
Abstract
Background and Aims:
Reduction mammaplasty is an increasingly common plastic surgical procedure. In the United States, majority of breast reductions are performed as outpatient surgery. In European public health care, outpatient breast reductions have still been rare. Our aim was to retrospectively determine clinical outcome and the success rate of outpatient reduction mammaplasty.
Material and Methods:
A total of 110 consecutive patients underwent bilateral reduction mammaplasty with a minimum resection of 200 g per breast in an outpatient unit between 2006 and 2009. A comparison group consisted of 28 inpatients. Demographic data and pre-, intra-, and postoperative events as well as complications were recorded.
Results:
A total of 83 outpatients (75%) were successfully discharged on the day of operation. Reasons for unexpected overnight admission were lack of adult company for the first postoperative night (13 patients, 12%), surgeon’s wish (4 patients, 4%), hematoma requiring evacuation (5 patients, 5%), nausea (3 patients, 3%), and pain (2 patients, 2%). Minor complications, especially delayed healing, were common (45 patients, 41%), but major complications were rare (18 patients, 16%). Complication rate was not increased in the outpatient group. Increased duration of operation correlated with increasing complications.
Conclusion:
Reduction mammaplasty can be successfully and safely performed as an outpatient procedure in European public health care.
Introduction
Reduction mammaplasty is a common plastic surgical procedure with high patient satisfaction rates (1). Traditionally reduction mammaplasty patients have been followed in hospital overnight postoperatively. As surgical and anesthesiological methods have developed, the need for overnight admission after surgery in general has decreased and a dramatic rise in outpatient surgery has occurred (2). Short et al. (3) have reported the first outpatient reduction mammaplasties as early as 1989 in the United States. They found the concept to be safe and effective compared to inpatient procedures and the good results were supported by other publications (4, 5). In these early patient series, the inpatients tended to be of higher age and to have higher body mass index (BMI) and larger resections. Later on, also aged and obese patients have been treated successfully as outpatients (6), although even in this series, the obese patients seemed to have more complications. Nowadays, in the United States, the vast majority of reduction mammaplasties are performed as outpatient surgery (7).
In spite of encouraging results from the United States, outpatient reduction mammaplasties have still been rare in European public health care. In 2010, only 14% of breast reductions were performed as outpatient surgery in Finland (8). Earlier studies on outpatient reduction mammaplasties (3 –6) describe the short- and long-term outcome of patients who were discharged on the day of operation as outpatients. Perhaps because of the good availability of patient hotels in the United States, these studies have not focused on unexpected hospital admissions. When evaluating the feasibility of reduction mammaplasty procedures to an outpatient setting in European public health care, it is important to know the rate of unplanned overnight admissions. If patients who are intended to be outpatients are not discharged on the same day, this creates an unpredicted burden to already saturated hospital wards.
Outpatient reduction mammaplasties were started in our university hospital outpatient unit in 2006. The purpose of this study was to analyze the outcome of this new concept. In addition, it offered an opportunity to compare complication rates between inpatient and outpatient groups.
Material and Methods
Reduction mammaplasty patient records from the authors’ university hospital outpatient unit were examined. The retrospective study comprised a time period between September 2006 and May 2009. Inclusion criteria were bilateral mammaplasties by either pedicled technique or rarely free nipple grafting with a minimum resection weight of 400 g. The study group comprised 110 patients operated on at Jorvi Hospital. The medical records of all the eligible patients were reviewed. Demographic information of age; BMI; preoperative sternal notch to nipple distance; results of preoperative mammogram, ultrasound, and other possible imaging techniques; smoking; previous medical conditions; regular medications; and previous breast operations was collected. Skin incisions, choice of pedicle, resection weight, operative time, placement of drains, use of prophylactic antibiotics, and local anesthetics were recorded. To evaluate the feasibility of the outpatient concept, complications, reoperations, and all unexpected hospital admissions and return visits along with their reasons were recorded. Complications were further defined as minor and major. Minor complications included delayed healing (wound dehiscence of less than 2 cm, spontaneously resorbing hematomas, persistent pain in the operation area lasting from 2 to 4 weeks postoperatively), superficial infections, and seromas. Major complications were wound dehiscence of more than 2 cm lasting for more than 4 weeks after the operation, hematomas that required evacuation, deep infections requiring drainage or intravenous antibiotics, and nipple or fat necrosis.
