
Abstract
Background and Aim:
To evaluate the amputation-free survival after below the knee percutaneous transluminal angioplasty in a consecutive group of patients with critical ischemia of the lower extremity.
Materials and Methods:
A total of 70 consecutive patients with critical ischemia were treated with below the knee percutaneous transluminal angioplasty at the vascular center at Rigshospitalet with the purpose of limb salvage. All patients were deemed unfit for major surgery due to anatomical limitations or severe co-morbidity, and no prior attempts of revascularization were performed. Follow-up clinical examinations were performed within 6 weeks and after 1 year. All medical records were crosschecked with the national vascular registry ensuring a valid 1-year status in 97% of the patients.
Results:
A total of 15 major amputations were performed during follow-up, with 11 amputations performed within the first year. Complications after percutaneous transluminal angioplasty were rare. Cumulative mortality after 1 and 2 years was 22% and 34%, respectively. Amputation-free survival at 1 and 2 years of follow-up was 68% and 58%, respectively. There were no association between known risk factors such as diabetes, ischemic ulcers, cardiac disease, history of smoking, major amputation, or overall amputation.
Conclusion:
Below the knee percutaneous transluminal angioplasty in patients with end-stage peripheral arterial disease and critical limb ischemia is a safe procedure in relieving critical ischemia, reducing the short-term rate of a major amputation as opposed to best medical treatment alone.
Introduction
Critical limb ischemia (CLI) is a dangerous condition with a high mortality rate, potential socio-economic loss, and risk of amputation, especially in people with diabetes (1–4).
Surgical bypass grafting has long been considered the gold standard of revascularization for lesions that are below the knee (BTK) (5). Percutaneous transluminal angioplasty (PTA) also improves limb perfusion; however, current treatment options are far from optimal even if this endovascular approach is the first-line option for patients with arterial occlusive disease above the inguinal ligament (6–8).
In the past, there has been reluctance toward endovascular procedures performed BTK as studies have indicated limited treatment effect (9, 10). Primary patency of BTK angioplasty has shown inferior results at 1-year level compared to peripheral bypass surgery (58% vs 82%); however, the clinical benefit is comparable with equivalent limb salvage rates (11–13).
The ultimate goal for treating BTK occlusive disease is to salvage the limb and promote wound healing. Implementing an endovascular first strategy for CLI using low-profile tools suitable for small vessel disease could access even the most challenging calcified arteries (14, 15). Furthermore, sub-intimal technique is also an option for crural arteries (16, 17). Drug-eluting stents (DES) and drug-eluting balloons (DEB) have emerged as potential alternative technologies to combat peripheral arterial disease (PAD) and its risk for restenosis. At present, studies have not convincingly confirmed the added value of these techniques (18, 19). Endovascular intervention of the crural arteries has largely been confined only to patients with CLI and in whom surgical options were limited (20, 21).
The aim of this retrospective study was to evaluate limb salvage and survival in BTK arterial segments in patients with critical ischemia following endovascular treatment.
Material and methods
Patients
All patients with CLI who were not eligible for BTK reconstructive vascular surgery were included. This inclusion criterion was determined by an experienced vascular surgeon at the time of referral to PTA. The main reasons for not being a candidate for open surgery are listed in Table 1. In 50% of cases, more than one reason to not consider surgery was present (mean: 1.7; standard deviation (SD): 0.8; range: 1–4). Approval from the regional institutional review board was not required for the performed research.
Primary reason for not considering open surgery in the 70 patients included in the series.
