
Abstract
Background and Aims:
The natural history of Kienböck’s disease is controversial. Only three papers report a pure natural history without treatment. We hypothesized that the natural course of Kienböck’s disease may be better than reported.
Material and Methods:
We examined eight patients with Lichtman stage III Kienböck’s disease without any treatment, evaluating clinical and radiological results (9 wrists; 7 men, mean age at onset of symptoms 34 years) over a period of 10–38 years (mean, 27.3 years) after symptom onset.
Results:
Lichtman stage remained the same in five of nine wrists. The inner structure of the lunate improved in three, remained the same in three, and deteriorated in three wrists, and its shape improved in two, remained the same in four, and deteriorated in three wrists. Pain averaged visual analog scale 3.1 at rest, 3.4 during motion, 3.6 with slight, and 5.2 with heavy exertion. The range of motion improved at extension 19% and at flexion 14%, reaching 81% and 72% of that of the contralateral wrist, and grip strength reaching 93%. The Disabilities of the Arm, Shoulder, and Hand averaged 11.3, Optional Disabilities of the Arm, Shoulder, and Hand 18.0, and Mayo Clinic score 70.0. The radiographic course did not correlate with clinical course.
Conclusions:
The long-term natural history of Lichtman stage III Kienböck’s disease is insufficiently good to suggest thoughtful observation alone as an option to treat it.
Introduction
The etiology of Kienböck’s disease is multifactorial: mechanical, anatomic, constitutional, or systemic mechanisms have been thought to initiate the avascular process, but with no specific etiology as yet identified (1). The natural course of Kienböck’s disease is obscure, according to a few studies (1–5). Its actual natural history appears in only three papers (6–8). Fujisawa et al.’s (7) results strongly suggest that Kienböck’s disease has the capacity to heal spontaneously in the long run. Kristensen et al. (8) concludes that Kienböck’s disease has a naturally benign course. Beckenbaugh et al. (6) notes that the disease settles into a mildly painful wrist malady with only modest reduction in motion and strength despite roentgenographic evidence of advanced wrist degeneration. In addition, some report an almost natural course, when the treatment has been temporary wrist splinting during painful periods at night or work (9–12) or longer immobilization (13–15). The aim of this study was to investigate the long-term natural outcome of Kienböck’s disease.
Material and Methods
In our hospital files from 1982 to 2006, we identified 11 patients with radiologically diagnosed Kienböck’s disease who had received no treatment; of these, nine agreed to participate and two declined because of poor physical condition and a lengthy trip for the follow-up. One patient with only 5 years of follow-up was excluded. The minimum follow-up of the remaining eight patients (nine wrists) was 7.0 years. These patients received no treatment, although the treatment option at the first consultation had been, in addition to thoughtful observation for five wrists, splinting during painful periods for one wrist, and surgery for three with the dominant wrist affected. The one who was recommended a splint did not use it, and the three advised to undergo surgery accepted no treatment due to rather mild symptoms and fear of surgery. Initial evaluation included posteroanterior and lateral radiographs, a medical history, and physical examination. No subjective assessment occurred at this initial evaluation.
Assessments
Initial data came from patients’ medical records (Table 1). All eight patients underwent physical and radiological examination at first consultation and at the final follow-up a minimum of 7 years after first consultation and 10 years after onset of symptoms.
Clinical data of patients with natural course of Kienböck’s disease.
