
Abstract
Background and Aims:
Large ventral hernias are often associated with physical, social, and health problems for the patient, and surgical repair remains a challenge. Open components separation has widely been applied to obtain closure of the midline and recently a minimally invasive technique has been introduced (endoscopic components separation). The effectiveness and safety of endoscopic components separation have been demonstrated in previous reports, whereas little is known about quality of life in these patients. With a focus on quality of life, we present the first patients from our center operated on with endoscopic components separation.
Material and Methods:
A total of 19 consecutive patients scheduled for open hernia repair with endoscopic components separation from October 2010 to June 2012 were included. All procedures included endoscopic components separation because of the hernia size. Demographic data, operative information, and postoperative complications were recorded. All patients completed two similar questionnaires regarding their function level, cosmetic satisfaction, analgesic medication, alcohol consumption, and self-estimated physical and mental health before and after the hernia repair. Patients were assessed as outpatient median 2 months and 16 months after operation for exclusion of hernia recurrence and completion of the postoperative questionnaire.
Results and Conclusions:
Operating room time was median 204 min and correlated significantly with the hernia size. A total of 21 postoperative complications occurred in 14 patients. The length of stay was median 6 days and correlated significantly with duration of the operation. Of these, 15 patients participated in late follow-up visit. Two patients experienced recurrent hernias. Postoperative function level, cosmetic satisfaction, and self-estimated physical and mental health improved significantly. Alcohol consumption was significantly reduced. Endoscopic components separation is a reliable method to repair large ventral hernias, although further studies are required to determine the exact benefits for endoscopic components separation hernia repair versus conventional hernia repair.
A large ventral hernia is often associated with major physical, psychological, and social problems for the patient. Repair of large ventral hernias is a significant challenge for the surgeon, and there are still controversies regarding the optimal surgical technique. The overall goal of ventral hernia repair is to restore the abdominal wall integrity and function, maintain a closure with physiologic tension, prevent hernia recurrence or evisceration, and esthetically improve body contour (1, 2).
Open components separation (OCS) has been widely used since 1990 (3) as a supplementary technique for repair of complex ventral hernia to provide mediatization of the abdominal rectus muscles following sharp division of both external oblique aponeuroses. The technique typically allows tension-free closure of the midline, but the tradeoff is an increased rate of wound complications due to impairment of the blood supply to the undermined skin flaps. Components separation (CS) has undergone modifications, and today the procedure is increasingly undertaken with minimally invasive techniques in many centers.
Lowe et al. (4) introduced endoscopic components separation (ECS) in 1997 and described the application of a balloon technique for subcutaneous dissection and external exposure of the external oblique aponeurosis, which was divided along the semilunar line with electrocautery. Further improvement and minimization of the technique was done by Rosen et al. (5) by internal exposure of the external oblique in combination with avascular separation of the external and internal oblique components by dissection with an endoscopic balloon, thus avoiding subcutaneous undermining of the skin flaps. ECS is associated with lower rates of wound complications (6, 7) because only limited subcutaneous dissection is undertaken, thus preserving the blood supply from the epigastric vessels to the skin.
Many reports have demonstrated the effectiveness and safety associated with the ECS technique for repair of large midline ventral hernias (5, 6, 8–10) as indicated by the rates of recurrent hernia and postoperative complications. In contrast, there are no corresponding publications on quality of life (QOL) in these patients following repair of their hernia with this new technique. With a focus on QOL before and late after surgery, we present the first patients from our center with giant ventral hernia operated on with ECS.