During the study period, some of the patients who were originally assigned for an outpatient procedure were reassigned to be treated as inpatients for legislative reasons (waiting time for an outpatient operation exceeding 6 months). The demographic and clinical data of these patients were also collected, amounting to an additional inpatient-comparison group of 28 patients. This allowed for analyses of possible differences between outpatient and inpatient groups.
Statistical analyses were performed using NCSS 2007 statistical program.
Results
The demographic and surgical characteristics of the 110 outpatients can be seen in Table 1. The mean age of the outpatients was 43 years and BMI 27 kg/m2. Majority of the patients had a procedure with a pedicular nipple transposition and the average resection weight was 1186 g (Fig. 1). The operations were done by 14 different surgeons, which is reflected in the variety of incisions and pedicles that were used. General anesthesia was administered in most cases (96 out of 110) by totally intravenous anesthesia (TIVA) with a combination of propofol and remifentanil. Inhalation anesthetics, mainly sevoflurane, were used in 14 cases. To prevent postoperative nausea, patients received dexamethasone and in some cases (49 patients) also granisetron. In the recovery room, postoperative pain was treated with intravenous fentanyl and per oral ibuprofen and paracetamol as such or in combination with codeine. Drains were used in 24 cases (22%).
Demographic and surgical information of the outpatient and inpatient groups.
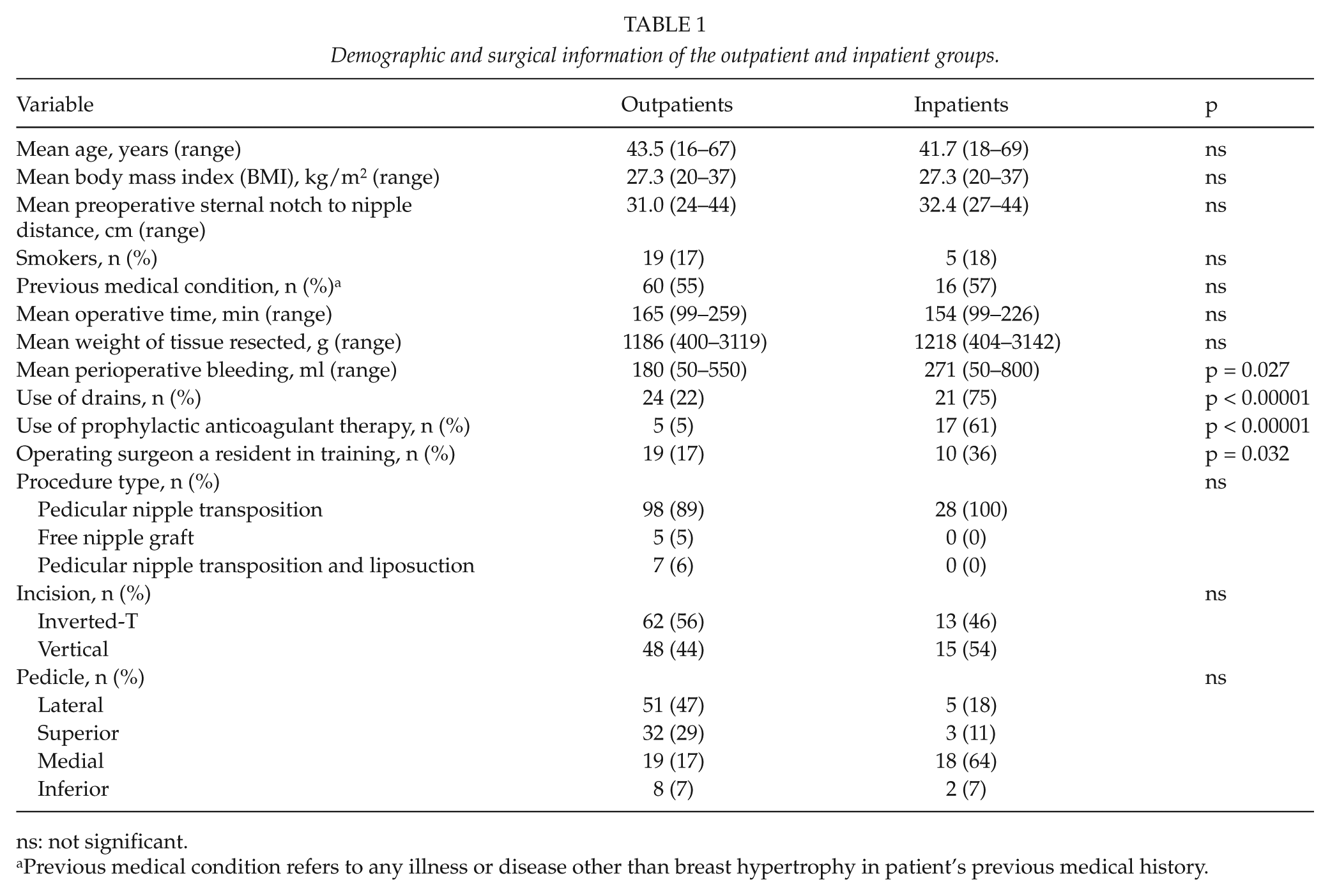
ns: not significant.