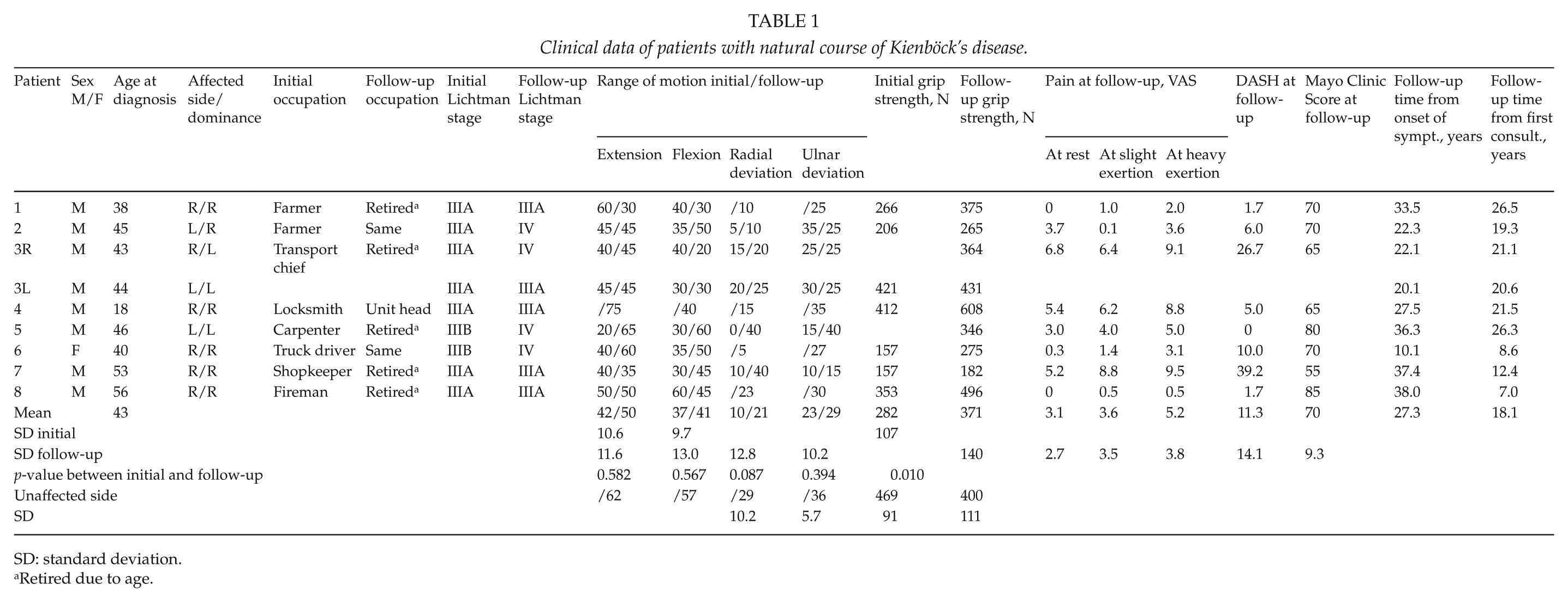
SD: standard deviation.
Retired due to age.
Objective Measurements
Range of motion (ROM) and grip (Jamar dynamometer, G.E.Miller, Inc., New York, NY, USA) and key pinch strength (B&L pinch gauge, B&L Engineering, Santa Ana, CA, USA) were measured in the affected and contralateral wrists by one author (T.V.). All the radiologic interpretations and measurements of plain radiographs were done by an experienced musculoskeletal radiologist (K.T.), accompanied by an experienced hand surgeon (T.V.). X-rays were performed in a standardized manor concerning wrist extension, forearm rotation, and radial-ulnar deviation. The radiographs for these examinations were a PA view (dorsopalmar view), a lateral view, and an oblique view to provide additional information as to the internal structure of the lunatum (16–18).
The following were radiologically measured in both wrists: ulnar variance, radioscaphoid, and scapholunate angles (19); metacarpal height ratio (metacarpal index) (20); ulnar translation ratio (19); Ståhl index (relation of height to breath of the lunate bone as a percentage); and lunate-covering ratio (calculated by dividing the amount of the lunate supported by the radius by complete radioulnar width of the lunate) (17). The metacarpal height ratio was calculated by dividing the height of the carpus by the length of the middle-finger metacarpal (normal: 0.54 ± 0.03). The ulnar translation ratio was calculated by dividing the carpal–ulnar distance by the length of the middle-finger metacarpal (normal: 0.30 ± 0.02). We also calculated an osteoarthritis index (arthrosis index) from 3 to 15, categorizing radioscaphoid, scaphotrapezoid, and scaphocapitate arthritic changes from 1 to 5 (1 = normal joint, 2 = joint line narrowed, 3 = joint line narrowed + sclerosis, 4 = joint line narrowed + sclerosis + osteophytes, 5 = joint deformed) (17). The inner structure of the lunate (cysts, uniformity, and density) was also assessed, as was the shape of the lunate bone from the posteroanterior and lateral views (21). The morphological features of the affected lunatum were compared to the primary radiographs on a scale comparing better, unchanged, or worse.