Material and Methods
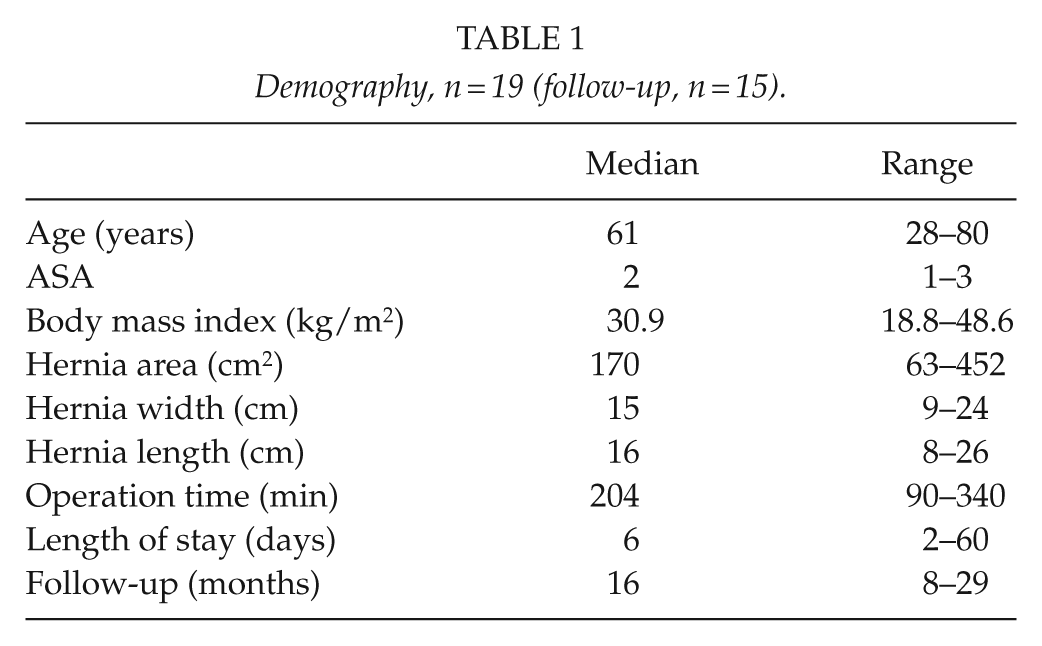
A cohort of 19 patients scheduled for hernia repair including uni- or bilateral ECS during the period October 2010 to June 2012 was included in the study (Table 1). The ECS procedures were undertaken in accordance with the technique described by Rosen et al. (5). All patients were previously subjected to a laparotomy through a midline incision and were not candidates for standard open or laparoscopic hernia repair because of the hernia size.
Demography, n = 19 (follow-up, n = 15).
The patients completed a questionnaire regarding their health and function level before and after the hernia repair. Self-estimated hernia gravity, pain, impairment of movement, discomfort, fatigue, and general hernia impairment on overall QOL were measured using a numeric rating scale (NRS), where 0 and 10 indicated no symptoms and maximal values, respectively.
Using a verbal rating scale (VRS), hernia-related pain, gravity, and mobility under eight different activity modes (laying down, bending forward, sitting down, doing daily activities, coughing, walking, walking on stairs, and exercise) were registered (Table 2). The median observation obtained from the eight conditions was then reported for each patient.
Verbal rating scale.
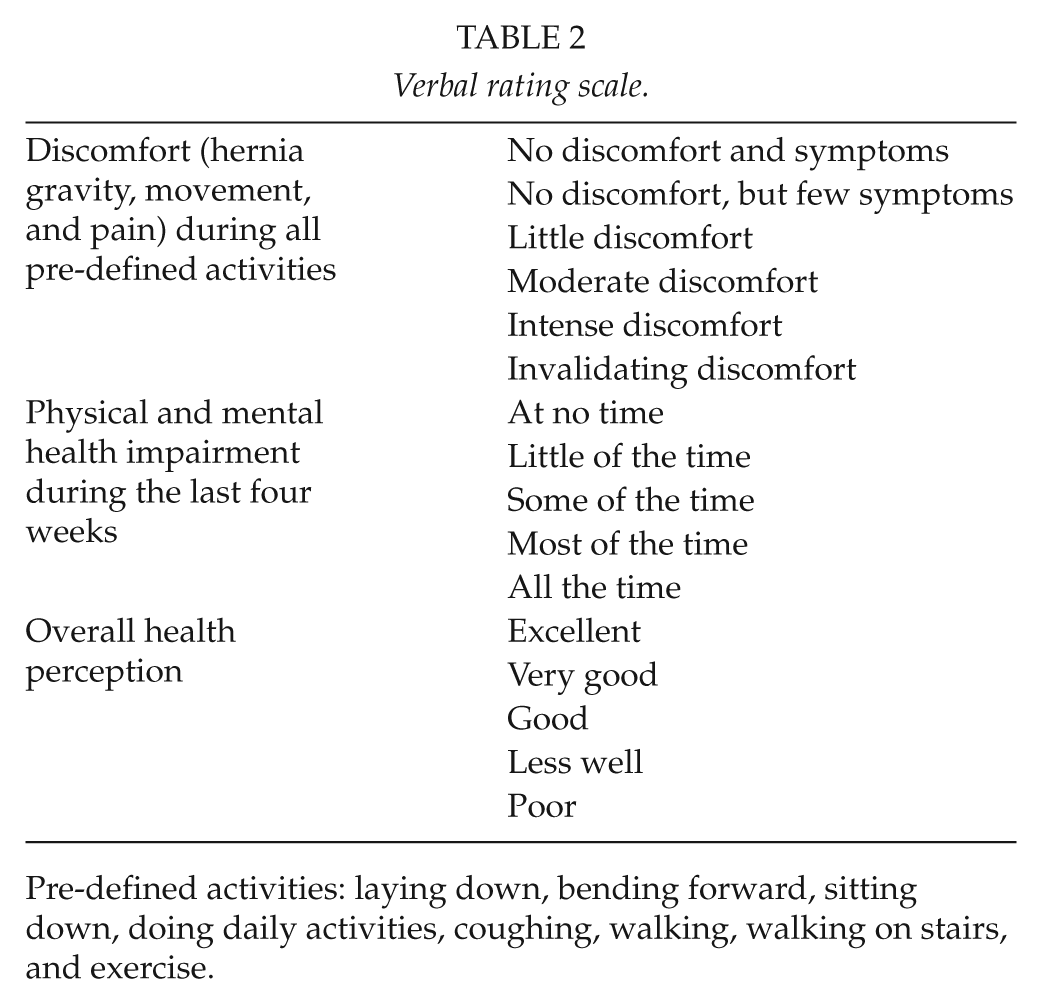
Pre-defined activities: laying down, bending forward, sitting down, doing daily activities, coughing, walking, walking on stairs, and exercise.
