
Abstract
Background:
Complications in the biliary tract occur in 5%−30% after liver transplantation and the main part of the complications is successfully managed with endoscopic retrograde cholangiopancreaticography (ERCP). The incidence and risk factors for post-ERCP complications in liver transplantation patients are not well described. Our objective was to define the frequency of post-ERCP complications in liver transplantation patients at the Abdominal Center, Rigshospitalet, the only Liver Transplantation Center in Denmark.
Methods:
Retrospective study of all ERCPs performed in liver transplantation patients during a 9-year period.
Results:
A total of 292 ERCPs were included. Overall post-ERCP complications occurred in 24 procedures (8.2%): pancreatitis in 8 (2.7%), bleeding in 5 (1.7%), and cholangitis in 13 (4.5%) procedures. Simultaneous pancreatitis and cholangitis, and simultaneous bleeding and cholangitis occurred after two procedures, respectively. Multivariate analysis concerning overall complications identified biliary sphincterotomy (p = 0.006) and time since liver transplantation within 90 days postoperatively (p = 0.044) as risk factors for post-ERCP complications. Specifically concerning post-ERCP pancreatitis (PEP), it was found that pre-ERCP cholangitis was another independent risk factor for PEP (p = 0.026). Stent in the biliary tract prior to ERCP seemed to be protective (p = 0.041).
Conclusions:
Complications were of surprisingly mild degree. The rates of post-ERCP complications in our study were in line with previous studies with liver transplantation patients. Cholangitis prior to ERCP may be another risk factor for post-ERCP pancreatitis.
Keywords
Introduction
Endoscopic retrograde cholangiopancreaticography (ERCP) is an invasive procedure that allows diagnosis and treatment of a variety of conditions in the pancreatic–biliary system, such as gallstones, benign or malignant biliary obstruction, sphincter Oddi dysfunction, chronic pancreatitis, and biliary leakage after cholecystectomy. ERCP is recommended solely for therapeutic purposes due to the occurrence of potentially lethal complications including pancreatitis, cholangitis, and perforation (1–3). The safety, success, and complication rate of ERCP in non-liver transplantation (non-LTX) patients have been shown in larger studies (1, 2, 4–9). The total post-ERCP complication rate in these studies was up to 12%, and the most common complication in non-LTX patients was post-ERCP pancreatitis (PEP). PEP occurs in 1%−12% with a mortality rate of 0.8%−3% (1, 3, 4, 9–12). Other complications include cholangitis, bleeding, and perforation. In both retrospective and prospective studies, a frequency of cholangitis between 0.8% and 5% (1, 2, 6 –8, 13, 14) and bleeding between 0.6% and 0.9% (1, 2, 6, 7, 13, 14) after ECRP have been reported. Perforation is a rare complication.
Complications in the biliary tracts occur in 5%−30% of all patients after LTX (15–17). These complications include anastomotic and non-anastomotic stenosis (Fig. 1), bile leakage, choledocholithiasis, and cholangitis. The most widely accepted treatment of these complications is ERCP. There are only few international papers mentioning the post-ERCP complications in LTX patients. In these studies, the overall rate of post-ERCP complications is between 3.7%−12.5% and includes bleeding, pancreatitis, and cholangitis. The PEP frequency is shown to be between 3.7% and 6.4% (18, 19), while the frequency of cholangitis and bleeding is 3.3%−5.3% (18–20) and 1.6%−8.5% (18 –20), respectively.

Cholangiogram showing anastomotic stenosis of the choledochal duct.
The aim of this study was to determine the frequency of post-ERCP complications in a large series of LTX patients prospectively assembled in the endoscopy database at the Abdominal Center, Rigshospitalet, the only Liver Transplantation Center in Denmark.
Method and Material
The study is a retrospective evaluation of post-ERCP complications in LTX patients. Data regarding the indication for ERCP, complications associated with the procedure, procedure codes, and the description of each ERCP in our department have been prospectively collected in a database, UNICBASE version 6 (Simonsen & Weel, Denmark), since 2002.