Subjective Measurements
At first consultation, Disabilities of the Arm, Shoulder, and Hand (DASH), Mayo wrist score, or VAS pain scales were not yet available. At follow-up, we determined pain by use of a visual analog scale (VAS, range 0–10) at rest, with unloaded movement, in slight exertion, and in heavy exertion (shoveling, hammering, chainsawing) to gain a better understanding of pain. We also measured the DASH-, work-, or hobby-related optional DASH, and Mayo wrist scores.
Questionnaires (17) were posted to the patients, along with an invitation to participate in the study. Patients completed the questionnaires at home and returned them at the follow-up visit.
Statistical Analysis
We determined differences between the wrists for ROM, strength, and radiological findings using the t-test (two-tailed). The paired sample t-test was used individually for ROM and grip strength between the first and follow-up examinations. Frequencies, proportions, means, ranges, and standard deviations (SDs) served as descriptive statistics. Significance was set at 0.05. We performed all statistical analyses with SPSS® (Version 20.0, SPSS Inc., Chicago, IL, USA).
Results
Age at onset of symptoms averaged 34 (range: 15–44) and at first consultation 43 years (Table 1). Of eight, five patients recalled some history of prior wrist trauma. Time from onset of symptoms to first consultation with one of the authors ranged from 0.5 to 31 (mean, 9.2; median 4) years. There were six right-handed patients, with the dominant wrist involved in six of them. At final evaluation, the mean age was 60.7 years (range: 40–72). Follow-up time from onset of symptoms was 27.3 years (range: 10–38).
Objective Results
The initial Lichtman stages are in Table 1. Initial ulnar variance ranged from −5 to 2 mm with a mean of −1.3 mm. The Lichtman stage remained the same in five at Stage IIIA (Fig. 1A and B), but two Stage IIIA and two IIIB wrists deteriorated to Stage IV. The shape of the lunate bone at follow-up had improved in two wrists and remained the same in four, but deteriorated in three. Lunate inner structure was better in three wrists and remained the same in three, but deteriorated in three. Significant differences between affected