A VRS (Table 2) was also used for self-estimated impairment of physical and mental health as well as overall health status. Impairment of self-estimated physical health was defined as “physical pain during the last four weeks hampering daily work both in-and out-house,” while impairment of mental health was “feeling sad/depressed during the last four weeks.” Overall health status was assessed by “the general physical and mental perception at the time of completing the questionnaire.”
Moreover, we registered analgesic medication, alcohol consumption, and self-rated pre- and postoperative cosmetic satisfaction (NRS 0–10). The same three surgeons working together in teams of two performed all the operations. The area of the fascial defect was calculated as length × width × π/4. Postoperative complications included surgical site infection, seroma, skin necrosis, wound dehiscence, skin fistula, or other postoperative infections.
All patients had a postoperative assessment by the primary surgeon median 2 months after the hernia repair to assess postoperative complications. Moreover, patients were invited for a second outpatient visit median 16 months after the index herniotomy for exclusion of hernia recurrence and completion of a questionnaire similar to the preoperative version. General satisfaction with the operation was estimated with the question: “Did the operation live up to your general expectations?” and “would you recommend this procedure to others?” Operative information, postoperative complications, and demographic data were recorded and analyzed using the SSPS software version 20.0.0. Wilcoxon test was applied for paired evaluations, and correlation was analyzed with Spearman test. A p-value less than 0.05 was considered statistically significant.
