
Abstract
Background and Aims:
Rib fractures can cause significant problems in trauma patients, often resulting in pain and difficulty with respiration. To prevent pulmonary complications and decrease the morbidity and mortality rates of patients with rib fractures, currently there is a trend to provide surgical management of patients with flail chest. However, the indications for rib fracture fixation require further specification.
Material and Methods:
Past and current strategies are described according to a review of the medical literature. A systematic review was performed including current indications for rib fracture fixation. MEDLINE (2000–2013) was searched, as well as Embase (2000–2013) and Cochrane Databases, using the keywords rib, fracture, fixation, plate, repair, and surgery.
Results:
Three retrospective studies were found that described different techniques for rib fracture fixation. The results demonstrated a reduced number of ventilation days, decreased long-term morbidity and pain, and satisfactory rehabilitation after surgical treatment. In addition to flail chest, age, Injury Severity Score, and the number of rib fractures were important predictive factors for morbidity and mortality.
Conclusion:
Surgical rib fracture fixation might be indicated in a broader range of cases than is currently performed. Prospective randomized trials are needed for further confirmation.
Introduction
Chest wall injury, after blunt thoracic trauma, is relatively common. This type of injury can vary in severity from isolated rib fractures to severe, bilateral crush injuries leading to respiratory problems. The mechanism associated with these injuries is often due to direct forces acting on the chest wall. Elderly patients and patients with osteoporosis or osteopenia have an increased risk of the number and severity of rib fractures. This is in contrast to children where higher forces are needed to cause rib fractures; they have a chest wall that is more pliable and compliant. The most common symptom associated with rib fractures is pain, which makes it difficult to take adequate breaths. Up to 30% of patients with rib fractures develop pneumonia; older patients are at risk of this complication (1, 2).
Rib fractures occur in 10% of all trauma patients and in approximately 30% of all patients with significant chest trauma (3). Rib fractures can be a sign of severe trauma. The greater the number of fractured ribs, the higher the associated morbidity and mortality (3). Flagel et al. (4) reported 10% mortality in patients with more than four rib fractures; this increases to 34% in patients with eight or more fractures. In addition, patients with more than four rib fractures, and who are 45 years of age or more, have an increased risk of adverse outcomes (4–7). In a retrospective study, from the National Trauma Data Bank, Kent et al. (7) reported that 56% of the mortality rate, in patients with thoracic trauma who were older than 65 years, was due to rib fractures and not other injuries.
The management of rib fractures involves pain control as well as adequate oxygenation and ventilation, with the use of positive pressure ventilation when necessary. However, use of mechanical ventilation is associated with several ventilation-related complications. It is known that patients with flail chest, not treated surgically, develop pneumonia in 27%–70% cases and have a mortality rate of 25%–51% (8).
Therefore, rib fractures can lead to significant morbidity and mortality, which increase with age and the number of rib fractures. An age of 45 years or greater and more than four rib fractures appear to be important risk factors associated with patient outcome.
Providing external stability by surgical fixation might offer an alternative treatment for the management of multiple rib fractures in older adults with the goal of avoiding mechanical ventilation. The aim of surgical treatment is to improve the respiratory mechanics, reduce pain, and prevent pulmonary restriction that can be associated with significant chest wall deformity. Although the majority of patients with rib fractures heal spontaneously, without surgical therapy, there might be a select group of patients who can benefit from surgical repair.
A recently published meta-analysis concluded that surgical fixation of a flail chest is associated with reduction in the duration of mechanical ventilation, the complications associated with prolonged mechanical ventilation, the length of hospital stay, as well as mortality (9). Although these data are based mainly on retrospective studies and a few prospective trials, the trend currently is to provide surgical fixation of the ribs in patients with flail chest (9). This management has been reported in the recent guidelines published by Surgical Critical Care, which has recommended surgical fixation of rib fractures in patients with a flail chest segment, severe chest wall deformity, with or without pulmonary herniation, or symptomatic fractures of three or more consecutive ribs (10). However, surgical management of cases with non-flail chest remains controversial.