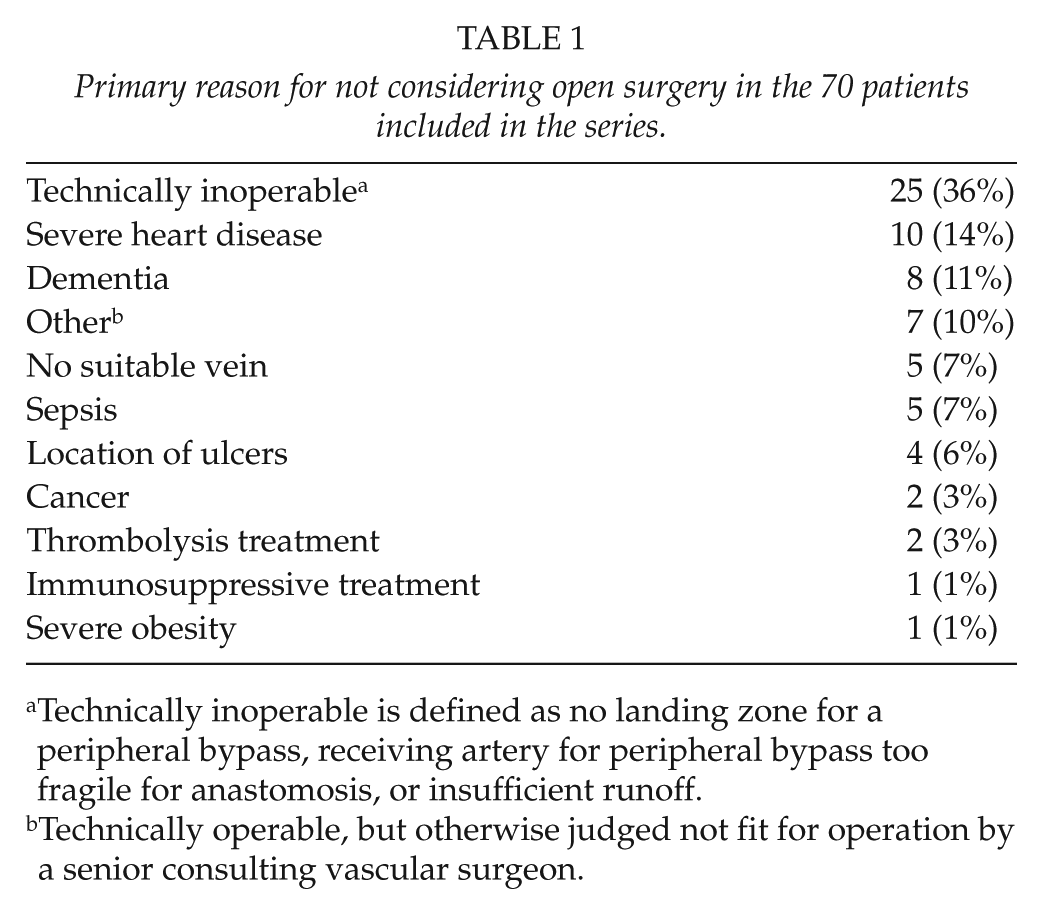
Technically inoperable is defined as no landing zone for a peripheral bypass, receiving artery for peripheral bypass too fragile for anastomosis, or insufficient runoff.
Technically operable, but otherwise judged not fit for operation by a senior consulting vascular surgeon.
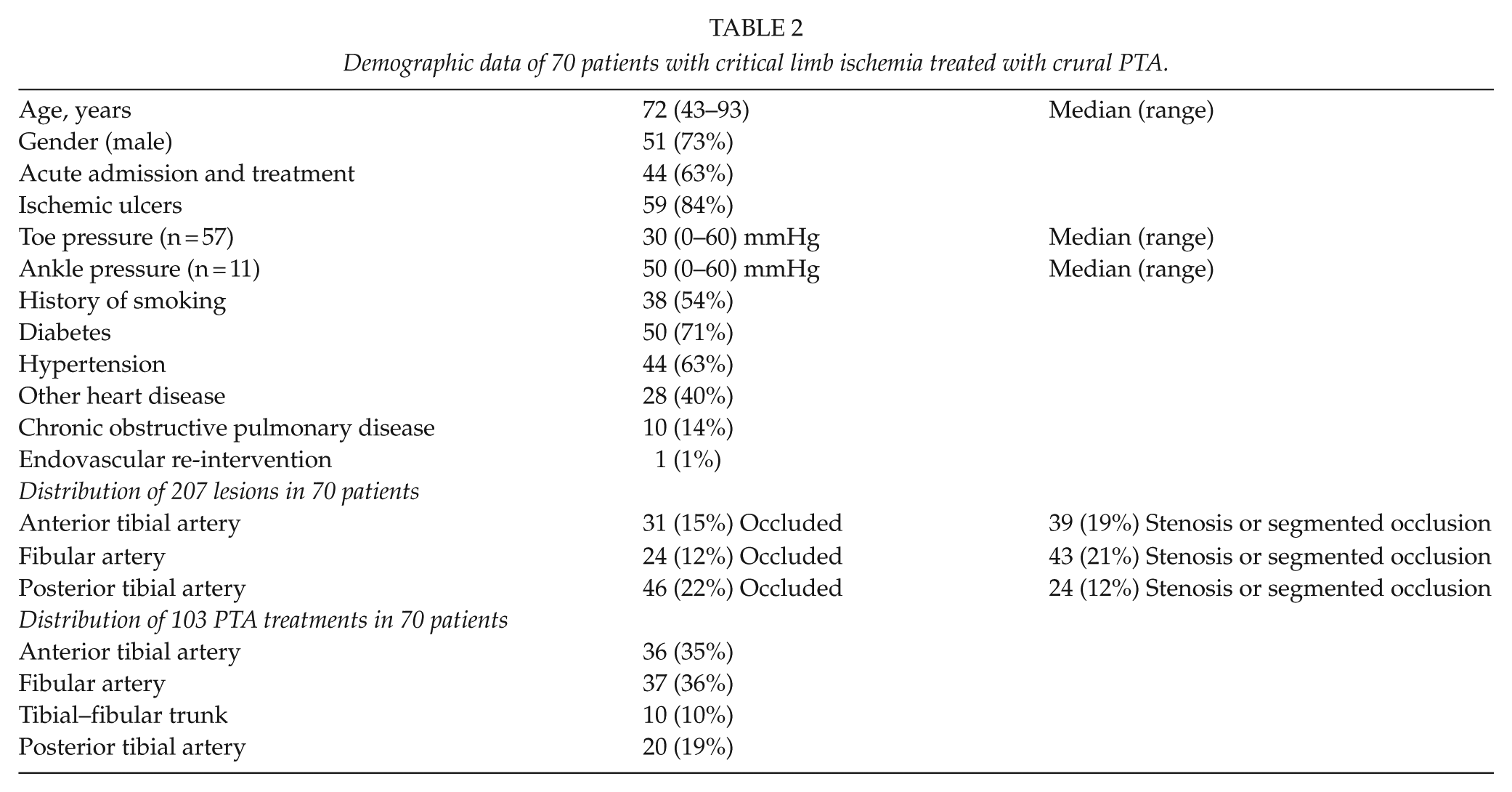
We identified 77 patients having 80 consecutive infrapopliteal endovascular procedures due to CLI from April 2010 through December 2012. Data were gathered prospectively from our in-house registry and were analyzed retrospectively. Six patients with prior in situ bypass graft were excluded due to in situ graft stenosis and not stenosis in the genuine artery, as well as one patient who was treated in the aftermath of a trauma and had no history of PAD. Two patients who had bilateral procedures performed were included; however, we excluded the least ischemic limb and only considered the most ischemic leg of each patient. Finally, we included the first treatment of a patient, who had a redo PTA procedure after 3 months, accepting this instance of assisted patency. In total, the series comprised 70 patients receiving 70 infrapopliteal endovascular procedures. Demographic data, preoperative clinical characteristics, endovascular interventions including re-interventions, as well as postoperative characteristics and complications were collected (Table 2). The distribution of the preoperative lesions in the anterior tibial artery, fibular artery, and the posterior tibial artery is presented in Table 2. Vessels were characterized as either open, occluded throughout the artery or with significant stenosis/segmented occlusions.
Demographic data of 70 patients with critical limb ischemia treated with crural PTA.