Results
Uni- and bilateral ECS were undertaken in 1 and 18 patients, respectively. Closure of the linea alba with mesh reinforcement was done by open technique in 17 and by laparoscopic access in two of the patients. The procedures were open repair with an intraperitoneal onlay mesh (IPOM) (Bard Composix Kugel® mesh; Bard, Cranston, RI, n = 11), open repair with a retrorectus mesh placement (Ultrapro® mesh; Ethicon, Somerville, NJ, n = 3; Vypro II® mesh; Ethicon, Somerville, NJ, n = 2; Parietene Progrip® mesh; Covidien, Mansfield, MA, n = 1), and laparoscopic IPOM repair (Bard Composix LP® mesh; Bard, Cranston, RI, n = 2). Panniculectomy before skin closure was done in all patients. Operative time was median 204 min and correlated significantly with the area of the fascial defect, r = 0.729, p = 0.002.
A total of 14 patients experienced a total of 21 postoperative complications (Table 3). One patient underwent early reoperation with re-fixation of an intraperitoneal mesh (Bard Composix Kugel) that was partially loose. Skin dehiscence occurred in three patients and was managed conservatively in two and by re-closure in one patient. Of these, 10 patients underwent antibiotic treatment for postoperative infections (Table 3). Length of stay (LOS) was median 6 days and correlated significantly with duration of the operation (r = 0.745, p < 0.0005) but not with hernia size (r = 0.509, p = 0.053). Two patients developed mesh-related cutaneous sinus after 4 and 6 months requiring complete removal of all e-polytetrafluoroethylene (ePTFE) mesh material (Bard Composix Kugel). Both patients received a new biologic mesh (Permacol, Covidien).
Postoperative complications.
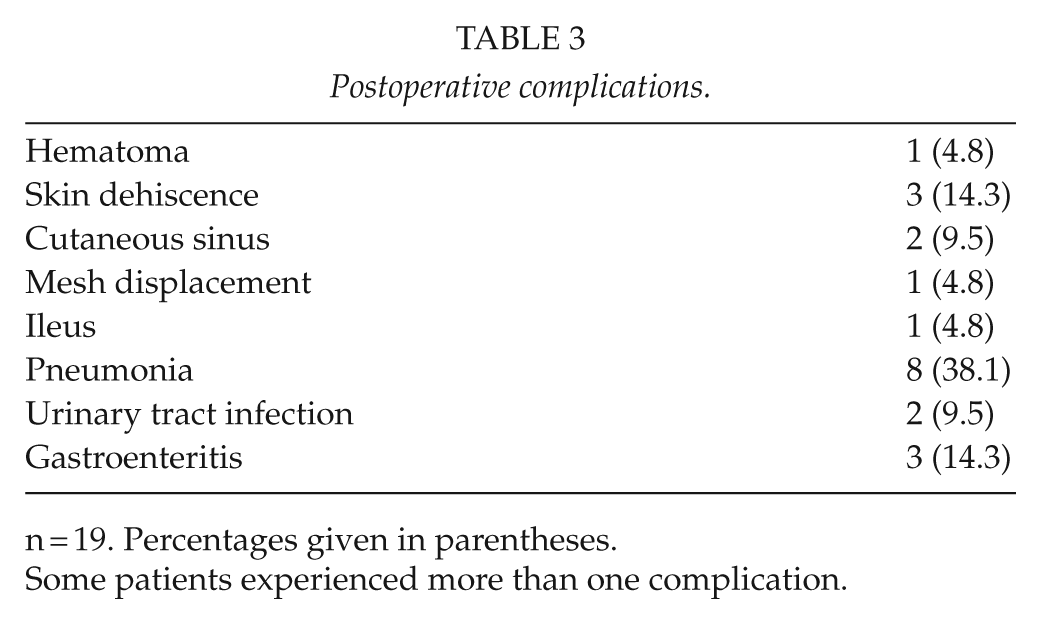
n = 19. Percentages given in parentheses.
Some patients experienced more than one complication.
A total of 15 patients were available for the late follow-up visit following exclusion of 4 patients (2 deaths not related to the primary operation and 2 patients unwilling to participate in the study) median 16 months (8–29 months) postoperative. Recurrent hernias after 13 and 29 months were diagnosed in two patients both of whom had undergone laparoscopic repair, including closure of the midline and an IPOM technique.