A protocol has been developed at this hospital, based on previous literature, for patients with multiple rib fractures. All patients with flail chest and/or more than four rib fractures and/or are 45 years of age or greater are treated surgically (Figs 1 to 3).
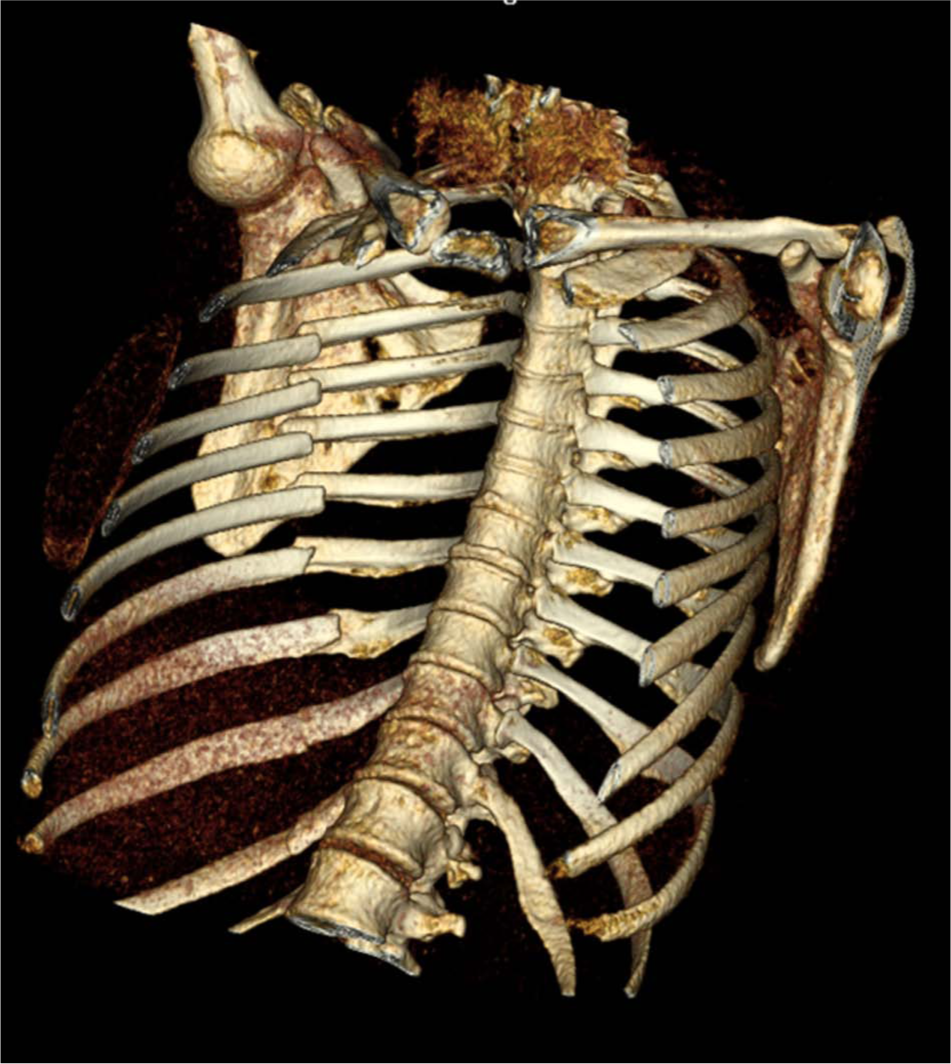
3D CT reconstruction of multiple rib fractures.