The patients were identified by searching in the database using procedure codes for ERCP, and were cross-referenced with the diagnosis codes to exclude non-LTX patients. Furthermore, all records of identified LTX patients were retrospectively reviewed and potential variables were collected.
Inclusion criteria were age above 15 years at the time of LTX and a primary duct-to-duct anastomosis. ERCPs without successful cannulation of the papilla Vateri were excluded. The National Patient Registry was controlled for 30-day mortality in case of discharge within 30 days and subsequent lack of contact to the department. If a patient had more than one ERCP within 3 days, the procedures were interpreted as one examination. In such cases, the first ERCP with a successful cannulation was regarded as the primary ERCP, and was included in statistical analysis. A successful therapeutic ERCP procedure was defined as a procedure that cured or reduced the clinical findings indicating ERCP, with no need for another intervention within 14 days. Post-ERCP complications were defined according to the established criteria by Cotton et al. (11) (Table 1). The primary outcomes in our analysis were overall complications, pancreatitis, cholangitis, and bleeding.
Grading system for the major complications of ERCP.
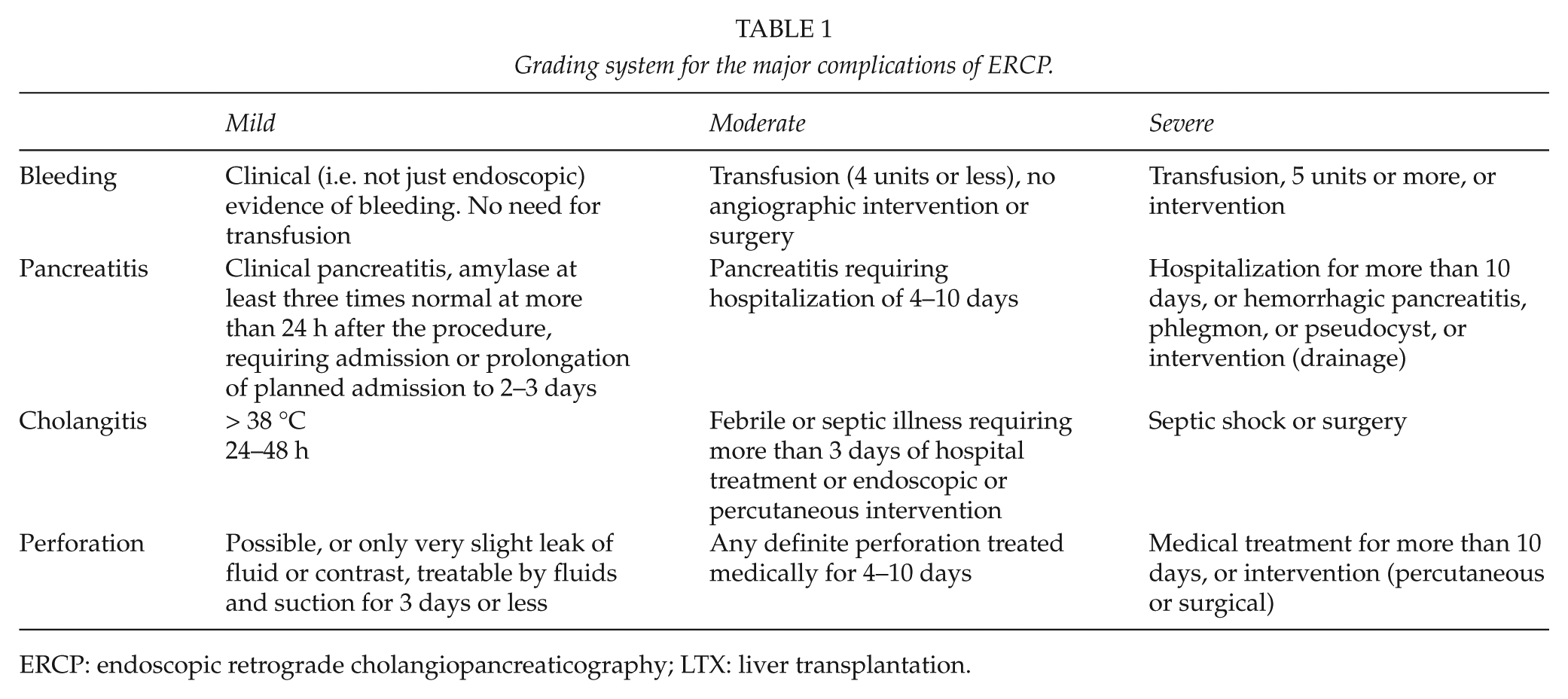
ERCP: endoscopic retrograde cholangiopancreaticography; LTX: liver transplantation.
