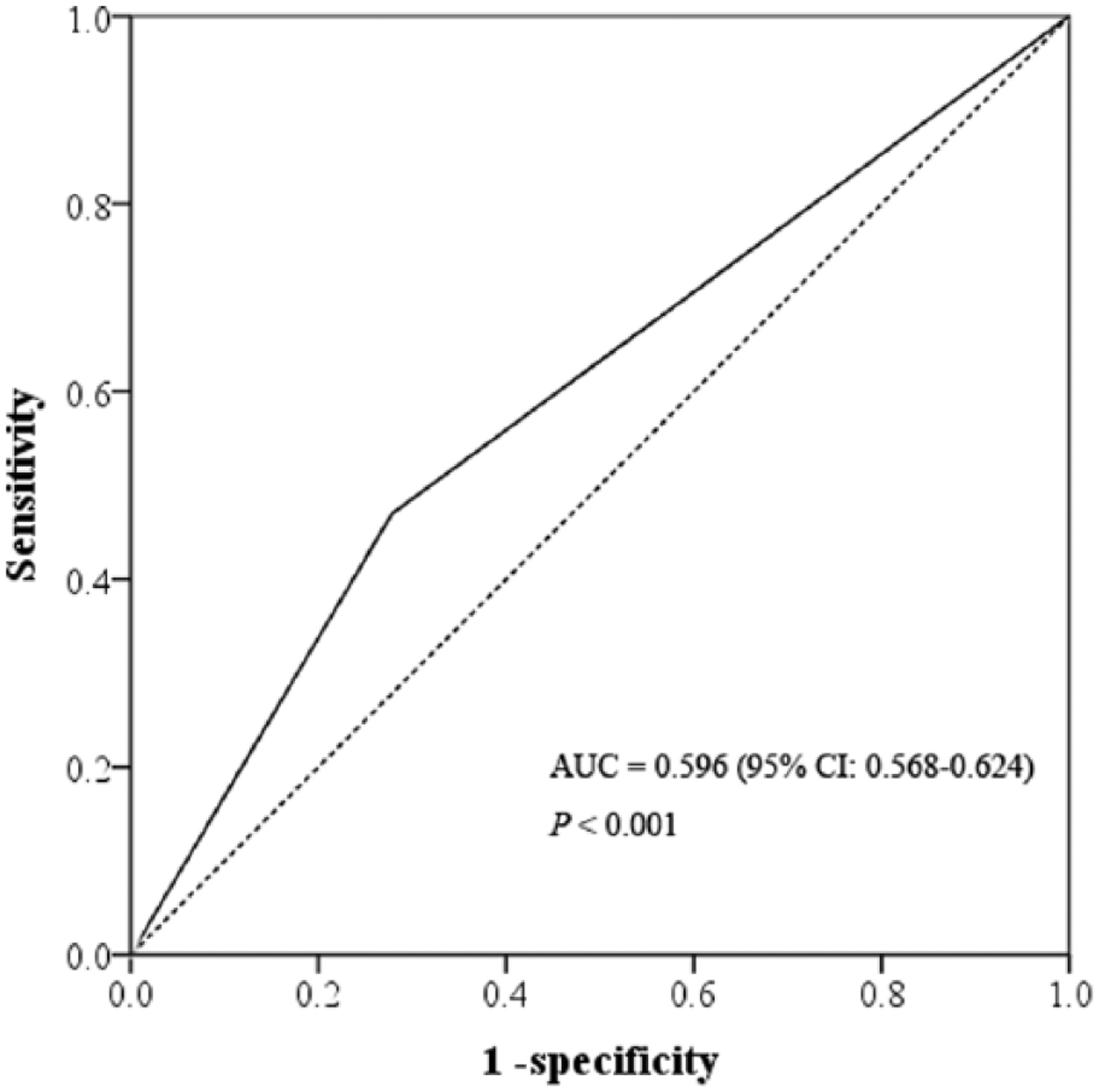
Receiver operating characteristic curve (ROC) analysis to detect the accuracy of abnormal patella height (patella alta and infera) in diagnosing patellar cartilage lesions.
Discussion
In this study, we first performed a population-based survey to investigate the prevalence rate of patellar cartilage lesions and their correlation with abnormal patella height in China with a large sample size.