Methods
Patient history and available preoperative imaging studies were reviewed by a consultant vascular surgeon and were discussed with a consultant interventional radiologist for consensus. None of the cases suggested peripheral bypass surgery as a viable solution prior to endovascular treatment. In two cases, the result of the crural intervention led to re-evaluation, and subsequent peripheral in situ bypass surgery was performed when the PTA-treated vessels thrombosed 1 and 6 days, respectively, post PTA.
Presenting signs of CLI patients were examined with distal pressures measurements and color duplex ultrasound and then referred to angiography for further diagnostics. If angiography and case history indicated no possible means of open surgery in BTK lesions, BTK PTA was performed in the same procedure.
The patients were treated with the purpose of limb salvage aimed at recanalizing at least one crural vessel. Treatment of specific angiosomes was not used as indication (22). Standard protocol for intraoperative heparin advised 70IU/kg and additional doses throughout the procedure. In practice, 5000 units were given according to operators discretion followed by 1000 units additionally per hour. Activated clotting time was not included in the standard protocol of the institution. All patients were prescribed statins, and a lifelong 75 mg daily acetylsalicylic acid (ASA) dose was prescribed after the procedure. Clopidogrel was prescribed postoperatively in selected cases (n = 4). The infrapopliteal procedures were performed in a dedicated angiosuite providing high-quality imaging and a large field of view. Vital signs were constantly monitored.
The Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Standards of Practical Guideline for BTK interventions (23) were followed, including standard low-profile materials of 0.018 and 0.014 in, 1.5–4 mm PTA balloons up to 240 mm long, and extra long shafts. Both monorail (rapid exchange) and over-the-wire systems were used. Over-the-wire systems create better pushability and column strength and were thus preferred. Long shaft systems up to 150 cm were used when a cross-over approach was deemed necessary. However, the antegrade ipsilateral approach was the preferred choice using an antegrade ultrasound-guided micro-puncture of the common femoral artery (CFA) for access. Baseline digital subtraction angiography (DSA) was obtained from the whole limb using a 4-5 French system. Significant stenoses, defined as 50% diameter reduction as compared to nearest non-diseased segment, of the superficial femoral artery (SFA) were treated primarily with PTA and/or stents. Thereafter, a long sheath/catheter was placed in the popliteal arterial segment and guided by a superselective DSA/roadmap along the crural vessels. Balloon and eventual stent diameters were chosen according to reference vessel diameter by quantitative vessel analysis. Balloon dilatation was up to 2 min, and efforts to treat more than one vessel were observed. Standard angioplasty balloons were used in 64 cases (91%), while DEBs were used in 6 cases (9%) (IN.PACT Amphirion n = 5, IN.PACT Pacific n = 1). No DES or bare metal stents were used in the BTK lesions in this series. In all, 11 patients had simultaneous angioplasty (n = 3) or stenting (Covidien EverFlex n = 5, Abbott Fox n = 2, brand undisclosed n = 1) of the SFA, 1 had an iliac PTA, and 1 patient had a popliteal bailout stenting due to recoil after PTA. Follow-up included clinical examination at 6 weeks and after 1 year. Distal pressure measurements and duplex ultrasound were performed if indicated to the examiners’ discretion. If patients needed closer observation, the standard regime was subsided by shorter intervals of follow-up.
The 1-year data we collected were incomplete (41%); therefore, we crosschecked the medical records with the national records for data on amputation and death at the National Vascular Registry (24) until 1 January 2014. This ensured a valid 1-year status of 97% of patients (two patients were lost to follow-up).
Amputation-free survival was defined as avoidance of major amputation. Toe, ray, and distal foot amputations were considered minor amputations.
Statistics
Statistical analysis was performed using SPSS statistical software (SPSS version 19; SPSS, Inc., Chicago, IL, USA). Amputation-free survival and overall survival were evaluated using Kaplan–Meier statistics. Association between categorical variables was calculated using Fisher’s exact test for small samples. The p-values below 0.01 were considered statistically significant.
