
Abstract
Background and aims:
Bone deficiency in revision total hip arthroplasty is a challenge to the surgeon. One option for restoration of the bone stock is impaction bone grafting and use of a cemented socket. The aim of this study was to evaluate the mid-term clinical outcome of impaction bone grafting and cemented socket revisions.
Material and methods:
A total of 59 patients (60 hips) underwent revision arthroplasty with impaction bone grafting and application of a cemented socket on the acetabular side in the Turku University Hospital from 1999 to 2004. The study end-point was re-revision for any reason. The cumulative percentages for survival were followed and estimated with Kaplan–Meier curves. Associations between occurrence of re-revision and potential risk factors were analyzed with logistic regression. Results were quantified by odd ratios and 95% confidence intervals. The mean age of the patients was 69 years (33% male). A total of 3% of the patients had a class I Paprosky acetabular defect, 38% had class II, and 55% had class III.
Results:
The overall survival rate was 73%. The mean follow-up time was 7 years. The most common reason for re-revision was aseptic loosening of the acetabular component (13 patients, 81% of re-revisions). Cox’s regression analysis did not identify any risk factors for re-revision.
Conclusion:
Our results were inferior compared to some previous studies. Impaction bone grafting of acetabular defects in revision total hip arthroplasty may not always provide a reliable bone stock in long-term.
Introduction
The need for primary and revision total hip arthroplasty (THA) is rising as a consequence of the growing number of elderly people (1). Bone deficiency around implants tends to increase over time and becomes a common risk for loosening of the prosthesis. In fact, aseptic loosening is the most common reason for revision THA (2–4). Deficiency of acetabular bone stock is usually caused by osteolysis due to wear of implants, stress shielding from an excessively stiff implant, loosening and migration of the cup, or infection (5, 6). The loss of bone stock poses a challenge for revision THA, but there are different options to overcome the problem. Porous-coated cementless acetabular cups can be used—with or without a cancellous bone graft—for small bone deficiencies (7), and larger bone defects may be treated with reconstruction cages (8) or structural bone grafts. However, the reconstructive procedure is demanding in the absence of a sufficient amount of bone. Furthermore, host tissue may resorb the allograft (9). A recent advance for the management of bone stock loss is the use of trabecular metal acetabular components and augments (10). Traditionally, major acetabular defects have been reconstructed for primary and revision THA by impaction bone grafting and a cemented socket (11). The mid-term and long-term results of impaction bone grafting have generally been favorable (12–17), but there are some reports of poor results when impaction grafting has been used (5, 18). Fresh frozen bone is currently associated with the best result (18), but this method carries the risk of disease transmission (19). In an effort to overcome this risk, the osseous tissue may be processed by irradiation and freeze drying. Both of these methods decrease the biomechanical properties of the graft and may reduce bone incorporation (19).
In the Turku University Hospital, impaction bone grafting and the cemented socket technique was used from 1999 to 2004. The aim of this study was to evaluate long-term results of these acetabular revisions.
Patients and Methods
Between 1999 and 2004, 59 patients (20 men and 40 women) underwent 60 acetabular revisions where impaction bone grafting and a cemented polyethylene socket were used. The patients were treated at one center (the Turku University Hospital), and the revisions were made on average 13 years (range 6–24 years) after the primary THA or previous revision THA. The information concerning the operative reports and follow-up visits was collected retrospectively from the electronic medical record database of the Turku University Hospital. Data cut-off was set at re-revision for any reason by 22 February 2013. A total of 18 patients died during the follow-up time.