and contralateral wrists at follow-up were detectable in most radiological indexes (Table 2). Arthritic changes progressed during follow-up in eight wrists of nine and were moderate in three wrists (index 7–9), but in no case classified as severe (index >9). Only one patient had no arthrosis at all, and our mean arthrosis index was 5.4 in the affected and 3.1 in the contralateral wrists. The radioulnar joint was normal in six wrists at follow-up, but mild artrosis (index 2/5) was noted in one wrist and moderate arthrosis (index 4/5) in two. The contralateral radioulnar joint was normal in six wrists at follow-up and moderately arthritic in one.
Radiographic findings at first consultation and at mean 18 years in Kienböck’s disease.
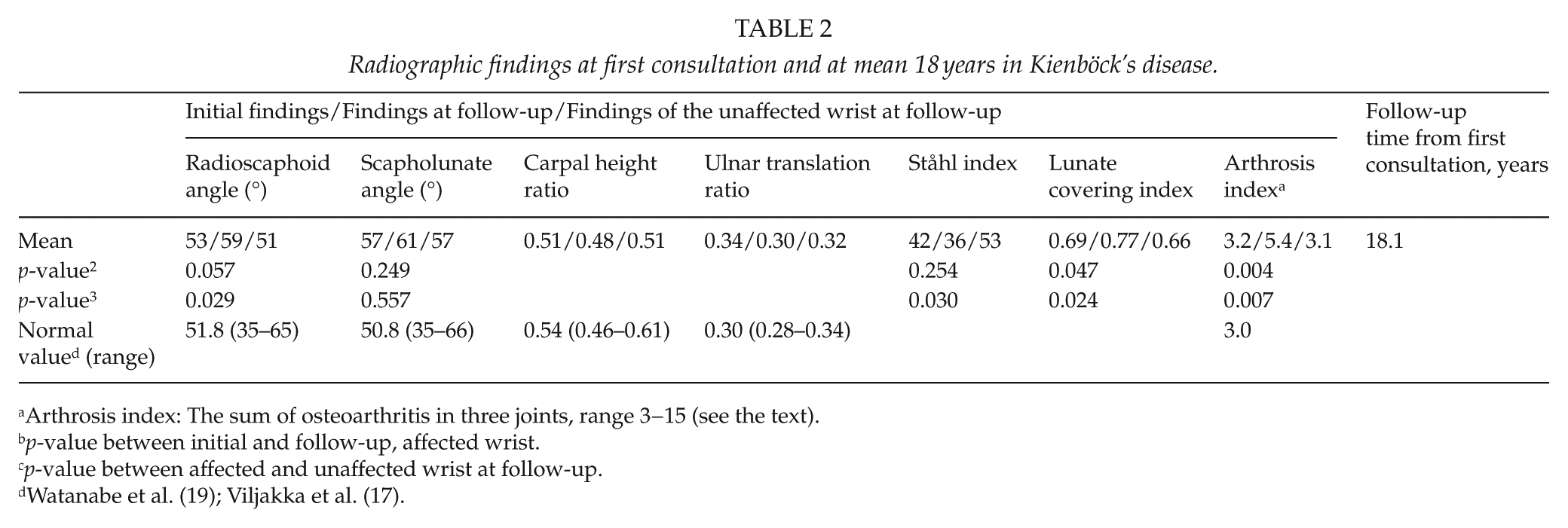
Arthrosis index: The sum of osteoarthritis in three joints, range 3−15 (see the text).
p-value between initial and follow-up, affected wrist.
p-value between affected and unaffected wrist at follow-up.

A) Patient number 3, left wrist, Stage IIIA Kienböck’s disease in 1992. B) The same wrist in 2012, 20 years later, still at Stage IIIA. Mayo wrist score 65, DASH 26.7.
Ulnar variance was at follow-up a mean −1.3 (−5 to +2) mm in the affected and −1.4 (−5 to +2) mm in the unaffected wrists. Two patients had a positive ulnar variance. They had arthrosis index of 8, VAS at rest 1.7, and DASH 5. Five patients with negative ulnar variance had arthrosis index of 4.2, VAS 2.9, and DASH 10.7. Ulnar variance did not correlate with the clinical result. At final follow-up, five wrists were Stage IIIA with arthrosis index 3.8, VAS at rest 2.7, and DASH 11.9. Four Stage IV wrists had arthrosis index 7.5, VAS at rest 2.3, and DASH 5.3. We could find no correlation between radiological results and clinical or subjective outcome (Table 3).
Clinical, radiographic, and subjective findings after natural course of on average 18 years in Kienböck’s disease.
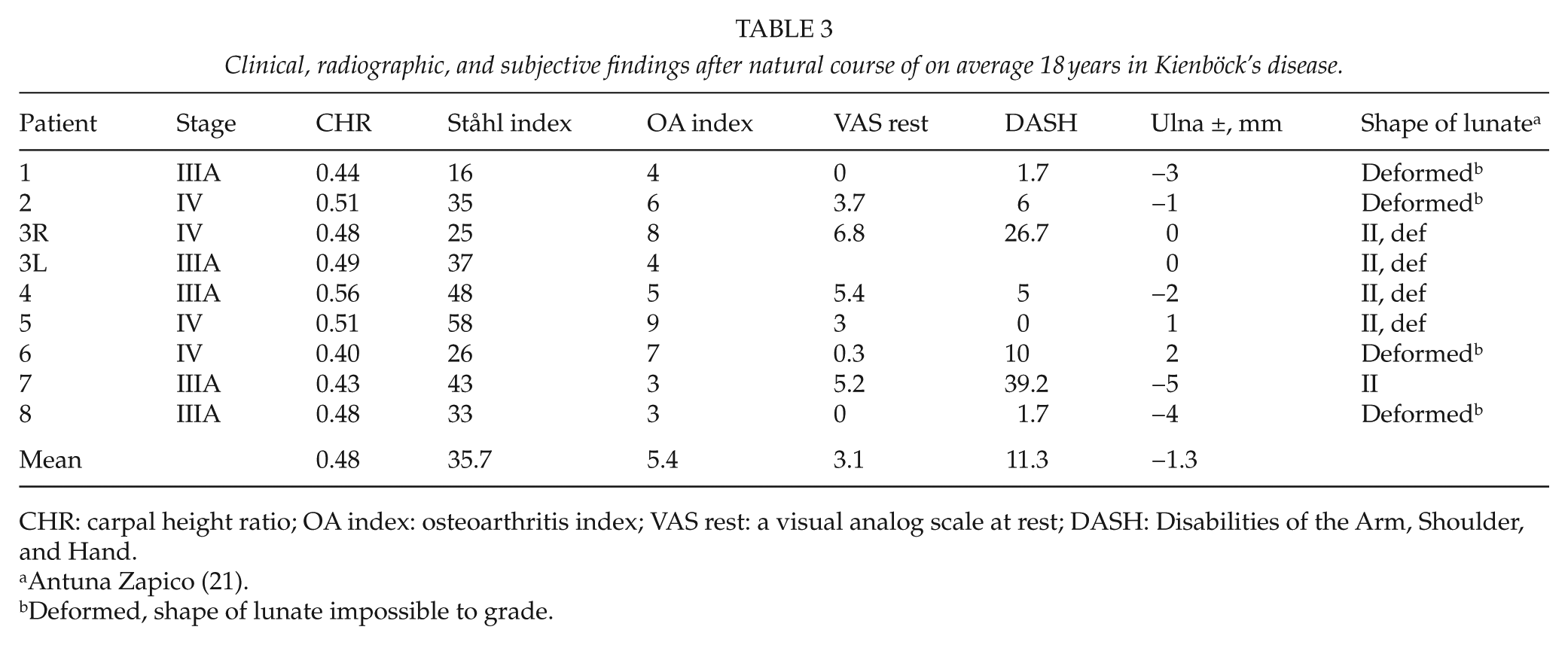
CHR: carpal height ratio; OA index: osteoarthritis index; VAS rest: a visual analog scale at rest; DASH: Disabilities of the Arm, Shoulder, and Hand.
Antuna Zapico (21).
Deformed, shape of lunate impossible to grade.
