
Abstract
Introduction:
Bile duct injuries occur rarely but are among the most dreadful complications following cholecystectomies.
Methods:
Prospective registration of bile duct injuries occurring in the period 1992–2013 at a tertiary referral hospital.
Results:
In total, 67 patients (47 women and 20 men) with a median age of 55 (range 14–86) years had a leak or a lesion of the bile ducts during the study period. Total incidence of postoperative bile leaks or bile duct injuries was 0.9% and for bile duct injuries separately, 0.4%. Median delay from injury to repair was 5 days (range 0–68 days). In 12 patients (18%), the injury was discovered intraoperatively. Bile leak was the major symptom in 59%, and 52% had a leak from the cystic duct or from assumed aberrant ducts in the liver bed of the gall bladder. Following the Clavien–Dindo classification, 39% and 45% were classified as IIIa and IIIb, respectively, 10% as IV, and 6% as V. In all, 31 patients had injuries to the common bile duct or hepatic ducts, and in these patients, 71% were treated with a hepaticojejunostomy. Of patients treated with a hepaticojejunostomy, 56% had an uncomplicated event, whereas 14% later on developed a stricture. Out of 36 patients with injuries to the cystic duct/aberrant ducts, 30 could be treated with stents or sphincterotomies and percutaneous drainage.
Conclusion:
Half of injuries following cholecystectomies are related to the cystic duct, and most of these can be treated with endoscopic or percutaneous procedures. A considerable number of patients following hepaticojejunostomy will later on develop a stricture.
Introduction
Laparoscopic cholecystectomy is one of the most commonly performed surgical procedures and since its introduction in the late 1980s has been the standard procedure for the management of symptomatic gall bladder stones or acute cholecystitis. Although there are major benefits related to the procedure, such as reduced pain and shorter hospital stay, laparoscopic access also has a downside, as in some publications it is associated with a higher incidence of bile leaks and injuries to the common bile ducts than was observed in the open cholecystectomy era (1, 2). So far, this has not been clearly documented, as some studies have shown an increased risk (3, 4), whereas others could not verify this (5–7).
The consequences of bile duct injuries might have severe consequences for some of the patients. Apart from early postoperative complications, there is also a risk of long-term sequelae as strictures of the common bile duct and repeated attacks of cholangitis. In addition, such injuries represent a vast economic burden to the society (8) and also represent a high rate of medico-legal claims (9).
The treatment of bile duct injuries has changed since the introduction of laparoscopic surgery. Most bile leaks are now treated with endoscopic procedures like stents and endoscopic sphincterotomy, whereas the more severe cases will still need a repair of the common bile duct (10, 11). Despite this, a rather high proportion of the patients will still have strictures and episodes of cholangitis (12).
Following the introduction of laparoscopic surgery, several registries were established in order to monitor the evolvement of possible bile duct injuries. Most of these aimed to evaluate the incidence and risk factors for complications, whereas rather few have looked into therapy and consequences of the injuries (3, 4, 7). At Haukeland University Hospital, we initiated a prospective registration of bile duct injuries in 1992. The purpose of this article was to evaluate the incidence and risk factors and analyze treatment options for this patient group.
Patients and methods
This series represents a prospective database of all patients who developed bile leakage or bile duct injuries from 1992 to 2013 and were treated at Haukeland University Hospital. The hospital is a tertiary teaching hospital in Western Norway as well as a local hospital for the Bergen area. According to the agreed policy for this health region, all major bile duct injuries should be treated at the university hospital, whereas bile leaks from cystic duct and mild diseases should be treated at local hospitals. None of the hospitals in the catchment area used intraoperative cholangiography (IOC) routinely during the study period. During the 14-year period 1999–2013, laparoscopic cholecystectomies were performed on 5013 patients in Hordaland county, and this forms the basis for calculation of incidence of bile duct injuries. These data were obtained from the Norwegian Patient Register. Data about bile duct injuries were prospectively retrieved from the hospital’s patient files and entered into a database.