Results
Recanalization of at least one crural artery was obtained in all patients (n = 70). Two or more crural arteries were recanalized in 41% of the cases (n = 29). Distribution of lesions and treated arteries can be seen in Table 2. One patient (2%) experienced procedure-related complications, developing a groin hematoma demanding surgical evacuation, leading to prolonged wound problems. One patient (2%) presented acute abdomen and respiratory distress suspected of acute mesenteric ischemia, which led to exploratory laparotomy after having peripheral in situ bypass surgery subsequent to endovascular treatment. Two patients died within 30 days (peri-operative mortality; 3%) due to toxicity awaiting amputation (n = 1) and cerebral hemorrhage occurring after a minor amputation (n = 1).
Two patients were offered peripheral bypass within 30 days of PTA. The first patient had a PTA as a first-line treatment due to severe lesions in all crural vessels and poor runoff, which occluded after 1 week. Peripheral in situ bypass was then performed after surgical exploration of the dorsal pedal artery. The patient suffered severe complications after surgery and died within a year. The second patient had a PTA of the posterior tibial and fibular artery which occluded within a day; therefore, a peripheral in situ bypass was performed to the dorsal pedal artery. The patient remained amputation-free in the observation period.
A total of 15 major amputations were performed at a median of 20 months during follow-up (range: 0–41). In all, 11 were performed within the first year. A total of 21 minor amputations were reported, with 8 performed prior to revascularization. All patients had at least two diseased crural vessels. In all, 207 crural arteries were diseased, and in the 70 procedures, 103 BTK PTA treatments were performed.
