
Abstract
Background and Aims:
Quadriceps and patella tendon ruptures are uncommon injuries often resulting from minor trauma typically consisting of an eccentric contraction of the quadriceps muscle. Since rupture of a healthy tendon is very rare, such injuries usually represent the end stage of a long process of chronic tendon degeneration and overuse. This review aims to give an overview of the current understanding of the pathophysiology, diagnostic principles, and recommended treatment protocols as supported by the literature and institutional experience.
Material and Methods:
A non-systematic review of the current literature on the subject was conducted and reflected against the current practice in our level 1 trauma center.
Results and Conclusion:
Risk factors for patella and quadriceps tendon rupture include increasing age, repetitive micro-trauma, genetic predisposition, and systemic diseases, as well as certain medications. Diagnosis is based on history and clinical findings, but can be complemented by ultrasound or magnetic resonance imaging. Accurate diagnosis at an early stage is of utmost importance since delay in surgical repair of over 3 weeks results in significantly poorer outcomes. Operative treatment of acute ruptures yields good clinical results with low complication rates. Use of longitudinal transpatellar drill holes is the operative method of choice in the majority of acute cases. In chronic ruptures, tendon augmentation with auto- or allograft should be considered. Postoperative treatment protocols in the literature range from early mobilization with full weight bearing to cast immobilization for up to 12 weeks. Respecting the biology of tendon healing, we advocate the use of a removable knee splint or orthotic with protected full weight bearing and limited passive mobilization for 6 weeks.
Introduction
Disruption of the extensor mechanism of the knee joint can be of bony or tendinous origin. Patellar fractures are two to three times more common than quadriceps tendon ruptures (QTRs), which in turn are two to three times more common than patellar tendon ruptures (PTRs) (1). It is generally accepted that rupture of a healthy tendon is rare. Tensile overload of the extensor mechanism usually leads to a transverse fracture of the patella, which is considered the weakest link of the extensor mechanism (2). PTRs or QTRs due to indirect trauma are in most cases the end stage of long-standing chronic tendon degeneration. Risk factors include age, repetitive micro-trauma, genetic predisposition, and systemic diseases, as well as certain medications (3). Kannus and Józsa (4) evaluated 891 biopsy specimens of spontaneously ruptured tendons (including 82 patellar and quadriceps tendons) and found that 97% showed degenerative changes, whereas these changes were detected in only 35% of intact tendons within age-matched control subjects.
The most common mechanism of injury is of a sudden contraction of the quadriceps muscle on a flexed knee, leading to an eccentric contraction and subsequent disruption of the extensor mechanism. Ciriello et al. (5) performed a systematic literature review in 2012 and reported that most QTRs are caused by a simple fall (61.5%) or a fall down stairs (23.4%). Other mechanisms such as rupture during sports activities (6%), car accidents (3.2%), spontaneous ruptures (3.2%), and agricultural injuries (2.3%, mainly penetrating trauma) are very uncommon. In about 14% of all cases, comorbidities such as diabetes, obesity, hyperparathyroidism, rheumatic diseases, and steroid use were reported. Bilateral QTR is a rare entity often leading to a delay in diagnosis of an average of 65 days, due to more than 50% of cases being missed on initial assessment (6). In all, 64% of these patients have predisposing comorbidities such as obesity (21.4%) and diabetes (17.8%), with half having more than one risk factor.
Patellar fractures are slightly more common in women, whereas the majority of tendon ruptures occur in males (1). QTRs are more commonly seen in patients older than 45 years (1, 7, 8) and are often associated with degenerative changes of the tendon (4). The rupture is typically situated 1–2 cm proximal to the superior pole of the patella (5), which corresponds to a relatively avascular region of the tendon (9). PTRs by comparison occur in patients who are younger (<45 years) and more active (1, 10) and more commonly result from direct trauma (11, 12) as well as iatrogenic injuries. The rupture site is most often in the proximal part of the tendon close to the inferior patellar pole (11, 12).
Diagnostics
Quadriceps and patella tendon rupture diagnoses can usually be reached through a thorough history and clinical examination. In traumatic cases, knee radiography is part of the basic diagnostics in order to rule out fractures. Clinical vigilance is required especially in spontaneous ruptures and the elusive bilateral cases.