Severity of injury was classified according to Dindo et al. (13) and type of injuries according to Strasberg (14). Apart from a follow-up during the first postoperative months, there were no regular planned visits. All patients were traced until death or were censored by 31 December 2013. The date of death was obtained from the hospital’s patient administrative system.
Data were analyzed by frequency tables and cross-tabulation as found appropriate by the statistics program IBM SPSS version 21. The Regional Ethics Committee (REC) of Western Norway considered, on a general basis, the study as a quality assurance study that should not be evaluated by them.
Results
During the study period, 67 patients—20 men and 47 women—were included in the database. The median age was 55 (range 14–86) years. Incidence data for Hordaland county were available for the period 1999–2013. Out of 5013 patients having a cholecystectomy during that period, 44 patients (0.9%) had a bile leak or injury to the bile ducts and 18 patients (0.4%) had an injury to the common bile duct or right hepatic duct.
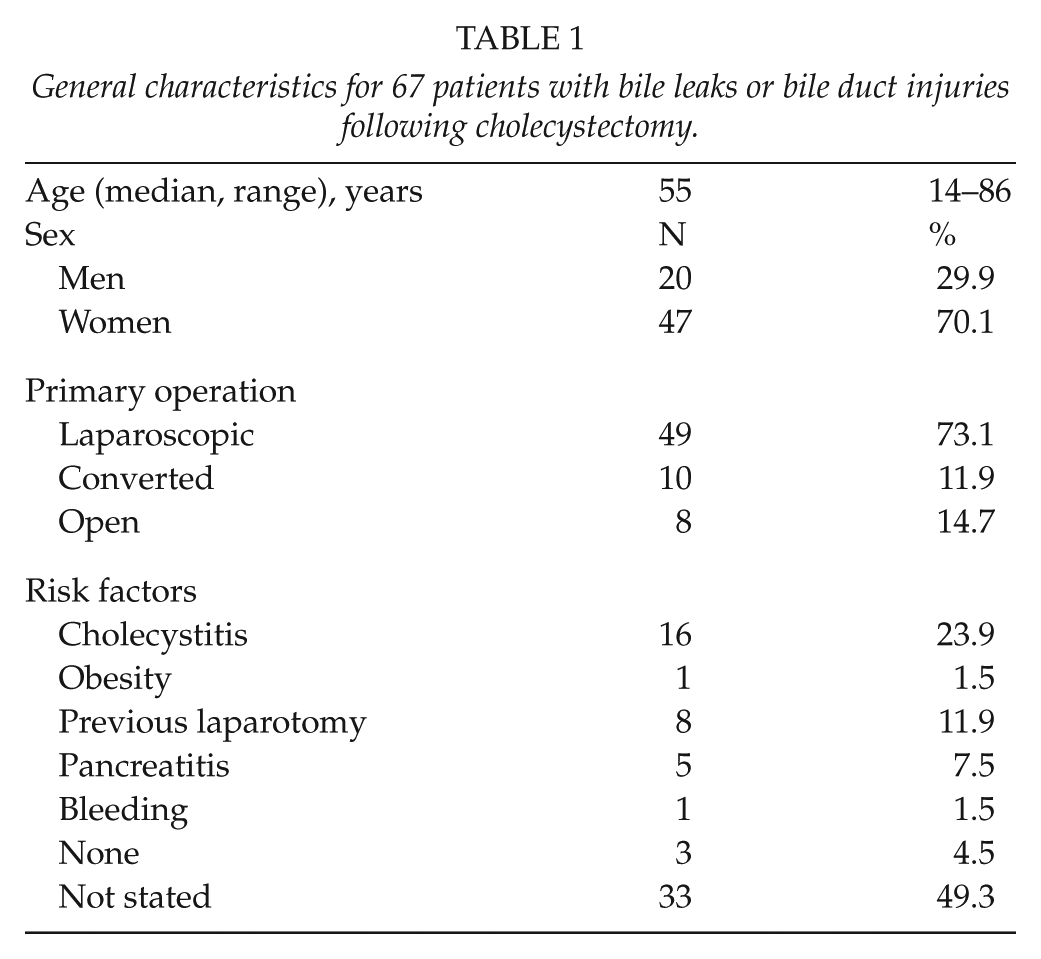
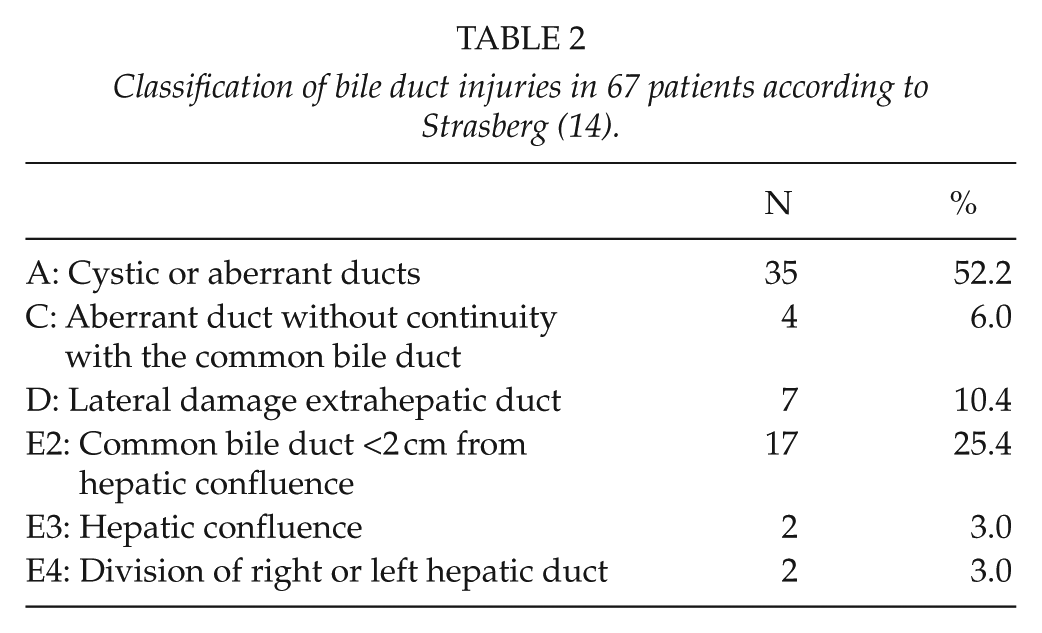