Reason for acetabular revision with impaction bone grafting and a cemented socket was in 59 instances because of aseptic loosening and in one instance because of implant breakage. The mean follow-up time was 7.4 years (range 0–14 years). The average age of the patients at surgery was 69 years (range 35–87 years). The index revision hip was the right hip in 39 (65%) cases. The indications for primary hip arthroplasty were osteoarthritis in 31 hips (51%), dysplasia in 8 hips (13%), rheumatoid arthritis in 7 hips (12%), fracture in 4 hips (7%), and other in 10 hips (17%). In 5 out of the 60 revisions, one femoral allograft was used, in 41 out of 60 two were used, in 7 out of 60 three were used, in 1 out of 60 five were used, and in 6 out of 60 an unknown number was used. A mesh was used for reconstruction in 50 revisions. The number of screws used for fixation was zero in 11 revisions, one in 1 revision, two in 3 revisions, three in 9 revisions, four in 8 revisions, five in 5 revisions, six in 3 revisions, and unknown in 20 revisions. Based on pre-revision radiographs, the hips were radiographed before revision and the degree of acetabular bone defects was classified according to Paprosky (20, 21). The radiographs were evaluated by two physicians experienced in reviewing hip radiographs, I.K. and K.T.M.
The Paprosky classification before index impaction bone grafting and a cemented socket is presented in Table 1. Preoperative radiographs were available for 57/59 patients (97%).
Paprosky classification a of 58 (16 failed and 42 successful) hips that underwent impaction bone grafting and application of a cemented socket for acetabular reconstruction for revision THA.
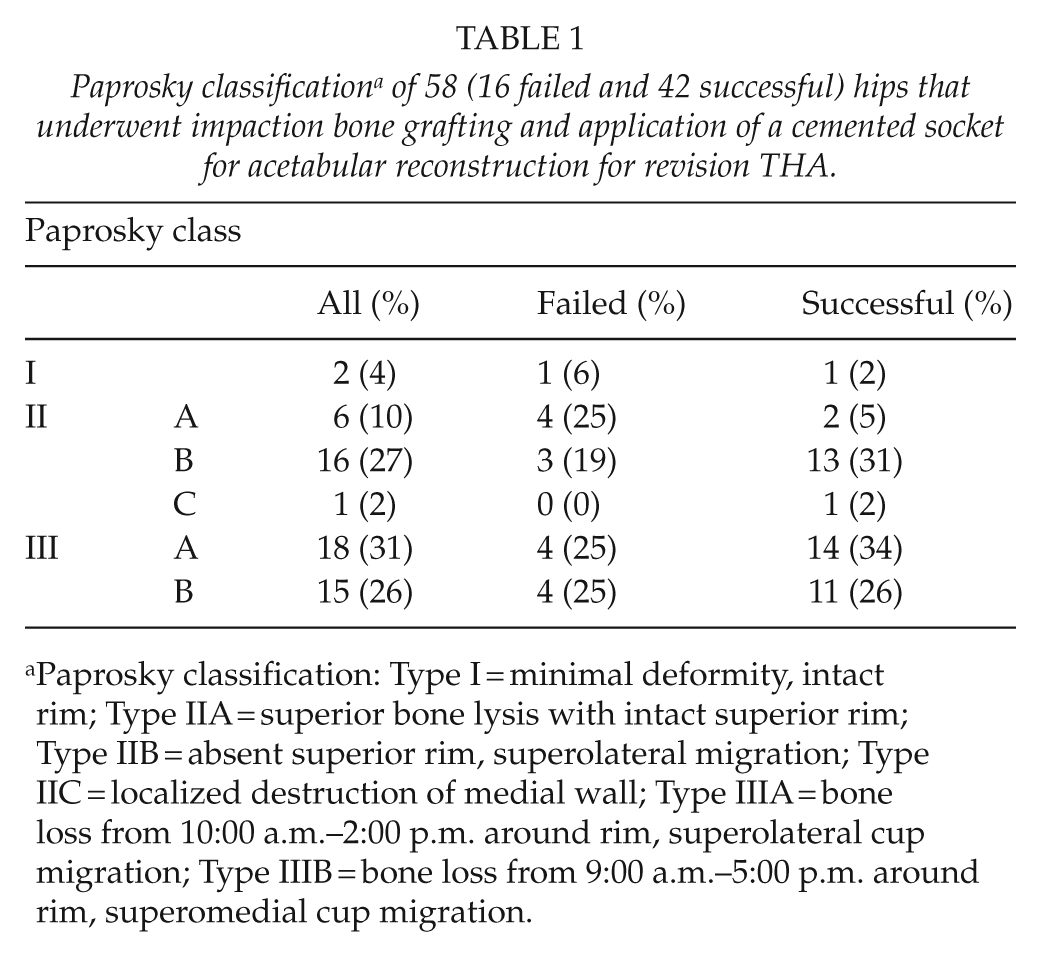
Paprosky classification: Type I = minimal deformity, intact rim; Type IIA = superior bone lysis with intact superior rim; Type IIB = absent superior rim, superolateral migration; Type IIC = localized destruction of medial wall; Type IIIA = bone loss from 10:00 a.m.–2:00 p.m. around rim, superolateral cup migration; Type IIIB = bone loss from 9:00 a.m.–5:00 p.m. around rim, superomedial cup migration.