ROM improved during 18 years: extension by 19% and flexion by 14%, but not significantly (Table 1). Extension of the affected wrists reached 81%, flexion reached 72%, radial deviation 73%, and ulnar deviation 80% of the unaffected side. One patient considered his wrist as interfering during normal daily activities.
Grip strength improved during the 18 years by 32% in the affected hand (Table 1), whereas grip strength of the unaffected hand deteriorated 14% during that time. Grip strength still was inferior by 7%, and key pinch by 3% compared to abilities of the contralateral hand.
Subjective Results
VAS pain averaged at rest 3.1 and in wrist motion 3.4 (Table 1). One patient was totally free of pain at rest and during motion. DASH averaged 11.3 (range: 0–39.2) and optional DASH 18.0 (range: 0–56.3). One patient had DASH 0 (Fig. 2A and B). Mayo wrist score averaged 70.0 (range: 55−85).

A) Patient number 5, Stage IIIB Kienböck’s disease in 1982. B) The same wrist in 2009, 26 years later, Stage IV, Mayo wrist score 80, DASH 0.
Six patients had continued their earlier work; two had changed to lighter work. Three patients still continued working, and five were retired, none due to the wrist problem. Wrist symptoms had diminished during these years markedly in one patient and somewhat in one, but remained unchanged in one and deteriorated in three; two patients did not respond. One patient did smoke, three patients drank alcohol regularly, and two seldom. None evaluated the result as excellent, one called it good, three said fair, and two said poor; two did not respond.
Discussion
The natural history of Kienböck’s disease is poorly understood (5). Results of one systematic review show that subjective pain in Kienböck’s disease improves regardless of treatment type. ROM and grip strength also significantly improve in all patients treated surgically, but not among those managed non-surgically (4). The assumption is that the disease progresses through its stages and the lunate will ultimately collapse and fracture (10). That did not happen in our patients. The symptoms gradually decrease over time, indicating a benign course; the radiographic course does not, however, mirror the clinical course (3,22), nor did it do so in our study.