A general overview of patient characteristics is shown in Table 1. A total of 26 patients (38%) had their primary operation at Haukeland University Hospital; others were transferred from local hospitals in the region. Median delay from injury to therapy was 5 days (range 0–98 days). In 11 patients (16%), the injury was discovered intraoperatively, whereas 90% were treated within 3 weeks. Difficult dissection due to previous cholecystitis was stated in 24% of the cases. Bile leak was the major symptom in 60% of the patients, whereas 13% had peritonitis or generalized septicemia. As for injured organ, 30 patients had a leak related to the cystic duct, either a laceration or an imperfect closure of the duct. Six leaks were assumed to be related to aberrant ducts (Luschka’s ducts), although this was difficult to prove. In 31 patients, there was an injury to the common bile duct, including the right hepatic or a right segmental duct (Table 2). When the common bile duct was injured, 14 appeared as leaks or peritonitis, whereas 6 had signs of obstruction.
General characteristics for 67 patients with bile leaks or bile duct injuries following cholecystectomy.
Classification of bile duct injuries in 67 patients according to Strasberg (14).
Severity of injury was classified according to Clavien–Dindo. Of the injuries, 39% were classified as IIIa, 45% as IIIb, 10% as IV, and 6% as V. Follow-up for patients surviving the postoperative period was 3 months to 20 years (median 6 years).