All acetabular revisions were performed as described for impaction bone grafting (11) through the direct lateral approach. The bone grafts were made from fresh frozen femoral heads obtained from the bone bank of the Turku University Hospital. The femoral heads had been processed and stored sterile at −80 °C according to protocol (22). The allograft femoral heads were ground to 0.3- to 1.0-cm chips during the operations. All cartilage was removed before grounding. The bone grafts were washed three times before impaction. Antibiotic fluid containing tobramycin was added. Joint infection was checked by bacterial sampling for culture during surgery. The graft was packed as described (11) and, if necessary, a wire mesh was secured with screws on top of the graft. Finally, a cup with polyethylene liner was cemented on top of the graft.
Two different cemented acetabular cup designs were used: Exeter (Stryker, Newbury, UK) in 44 revisions and Elite plus LPW (DePuy, Warsaw, Indiana, USA) in 13 revisions. The acetabular design remained unclear in 6 cases. An acetabular mesh was used in 52 cases. The surgical data are detailed in Table 2.
Logistic regression results of different factors related to the rate of re-revisions.
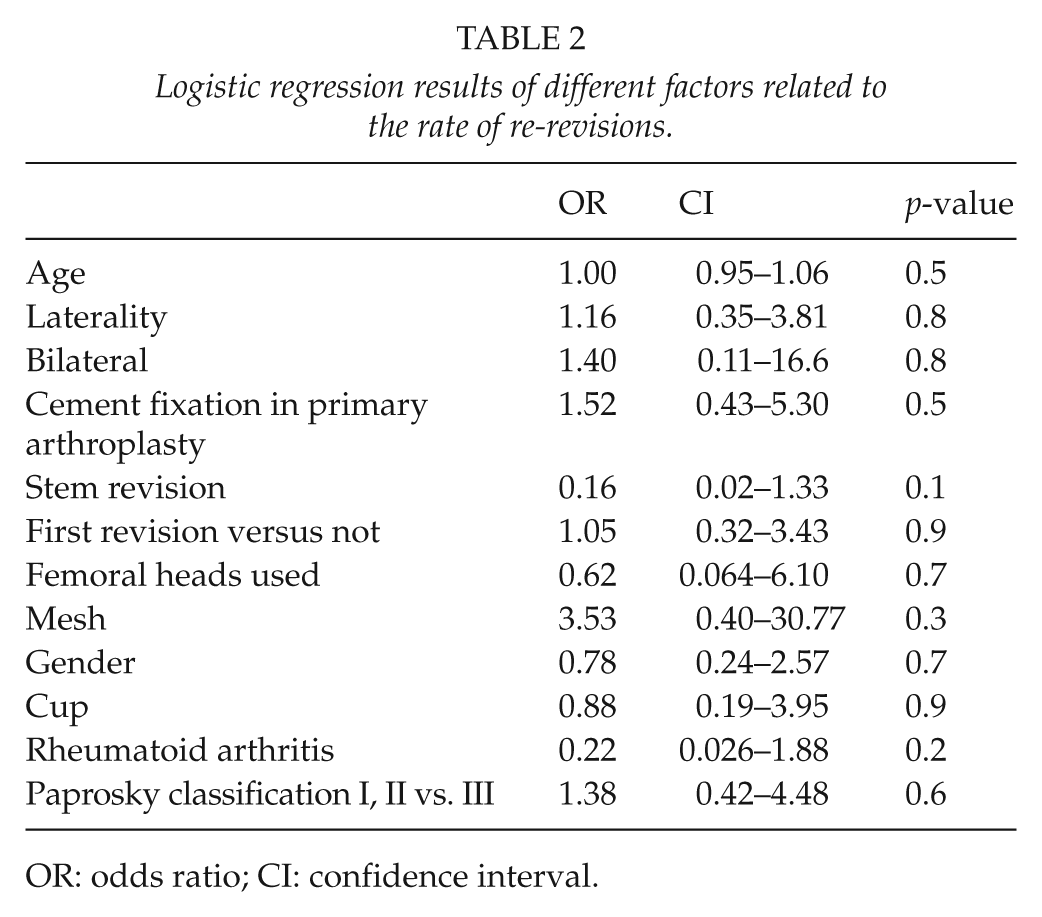
OR: odds ratio; CI: confidence interval.