Actually, the natural history of Kienböck’s disease is covered in only three papers (6–8). Fujisawa et al. (7) evaluated 17 patients with the disease at 15 years. Of those, five had received no treatment, and five had used a wrist splint for 1–2 months. Kristensen et al. (8) evaluated 26 wrists at 18 years, and Beckenbaugh et al. (6) reviewed clinically 23 patients at 7 years, of which 10 were without any treatment.
Immobilization fails to help, but Kienböck’s disease has a naturally benign course, although the lunate is never normal nor does it become less deformed than at the time of the diagnosis (8) (Table 4). However, in our study of nine wrists, the shape of the lunate bone at follow-up had improved in two, and lunate inner structure was better in three. Fujisawa reported the same: Kienböck’s disease has the capacity to heal spontaneously in the long run. Radiological improvements evident are restoration of bone height, fracture healing, decrease in excessive radio density, and reconstitution of the deranged bony trabeculae (7) (Table 2). Martini states that remission is possible in the early stage of lunatomalacia within 4–35 months after symptom onset (23).
Literature on the natural course of Kienböck’s disease.
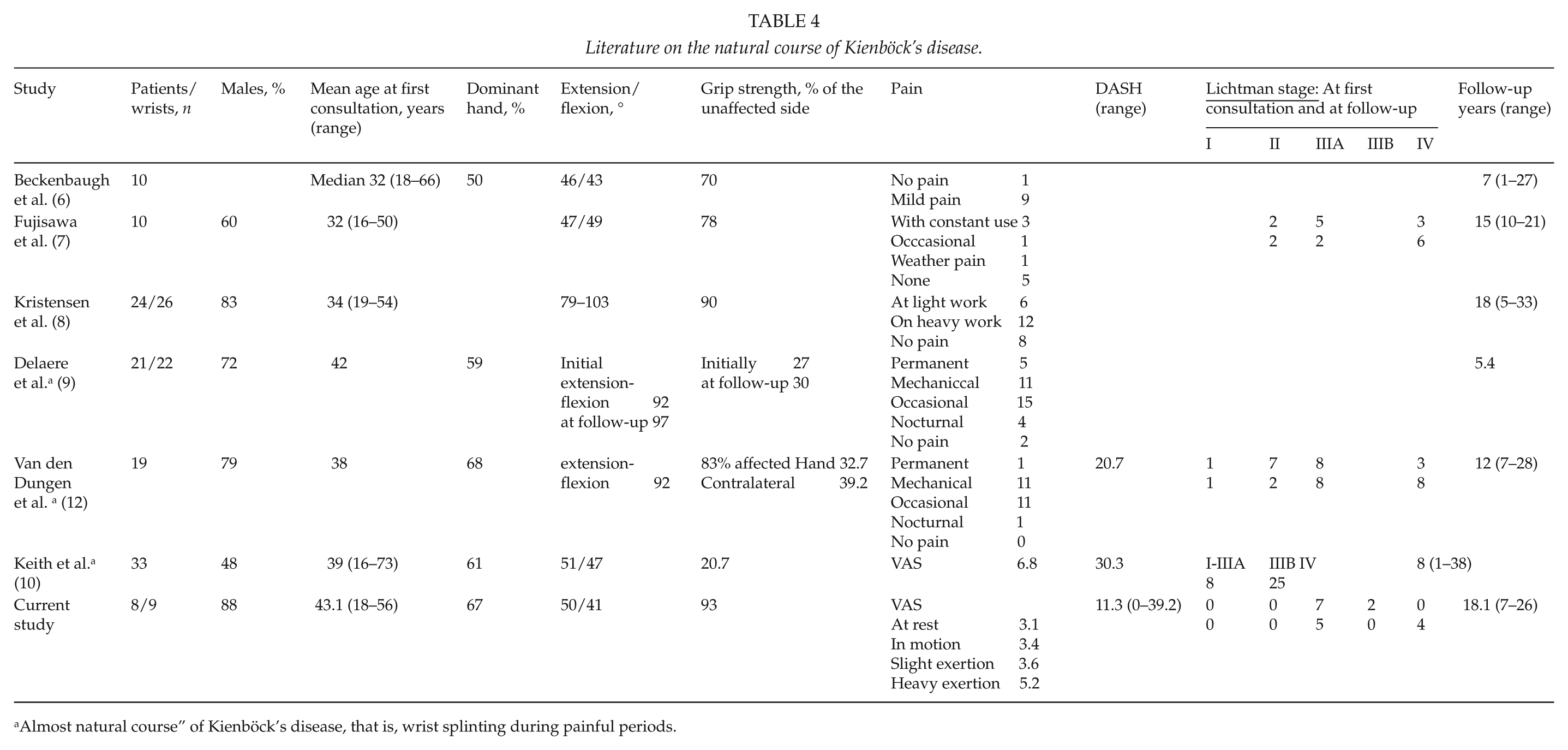
Almost natural course” of Kienböck’s disease, that is, wrist splinting during painful periods.