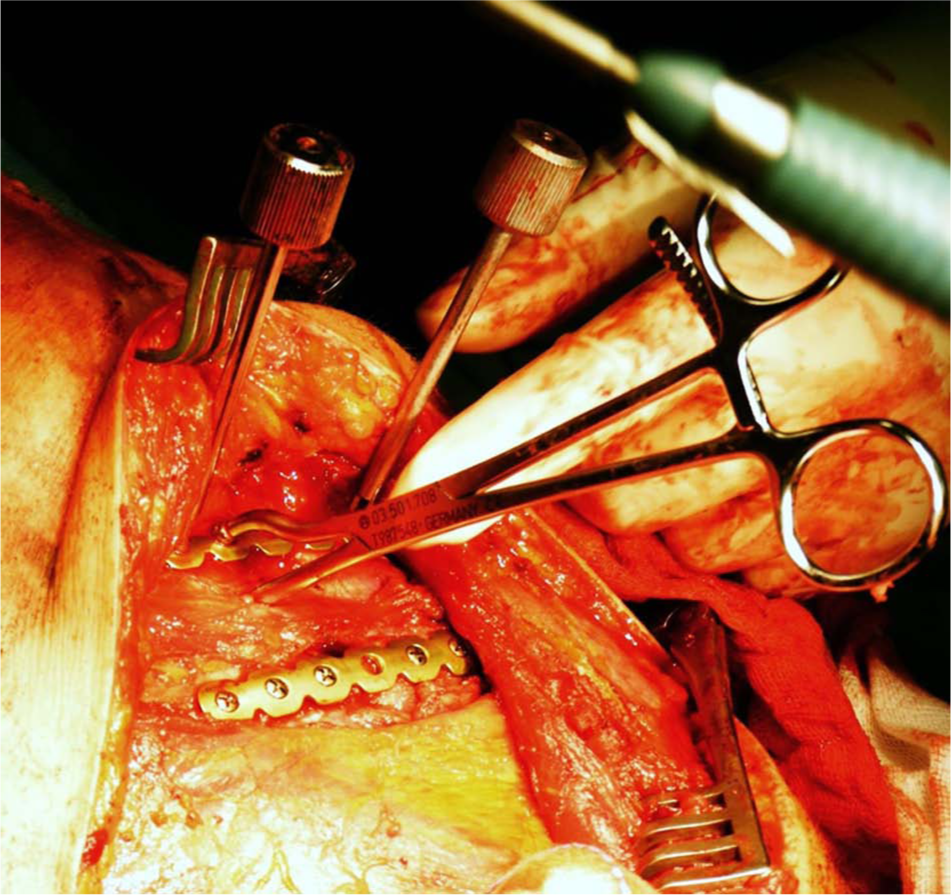
Rib fixation.
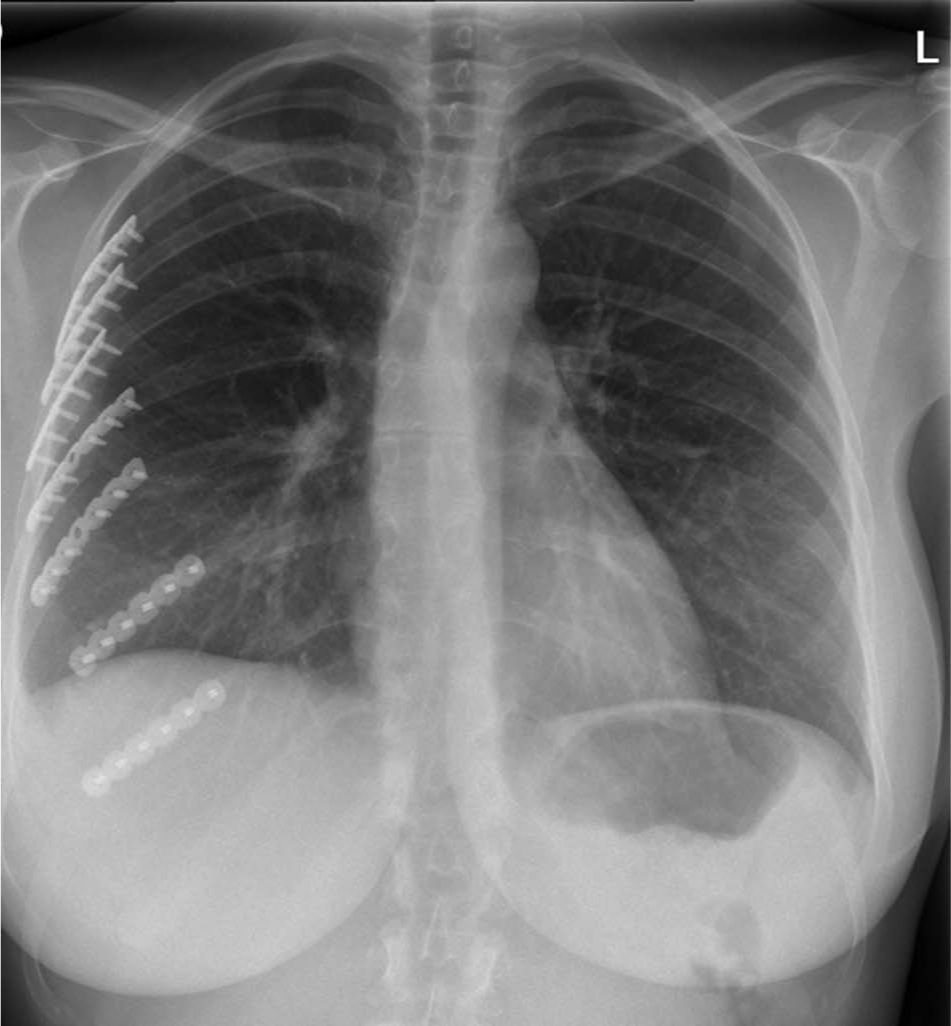
Chest X-ray after rib fixation.
History
The treatment of multiple rib fractures can be divided roughly into two main groups: internal support techniques and external support techniques (11). Jones reported the first case of external support for a flail chest 25 years before the introduction of mechanical ventilation. He described a percutaneous technique where traction was applied to the ribs (12). Many alternatives to this technique followed thereafter. A non-operative device used was the Cape Town limpet, described by Schrire (13); this sink plunger–like device was used to give traction to the flail segment. Significant complications from these external traction devices were associated with the prolonged bed rest required. After the introduction of mechanical ventilation, the external traction devices became more or less obsolete. Avery et al. (14) first described continuous mechanical ventilation, which could provide internal stabilization for flail chest. Garzon et al. (15) reported combined mechanical ventilation with tracheostomy to remove problematic pulmonary secretions.
Over time, after the introduction of mechanical ventilation, the associated problems became apparent. Therefore, a few years after the introduction of mechanical ventilation, the search for a safe and effective internal fixation technique to treat rib fractures, to provide stability to the chest wall, and to reconstruct the chest shape continued. The use of K-wires, intramedullary repair, and an arsenal of self-made plates have been described. Even drittel rohr plates were used, but they broke after 12 h (16). In 2008, the STRATOS™ system (MedXpert GmbH, Heitersheim, Germany) was introduced; this plate is fixed to the ribs with