The patients reported postoperative improvements of all pre-defined outcomes (Fig. 1) as well as physical, mental, and overall health perception (Fig. 2). Significant improvement following the hernia repair was also reported for the experience of hernia gravity, movement, and pain (preoperative median “moderate discomfort” to postoperative median “few symptoms, but no discomfort” (p < 0.0005) during all given activities. Cosmetic dissatisfaction decreased from median 10.0 (interquartile range (IQR): 8.75–10.0) before surgery to median 5.5 (IQR 0.75–10.0) after surgery, p = 0.011.
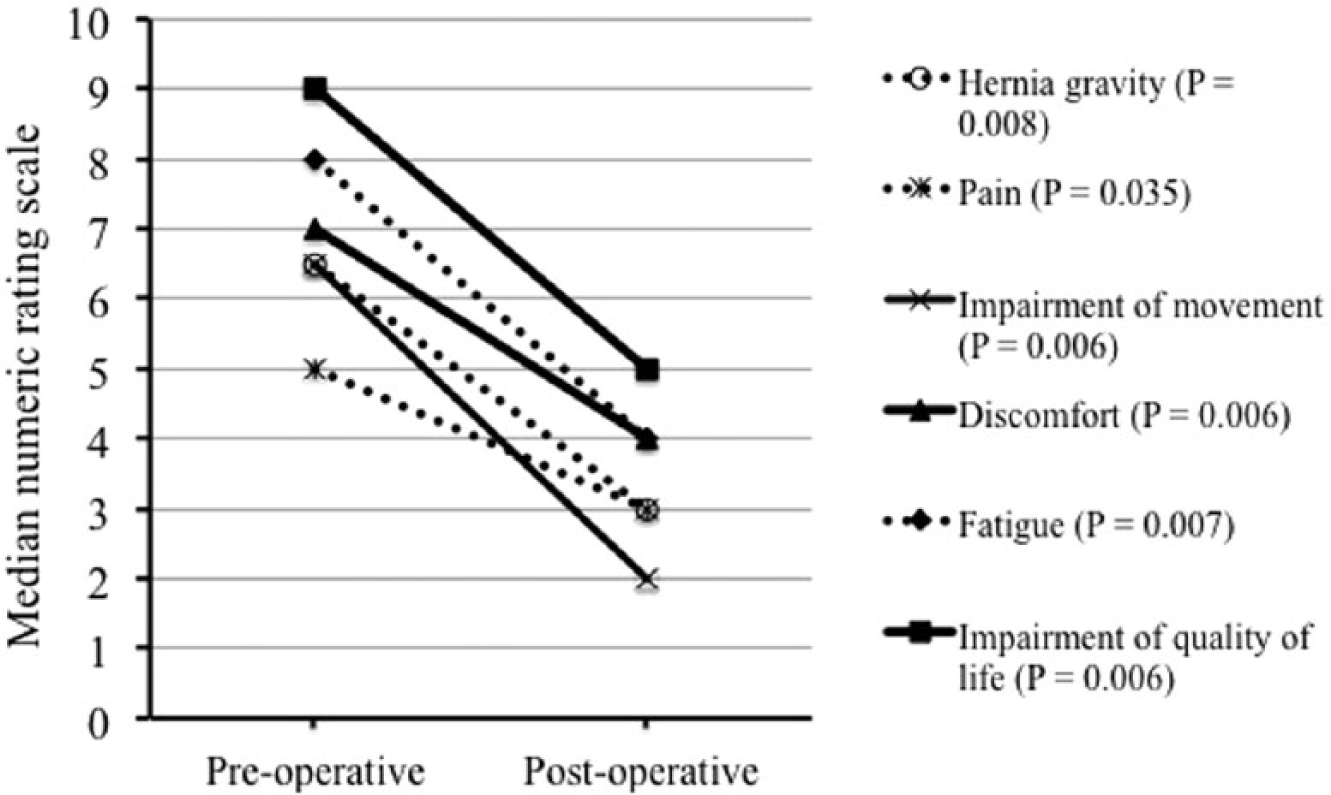
Self-estimated assessment of hernia-related pre- and postoperative outcomes (numeric rating scale 0–10).