Previous medical condition refers to any illness or disease other than breast hypertrophy in patient’s previous medical history.
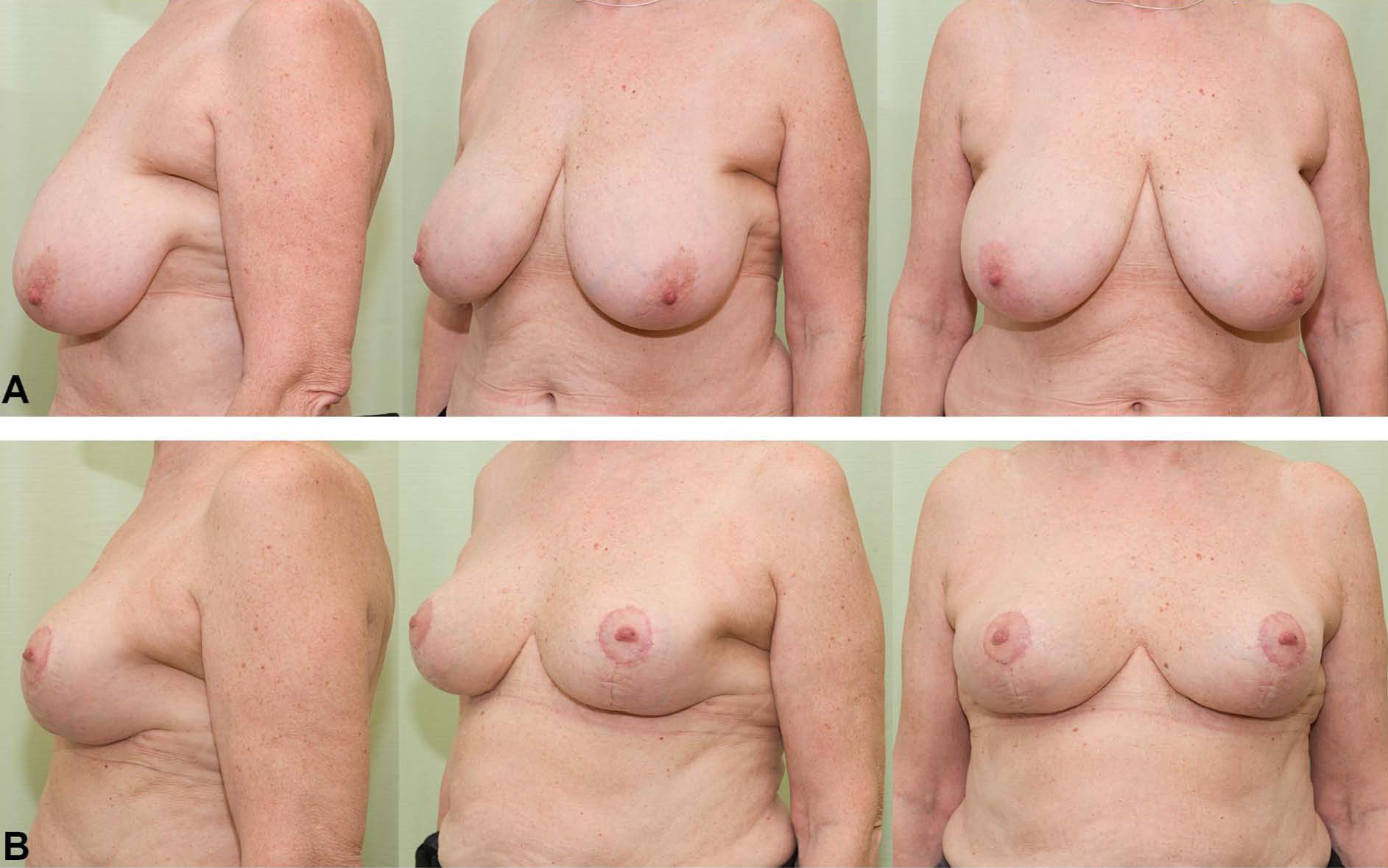
(A) A 65-year-old woman with symptomatic macromastia. In her case, the resection weights of right and left breast were 550 and 600 g, respectively. (B) The same patient 1 month after bilateral pedicular reduction mammaplasty with inverted-T incisions healing without complications.