hooks. In addition, the RibLoc® plate (Acute Innovations, Hillsboro, OR, USA) used a U-shaped plate that slides over the rib combined with fixation using stable angular screws. In 2009, Ivancic et al. (17) described a technique based on the use of K-wires with a figure of eight wires to create stability. Most recently, DePuy Synthes® (Amersfoort, the Netherlands) introduced the MatrixRIB™ system, consisting of specifically contoured titanium plates, which are fixed to the ribs with locking screws.
Surgical Technique
There are several options for hardware available for fixation of rib fractures: metal plates, absorbable plates, and intramedullary fixation. One technique reported by Mayberry et al. (18) includes plates fixed with a cerclage. Common disadvantages associated with this method are intercostal nerve impingement and wire breakage. The Judet (19) plate is a metal plate with crimps on the side that clamps around the ribs. This technique can also damage nerves. The U-plate, which is fixed with locking screws, also uses crimps, but they only clamp onto the superior aspect of the ribs; this avoids damage to nerves, which can cause chronic pain. A cadaveric study reported by Sales et al. (20) demonstrated that the U-plate is more durable than anterior plate fixation. These 3.5 mm reconstruction plates require intra-operative contouring, which results in increased operating time. Using pre-contoured locking plates can save time. Alternatives include absorbable plates; however, these plates have been associated with a greater risk of tissue reaction. Both Mayberry et al. (21) and Marasco et al. (22) described several complications associated with absorbable plates, when used alone; they advised that these plates be used in conjunction with metal plates for posterior chest wall stabilization.