History And Clinical Examination
The typical history for an extensor tendon rupture involves some kind of trauma, albeit much smaller than expected. It is typically indirect in nature, involving sudden eccentric muscle contraction while trying to avoid a fall and is felt as an intense pain. The clinical diagnostic triad includes acute pain, inability to actively extend the knee, and a palpable gap at the rupture site (10). Especially in QTR, the extensor mechanism may still be partially working, due to an intact retinaculum and iliotibial tract, allowing for straight leg raising. The palpable gap might be masked by a posttraumatic hematoma particularly with delayed presentation. Clinical findings of QTR can also include a low riding patella (patella baja). Due to the lesser amount of soft tissue surrounding the patellar tendon, the gap of a PTR is more clearly palpable. On inspection, a high riding patella (patella alta) is a common finding, and it fails to follow the tibia on knee flexion.
Radiology
Radiological investigations include plain radiography, ultrasound (US), and magnetic resonance imaging (MRI). In cases of traumatic knee injury, plain radiography is part of the standard diagnostic protocol. Apart from fractures and avulsions, degenerative changes such as the Tooth sign as well as patella positioning are assessed (see Fig. 1). According to a study by Hardy et al. (13), patella spurs are present in 79% of QTRs, 27% of PTRs, and in only 15% of patella fractures. Insall-Salvati described a ratio between the length of the patella (LP) and the patella tendon (LT) as assessed from a lateral knee X-ray or sagittal MRI. If the quadriceps tendon is torn, the index (LT/LP) is less than the physiological range of 0.74–1.5, whereas a PTR causes the ratio to be above the physiological range (14).
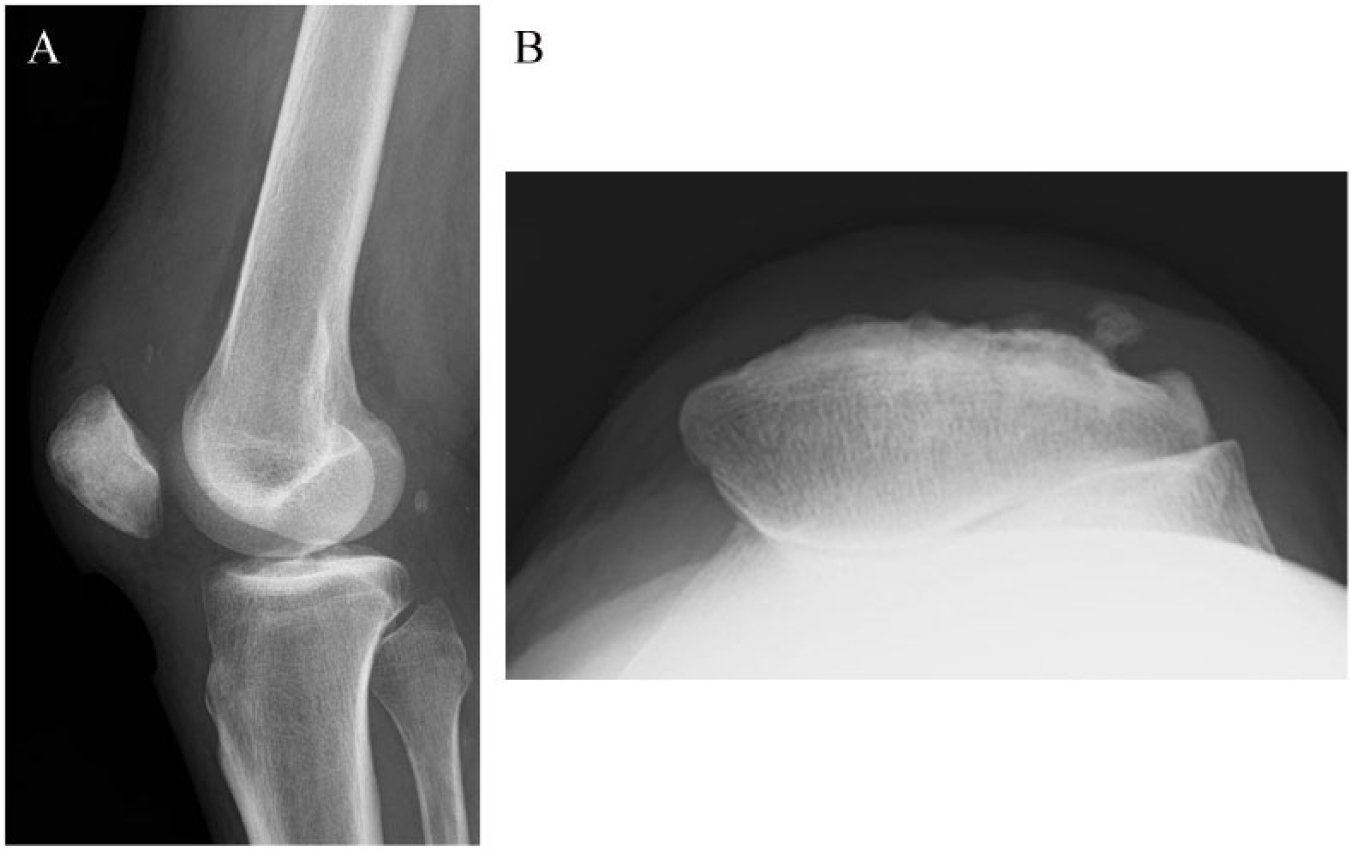
The typical radiographic findings in quadriceps tendon rupture. A) Low riding patella (patella baja) with anterior tilt of proximal pole and B) Tooth sign on skyline view of patella.