Table 3 shows re-operative procedures by injured organs. Of the 36 patients with cystic duct problems or aberrant ducts, 30 could be treated with endoscopic procedures and/or percutaneous drainage, whereas 6 patients had to undergo an open procedure with closure of the cystic duct or T-tube drainage. In two of these, severe general peritonitis was the indication for operative treatment. In three patients, we found common bile duct stones that were subsequently removed by endoscopic retrograde cholangiography (ERC) and probably were partially responsible for leakage from the cystic duct. During the last decade, all patients with cystic duct problems were treated endoscopically.
Therapeutic procedures in 67 patients undergoing bile duct injuries/leaks following cholecystectomy.
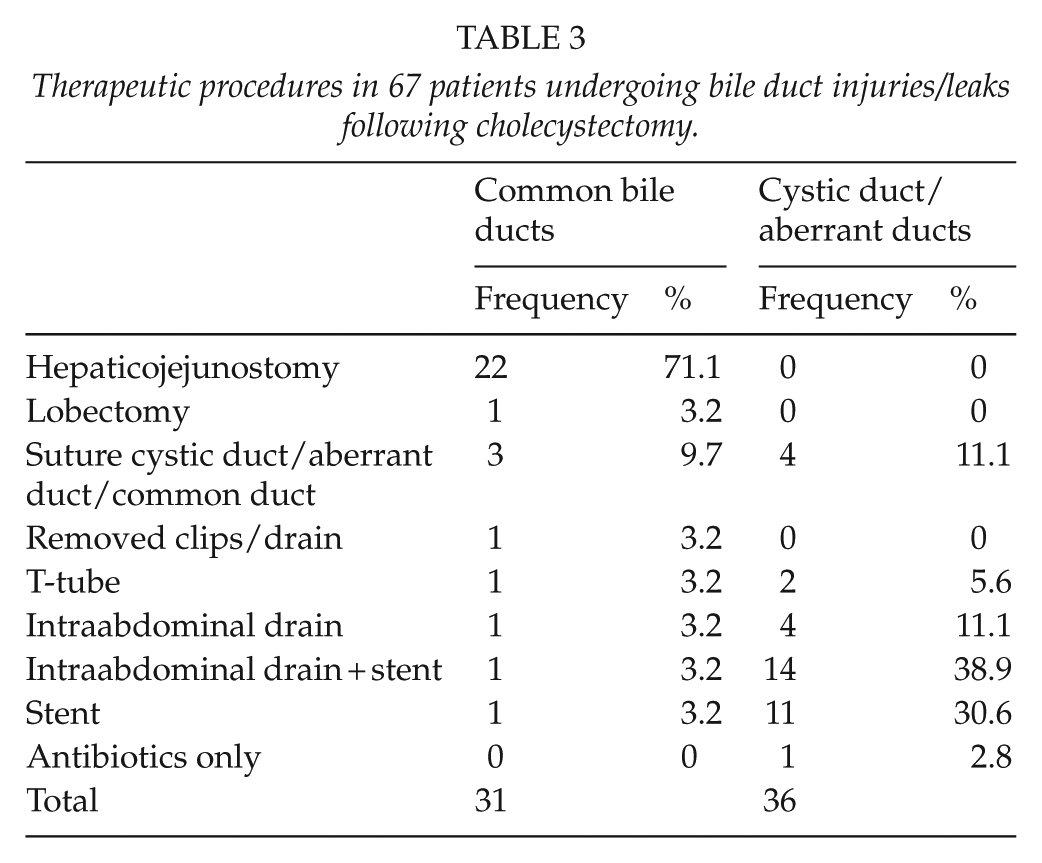
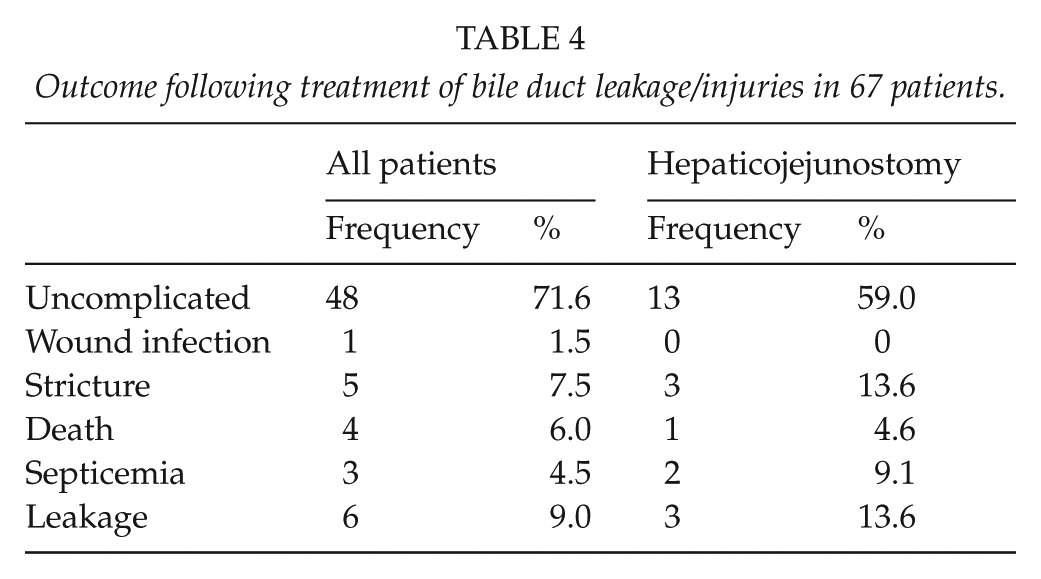
Of the 31 patients with damage to the common bile ducts, 74% had hepaticojejunostomies or hepatic resection (Table 3). For the whole patient series, we found that 47 out of 67 patients (70%) had no postoperative problems or sequelae. In patients treated with hepaticojejunostomies, 13.6% developed a stricture later on (Table 4).
Outcome following treatment of bile duct leakage/injuries in 67 patients.
Four patients died following their bile duct injuries. A 69-year-old woman had a tangential injury to the common bile duct that was discovered during the primary laparoscopic operation and repaired with a single suture. Two days later, she developed a minor segmental gangrene of the small bowel. She underwent a resection but died 2 weeks later following multiple organ failure. A 71-year-old woman with severe comorbidity