Cumulative mortality after 1 and 2 years was 22% and 34%, respectively (Fig. 1). Amputation-free survival at 1 and 2 years of follow-up was 68% and 58%, respectively (Fig. 2).
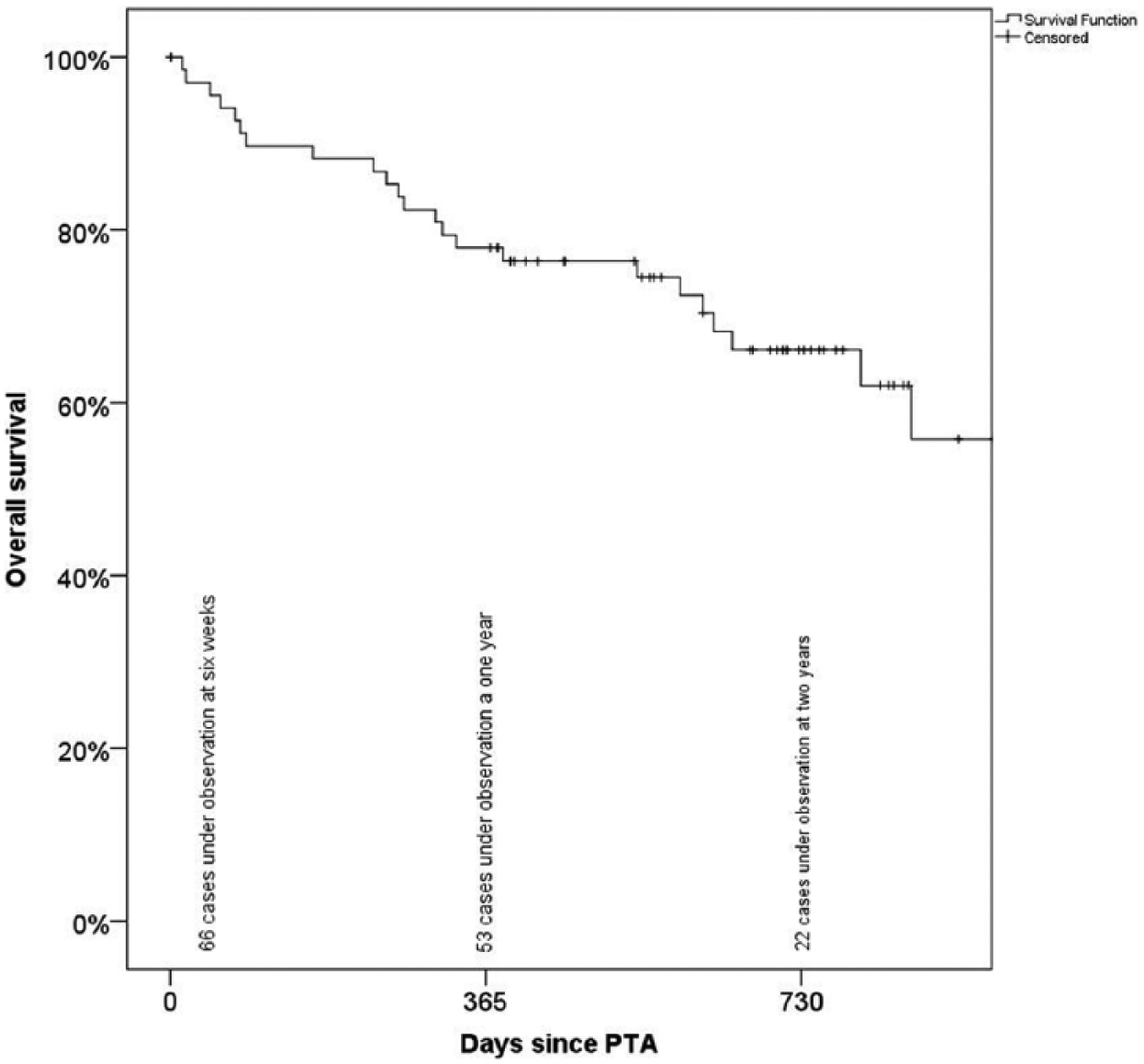
Kaplan–Meier curve showing overall survival.
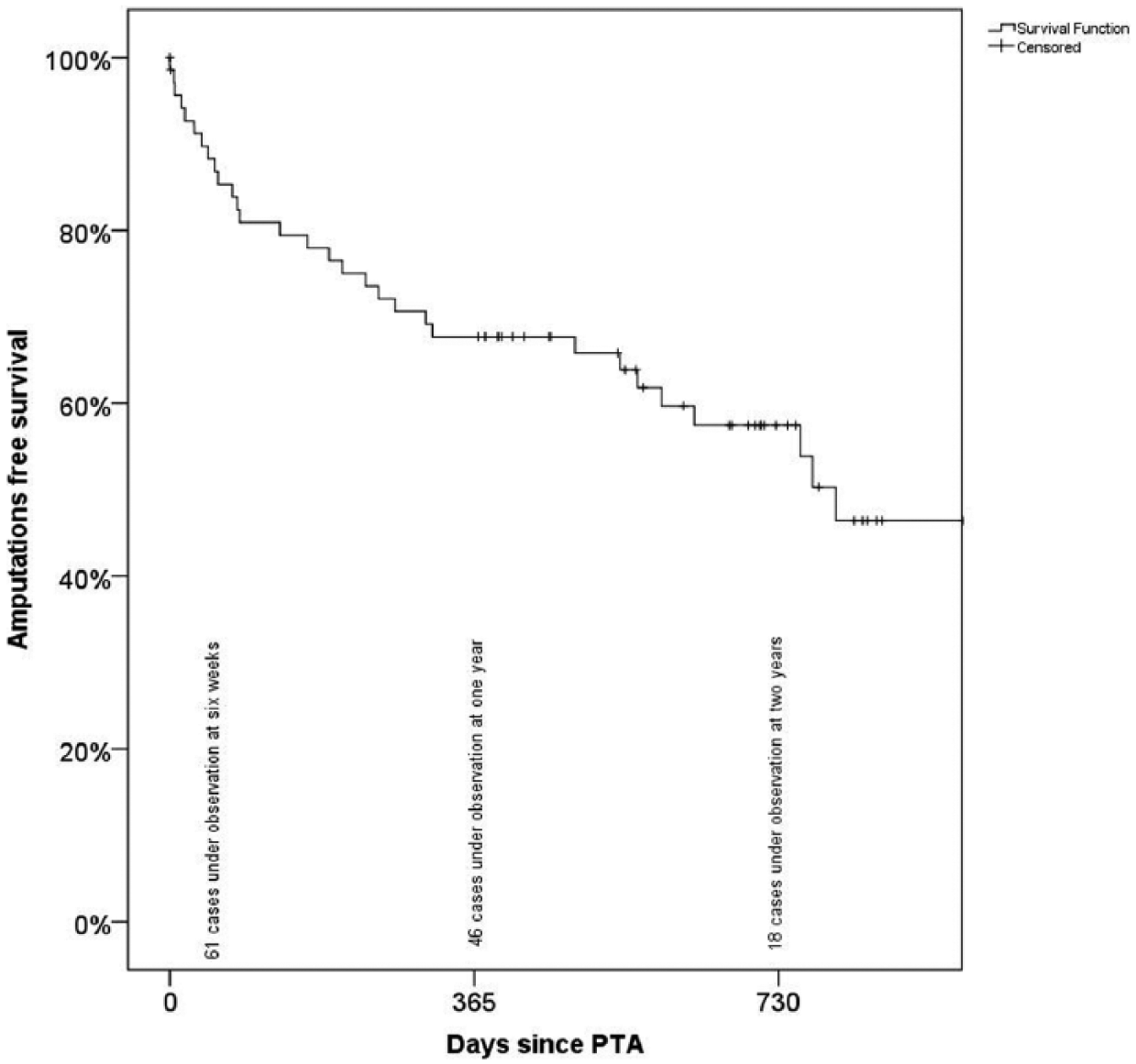
Kaplan–Meier curve showing major amputation-free survival.
Mortality at 1 year among major amputees was 36% and among non-amputees (n.s.) was 19%. We found no significant association between amputation regardless of location (both major and minor) and death at 1-year level (p = 0.044).
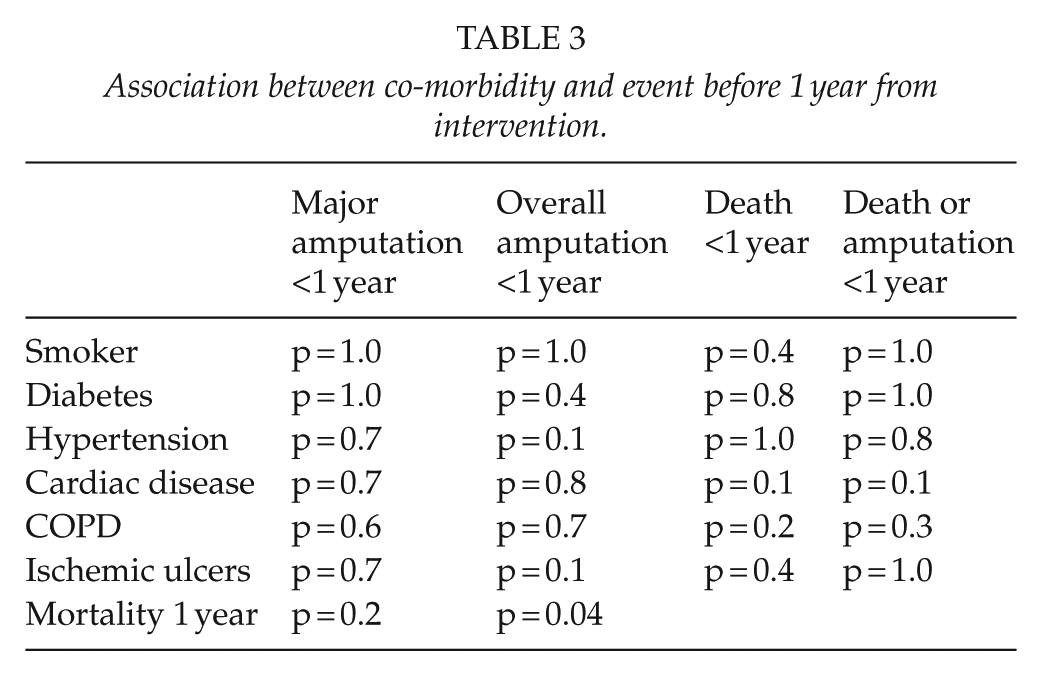
No association was found between diabetes, ischemic ulcers, cardiac disease, and history of smoking versus major amputation or overall amputation (Table 3). Furthermore, we found no significant association between outcome and number of treated arteries, nor which arteries were treated.