Statistics
Statistical analysis was performed with IBM SPSS 20 (SPSS, Inc., Chicago, IL). Data significance was tested with χ2-test. Fisher’s exact test and Student’s t-test were used when required. Variables with a p value < 0.30 in univariate analyses were considered in multivariate logistic regression, using backward stepwise (Likelihood ratio) for each of the primary outcome categories. A p value < 0.05 was considered significant.
Results
From January 2003 to January 2012, a total of 323 ERCP procedures were carried out in 127 LTX patients. Of these, 31 procedures in 17 patients were excluded from the analysis, of which 30 were due to too short interval between two procedures (4 procedures), unachieved cannulation (7 procedures), or low age at LTX (19 procedures). One procedure was excluded since records concerning the procedure could not be found.
A total of 292 ERCP procedures were included, 149 (51%) in men and 143 (49%) in women. Of these, 118 (40.4%) procedures were performed in patients with native papilla, with no differences between the sexes (p = 0.17). The most common diseases resulting in LTX with duct-to-duct anastomosis were alcoholic cirrhosis followed by primary biliary cirrhosis (PBC), fulminant hepatic failure of unknown genesis, cryptogenic cirrhosis, and hepatitis C, with or without hepatocellular carcinoma (HCC). The most common indication for ERCP was biliary obstruction (or biopsy showing large duct obstruction, LDO) (51.7%) followed by cholangitis (17.5%) and stent replacement (13.7%). Of these, 261 (89.4%) and 31 (10.6%) ERCPs ended up being therapeutic and diagnostic, respectively. Of the therapeutic ERCPs, 223 (85.4%) procedures were successful and resolved or reduced the clinical findings indicating ERCP. There were no differences among men and women in the therapeutic group (p = 0.65). Of these, 38 (14.6%) procedures required further intervention (e.g. operation, percutaneous transhepatic cholangiography (PTC)) or another ERCP within 14 days (p = 0.02).
Post-ERCP complications were found after 24 (8.2%) procedures, pancreatitis following 8 procedures, cholangitis after 13 procedures, and bleeding after 5 procedures. One incidence of simultaneous post-ERCP bleeding and cholangitis, and one incidence of PEP and cholangitis occurred. There were no recorded cases of serious complications or death due to ERCP. The eight cases of PEP (2.7%) were all of a mild degree with normalization or near-normalization of S-amylase and little or no abdominal pain within 3 days after the procedure. All cases of cholangitis (4.5%) were treated with intravenous antibiotics and all post-ERCP bleeding cases (1.7%) were of mild degree (Tables 1 and 2). Sphincterotomy was performed in 80 ERCPs, of which 68 (82.9%) were at procedures without post-ERCP complications. The remaining 12 sphincterotomies accounted for 50% of the procedures (12/24), which subsequently developed post-ERCP complications.
Post-ERCP complications following 292 ERCP performed in LTX patients.