In the literature, Lichtman stage improved in two, deteriorated in four, and remained the same in one at Stage III and in three at Stage IV (7). The lunate was never normal nor was it less deformed after 18 years than at the time of diagnosis (8) (Table 4). Beckenbaugh et al. (6) states that roentgenograms show progressive changes as the follow-up period lengthens. We found that five of our nine wrists with Kienböck’s disease without any treatment remained at Lichtman stage IIIA during 18 years.
Kristensen et al. (8) reported 82% osteoarthrosis in the radiocarpal joint after 18 years. We found mild or moderate arthrosis in 89%. Fujisawa et al. (7) reported an improved Ståhl index in one of five patients, meaning some kind of restoration of the lunate. In our series, the Ståhl index improved in four wrists and deteriorated in five. Thus, it seems that the natural course of Kienböck’s disease is better than believed, at least radiologically. However, we found significant differences between initial and follow-up x-rays in all indexes except scapholunate angles.
Concerning ulnar variance, an association has emerged between ulnar negative variance and development of Kienböck’s disease (24), but contrary findings have also appeared (25). In the present small series, we found no relation between ulnar variance and radiological or clinical results.
Pain among 10 wrists existed in 3 with constant use but 5 wrists were painless after a 15-year natural course (7) (Table 4). At 18 years, in another study, of 26 wrists, 8 (31%) were painless (8). A different set of nine patients with Kienböck’s disease without any treatment had only mild pain after a mean 7 years (6). At 18 years, we had only one painless wrist at rest and during motion. Our mean VAS values during motion as well as in light and heavy exertion were higher than we had expected, indicating that Kienböck’s disease was progressing.
A systematic review showed that ROM does not improve among those Kienböck wrists managed non-surgically (4). Beckenbaugh et al.’s (6) patients had decreased motion. Fujisawa et al. (7) reported extension of 37° and flexion of 42° after 15 years, figures about the same as our 50° and 41°. In our study, ROM improved in all directions in only two wrists, but mean values in extension, flexion, and deviations were all a little better at follow-up.
Among studies, grip strength has averaged 81% of the unaffected side after 15 years’ natural course (7). In this study, grip strength improved in all seven cases available without any treatment, averaged 93% of the unaffected side, and improved 32% in 18 years, while strength of the contralateral hand deteriorated 14%. These findings seem to be in accordance with the reports that after non-surgical treatment, results gradually improve concerning pain, ROM, grip strength, and subjective results (6,26).
Concerning the clinical result without any treatment, Fujisawa et al. (7) reported that it was not so good: of 10 cases at 15 years, three had fair and two had poor clinical results. In this study, of seven responding patients, none evaluated the result as excellent, one called it good, three said fair, and two said poor, and DASH averaged 11.3 after 18 years. The radiographic course, for example, the shape of the lunate (21) (Table 3), did not correlate with the clinical course as other authors have also found (3,22). This, we cannot explain.
The many suggested surgical options for Kienböck’s disease include radial shortening osteotomy (RSO), proximal row carpectomy, and STT arthrodesis. Especially after RSO, some authors have reported better results than ours after a natural course of Kienböck’s disease (17,19,27–29).
There exist limitations to this study. We used no validated scores for pain or wrist function at the time of the Kienböck’s disease diagnosis. Second, our material comprises so few patients that significance is not always reached in our statistical analysis.
In conclusion, the natural long-term course of Lichtman stage III Kienböck’s disease is not good enough to state that thoughtful observation alone is an option as treatment. However, conservative treatment or observation may be an option, if the patient already has a long history of the disease with only mild symptoms.