In cases where clinical assessment is deemed insufficient, ultrasonography is considered a reliable and inexpensive method to verify the diagnosis in acute as well as chronic cases and also helps differentiate partial from total ruptures (15). It also allows dynamic examination of the extensor mechanism and is not affected by metal implants.
MRI can be considered the gold standard imaging modality, but it rarely provides additional information that would alter management. It is more expensive and not as readily available as US, but might provide additional information in some chronic cases regarding tendon quality and muscle atrophy/fatty degeneration. In addition, a recent study by McKinney et al. (12) showed a surprisingly high incidence of associated intra-articular knee injuries with 9.6% in QTR and 30% in PTR. Most common were anterior cruciate ligament tears (18%) and medial meniscus tears (18%), with these injuries being more likely in high-energy trauma. In light of these findings, MRI should be considered in younger patients with high-risk mechanisms.
Treatment
Acute Tears
Acute PTRs and QTRs should be treated with early operative repair. The main prognostic factor influencing outcome is timing of surgery and less so the choice of surgical technique (8). Most authors advocate surgical treatment within 2–3 weeks from trauma, with incidence of poor functional outcomes and the need for augmentation growing in delayed repairs (10, 16).
According to literature, the most common surgical procedures, when treating tendinous knee extensor mechanism injuries, are fixation through patellar drill holes and simple end-to-end sutures (1, 5, 17–19). Fixation through patellar drill holes can be considered the gold standard in ruptures near the poles of the patella (see Fig. 2), whereas mid-substance tears have also been successfully treated with simple end-to-end sutures. Ciriello et al.’s literature review showed that 50% of quadriceps tendon tears are treated by patellar drill holes and 22.5% by simple suture. No significant difference was noted in the outcome between these surgical techniques (5, 8). Recently, repair using anchors instead of patellar drill holes has been described. Results from biomechanical studies failed to show notable differences between the anchor repair and patellar drill hole techniques (20), but no large clinical series or comparative studies are available to allow firm conclusions to be drawn. According to Hart et al. (21), both fixations are sufficiently strong, but trans-osseous fixation is stronger with higher ultimate tensile load. Fixation through patellar drill holes has a longer track record and has been shown to be a reliable, inexpensive, and straightforward procedure (18). The possible advantages of anchor fixation, however, are smaller skin incisions (22) and reduced operative time (20). Some authors recommend additional augmentation by cerclage wire, suture, Dall-Miles cables, or autogenous tendon graft bridging in patellar tendon repairs as a means of providing additional stability during early mobilization (23–25). Marder and Timmerman (26), however, published a series of PTRs treated without augmentation and early mobilization with excellent results, putting the need for augmentation into question.