Intramedullary fixation provides less stability; however, it is suitable for fractures that are difficult to reach, like fractures behind the scapula. In addition, there are pre-contoured rib splints that are fixed with one locking screw to prevent migration. The problem with these splints is that they can easily perforate a rib, especially in older patients. Therefore, at this center, we prefer to use splints only in combination with plates and do not rely on them alone.
Radiology Evaluation
The standard chest X-ray commonly underestimates the number of rib fractures present but gives accurate information about the presence of a pneumothorax or hemothorax (23). A computed tomography (CT) scan is more reliable for the detection of rib fractures but is not a standard investigation for the detection of rib fractures; the additional information gained usually does not significantly change the management of rib fractures. However, as part of modern trauma screening, after high-energy accidents, a chest CT is usually performed. A CT scan gives more detailed information about the location and number of rib fractures present as well as the magnitude of dislocation, which can be useful in the preoperative planning of rib fixation (24, 25).
Indications For Rib Fixation
There is no hard evidence on the best method to use for the repair of rib fractures. However, there are some generally accepted indications for surgical rib fixation. The most common indication for rib fixation is the presence of a flail chest (26). Other accepted indications are patients with rib fractures who, notwithstanding good pain management, are still in pain, have a chest wall deformity, or have one or more symptomatic non-union rib fractures. Furthermore, rib fractures can be fixed while performing a thoracotomy for other indications (26).
A literature search was performed to determine suitable indications for rib fracture fixation, in addition to the current indication of flail chest, as described in prior meta-analyses and guidelines (18, 26, 27).
Review
Literature Search
A systematic literature search was performed. MEDLINE (2000–2013) was searched, as well as Embase (2000–2013) and Cochrane Database, using the keywords rib, fracture, fixation, plate, repair, and surgery. The last search was performed in December 2013. The literature search was restricted to articles published after 1999, as surgical techniques changed dramatically after this point in time. Two reviewers independently decided whether the studies met the inclusion and exclusion criteria and reviewed all titles and abstracts.
Study Selection and Data Extraction
First, a MEDLINE search was performed and the two reviewers screened all titles. The abstracts of selected titles were further screened to ensure that the study included surgical treatment of non-flail chest. If adequate information was not present in the abstract or the abstract was absent, full text of the article was requested. After the abstracts were selected, the two reviewers analyzed the full text of the articles. Included in the review were all studies with at least 10 surgically treated human patients with non-flail chest rib fractures. The articles had to be written in English, Dutch, or German. Excluded were case reports, biomechanical studies, animal studies, expert opinions, and studies with less than 10 surgically treated patients. Then, review of the Embase and Cochrane Database was performed in the same way. A supplemental search of all references included with the articles, found by the initial search, did not yield extra abstracts. All relevant outcome data, for each of the included studies, were extracted independently, by the two authors, using the Cochrane Collaboration tool (28).
Results
There were 673 titles reviewed, 10 full-text articles were retrieved. Seven articles were excluded and three manuscripts remained for data extraction. Table 1 summarizes the included studies. All of the studies were retrospective; one study was a matched case-control study (Table 2). For the comparison group, treatment consisted of analgesia and mechanical ventilation when necessary. A variety of surgical techniques were used including struts, intramedullary fixation and absorbable or non-absorbable plates. The indications used in the studies are described in Table 3.
Description of included studies.