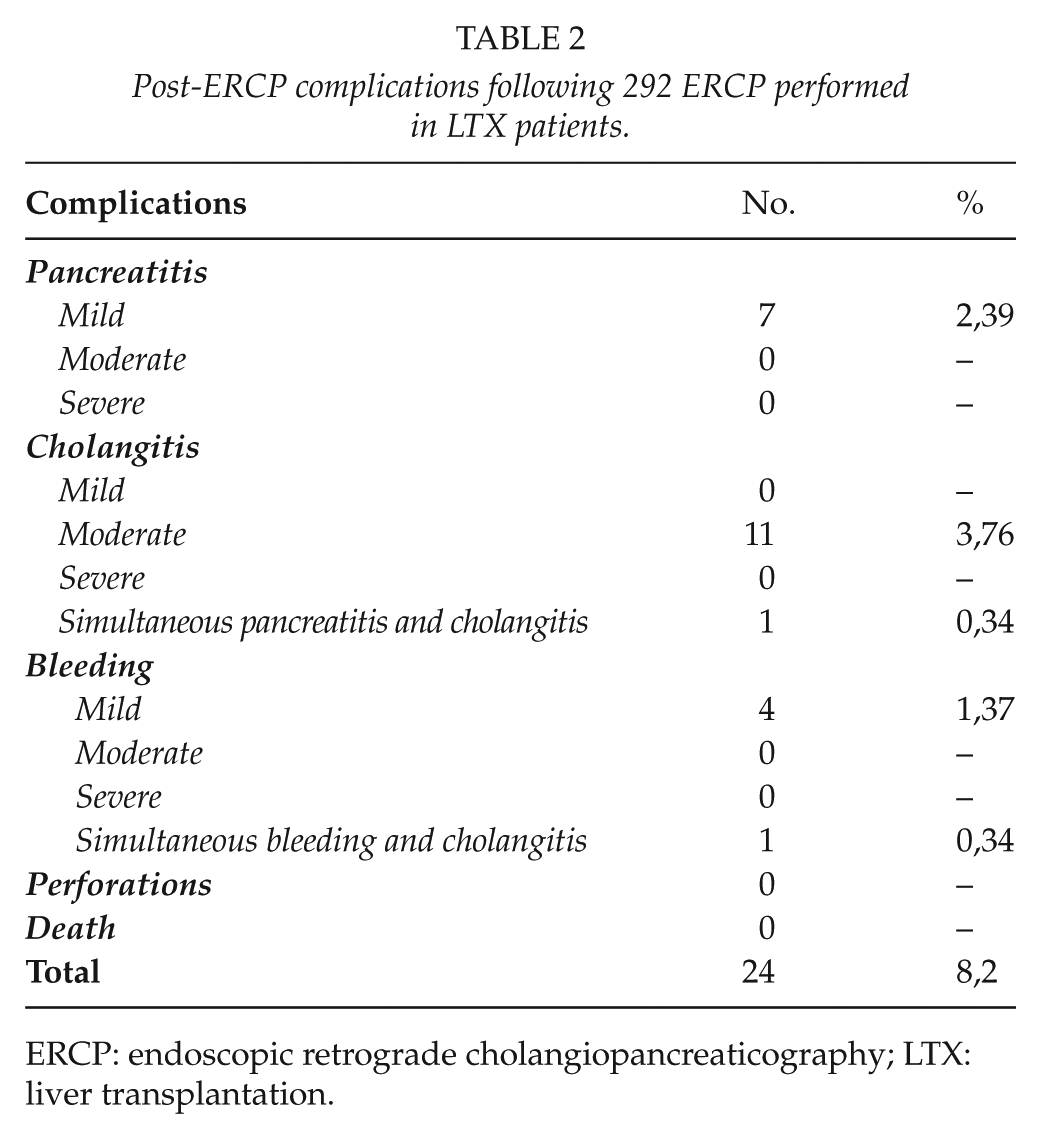
ERCP: endoscopic retrograde cholangiopancreaticography; LTX: liver transplantation.
Of the potential variables collected, univariate analyses revealed four risk factors for overall complications and one protective factor. These risk factors were biliary sphincterotomy; time since LTX within 3 months and 60–119 months, respectively; and pre-ERCP cholangitis (i.e. cholangitis as an indication for ERCP). Only biliary sphincterotomy and time since LTX within 3 months were subsequently found to be independently associated with overall complications (p = 0.006 and 0.044, respectively). Sphincterotomy was mainly associated with an increased incidence of PEP (p = 0.004) and bleeding (p = 0.026) in multivariate analysis, but demonstrated no correlation with post-procedural cholangitis. In addition, native papillae were related to overall complications (p = 0.021). When subdividing the complications, native papillae were also related to PEP (p = 0.05), but not bleeding (p = 0.34) nor cholangitis (p = 0.37).