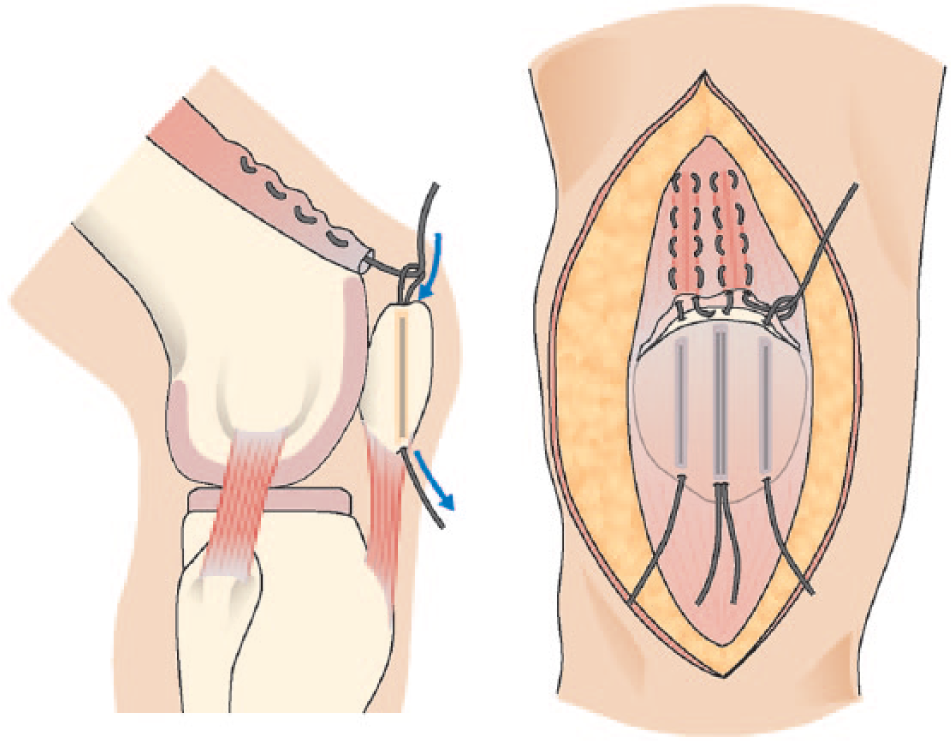
Operative technique of quadriceps tendon repair with tendon grasping sutures pulled through patella drill holes using suture lasso.
Operative management of PTRs and QTRs yields good clinical results with a low rate of complications. The reported rate of re-ruptures is 2%, with other complications including heterotopic ossification (6.9%), deep venous thrombosis or pulmonary embolism (2.5%), and superficial and deep infection (1.2% and 1.1%) (5).
Old Tears
In missed injuries with chronic ruptures or re-ruptures of the quadriceps tendon, the Scuderi (27) technique has been advocated to reinforce and the Codivilla technique to lengthen the tendon (18). In both techniques, a wide-based inverted V tendon flap is placed 1.5–2 cm proximal to the rupture and folded down and sutured over an end-to-end repair of the rupture site (see Fig. 3). The remaining tendon released from the old scar is then sutured side to side according to Codivilla. Delayed PTR repairs are often even more arduous as the quadriceps has drawn the patella proximally. These repairs should be augmented by tendon autografts (semintendinosus or gracilis tendon) as advocated by Matava or allografts or synthetic materials like Dacron or strong braided resorbable suture (PDS II) applied through transpatellar and transtibial drill holes (28, 29).