MRI is considered as an accurate and noninvasive means. We used a low-field MRI machine to test patellar cartilage lesions. Unlike other high-field MRI machines which determine multiple body parts such as head, chest, and abdomen with different coils, the 0.2T MRI system used in this study is specialized for the joints of extremities. Second, volume of equipment is much smaller than the high-field MRI machines. Third, the extremity-dedicated MRI system only scans one joint of extremities, which shortens the testing time and improves patient comfort level, especially for claustrophobia patients. Most importantly, the 0.2T MRI system is sufficient to detect patellar cartilage lesions using T1-weighted, T2-weighted, coronal and axial GRE-STIR, and fat-suppression GRE-STIR images, as shown in Figs. 2 to 4.
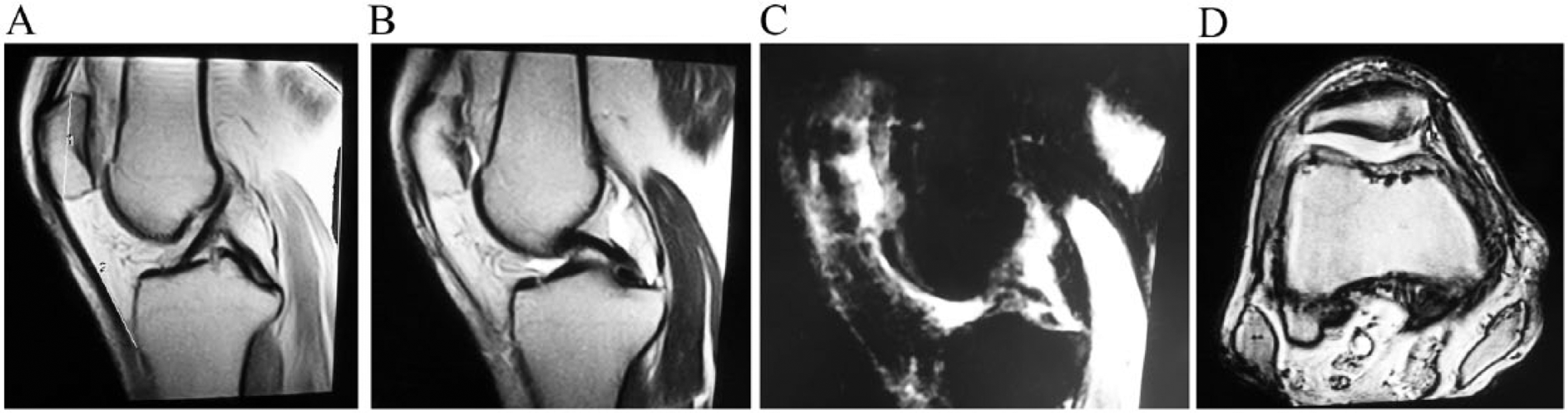
A 47-year-old female without patellar cartilage lesion. A: T1-weighted magnetic resonance image (MRI) of the left knee. “1” represents patellar length (PL) and “2” represents patellar tendon length (TL). PL = 40.4, TL = 40.5, TL/PL = 1.00. B: T2-weighted and T1-weighted (A) MRIs showed no abnormal signal in the posterior marginal cartilage of patella. C: Fat-suppressed MRI showed no cystic, abnormal signal. D: Axial MRI showed smooth posterior margin of patellar cartilage.