Loading of the hips was restricted for 2 months after the operation; a maximum weight of 30 kg was allowed. The most common reason for impaction bone grafting and use of a cemented socket was aseptic loosening (59 hips, 94% of all operations). Other reasons for the revisions were prosthetic infection (3 hips, 5% of all operations) and prosthetic component breakage (1 hip, 1% of all operations). The acetabular component alone was revised in 44 cases, both components in 14 cases, and in 5 cases involvement of the stem in the operation was not sufficiently documented.
Statistical Analysis
Continuous variables were described by means and standard deviations (SDs) and categorical variables by frequencies and percentages. The associations between the occurrence of a revision and risk factors were analyzed with logistic regression. Results were expressed by odd ratios (ORs) and 95% confidence intervals (95% CIs). The cumulative percentages for survival were estimated with the Kaplan–Meier technique. P-values less than 0.05 were considered statistically significant. Statistics were run on the SAS for Windows, Version 9.3 (SAS Institute Inc., Cary, NC, USA).
Results
A total of 16 hips in 16 patients with acetabular impaction bone grafting and a cemented socket required re-revision. The overall survival rate for acetabular revision with impaction bone grafting and a cemented socket at 7-year follow-up was 77% (95% CI: 63–85) (Fig 2). The primary reason for re-revision was aseptic loosening of the acetabular component (13 patients, 81% of re-revisions). Two of re-revisions (13%) were performed due to prosthetic infection and one (6%) due to recurrent dislocations. The first re-revision occurred 1 month after the index impaction bone grafting due to early cup displacement. For the other patients, the revisions became necessary 1–9 years (mean 3.9 years) after the index revision.
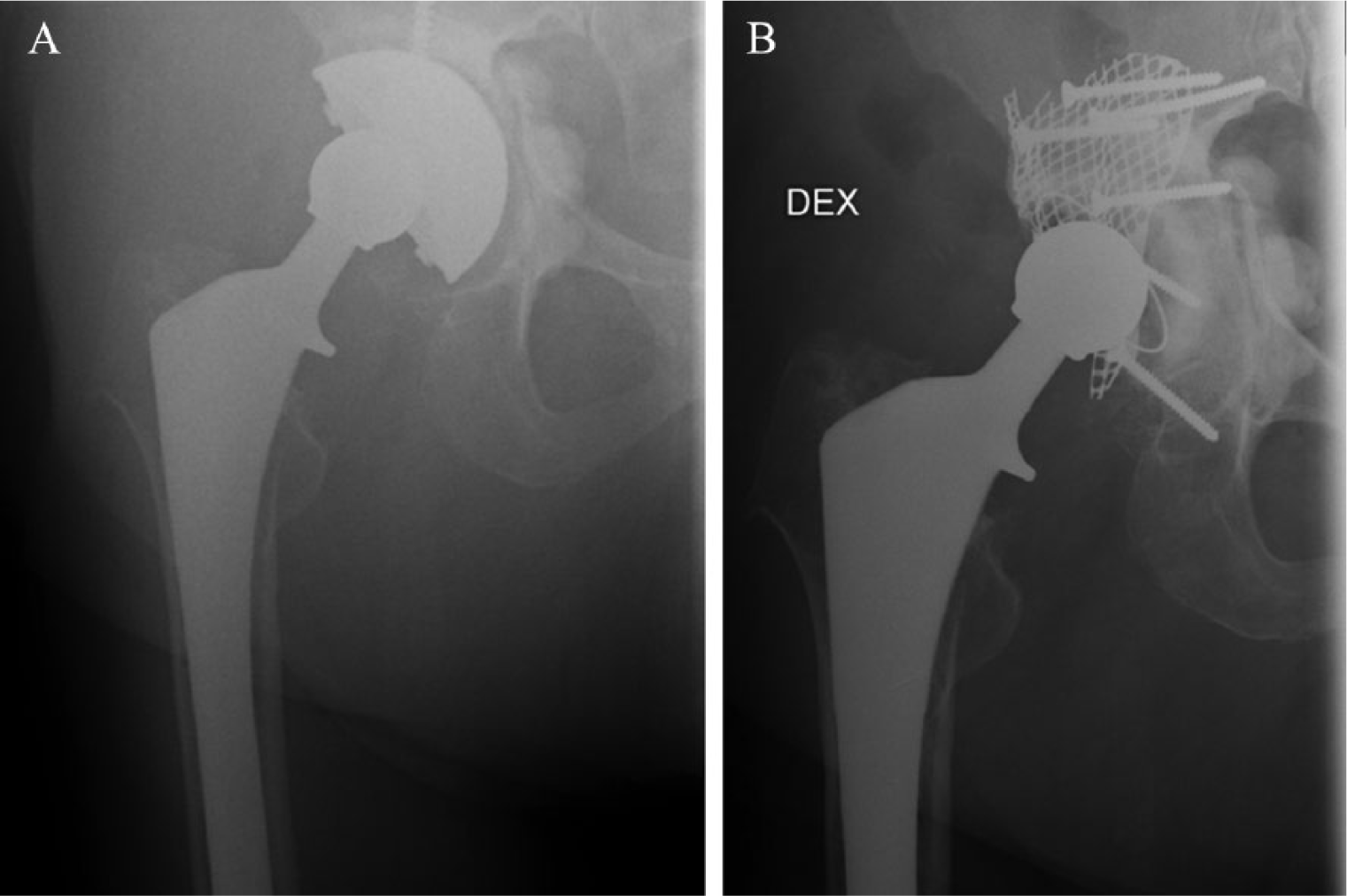
(A) Preoperative radiograph of a 72-year-old woman 18 years after THA with a cementless stem and a cemented cup. (B) One-month postoperative radiograph of the hip shown in Fig. 1A. Note large pelvic and trochanteric osteolytic cysts. Acetabular bone defects reconstructed using impaction bone grafting with mesh augmentation, and cemented socket.
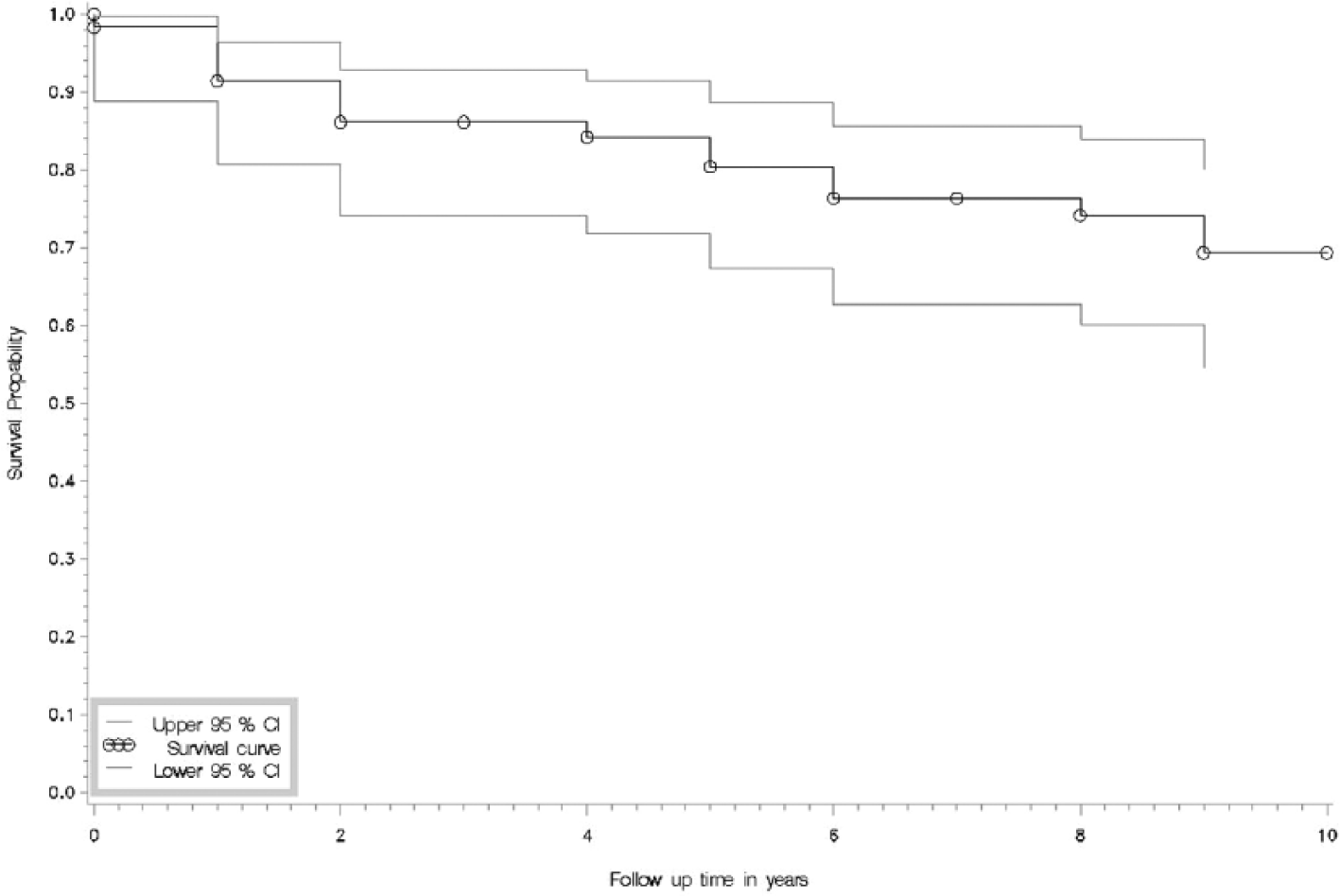
Kaplan–Meier survival curve of 60 acetabular reconstructions. Impaction bone grafting and construction of cemented sockets have been carried out. The mean follow-up time was 7.4 years. The end-point was revision for any reason.
Paprosky classifications are presented in Table 1. Survival of the bone graft and the Paprosky acetabular defect class did not correlate with each other (p = 0.4). A total of 11 patients (19%) had rheumatoid arthritis. Rheumatoid arthritis did not affect the re-revision rate (Cox’s regression analysis, p = 0.2).
The results of logistic regression analysis are presented in Table 2. The results show that there was no association between circumstances like age, gender, presence or absence of rheumatoid arthritis, and Paprosky type on the rate of re-revisions.
Discussion
The overall 7-year survival rate was 77% (95% CI: 63–85). Our results of the use of impaction bone grafting with a cemented polyethylene socket for revision THA were inferior compared with some earlier studies. There are several studies on impaction bone grafting and cemented sockets for acetabular reconstruction when revision THA is required. Van Egmond et al. (12) reported a 95% survival rate for aseptic loosening at 8.8 years of follow-up. Garcia-Cimbrelo et al (17). used impaction bone grafting with a cemented socket and reported an 82%−84% survival rate for Paprosky grades IIIA and IIIB at 8 years of follow-up. Schreurs et al. (14) reported a survival rate of 84% at 15 years following acetabular revision for aseptic loosening and Slooff et al. (16) a survival rate of 88% following acetabulum revision for any reason. Welten et al. (15) reported a 79% survival rate for any reason at 15 years of follow-up. In these studies, the bone grafts were not washed, but the bone bed was. The bone chip size they used was 0.7–1.0 cm, which is slightly larger compared to our 0.3–1.0 cm.