A total of 83 patients (75%) were successfully discharged on the day of operation. The most common reason for delayed discharge was social (13 patients, 12%): there was no adult person to accompany the patient for the first 24 h postoperatively. In four cases (4%), the surgeon wished to keep the patient in hospital for the first postoperative night. Problems arising in the recovery room that hindered discharge on the same day were hematoma requiring evacuation (5 patients, 5%), pain (2 patients, 2%), and fatigue or nausea (3 patients, 3%). In statistical analysis, there were no associations between any of the demographic or surgical variables and unexpected hospital admission. Even patients with the highest age (67 years), highest BMI (37 kg/m2), and largest resection (3119 g) were successfully discharged on the day of operation. The median length of stay in the outpatient surgery unit was 9 h 10 min (range 6 h 22 min to 12 h 2 min).
Four patients, who were originally discharged from the outpatient unit expectedly, had to be readmitted to the hospital. Two of them had a postoperative infection within 2 weeks of the operation requiring intravenous antibiotics. One patient was readmitted for severe postoperative nausea on the day of the operation and one had a hematoma evacuated on the first postoperative day. During the first postoperative month, 19 patients (17%) visited the emergency room. Of these, 12 visits were made because of a suspected wound infection, 5 for other wound-related problems (bleeding, dehiscence), 1 for nausea, and 1 for chest pain, which turned out to be wound pain. There were also unplanned visits to the plastic surgery outpatient clinic (17 patients, 15%) and the nurse’s dressing clinic (24 patients, 22%) related to problems in wound healing.
The mean follow-up time was 18 months (range 6–35 months, median 12 months). Major complications were rare (Table 2). These included deep infections (7 patients, 6%), wound dehiscence of more than 2 cm (5 patients, 5%), and hematomas (5 patients, 5%). Partial necrosis of the nipple–areola complex occurred in five (4.5%) and total necrosis in four (3.6%) cases. Minor complications were more frequent: delayed healing in 49 patients (45%) and superficial infections in 17 patients (15%) (Fig. 2). Reoperations were performed for the evacuation of hematomas, necrosis, and later improvement of shape. When groups of outpatients who had either no complications or minor or major complications were compared, the only statistically significant difference was found in the operation time. The length of operation correlated positively with increasing complications (Table 3). The mean operative times for groups with no complications, minor complications, or major complications were 154, 168, and 183 min, respectively. Patient’s age, BMI, and resection weight also appeared to be higher with worsening complications, but the differences were not statistically significant. Since delayed healing was the most common complication, statistical analysis of these patients’ demographic and surgical variables was also made. Surprisingly, the only statistically significant difference was that the outpatients who had drains postoperatively had less delayed healing (5 out of 24 patients with drains (21%) vs 44 out of 86 patients without drains (51%), p = 0.008). There were also no statistical differences between groups of outpatients with or without hematomas or major wound complications.
Frequency of complications.