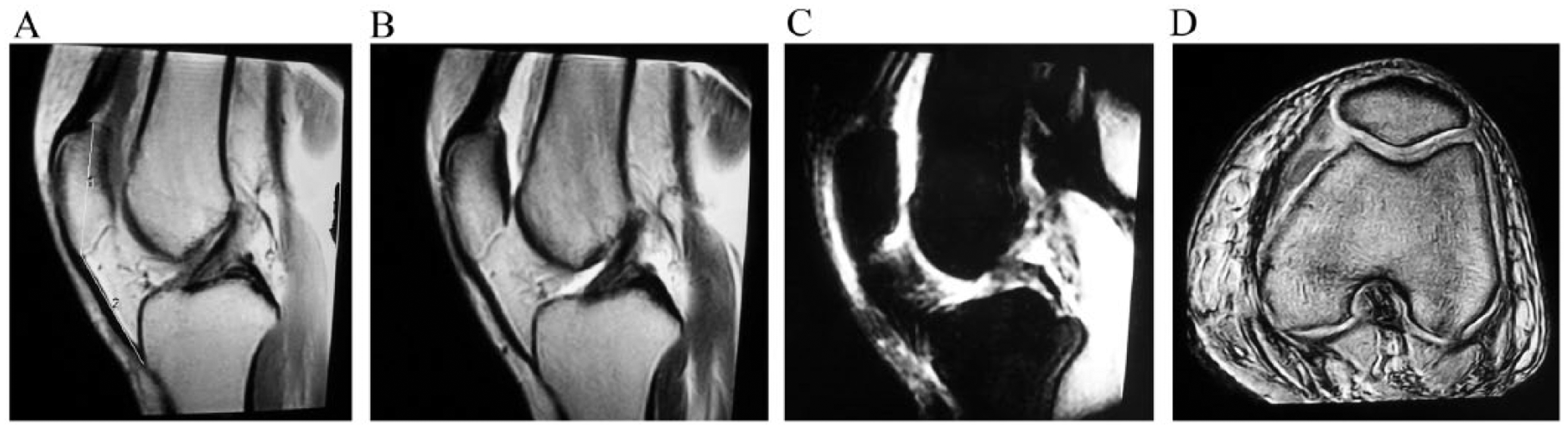
A 18-year-old male with mild patellar cartilage lesion. A: T1-weighted magnetic resonance image (MRI) of the left knee. “1” represents patellar length (PL) and “2” represents patellar tendon length (TL). PL = 35.5, TL = 52.3, TL/PL = 1.47. B: T2-weighted and T1-weighted (A) MRIs showed non-uniform low signal and focal thickening of the posterior marginal cartilage. However, the surface remained smooth. C: Fat-suppressed MRI showed non-uniform high signal. D: Axial MRI also showed non-uniform signal and focal thickening of the posterior marginal cartilage.
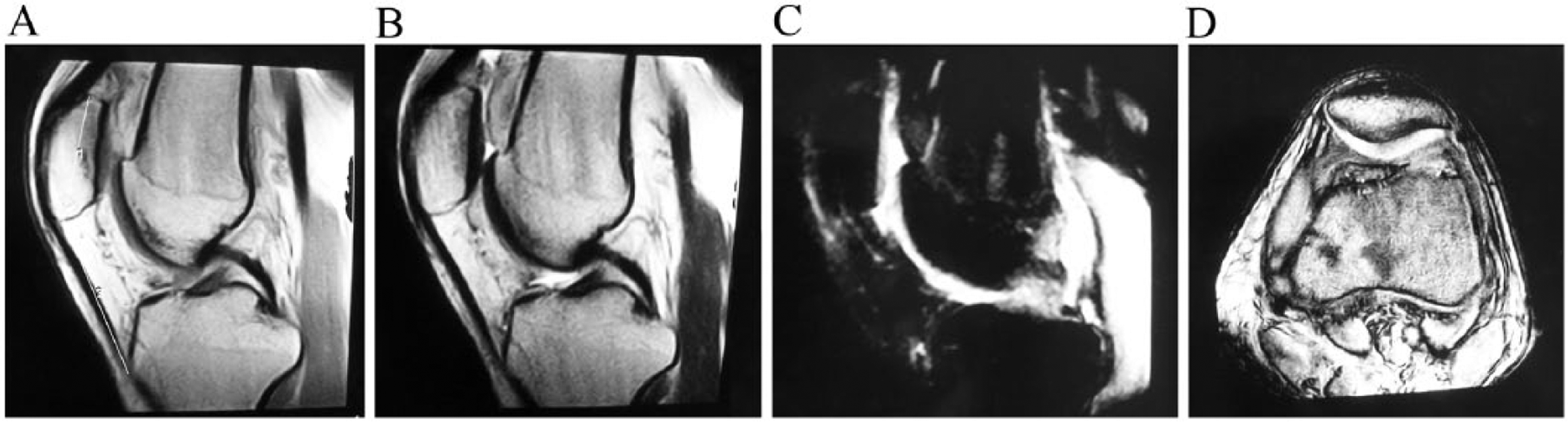
A 54-year-old male with severe patellar cartilage lesion. A: T1-weighted magnetic resonance image (MRI) of the right knee. “1” represents patellar length (PL) and “2” represents patellar tendon length (TL). PL = 34.8, TL = 51.9, TL/PL = 1.49. B: T2-weighted and T1-weighted (A) MRIs showed abnormal signal in the posterior marginal cartilage. C: Fat-suppressed MRI showed cystic, abnormal signal and subchondral bone exposure. D: Axial MRI showed non-uniform thickness and low signal.