Concerning increased PEP, the two important risk factors were pre-ERCP cholangitis (p = 0.026) and sphincterotomy (p = 0.004). Three out of four patients with cholangitis as an indicator for ERCP with subsequent PEP had normal pre-procedural values of amylase. The fourth patient had no records regarding pre-ERCP amylase.
The complication rate was 11.4% in patients without stent in the biliary tract prior to ERCP, while it was 3.7% in patients with a stent (p = 0.041). Stent in the biliary tract prior ERCP seemed to reduce the incidence of overall complications in univariate analysis. Multivariate analyses failed though to identify stent in the biliary tract prior to ERCP as a protective factor against any specific post-ERCP complication. Most LTX patients were administered prednisolone as a part of the immunosuppressive therapy. It was administered in different doses, depending on the time interval since LTX. Prednisolone doses showed no significant correlation with post-ERCP complications.
A total of 39 patients ended up going through three or more ERCPs during the period of study, counting for 186 (63.7%) of the total 292 ERCPs. There was no difference in the rate of post-ERCP complications in the group with three or more ERCPs, compared to the group with less than three ERCPs (p = 0.31).
Discussion
The Abdominal center at Rigshospitalet is the only liver transplantation center in Denmark and complications to the procedures are also cared for at this center. This offers an exceptional opportunity for establishing a database with a precise access to all patient data, and through the Danish personal identification number system (called the Civil Personal Registration (CPR)-number system), each person has a unique set of numbers which makes it possible to follow a patient through the entire affliction. We found post-ERCP complications following 24 procedures in the period from January 2003 to January 2012. Complications were observed after 8.2% of the procedures at our department, compared to 9%−16% in other studies mentioned above (Table 3). The study is one of the largest series of its kind, revealing both procedural and patient-related risk factors for complications.
Overall complications, compared with earlier studies of LTX patients.
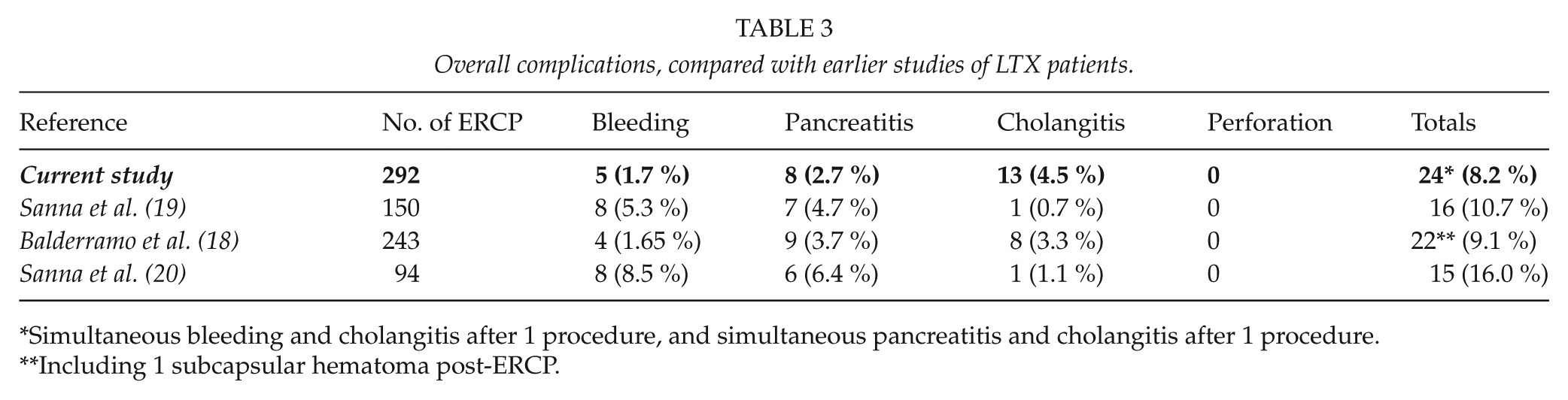
Simultaneous bleeding and cholangitis after 1 procedure, and simultaneous pancreatitis and cholangitis after 1 procedure.