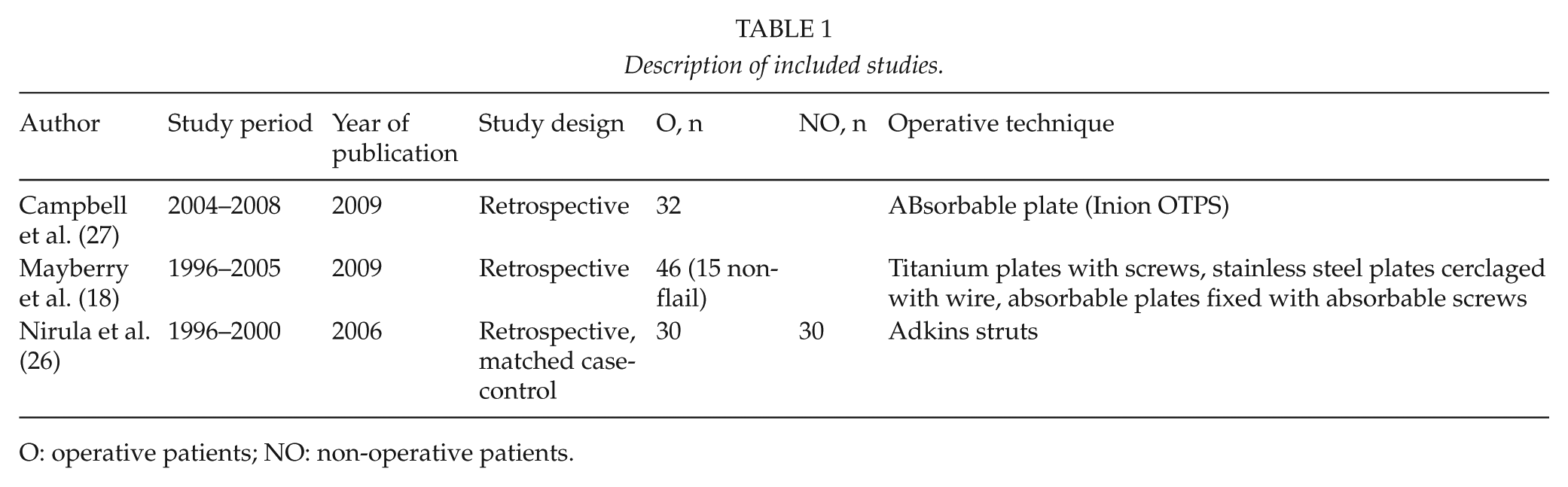
O: operative patients; NO: non-operative patients.
Matched case-control study.
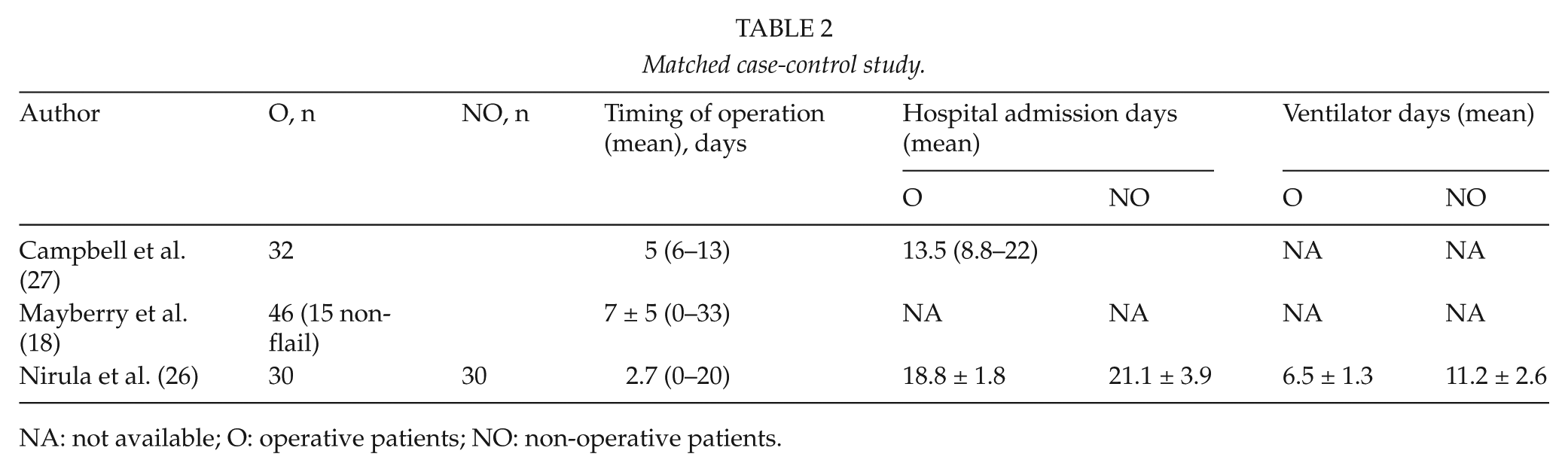
NA: not available; O: operative patients; NO: non-operative patients.