Among the 1703 enrolled patients, the prevalence of patellar cartilage lesions was 38.0% and was higher in females. The distinct structure of pelvis in women causes a larger Q angle, which increases the risk of patellar subluxation and consequently enhances the surface pressure on lateral patellar facet joint, finally leading to the damage of patellar cartilage (21, 22). We also found that patellar cartilage lesion is an age-dependent disease, and the prevalence was increased with age. CP is most frequently encountered in young or middle-aged people, especially in athletes (23) due to the high risk of trauma to the knee, while osteoarthritis is more common in older population. Thus, the higher occurrence of cartilage lesion in cases aged more than 50 years may be the result of increased degenerative joint changes. In addition, over-exercise is relatively rare in young population and the visit rate for young people with knee pain or discomfort in the knee joint is relatively low in China, which may introduce age-related bias.
The ratio of TL/PL is a common and reliable index to determine the height of patella (18, 19). Inconsistent results were found in the relationship of TL/PL with patellar cartilage lesions. Some studies reported that no correlation was observed between the TL/PL ratio and cartilage lesions (14, 15), while other investigation demonstrated the opposite conclusion (16). In this study, we examined a much wider population in China and found that ISI increased in cases with cartilage lesions and represented as one of the independent risk factors. In addition, abnormal patella height including patella alta and infera could diagnose cartilage lesions with a relatively high specificity despite a low sensitivity and AUC, which indicates that abnormal patella height possessed superior ability to identify cases without a chondral lesion of the patellofemoral joint. This discrepancy in result may partly be due to different race or study population as the normal ratio of TL/PL varies based on the population: 0.90–1.30 for New York, USA (24); 0.74–1.50 for Wisconsin, USA (18); and 0.18–0.80 for Georgia, USA (15). Thus, the normal ratio should be determined in order to set the criteria for patella alta and infera by upper and lower limits of 2 SDs or upper and lower 2.5% of the study population (18). However, cases in the control group of this study could not represent the healthy population, since most of the cases underwent knee joint inspection with MRI equipment due to clinical symptoms such as knee joint pain, discomfortableness, or trauma. Hence, we used the original criteria for patella alta and infera which defined patella alta as a TL/PL more than 1.2 and patella infera as a TL/PL less than 0.8 (18, 19). Nevertheless, this may introduce the race bias, and the actual normal range of TL/PL in Chinese population should be detected in a prospective study. Besides, different selection criterion for control and defect cases may also influence the conclusion. We consecutively included cases that underwent knee joint inspection with MRI equipment in two hospitals, which was much closer to the clinical practice. Additionally, small sample size of the previous studies limits their validity.
Furthermore, we tried to analyze the relationship between TL/PL ratio and the stage of CP. However, data of stage were only recorded in 348 patellar cartilage lesions patients from Tongren Hospital. According to the limited data, no correlation was found between TL/PL ratio and stage of patellar cartilage lesions (p = 0.563, Supplementary Table 1). Nevertheless, this result needs to be further confirmed in a multicenter study with a large sample size.
In conclusion, we investigated the current situation on patellar cartilage lesions in a wide hospital population in China and analyzed the association between abnormal patella height (patella alta and infera) and patellar cartilage lesions. Females are more susceptible to patellar cartilage lesions, and the prevalence rate is increased by age. The abnormal patella position is significantly correlated with patellar cartilage lesions and could be used as a potential diagnostic marker.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Details and Details of Informed Consent
This study was approved by the Ethics Committees of the two hospitals. In addition, the written informed consent was obtained from each study participant.
Funding
This study was supported by grant from Shanghai Municipal Commission of Health and Family Planning (No. 20144Y0174) and Changning District Commission of Health and Family Planning (No. 20134Y01001).