Including 1 subcapsular hematoma post-ERCP.
At our department, all ERCPs performed on LTX patients are therapeutically intended. Of the 292 ERCPs during the period, 223 (76.4%) ended up being successful. There are no differences between the reported rates of post-ERCP complications in LTX patients and the complication rates in all types of patients, which have been reported to occur after 4%−12% in larger retro- and prospective studies. This is despite the fact that ERCP in LTX patients is more technically challenging. The dissimilarity may be explained both by the circumstances under which the procedures are performed (specialist center) and by patient-related factors. Moreover, LTX patients are predominantly in long-term treatment with immunosuppressive drugs that may have an influence on the complications. Long-term administration of mammalian target of rapamycin (mTOR) inhibitors (sirolimus and everolimus) has in one study been shown to increase the risk of PEP and bleeding, while long-term treatment with prednisolone may be protective (18). The potentially protective effect of prednisolone on PEP has been studied in larger prospective studies and meta-analysis in non-LTX patients. These studies showed no beneficial effects of prophylactic steroid injections prior to ERCP. However, in these studies, only the effect of single or double doses of prednisolone prior to ERCP was analyzed (21, 22). Long-term therapy with prednisolone in LTX patients could possibly reduce the negative effect of repeated cannulation and contrast injections due to the local and systemic anti-inflammatory effects. However, in our series, multivariate analyses failed to show any beneficial effect of prednisolone on either PEP or other post-ERCP complications. Future studies are needed to clarify the long-term effect of prednisolone in LTX patients.
In studies assessing post-ERCP complications, patients with a high serum-amylase (S-amylase) value prior ERCP should be excluded. At our center, S-amylase was unfortunately not consistently analyzed prior to ERCP in an exceedingly deal of the patients, and hence no patients were excluded from statistical analyses due to a high pre-ERCP S-amylase value. However, in those patients with S-amylase analyzed prior to ERCP, none had a higher than normal value of S-amylase.
Procedure-related factors have been shown to influence the incidence of complications. We found that the rate of complications following ERCP was significantly elevated in the first 90 days (interpreted as in hospital morbidity) after LTX. Anatomic factors related to the recent surgery, in combination with potential altered wound healing caused by the immunosuppressive drugs (23 –27), may partly explain the result. Also patient-related factors such as co-morbidity, use of other drugs, general health, and age are likely to have had an impact on the results, although this was not further investigated in this study.
Local procedures, such as biliary sphincterotomy, have been shown to correlate with PEP both in non-LTX and LTX patients (1, 2, 4, 8, 13, 14, 18). Surprisingly, cholangitis as an indicator for ERCP was shown to independently correlate with PEP in LTX patients. The most interesting detail is that 75% of patients (three out of four) with pre-ERCP cholangitis with subsequent PEP had normal amylase days prior to the ERCP procedure. This may reveal pre-ERCP cholangitis as another risk factor for PEP and has not earlier been mentioned in literature. The finding of pre-ERCP cholangitis as a risk factor is difficult to explain. One possible interpretation could be that post-LTX cholangitis, often coincident with anastomotic and non-anastomotic stenosis with biliary obstruction, inflammation, and edema, subsequently results in more complicated procedures using repeated cannulations and injections. It seems reasonable to assume that the number of different procedural steps in a single ERCP session have relevance for the occurrence of complications, that is, the greater the numbers of procedures at ERCP, the higher the risk for post-ERCP complications. Repetitive cannulations and injections are risk factors for pancreatitis, as repeatedly documented in non-LTX patients (2, 4, 9, 10, 13, 14). However, the results indicating pre-ERCP cholangitis as a risk factor for PEP should be interpreted cautiously, since a graft rejection may well generate the same blood sample results as a LDO/cholangitis. Furthermore, the antibiotics the patients are treated with when cholangitis is suspected may also influence the post-ERCP outcomes. At our center, all patients suspected for pre-ERCP cholangitis got the same antibiotics during the period of study, and statistical analysis concerning the effects of antibiotics could therefore not be made since it merely expresses the relationship between pre-ERCP cholangitis and post-ERCP outcomes. Nevertheless, the effects of antibiotics on PEP cannot be ruled out.