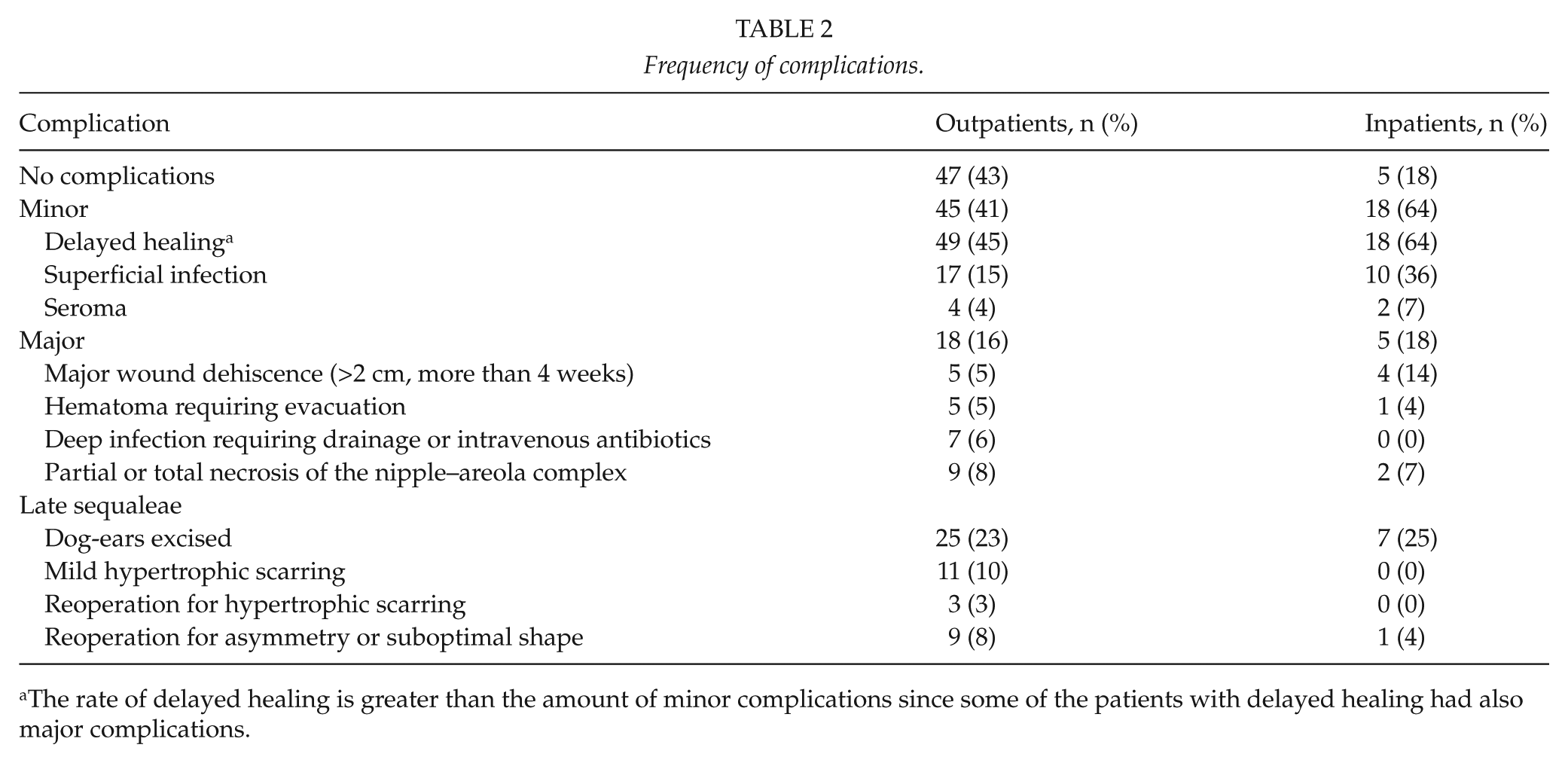
The rate of delayed healing is greater than the amount of minor complications since some of the patients with delayed healing had also major complications.

Postoperative pictures at 1 month after bilateral reduction mammaplasty with inverted-T incisions. The patient had delayed healing in the form of suture fistulae at both inverted-T junctions and below the right areola.
Comparison of complication groups.