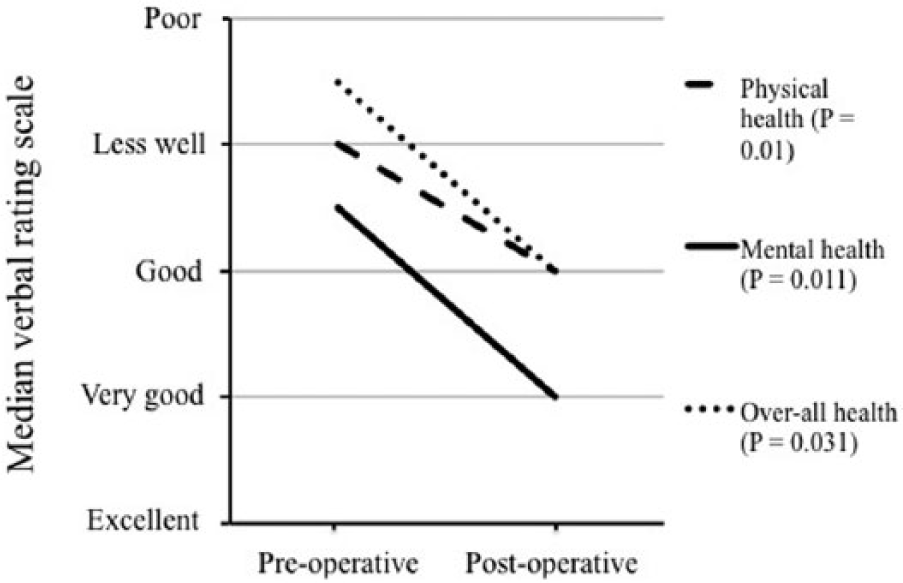
Self-estimated assessment of physical, mental, and overall health perception (verbal rating scale).
A total of 11 patients did not report any change in their postoperative consumption of analgesics as compared with their preoperative administration. Three and one patient reported an increased and a reduced consumption, respectively. A significant reduction of alcohol consumption was reported from a mean 7.3 units before surgery to 4.3 units per week at the last follow-up visit (p = 0.024).
Seven patients (47%) reported that their expectations regarding the operation were fulfilled, six (40%) did not, and two (13%) were uncertain. Nine patients (60%) would recommend this specific procedure to other patients with a similar condition, two (13%) would not, and four (27%) were ambiguous.
Discussion
Open hernia repair including ECS for reconstruction of the linea alba caused a significant improvement of QOL and self-perception of body contour, although immediate postoperative morbidity was not negligible. Since the introduction of CS in 1990, modifications of the technique have emerged including various ways to perform the division of the lateral aponeurotic component. Moreover, the surgeon has a choice between a nonmesh repair and mesh reinforcement with either a synthetic or biological material (11). The Ventral Hernia Working Group (11) advocates the use of mesh as the recurrence rate is reduced from 18%−62% to 2%−32%. The wide ranges are partly explained by the varying sizes of hernias in the series (10, 12).
Porcine and cadaver model studies have shown that ECS results in only 85% of the release obtained by OCS (12, 13). Despite of this, the release that is obtained by ECS is often sufficient to allow closure and reconstruction of linea alba. The advantages of ECS as compared with OCS include a lower rate of skin ischemia, intraoperative bleeding, and seroma (6, 8, 9, 14, 15). Wound complications occurred in 30%−50% of the patients subjected to OCS versus less than 30% after ECS. This difference was most pronounced for major wound complications as defined by wound morbidity that required operative debridement (6, 14).
Postoperative infection excluding surgical site infection after repair of large ventral hernia including CS is reported in 10%−40% of the patients (6, 16–18). The 38% rate of postoperative pneumonia and 9% rate of urinary tract infections in the present series made us introduce routine prophylactic chest-physiotherapy from postoperative day 1 and early removal of urethral catheters. Moreover, only nonsmokers undergo elective repair of giant hernias in our center.
A comparison between ECS and OCS demonstrated that the cost associated with ECS was less than for OCS despite the increased direct costs of utensils for performance of ECS (14). This finding was mainly due to fewer wound complications and therefore fewer postoperative outpatient visits in the ECS group.