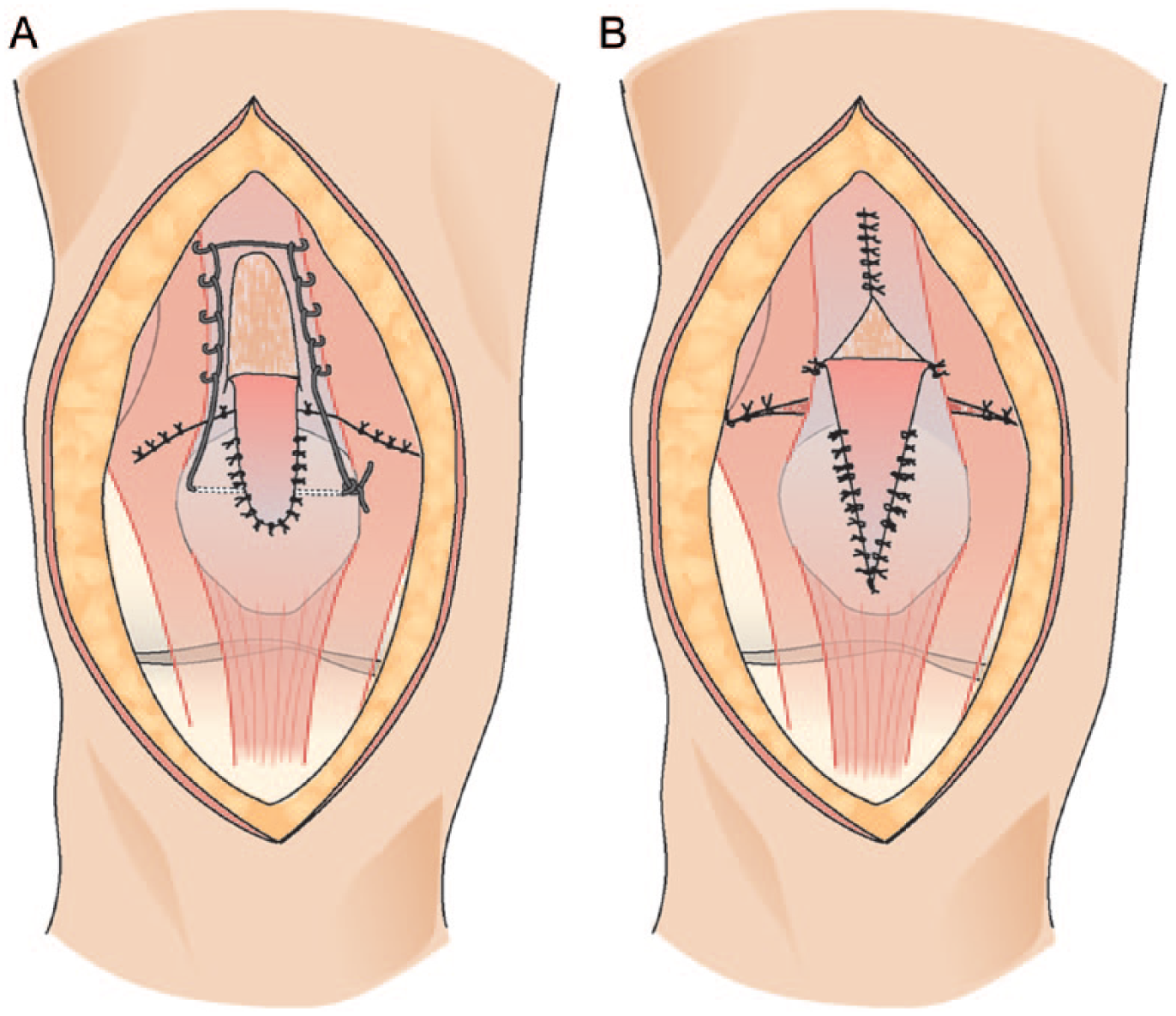
Operative schematic of A) Scuderi and B) Codivilla techniques.
Postoperative Protocol
There is a wide range of postoperative treatment protocols suggested in the literature, ranging from early mobilization and full weight bearing to cast immobilization for 6–12 weeks. Based on current knowledge of the biological process of tendon healing as well as clinical evidence available, immobilization should not exceed 6 weeks. Tensile stress is necessary to improve tendon biological and biomechanical characteristics, and knee mobilization is indicated to avoid joint stiffness and reduce muscle atrophy (5). There is good evidence that where stable fixation in acute ruptures is achieved, early weight bearing in extension and limited passive mobilization lead to good clinical results (11, 24, 25, 30).
Töölö Hospital Treatment Protocol
Diagnostics
In most cases, the history and clinical examination will lead to the correct diagnosis. Patients able to perform straight leg raise should, if possible, also be asked to perform knee extension from 90° of flexion. In traumatic injuries, plain radiology is routine, while US is reserved for ambiguous cases. In the typical middle-aged patient with a low energy mechanism, MRI is not advocated in our opinion, as any additional injuries uncovered would not alter management. MRI is indicated only in younger patients with higher energy trauma or in cases with particular clinical suspicion for additional injuries.