Summary of study characteristics.
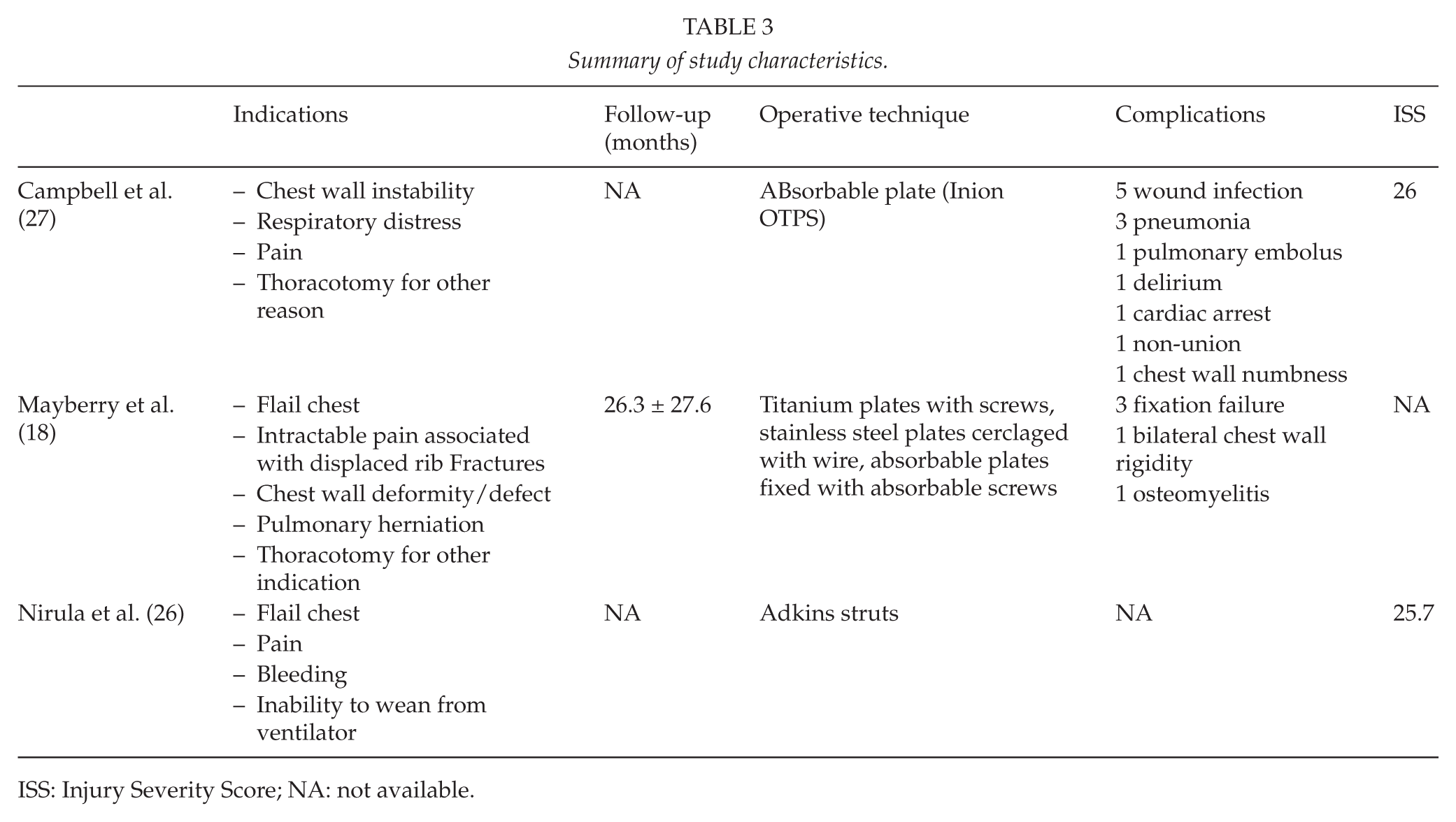
ISS: Injury Severity Score; NA: not available.