had a leak from what was assumed to be an aberrant bile duct. She had a drainage procedure 2 days later but died during the same day following sudden cardiac arrest. A 76-year-old man had an injury to the common bile duct and a severe bleeding from the cystic artery as well as a major defect in the duodenal bulb. He was treated with a hepaticojejunostomy and gastric resection and had postoperatively several bleeding episodes that were treated endoscopically. The patient died during the postoperative course 40 days later due to multi-organ failure. The last patient was a 74-year-old woman with an imperfect closure of the cystic duct. Due to postoperative leak and peritonitis she underwent an open operation and closure of the duct. She died from septicemia 1 day later.
Discussion
The main findings in this study were that more than 50% of bile duct injuries or leaks following cholecystectomy were related to the cystic duct or assumed aberrant bile ducts in the liver bed of the gall bladder. This is in the same order as was found in an extensive American study comprising 83,000 patients where about 60% of the leaks were related to the cystic duct (5). As many as 12% of the operations in our series were open cholecystectomies and another 15% were conversions from laparoscopic to open surgery. The reason for this might be that the hospitals have a rather conservative attitude toward recommending operative treatment for gall bladder stones as well as acute cholecystitis. As a consequence, more patients have gall bladders considered difficult to remove during laparoscopic surgery. In addition, most of the open procedures were performed in the first years of the study period.