However, in a study of Van Haaren et al. (5), the survival rate of cemented impaction bone grafting of the acetabulum was only 72% during 7 years of follow-up when aseptic loosening was the end-point. In that study, grafts were not washed before impaction and the authors propose that this may have affected the mechanical stability of the grafts and thus the outcome (20). Bone graft washing may increase friction and allow tighter impaction of the material, since fat and bone marrow are eliminated from the graft. Also, the risk of bacterial infection is reduced (23). Our results are in agreement with those of Van Haaren et al. (5).
One patient’s hip became dislocated repeatedly after revision with impaction bone grafting and a cemented socket, and a re-revision was necessary. This patient abused alcohol, which is a clear risk factor for prosthetic failure. Two patients had a prosthetic infection requiring a two stage; these infections occurred 1 and 5 years after the index operation. These numbers are similar to previous studies (7, 12).
The degree of acetabular deficiency is critical for the survival of the impacted bone graft. Some studies have reported a correlation between acetabular defects and revision rate (5), but the study of Garcia-Cimbrelo et al. (17) found that the degree of acetabular bone loss was not associated with the revision rate. In our study, the failed as well as the successful group had a similar overall rate of Paprosky acetabular bone defect classes, and there was no association between failure rate and acetabular defects. Having stated this, it is fair to remind that, in the most severe cases, bone deficiencies may have been treated with other methods, for example, cages.
Acetabular impaction bone grafting is a demanding technique, and some of the re-revisions in this study may have been due to surgical inexperience. However, 10 of our 18 re-revisions occurred 4 or more years after the primary revision. This implies that the procedure as such was technically successful, but the impacted bone grafts did not osteointegrate over follow-up time. Bone graft thickness is an important factor in graft ossification, and thick grafts may not become integrated into the skeletal structures of the host.
Graft size may also affect their osteointegration. Bone graft size may even be of more importance than graft washing (24). Larger particles, approximately 1 cm in diameter, are stiffer than smaller ones (24, 25). Our bone graft size was 0.3–1.0 mm. Larger grafts have both biomechanical and biological advantages: larger chips may produce a more porous bed between the graft particles and encourage bone ingrowth (26). In our study, the bone chip diameter may have been a bit too small for an optimal outcome.
Some studies report a higher survival rate for impaction bone grafting when wire mesh is used compared to impaction bone grafting without a mesh (27). In our study, mesh usage did not correlate with the survival rate (p = 0.3). Revisions that require a mesh probably have more severe bone defects, and since our patient number was relatively small, we need to be careful in making too hasty conclusions on the relation between survival rate and mesh usage. In previous studies, patients with rheumatoid arthritis have experienced inferior results from acetabular revision impaction bone grafting compared to patients with other medical conditions requiring grafting (28, 29). In our study, there was no statistically significant correlation between rheumatoid arthritis and the re-revision rate (p = 0.2).
Our bone grafts were made from fresh frozen bone, and all grafts were washed twice with water and once with antibiotic fluid before use. Washing does not influence the penetration of the cement, but it improves bone graft incorporation (19). Large and washed bone grafts exhibit the least cup migration, and cement penetration to larger graft seems to be better (25). Fresh frozen bone seems to yield the best results (29). However, there is a risk of transmission of contagious diseases when fresh frozen grafts are used (30). Thus, an option for fresh frozen bone is processed bone, which consists of irradiated and freeze-dried bone. Both of these processing methods impair the biomechanical properties of the graft and may affect bone incorporation disadvantageously (30).
The weakness of this study is that we were not able to assess graft incorporation or resorption from postoperative imaging studies (radiographs). Second, the data were collected retrospectively. Furthermore, our patient records do not include pain scores or quality of life indicators which could indicate aseptic loosening of the acetabular component before radiographic findings (31). The end-point of our study was re-revision for any reason. Some patients may have had symptoms of implant failure, but due to patient-related features, for example, high age or concomitant illness, a re-revision may not have been performed.
There were no statistically significant risk factors related to the risk of re-revision after impaction bone grafting with a cemented cup. The overall results of this study were inferior compared to some previous studies (12, 14, 15). In conclusion, impaction bone grafting of acetabular defects for revision THA may not always provide a reliable bone stock.