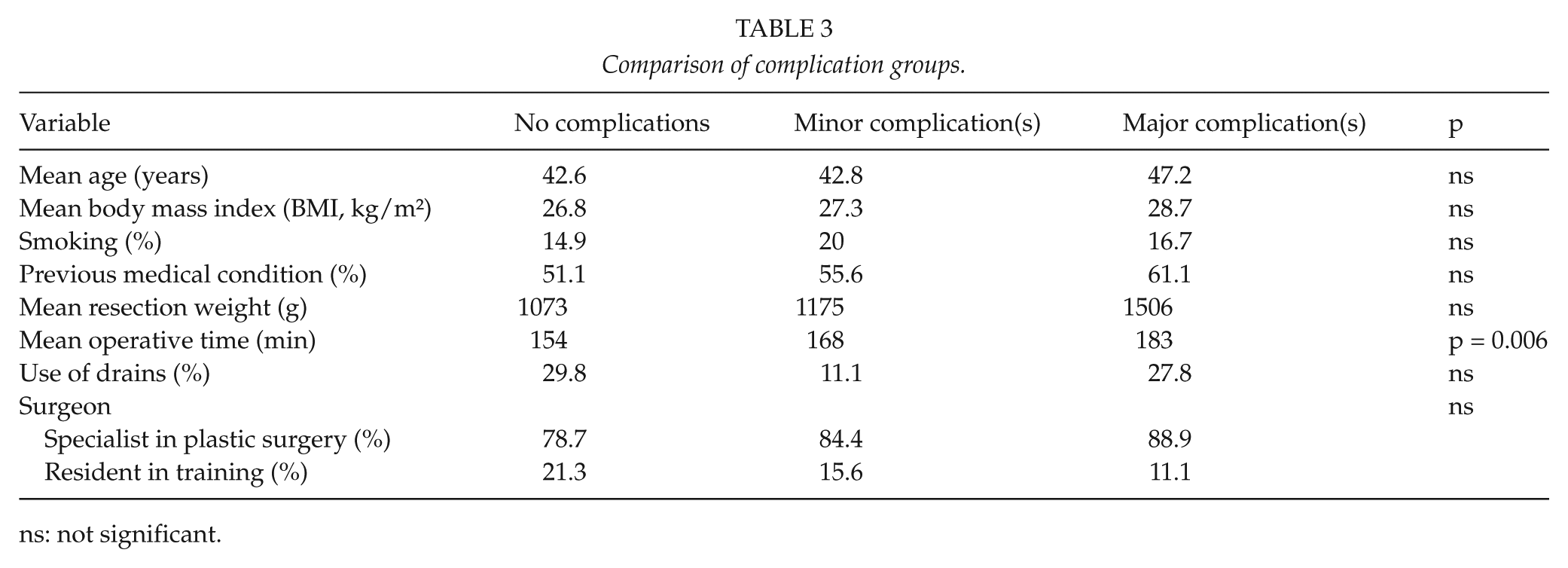
ns: not significant.
A total of 19 (17%) of the operations done in the outpatient unit were performed by a resident in training, in most cases supervised by a plastic surgeon. This did not increase the operation time (169 min for residents vs 164 min for specialists, ns), and the patients, who were operated by a resident, were as successfully discharged as those operated by a specialist in plastic surgery (16 out of 19 patients (84%) vs 67 out of 91 patients (74%), ns). The proportion of patients who had complications was also similar (9 out of 19 patients (47%) vs 54 out of 91 patients (59%), ns).
The inpatient group consisted of 28 patients. The patient characteristics were similar to the outpatient group (Table 1). The operative techniques were also similar, but the surgeon was more often a resident in training. Drains were used significantly more often, in 21 patients (75%). Unlike in the outpatient group, the use of drains did not decrease the rate of delayed healing. When drains were used, delayed healing occurred in 14 cases (66%) and without the use of drains in 4 cases (57%). Of the inpatients, 17 (61%) also received prophylactic anticoagulant therapy, which was rare in the outpatient group. Median length of stay in the hospital was 31 h (mean 41 h, range 27.5–101.5 h). There were no readmissions to hospital in the inpatient group, but the amount of unplanned visits to emergency policlinic was significantly higher than in the outpatient group (10 patients, 36%, p = 0.032). The overall rate and especially the rate of minor complications were significantly greater in the inpatient group when compared to the outpatient group (18 inpatients (64%) vs 45 outpatients (41%), p = 0.041), but there was no difference in the amount of major complications (5 inpatients (18%) vs 18 outpatients (16%)) (Table 2).
Discussion
Reduction mammaplasty patients can be successfully treated as outpatients. In our study, we found that a common reason hindering discharge on the same day was a lack of adult company for the following 24 h or the surgeon’s insecurity with the outpatient concept. These reasons should have been acknowledged already preoperatively in the patient selection phase and the patients should have been treated as inpatients to begin with. The rate of unplanned admissions in our study (25%) was higher than expected when compared to outpatient surgery in general (0.85%–4.7%) (9, 10) and to plastic surgery specifically (3.55%) (11). This difference may be due to the less invasive and shorter operations included in the above-mentioned studies. In a meta-analysis of laparoscopic cholecystectomy, which nowadays is widely accepted as outpatient procedure and similarly involves general anesthesia and variably long operation time, the admission rate was 19% (12). If the patients who were admitted for social reasons and surgeon’s wishes were omitted from the outpatient group, the rate of unplanned admissions would have been as low as 11% in our study. Therefore, with careful patient selection and information, acceptable admission rates can be achieved. There were no specific patient- or surgery-related factors that could predict unplanned overnight admission, and thus, normal widely accepted criteria for the selection of outpatients can be applied (13).