The reported frequency of bile duct injuries varies considerably in published studies (3, 4, 15). Retrospective studies might contain selection bias, thereby giving a too low incidence of injuries. In a prospective Swedish registry, the frequency of bile duct injuries was reported to be 1.5% which is much higher than the usually stated frequency of 0.2%–0.9% (16). In our series, we found a frequency of 0.4% injuries of the main bile duct and 0.9% when cystic duct problems and aberrant ducts are included.
Risk factors for bile duct injuries (BDIs) are assumed to be related to age, sex, acute cholecystitis, and impacted gallstone within the Hartmann’s pouch. Anomalies and anatomical variations of biliary ducts or vascular system are not uncommon and represent operative challenges and looming sources for operative complications. In our series, chronic cholecystitis and previous laparotomy with adhesions were the most commonly reported postoperative problems encountered.
The role of IOC in order to reduce the occurrence of bile duct injuries has been extensively debated (3, 16–18). The reason for performing IOC might be to avoid bile duct injuries as well as discovering stones in the common bile duct. In our series, IOC was rarely performed, as laparoscopic exploration of the common duct is not an option in this health region, due to an excellent endoscopic retrograde cholangiopancreatography (ERCP) service. It should also be noted that more than 50% of the injuries were related to the cystic duct and IOC would not prevent this. The conclusions of the published studies related to IOC are also conflicting, as only half of them show a benefit from IOC.
Iatrogenic injuries to the common hepatic duct or right hepatic duct with side branches are normally severe requiring operative management. Following complete division of the common bile duct, there are mainly two options for repair: direct anastomosis between the cut ends or hepaticojejunostomy with a Roux-Y limb. Most authors consider the last option as the most appropriate method (10, 19). This was also the main policy at our department. The outcome after hepaticojejunostomy is generally fair, with strictures as the most severe long-term challenge. Following systematic literature search, it has been concluded that there is only limited evidence from clinical studies to support specific recommendations as for treatment of bile duct injuries (15). As for primary versus late repair of injuries, this has been a topic of different opinions. Some recommend repair as soon as possible, whereas others advocate a “wait and see” approach for up to 3 months in order to obtain dilatation of the bile ducts, thereby being able to make an anastomosis more easily (20, 21).
Recurrent cholangitis as a consequence of postoperative strictures is commonly found following surgical repair of the common bile ducts (22). In addition to a well-timed planned operation, there might be several reasons for the development of strictures, like technical failures during reconstruction, unawareness of constrained blood supply, or extensive damage making anastomoses difficult. Treatment of postoperative strictures should also be individualized, and balloon dilatation might be a good option for many patients (23).
The consequences of a major bile duct injury might be severe and may alter a patient’s perceived quality of life (24). In general, it is found that the long-term quality of life is reduced following bile duct injuries compared to all patients undergoing laparoscopic cholecystectomy (25). In a study from Poland, Jablonska et al. (26) found that quality of life was better in patients undergoing end-to-end anastomoses compared to hepaticojejunostomies.
As four of our patients in this small series died in the course of bile duct injuries, this should focus on the severity of these lesions. This is especially relevant in elderly patients who will tolerate postoperative sepsis and reoperations badly. It is important to act immediately when bile leaks occur. Whether drainage should be performed percutaneously or endoscopically is, however, still debated (11, 27). In our series, most patients could be treated with endoscopic procedures, which was also the conclusion in a paper by Pitt et al. (28).
In conclusion, bile duct injuries are relatively uncommon following laparoscopic cholecystectomy. About 50% of the injuries are related to the common bile duct, and these should be centralized to hospitals familiar with major hepatobiliary surgery. Strictures following hepatojejunostomies are still a major concern.
Footnotes
Acknowledgements
Data from the Norwegian Patient Register have been used in this publication. The interpretation and reporting of these data are the sole responsibility of the authors, and no endorsement by the Norwegian patient register is intended nor should be inferred.
Declaration of conflicting interests
All named authors hereby declare that they have no conflicts of interest to disclose.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.