Stent in the biliary tract prior to ERCP seemed to reduce the incidence of complications in general. This has been shown in non-LTX patients earlier (14). One explanation may be the fact that all patients in our series with stent pre-ERCP had a sphincterotomy from a previous procedure, which made it easier to cannulate the biliary tract with fewer traumas, consequently resulting in fewer post-ERCP complications. Therefore, previous sphincterotomy with placement of biliary stent may be a protective factor against post-ERCP complications in subsequent ERCP procedures in LTX patients. With the foregoing in mind, patients with native papilla are anticipated to carry the highest risk of post-ERCP complications, especially in LTX patients, since this group is many times frail and cannulation can prove to be challenging. Our study demonstrated a significantly increased risk of overall complication and PEP in patients with native papilla, but no association between native papilla and post-ERCP bleeding or cholangitis. This may express the LTX patients as a complex group, with anything but normal ERCP procedures, and the risk of post-ERCP complications is therefore always eminent when performing ERCP in patients with native papilla. Also, we cannot rule out the possibility that patients with native papilla found in this study actually have a sphincterotomy from previous ERCPs many years back in time, as some patients are transplanted 15–20 years ago, with subsequently easier cannulations. This may result in understatement of the risk of post-ERCP complications following the first ERCP in this group of patients. Since only records from January 2003 were analyzed, no data regarding this issue are available in this study.
Despite the fact that LTX patients are a challenging group of patients to treat, PEP has repeatedly been shown to be of a mild grade and a relatively seldom occurring event (< 5%), both in our study and in earlier results (18 –20). The pathophysiological mechanisms of PEP are multiple and their degree of involvement unknown. These mechanisms are among others believed to be mechanic injury of pancreatic sphincter, pancreatic edema caused by sphincterotomy or thermal injury, excessive injection of contrast, and pancreatic bacterial contamination. Regardless of the mechanism, once triggered, the activation of extra-ductal enzymes is thought to cause the occurrence of pancreatitis (5, 28). Systemic inflammation follows the local activation of ductal pro-enzymes and causes a concomitant compensatory anti-inflammatory response syndrome (CARS) (29). However, CARS can be excessive, and it is believed that the imbalance between the systemic inflammatory and the anti-inflammatory response is the cause of organ failure often seen in patients with severe pancreatitis. Therefore, long-term immunosuppressive therapy in LTX patients may decrease the systemic inflammatory response, ameliorating the consequences of pancreatitis.
Limitations in this study are the retrospective design and the relatively small cohort, which among others includes risks of underreporting. Only the success or failure (success = included, failure = excluded) to cannulate papilla Vateri was recorded, not the number of attempts. For that reason, repetitive trauma to the papilla Vateri, even without achieved cannulation, may be a risk factor for PEP not mentioned in the study. Even so, the eight procedures excluded because of non-achieved cannulation of papilla Vateri showed no sign of PEP. Additionally, it is realistic to presume that a short time interval between two ERCPs (but longer than 3 days) may also be a risk factor for post-ERCP complications after the second ERCP due to the recent distress. Furthermore, the above results derive from the Abdominal center, Rigshospitalet, a highly specialized department with the required expertise and routine in the patient category, and reservations should therefore be made when comparing our results with series of non-LTX patients. Although the trend of post-ERCP complications in LTX patients seems to be similar to that of non-LTX patients, future prospective studies and meta-analyses are needed to confirm these results.
In conclusion, the rates of post-ERCP complications in our study are in line with previous studies with LTX patients. Most complications were of mild degree. Furthermore, cholangitis as an indication for ERCP may also be a risk factor for PEP in LTX patients, while pre-ERCP sphincterotomy and stenting seem protective.
Footnotes
Declaration of Conflicting Interests
None.