Treatment
Based on available evidence and our clinical experience, we recommend early operative treatment for acute patellar or QTRs, ideally within 2 weeks of injury. Our standard procedure includes fixation of two tendon grasping (Kessler, Krakow or Bunnell) No. 5 non-absorbable sutures through three longitudinal patellar drill holes. The drill holes are made using a 2-mm drill and should be at least 1 cm apart. If a tourniquet is used, it is deflated before tightening of the sutures to allow maximal tendon lengthening. The stitches are tightened with the knee in extension and an intraoperative range of motion of 0–90° should be achieved. The tendon ends and retinaculum on both sides can additionally be opposed using absorbable No. 0 stitches. In cases with severe tendon fraying or questionable patient compliance, the tendon repair can be augmented using a relaxing suture as described by West et al. (24). The relaxing suture is tightened with the knee in 30° of flexion. We prefer utilizing absorbable (PDS II) suture material instead of cerclage wire because of less soft tissue irritation and avoiding the need for implant removal (see Fig. 4). Before wound closure, correct alignment and patella tracking are verified using clinical and/or radiological means.
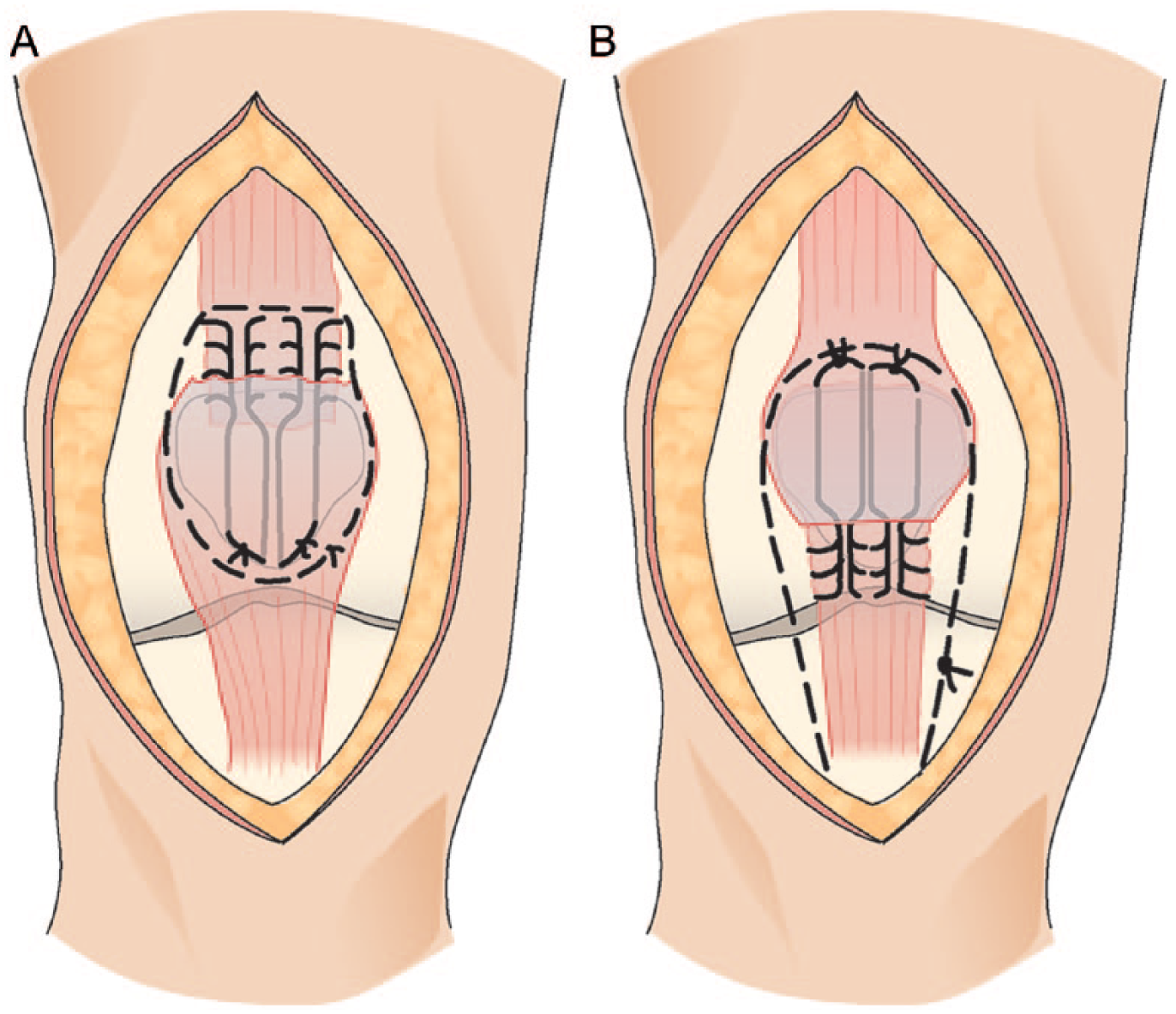
Operative technique schematic of A) quadriceps tendon repair and B) patella tendon repair, both with use of a relaxing suture.