Only four patients were readmitted to hospital after discharge, indicating the safety of same day discharge. All readmissions and unscheduled visits were related to true or suspected surgical complications. There were no other medical, nonrelated morbidities (e.g. cardiovascular morbidity) in the postoperative period as well as no mortality. Many of the outpatients needed unscheduled visits to policlinic, but the amount was even higher in the inpatient group. A large number of the visits were related to the patient’s concerns of the wound healing process. Simple counseling was all that was needed and the visits were often unnecessary from a medical point of view. Therefore, it can be stated that the outpatient concept did not increase the need for policlinical services but rather might even decrease it. This may be due to the fact that outpatient surgery unit personnel are especially dedicated to give coherent information to the outpatients on the convalescence period and wound treatment thus decreasing the need for revisits.
The complication rate in our study was high, and less than 50% of the patients healed with no complications. True, self-critical, and accurate reporting of complications is a trade mark of the Finnish health-care system and is also reflected in our study. In literature, the complication rate of reduction mammaplasties ranges from 11.4% (14) to as high as 77% (15), but is mostly between 40% and 50% (16 –18) and thus similar to our study. The overall rate of complications was significantly lower in the outpatient group when compared to the inpatient group, indicating that the outpatient concept was also safe from this aspect. The majority of the complications in our study were minor, mostly wound dehiscence, which is in accordance with earlier studies (16 –18). The amount of major complications was also similar to earlier studies (15, 16, 19). As the complication data were collected retrospectively and very precisely from patient charts, it might be that the wound dehiscence group contains even the smallest suture fistulae, thus increasing falsely the rate of complications. Patients, who had longer operations, had more complications. Other than working to decrease the operation times, the statistical analysis did not reveal any factors that could be avoided or treated in the hope of preventing complications. Altogether, wound healing problems in this type of surgery are very frequent, and scheduled control visits to the dressing clinic are beneficial for outpatients and inpatients alike.
The use of postoperative drains after reduction mammaplasty has previously been shown to be unnecessary (20, 21). In this study, drains were used on 22% of the outpatients but significantly more often on inpatients (75%). Similar drainage percentages were reported in an earlier study comparing outpatient and inpatient reduction mammaplasties (3). There was no difference in hematoma formation between the inpatient and outpatient groups, thus indicating the safety of outpatient procedure without drainage. In the outpatient group, drains were removed either before discharge on the operative day, like was done by Mandrekas et al. (14), or the following day in the patient’s own health-care center. In two cases, the surgeon wished for overnight surveillance in hospital because of the placement of drains. There was no hematoma formation in these cases, but both of them developed later a deep wound infection requiring drainage or intravenous antibiotics, suggesting that the drains might have acted as routes for postoperative infection. In the outpatient group, drainage was associated with a lower rate of delayed healing. This was not true in the inpatient group, where the rate of delayed healing was greater for patients with drains. The reason for this finding remains unclear, as delayed healing was not associated with any other demographic or surgical variable, including surgeon’s experience. Altogether, if the surgeon wishes to use drains, it is not an obstacle for same day discharge as an outpatient.
In conclusion, our study showed that reduction mammaplasties can be performed in the outpatient setting also in European public health care. The rate of unexpected admissions was acceptable and there was no increase in the number of complications but a tendency of decreased revisits was noted. The number of admissions for social reasons in our study was too high, pointing out the importance of careful patient selection for outpatient surgery. With the increase in outpatient procedures, resources needed for in-hospital treatment can be decreased or better allocated to patients in true need of hospitalization. A cost–benefit analysis on outpatient reduction mammaplasties is in progress.
Footnotes
Acknowledgements
The authors wish to thank Tero Hanski ja Jussi Kirjavainen for the photographs and Timo Pessi for the performance of statistical analyses.
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
This study was supported by a grant from the University Central Hospital of Helsinki (EVO grant no. T102020P27) and a grant from the University Central Hospital of Turku (EVO grant no. 13605).