Two patients (13%) were diagnosed with recurrent hernia after 13 and 29 months. In previous publications, the hernia recurrence rate after OCS ranged between 17% and 29% after mesh repair and between 27% and 61% without mesh repair (6, 8, 9, 18, 19). Following ECS, Tong et al. (8) reported a 17% recurrence rate without mesh, while Harth and Rosen (6) reported 27% rate following mesh reinforcement. Direct comparison of these rates should be avoided due to diversity in follow-up time and patient demographics.
The present series included the first patients subjected to ECS at our center, and it is likely that the immediate postoperative outcome is under influence of a learning curve. Because ECS is a rather new technique, we found it necessary to present our early results when the first follow-up data were available. To statistically address the low number of patients in our study, we chose to use paired analyses letting each patient serve as his or her own control. Due to centralization of operations for giant ventral hernia in our region, we have now performed more than 100 procedures for giant ventral hernia including the ECS technique.
Due to the implementation of ECS as a new technique in our department, we tested different kinds of mesh products. Experience gained from the first patients prompted us to apply a self-adhering synthetic large pore non-ePTFE based mesh product (Parietex Progrip®, Covidien) and fixate this in a retrorectus position by an open Rieves-Stoppa technique.
Median LOS in the present trial was 6 days, which is comparable with data from other groups (6, 9, 10, 14). There is controversy as to whether ECS diminishes LOS as compared with OCS (6, 9, 14). We found a close correlation between operative time and LOS suggesting that the surgical challenge of a complicated hernia rather that hernia size per se predicted postoperative LOS.
One study reporting on QOL as assessed with the Carolinas Comfort Scale in two comparable groups did not show any difference between open ventral hernia repair and open ventral hernia repair in combination with CS (20). Liang et al. reported on 122 patients comparing open and laparoscopic ventral hernia repair. After laparoscopic repair, 25% of the patients dissatisfied with the result, 26% had poor functional status, and 17% reported chronic abdominal pain. Decreased patient satisfaction was associated with chronic pain and poor cosmetic result (21). De Vries Reilingh et al. (18) reported on postoperative QOL using the 36-Item Short-Form Health Survey (SF-36) questionnaire in 39 patients who underwent OCS. Nearly all patients (97%) reported improvement and were satisfied with the postoperative situation compared to their preoperative scoring. Preoperatively, the patients had an average or inferior score regarding mental and general health perception, pain, vitality, and physical/social functioning as compared to the general population. No postoperative scores compared to the general population were reported. A recent study reported the results from 13 patients undergoing repair of large hernias by an open Rives-Stoppa repair combined with posterior compartment separation (transversus release). Interestingly, objectively measured abdominal wall function was significantly improved and reflected by enhancement of QOL as demonstrated in the present series (22).
Liang et al. (21) reported an association between reduced functional status and alcohol abuse in patients after laparoscopic ventral hernia repair. We did find a significant reduction in the weekly alcohol consumption when comparing the pre- and postoperative values, which may partly be explained by the reported improvement of mental and physical health.
During the interview at the follow-up visit, patients expressed general satisfaction with the preoperative information about possible surgical complications. However, many of the patients called for more detailed preoperative information regarding postoperative pain, vitality, and the risk of continued problems in physical and social functioning. This is illustrated by the fact that 40% of the patients reported that the result of the operation did not reach their general expectation despite their reported improvement of physical and mental health as well as cosmetic satisfaction after the operation. This finding underscores the importance of a preoperative alignment of expectations between patient and surgeon.
It is feasible to obtain closure of the midline with a minimally invasive technique combining ECS with open mesh repair of large ventral hernias. This procedure results in improvement of QOL and cosmesis, but further research is warranted to reduce a considerable incidence of postoperative morbidity. Further research is warranted to address potential differences between ECS and OCS with respect to postoperative complications, QOL, hernia recurrence, and costs.
Footnotes
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Ethical approval
The study was approved by the local data registration authorities (BBH-2014-017/02717). Approval from the Ethics Committee was not required.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.