Rehabilitation
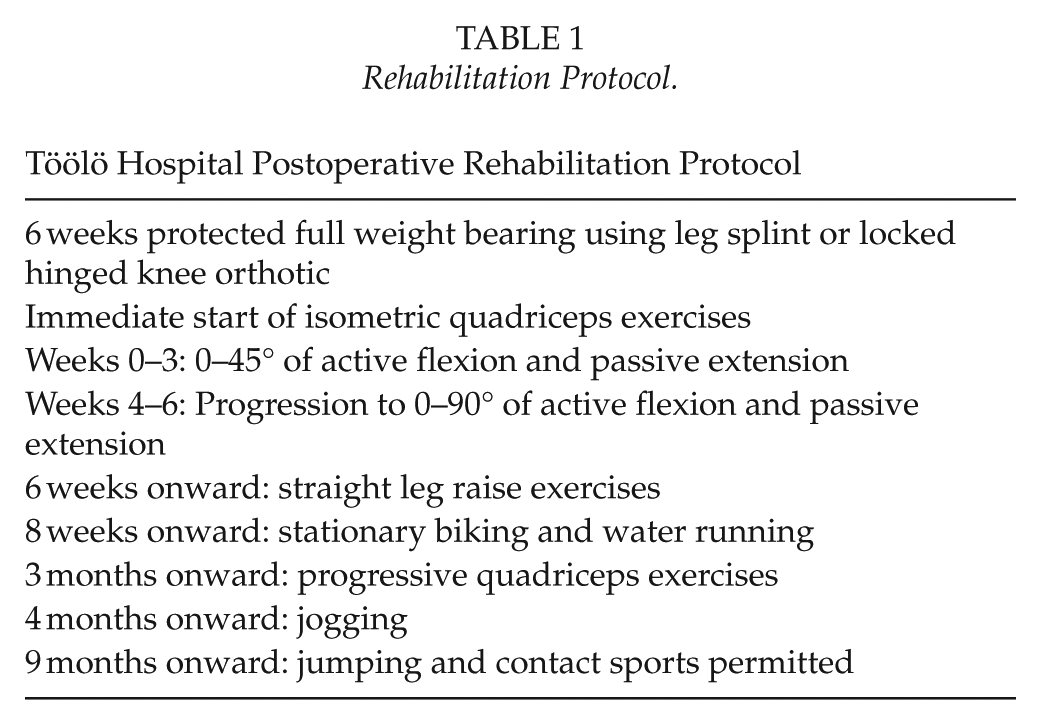
All knees are protected in a custom-made leg splint or locked hinged knee orthotic for a period of 6 weeks. In our experience, a custom-made removable leg splint is better tolerated by patients as premade orthotics often fit poorly and can cause irritation around the operative wound leading to wound complications (see Fig. 5). We begin with isometric quadriceps exercises immediately and allow active flexion up to 45° and passive extension up to 0° within 1–2 days postoperatively at least three times a day. The knee is maintained in extension at all other times, and protected full weight bearing as tolerated is allowed. After 3 weeks, the flexion range is increased gradually aiming to achieve 90° by 6 weeks. After 6 weeks, straight leg raise exercises are initiated and free range of motion allowed. Stationary biking and water running are utilized from 8 weeks on and progressive quadriceps exercises allowed at 12 weeks. Running is permitted at 4 months with jumping and contact sports restricted until 9 months (see Table 1).

An example of the custom-made leg splint used in Töölö Hospital for postoperative protection of the tendon repair.
Rehabilitation Protocol.
Footnotes
Acknowledgements
We thank for the support and encouragement of Markus Parkkinen and Jan Lindahl, from The Pelvic and Lower Limb Department of Töölö Hospital, in the writing of this article.
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.