Conclusion
Pneumonia and ventilator-associated complications pose a major threat to patients with rib fractures. With the development of specifically designed rib fixation devices, the materials used for surgical treatment of rib fractures have undergone a revival. Although there is accumulating evidence to support surgical treatment of flail chest, the evidence for surgical treatment of non-flail chest rib fractures is limited. In our experience, there is a benefit from early stabilization of rib fractures in selected patients, which increases the likelihood of preventing ventilator support and pneumonia. We searched the literature to determine whether there is support of our own experience. However, there were only a limited number of articles on rib fracture fixation fulfilling the selection criteria, when flail chest was excluded. None of the included articles reviewed were prospective randomized trials, and they all consisted of only a small number of patients. Moreover, the three manuscripts finally selected on rib fixation were difficult to compare because of the significant variation in study design. Only Nirula et al. (26) concluded that rib fracture fixation showed a trend toward fewer total ventilator days. Mayberry et al. (18) investigated the quality of life after rib fixation, and they concluded that there was low long-term morbidity and pain. Campbell et al. (27) demonstrated low levels of pain and satisfactory rehabilitation. There was significant variability in the timing of surgery, and the indications for surgery were not standardized. Brasel et al. (29) demonstrated that age and Injury Severity Score (ISS) were the only important predictors of mortality in patients with rib fractures, which might suggest that every older patient with a high ISS might benefit from surgical treatment of their rib fracture(s). Flagel et al. (4) reviewed the National Trauma Data Bank. He concluded that an increase in the number of rib fractures correlated directly with an increase in pulmonary morbidity and mortality.
A recently published meta-analysis showed that surgical treatment of flail chest was associated with a significant reduction in morbidity, mortality, and resource expenditures. The comparison of studies, in this meta-analysis, showed a tendency toward reduction of ventilator days as well as hospital admission days (30). This reduction was more evident when the interval to surgery was short.
These findings are consistent with our own experience in patients with both flail chest and non-flail chest rib fractures. We have observed a reduction in ventilator time and the need for intensive care unit (ICU) admission as well as hospital admission days (unpublished data). For the non-flail chest rib fractures, this includes patients with continued pain despite adequate analgesia, inability to wean from the ventilator, and the presence of a chest wall deformity.
The presence of multiple rib fractures is associated with a significant mortality rate and pulmonary morbidity. Age, ISS, and the number of rib fractures are important risk factors. The level of evidence for rib fixation for flail chest is limited because of the lack of randomized controlled trials. Although it is more common currently to operate on patients with a flail chest, a prospective randomized trial is needed with standardized indications for surgical management of rib fractures, not only as part of a flail chest but also in patients with non-flail chest rib fractures. Age, the number of rib fractures, timing of surgery, and ISS must be taken into account when starting such a trial. As it was previously suggested, any attempt to reduce pneumonia may also reduce mortality, and as such, rib fracture fixation might have much broader indications than is currently accepted in routine practice.
Footnotes
Declaration Of Conflicting Interests
The authors declare no conflict of interest.
Funding
The authors did not receive additional funding for this research.