Association between co-morbidity and event before 1 year from intervention.
Discussion
The present series demonstrated the clinical outcome after crural angioplasty in patients with CLI. Outcomes were based on hard endpoints, that is, death and amputation since patency was not investigated systematically. Complications were infrequent, with only one instance that was directly associated with the endovascular procedure. This confirms the low complication rate reported in the literature (15). Critical ischemia is associated with a general poor prognosis for limb salvage and life expectancy. All patients with peripheral artery disease should be given statins and a platelet inhibitor. If intolerant to ASA, clopidogrel is advised. There is no solid evidence to guide the level of choice between platelet inhibitors. All patients in the series were medicated according to this protocol. The 1-year amputation-free survival in patients with critical ischemia receiving conservative treatment is only 51% (25, 26). In this study, intervention was aimed at reducing the level of ischemia in order to avoid major amputation. The obtained 1-year amputation-free survival of 68% is superior to best medical treatment only (19, 25). In contrast, peripheral bypass surgery in patients with critical ischemia indicated an amputation-free survival rate after 5 years of over 80% (7). Peripheral bypass was not a viable option in our study; therefore, a direct evaluation of “PTA first strategy and a surgery later strategy” was not feasible. In the two cases where peripheral bypass were performed, the cases were re-evaluated when the PTA-treated artery occluded and a new decision was made to try surgery. The risk of amputation increases according to the severity of crural lesions (27). We found no association between the number of recanalized crural vessels and amputation-free survival nor were crural interventions associated with amputations alone. These findings are not unexpected considering the modest sample size and heterogeneity of the patients. The 1-year mortality rate of 22% is in line with the current literature. This high mortality, as well as the association between overall amputation and death at 1 year, indicates the severity of CLI. Endovascular attempt was initiated under consideration that the risk superseded the possible gain of the open surgical procedure (28).
Freedom from amputation after 1 year is as high as 84% in the current literature (11, 29). However, most studies evaluate patients receiving subsequent treatment in order to keep the reconstruc-tion patent. The freedom from re-intervention is described as low as 54%. In our series, only one re-intervention was performed and two peripheral bypasses were attempted. Our population comprised patients in whom the ischemia was advanced to a degree where 11% had minor amputations performed prior to revascularization. The 1-year mortality in our study was expected and in line with the current literature. The long-term efficiency could not be evaluated at present time due to the short follow-up time.
We have presented a small retrospective single center study, and the results are thus limited. The follow-up period is short, but as last resort of intervention in severely ill patients, the primary goal was to investigate short-term outcome. Results are compared to literature as we have no comparator group.
At our facility, patients without the possibility of vascular intervention are referred to either local orthopedic department or a specialized wound department for further treatment, and follow-up is terminated. In the same period, 114 BTK peripheral bypasses were performed. However, comparing the outcome of these patients to our study group would possibly be confounded due to discrepancy in morbidity and severity of lesions. Furthermore, while all patients with CLI will not be suffering major amputation, selecting the ones who will without intervention can be daunting, and it would be an ethical challenge to undertake a randomized study of intervention versus best medical treatment, when means of treatment are available.
To further investigate the effect of BTK PTA, we suggest a prospective study with a longer follow-up period including data on wound healing, lesion size, site, endovascular tool (DEB vs non-DEB), and assisted patency. To show an increase in 1-year amputation-free survival from 70% to 80%, we suggest a multicenter effort as power analysis necessitates nearly 600 patients for randomization.
Conclusion
We found a 1-year major amputation-free survival of 68% and cumulative 1-year mortality of 22% in a group of patients with CLI who were not eligible for open vascular surgery.
For patients with end-stage PAD and CLI, who are not fit for surgery, BTK PTA is a safe procedure in relieving critical ischemia, reducing the short-term rate of a major amputation as opposed to best medical treatment alone.
Footnotes
Declaration of Conflicting Interests
The authors declares that there is no conflict of interest
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.